
Abstract
Pharmacy plays a pivotal role in supporting acute clinical care pathways. However, across hospital environments, pharmacies are often stretched by growing service demands and conflicted by increased medication and service costs. Ultimately, such factors contribute towards process inefficiencies that impact on the provision of healthcare services. Following a literature review, we examined clinical pharmacy services by undertaking three acute hospital pharmacy case studies. We adopted an ethnographic approach, observing and interviewing pharmacists, pharmacy staff and nurses. With a view to improving healthcare information systems (ISs), we identified the enablers and barriers in service efficiency, thus identifying opportunities for pharmacy IS implementation across acute hospital environments. The findings also reveal some of the key enablers and barriers towards the introduction of hospital IS innovation. We present recommendations to overcome such barriers.
Introduction
Healthcare informatics is one of the fastest growing healthcare disciplines in the world today, 1 with much of its focus on specific technologies2,3 and patient empowerment4,5 through health technology–enabled solutions. 6 In this article, we are interested in pharmacy informatics which has been defined as ‘the scientific field that focuses on medication-related data and knowledge within the continuum of healthcare systems – including its acquisition, storage, analysis, use and dissemination – in the delivery of optimal medication-related patient care and health outcomes’. 7 In particular, we are focusing on pharmacy in the acute hospital setting where it is central to care. In this setting, patients often present with multiple medical issues. Nearly every patient who is admitted to hospital will receive at least 1 medicine during their stay, with many of the medical patients being prescribed anything between 5 and 9 medicines and some patients receiving up to 30 medicines. 8 In a recent Irish study by O’Sullivan et al., 9 84.5% of older hospitalised patients had polypharmacy on admission, with 43% having 10 or more medicines prescribed, illustrating the complex medicine needs which patients frequently have. The combined national drug budget for hospital medicines is in excess of €300 million per annum. 10 These medicines vary from simple aspirin to more complex intravenous medicines that need to be specially compounded for patients for their cancer and other treatments. In 2014, €1.8bn out of a total Irish health budget of €12.4bn (14.5%) was spent on drug treatment. 11 Such rising costs require that healthcare examines how it can become more efficient and effective.
Therefore, we look to information systems (ISs) that are typically viewed as an enabler for improved efficiencies and effectiveness across all sectors including healthcare. However, prior to considering the implementation of any new healthcare ISs in hospital pharmacy practice, enablers and barriers should be identified. The research presented in this paper aims to do this, reporting on three hospital pharmacy case studies.
Research aim and methodology
The aim of the research is to understand the enablers and barriers within acute hospital pharmacy services, with a specific interest in how pharmacy ISs can potentially work. Therefore, we set out to address the following research questions:
What are the enablers that support acute hospital pharmacy service improvements?
What are the barriers that prevent acute hospital pharmacy service improvements?
We have undertaken case studies in three acute hospitals, comprising of two public hospitals and one private hospital:
We were guided through the clinical pharmacy service with the support of the chief pharmacists where we observed the pharmacy team carry out certain tasks (see Figure 1). We employed techniques outlined by Nelson et al., 12 for example, using various writing locations, writing key themes and verifying information with key stakeholders across the pharmacy team and wider hospital staff. Observations were conducted through a total of four visits (each visit averaged 4 hours), followed by semi-structured interviews with key members of staff. A walk through the hospital pharmacy environment was undertaken, providing the opportunity to interact with key staff involved in various functions to deliver clinical pharmacy services, including pharmacists, pharmacy staff and nurses. The pharmacy teams comprise an average of 6–8 members, mainly pharmacists, dispensary staff and technicians. We were provided with an opportunity to examine a snapshot of how clinical pharmacy services were managed and conducted on a day-to-day basis. We shadowed pharmacy staff in their specific roles while delivering drugs to ward staff and to specific patients. We posed questions about key pharmacy processes, their subprocesses and specific tasks. We also observed how staff interacted with one another and how patients would typically receive medicines. While we documented our observations and answers to questions throughout the whole observation and interview process, notes are not included in this paper to protect the anonymity of our research participants.
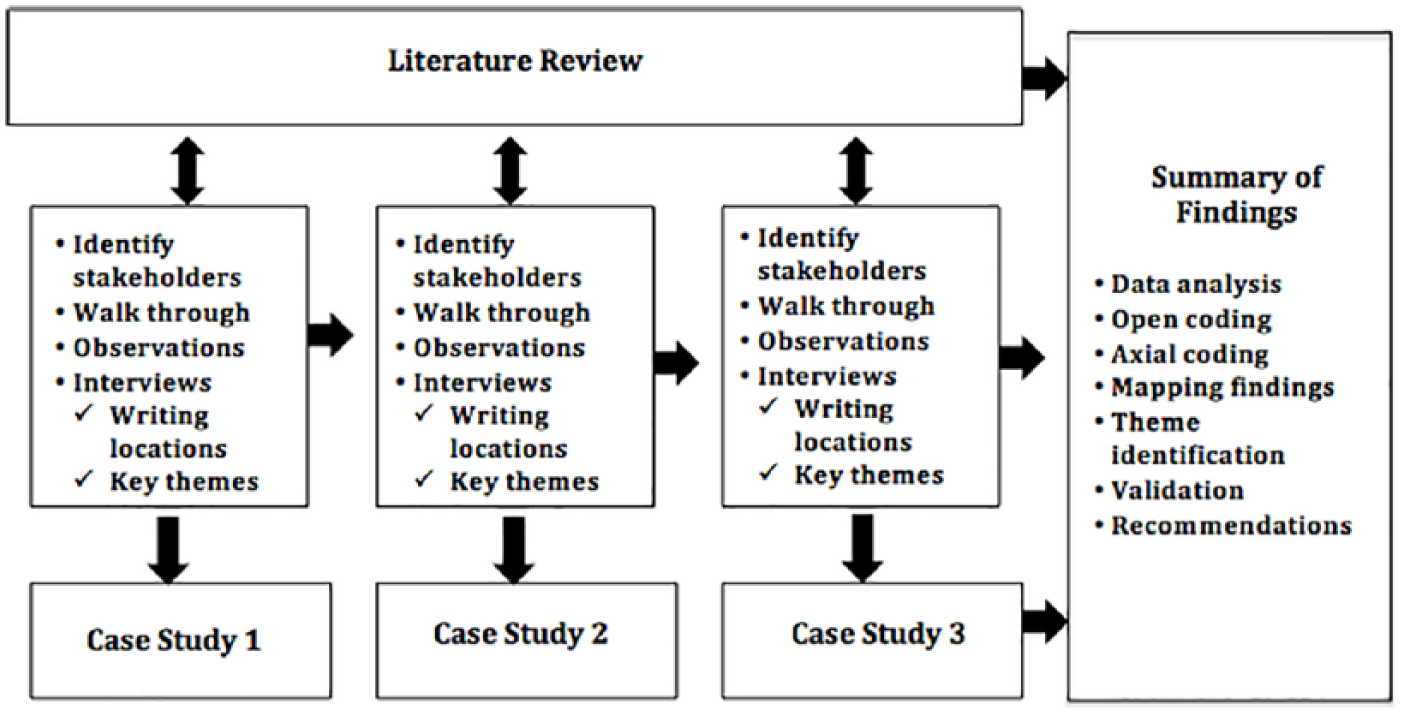
Research overview.
Data analysis was undertaken using various coding techniques. In the initial phase, ‘open coding’ was used to determine the main ideas and themes in each transcript. The open coding phase was initially categorised according to key concepts and various subcategories. This was followed by ‘axial coding’, which is the process of relating categories to their subcategories. We then mapped our findings according to the literature while remaining open to the identification of alternative and new categories of concepts. Once a relationship was determined, the focus returned to the data to question the validity of these relationships to pharmacy. During this stage of analysis, category processes were also examined, which involved looking at the actions and interactions performed in the context or intervening conditions. Thus, by blending the strengths of existing text analysis techniques and coupling them with our literature review, concept mapping offered a way to represent meaning. Ethical approval was granted for these studies through the HSE and university ethics committees.
Findings: key enablers of pharmacy processes
Our first research question studied the enablers that support acute hospital pharmacy service improvements. Results can be categorised into (1) the need for pharmacy informatics, (2) a national pharmacy strategy, (3) empowerment of pharmacists, (4) medicine management and (5) pharmacy workflow.
Need for pharmacy informatics
There are several key enablers for process improvements within pharmacy management which contribute value on a number of levels: healthcare quality, behavioural change, economic impact, service delivery and staffing performance. The literature focuses on three main roles: documentation, medication reconciliation, and patient evaluation and monitoring. However, according to Nelson et al.,
13
‘as health information technology proliferates, it is imperative that pharmacists’ workflow and information needs are met within the EHR to optimise medication therapy quality, team communication, and patient outcomes’. However, our findings indicate that there is a lack of standardised modelling techniques to guide process improvement and to identify service bottlenecks. For example, we were presented with Microsoft Excel files and whiteboard charts capturing ordering and dispensing times to measure efficiency and delay times: We don’t exploit modern technologies to provide a world-class service. We know that technology supposedly offers new opportunities to improve efficiency within a service, and therefore, can save us time while improving safety and quality of care. Excel is a little dated? There must be other opportunities, not just new tools but in terms of new techniques also? I think we need to get our technical and clinical people into the same room to discuss such opportunities rather than working in silo. (Pharmacist – Hospital 1)
Such efforts merely identify a problem but do not capture the root cause or indeed the consequence of inefficiencies and potential pharmacy errors. Our results indicate that there is a lack of a process improvement vocabulary across hospital pharmacy services. In particular, the concept of lean 14 (e.g. ‘lean hospitals’, ‘lean healthcare’ or ‘lean medical’) emerged as a critical factor for pharmacy throughout the literature and indeed through our observations. Lean techniques offer a methodology towards an improvement approach that eliminates waste and processes that do not add value to the patient. The key objective in eliminating waste is to improve efficiencies by reducing costs and improving the flow of patient care and healthcare resources. This would ensure the adoption of an interdisciplinary approach to pharmacy management and service innovation. However, as approaches such as ‘lean’ have stemmed from manufacturing-oriented disciplines focusing on input-process-output, we suggest that translating such workflows directly from their current format underrepresents the complexity and dynamics of pharmacy and fails to capture the multifaceted nature of pharmacy practice and calls for more emphasis on pharmacy informatics management. The literature suggests that we need pharmacy informatics expertise to identify what and how pharmacy ISs are used, designed and managed. For example, Fox et al. 15 have highlighted that pharmacy informatics education is inconsistent and describes how pharmacy informatics will inevitably become commonplace in pharmacy graduates’ practice environment. However, years later at the time of presenting these findings, our evidence suggests that such ambitions are far from ‘commonplace’. Indeed, Enright et al. 16 suggest that within pharmacy ‘leadership skills development is inadequate in our education and training, and few of our highest potential talents are equipped to handle emerging leadership responsibilities’. Pharmacy informatics should not be viewed as a role per se but rather as a cultural philosophy and practice shift towards process optimisation and healthcare quality effectiveness.
It’s not that we don’t have good ideas to improve practice but you must understand that any innovation is stifled within this heavily regulated area of pharmacy. And even if we managed to get over that, from my experience, it is extremely challenging to get buy-in from senior management because they either don’t see the benefit of investing in technology, i.e. the “why fix it if it’s not broken” attitude, or simply don’t understand the complexities of pharmacy to identify the clinical benefits of freeing up some of our time-consuming tasks. (Pharmacist – Hospital 2)
National pharmacy strategy
Developing a national pharmacy strategy within the Irish healthcare system (or indeed any other healthcare grouping) would encourage, facilitate and support the greater participation of pharmacists in the redesign and delivery of patient-centred and cost-effective pharmacy services. Such a strategy would also facilitate pharmacy service development in accordance with international evidence-based practice. Our findings indicate that there is little evidence of national pharmacy informatics programmes which would support pharmacies to optimise service operation.
I think that one of the major stumbling block for national improvement in hospital pharmacy is the lack of a core national strategy so that we are all on the same wavelength when it comes to driving excellence in our service. I think the reason for a lack of a strategy comes down to pharmacist being a very small group within the broader hospital context and therefore and underrepresented when compared to wider hospital strategies. So for example, looking to the future of e-health, in the case of hospital informatics, we see this as a need yet such ideas get little airtime when compares to other hospital departments or divisions. (Pharmacist – Hospital 1)
Without a clear national strategy, there is little guidance to support pharmacists and therefore a lack of a solid foundation to build pharmacy informatics to meet national hospital pharmacy needs. Thus, the development of a national pharmacy strategy should be prioritised, forming a national team with various pharmacy special interests.
Empowerment of pharmacists
Similar to the Royal Pharmaceutical Society,
17
our findings suggest that pharmacists are an underutilised resource in the delivery of patient care. On three separate occasions at both public hospitals, we observed how pharmacists’ interactions with patients provided a clear and timely benefit to delivering patient-centric care: I much prefer to be out discussing treatment plans with patients and learning about their needs rather than being in the pharmacy department. (Pharmacist, Hospital 1) I think our role as pharmacist is changing with we have a greater workload to cater for such change. We need to be on patient wards as medicine is a core part of any treatment plan so we play an integral part of that process. (Pharmacist, Hospital 2) The simplest way to describe why we need to be more patient-centric (… and by that I mean visible to the patient) is to simply follow the drugs. If you track the movement of drugs in terms of medicine management, you’ll see numerous areas for improvement and reduce possible threats to patient. We often learn about the problems when its too late but of we are on the ward we would have greater vigilance to potential mistakes and threats to patient care. (Pharmacist, Hospital 1)
In these cases, the availability of the pharmacist was effective. Exploring ways to redesign patient care would encourage pharmacists to engage in more collaborative healthcare developments. This could dramatically reduce errors, eliminate wasted resources and improve safety, thus freeing up service capacity. Pharmacists should be empowered to play a more visible role in patient care and to redesign medicine management processes.
I guess, in this private hospital we do learn from new business developments such as lean practices. We are entrusted to improve pharmacy practices where possible but any proposed change must be validated without jeopardising patient care. By being empowered to propose change, we are encouraged to seek improvements in practice. (Pharmacist – Hospital 3)
Pharmacists were also empowered to address concerns associated with patients’ lack of understanding of their treatment plans. Indeed, pharmacy informatics could expand into other areas outside of the pharmacy dispensing workflow, such as supporting how pharmacists document their clinical notes in the electronic health records. This demonstrated how pharmacy expertise may be best utilised within wards and providing care closer to patients.
Medicine management
Medicine management is a complex process and requires service transparency and monitoring to support key decision-making tasks. In addition, it is important that pharmacy dispensing provides efficient, effective and auditable delivery of medication to patients. The use of IS can improve interaction between the wider healthcare professional team on patient rounds. For example, using an IS ensures a structured approach to capturing data while employing specific rules in accordance with pharmacy guidelines. On one occasion, we witnessed a decimal point error on a prescribed dosage for a patient: Sometimes, it the simple things such as handwriting or note-taking which becomes a critical issue for medicine management. We know that digitising processes would pick up on errors, for example, over-prescribing a high-risk drug for infants. (Pharmacist, Hospital 1)
This has two key implications. On one hand, depending on the risk associated with the drug and the patient’s condition, if a patient received too high a dosage, it could have fatal consequences for a patient. One the other hand, if a patient received too low a dosage, it fails to provide safe and quality care to the patients and also generates costs without any benefits. IS can ensure adherence to data entry rules. IS can also be used to disseminate patient information while delivering required medication or to support patient discharge counselling. Medicine dispensary processes could include an electronic prescription system authorised by pharmacists. Robotic dispensers have been successful in hospitals internationally and our research participants identify the potential benefits of such innovations.
There are some hospitals in Ireland using robotic dispensing systems and they are really efficient and safe systems. I guess we are often tasked with making the business case for such innovations but we are simply to busy to get time to develop cases for these technologies. (Pharmacist, Hospital 2) We have looked into a robotic dispensing system and it is still on the cards as part of our hospital strategy. Having experience working in other hospitals I can really see the benefits of robotics in this hospital. I have had a team explore the cost-benefit analysis which presented some pros and cons. The next step for me would be to invite managers on-site to other Irish hospitals to witness the benefits. (Pharmacist, Hospital 3)
The current pharmacy model we observed does not provide any form of weekend working shifts which needs to be addressed as in other Organisation for Economic Co-operation and Development (OECD) nations. More flexible staffing arrangements could be put in place to accommodate patient’s needs, for example, weekend pharmacy services. In addition, the level of pharmacy–patient contact time should be improved, that is, number of hours pharmacists work in a hospital (e.g. approximately 39 hours) versus the number of hours patients wait in hospital (e.g. 7 days × 24 hours). This highlights the need to revisit how pharmacy should integrate ‘patient-centric’ care or begin to explore alternative pharmacy workflow innovations. It also highlights what the American Society of Health-System Pharmacists 18 describes as the need to ensure technologies lead to safer and more effective medication use.
Pharmacy workflow
There is an apparent need to improve the workflow of medicines in hospital, which suggests that this could improve nursing and pharmacy staff productivity. We witnessed manual efforts capturing order times and dispensing times that was disconnected to other hospital workflows. For example, monitoring medicine workflows throughout the hospital and ensuring that drugs ordering is monitored, measured and managed right up to the medicine adherence process by patients will shed more insights into areas for improvement and zones where potential risks exist.
I think there is a real opportunity to model how the system operates day-to-day and examine the flow of medicine entering the healthcare system all the way up to medicine adherence across patients and their effects. Our current system doesn’t really capture the risks associated with pharmacy workflow in medicine management. As the saying goes, its you can’t measure it, you can’t manage it. (Pharmacist, Hospital 3)
By establishing innovative pharmacy workflows, this could relieve healthcare professional stress while providing improved safety benefits to patients. For example, new workflow methods have been adopted, for example, the Foundation Improvement Science in Healthcare (FISH) at Hospital 1. However, to initiate hospital-wide change, this requires culture change to move from the local pharmacist to the wider healthcare institution. For example, the introduction of a job-tracking system that provides feedback on the service performance at different stages would provide the team with a real-time insight into how they are responding to healthcare demand. Our findings also uncovered that there was also a growing sense of opportunity to foster an innovation culture to examine how the introduction of ‘small-technology changes’ could impact pharmacy workflow.
We encourage our team to solve problem in practice even if they are small such are recording medicine management in a new format, or more advances solution. We need to empower our team to take responsibility for the service they provide. So it makes sense for them to lead improvements across our pharmacy service. (Pharmacist, Hospital 3)
Findings: key barriers of pharmacy processes
Our second research question focused on identifying the barriers which prevent acute hospital pharmacy service improvements. Our findings are categorised as follows: (1) barriers to innovation, (2) cost of pharmacy inefficiencies and (3) measuring to manage pharmacy services.
Barriers to innovation
We learned about innovations which pharmacists had been working on and/or proposed to continuously improve service operations. For example, at Hospital 1, the pharmacists identified the need to optimise pharmacy services. At Hospital 2, the pharmacist had developed a business case to implement dispensary robotics within the hospital. At Hospital 3, there were efforts to examine service quality improvements. Each of these examples demonstrates the strong desire among the hospital pharmacy community to improve patient safety, quality of service and service efficiency. However, there are significant barriers that hamper innovation for them. Most notably are legislation requirements and dwindling public funds to invest in pharmacy innovations. This adds to the complex nature of the pharmacist role and the tensions between innovation and regulation.
Ireland is one of many countries where pharmacy operates within a heavily regulated environment governed by legislation. This makes it extremely challenging to innovate. In addition, the lack of government funds makes it extremely challenging to implement change and to introduce new healthcare resources indicating that the pressure to deliver a more efficient pharmacy service is likely to persist. (Pharmacist, Hospital 2)
Cost of pharmacy inefficiencies
There is a need to push hospital and community care closer to patients and to develop pharmacy IS innovations for the provision of access to consumer data. Our findings indicate that there is a disconnect between hospitalised patients and patients discharged. Ensuring that the patient journey is monitored within a community setting enables hospital pharmacy to extend services at potentially high-risk stages after being discharged from hospitals. Catalysing collaborations throughout the hospital and community environments are forging new developments on drug value and delivery, moving from traditional business process concerns towards a new health economy and focusing on patient-centric solutions and improved value networks. The findings suggest that different healthcare services can work collectively to offer cost efficiencies.
We should think about how we can better manage the cost of operating pharmacy departments, ranging for exploring generic drug brands against high cost drugs, dispensing and storage, and dispensing. This would be common practice in business. It should be examined in high risk environments such as healthcare. (Pharmacist, Hospital 1)
We believe these can be transferred to other healthcare systems such as public healthcare services. New models of care and collaboration between various healthcare professionals and departments will support more joined-up thinking, sharing of knowledge and skills that support hospital and pharmacy management. It would also allow us to redesign the delivery of pharmacy services beyond a hospital context and extend services into the community environment.
Measuring to manage pharmacy services
Examining how pharmacy processes are executed and measured provides a vital insight on management processes and enablers to optimise service operations. There have been some studies that identify a correlation between pharmacy services and mortality rates.19,20 Within an Irish context, which operates with scarce resources, our findings indicate that more insights need to be developed on hospital pharmacy supply service levels and patient safety, for example, queuing systems and service analytics. From a pharmacy perspective, the main strategic goal is to achieve a substantial reduction in medicines supply lead time from prescription to administration, and missed doses should be the key safety metric to identify relationships between queuing systems, safe medication supply and patient well-being. Our findings also highlight the need for improved hospital’s pharmacy staffing levels to improve patient safety and medicine management. For example, staffing hospital pharmacy departments for on a 24/7 model should be available to patients to ensure patient care is available on demand across hospitals. In addition, this research highlights the potential waste of medicines, costs associated with waste (millions of euros) due to poor stock control management strategies and tools and the impact of poor quality medicine products on patients’ healthcare. While it is considered appropriate to maintain high stock levels of medicines, there may be new opportunities to move away from the ‘just-in-case’ approach and towards a ‘just-in-time’ approach in medicine management. Central to improving medicine management may be the need to reconnect to community healthcare providers to gain early insights of possible patients entering the hospital healthcare system. While acknowledging the difficulties this may pose given the wider national healthcare staffing crisis, it may also be an opportune time to examine the business case for pharmacy IS solutions to support workloads and lead times in medicine management.
Discussion
Our research indicates that pharmacy, from a generalised perspective, needs to be improved and redesigned to benefit from process improvements. To this end, we are using Ireland as an exemplar of what is currently taking place. Within the hospital sites we learned that, to develop an understanding of how different healthcare services can work collectively, new models of care and collaboration between various healthcare professionals are required.
Related work
Healthcare IS innovations can provide access to consumer data throughout the hospital and community environments. 40 The benefits of implementing healthcare IS include the growing focus on patient-centric solutions and improved value networks.21,22 A hospital pharmacist has an important role in the patient’s hospital journey. They are tasked with the provision of pharmaceutical services for a number of different hospital units and wards and largely deal in prescription drugs, fill out the script and working with physicians to provide safe and quality care. Hospital pharmacists ensure safe and effective use of medication, provide drug information and advice, educate prescribers, nurses and patients and prevent medication errors. Thus, hospital pharmacy service is complex and a core part of any clinical care pathway, and our previous research has shown that the improvement, redesign and management of pharmacy through the implementation of pharmacy IS are fundamental to improving the healthcare service system. 23 Furthermore, there is evidence that clinical pharmacy service providers view their healthcare service systems in a process-orientated manner,24,25 borrowing many techniques from businesses, for example, lean healthcare 26 and business process analysis. 27
Focusing specifically on clinical pharmacy services, it is important to ensure that everyone involved, for example, schedulers, laboratory staff and clinicians, understands the purpose and scope of pharmacy services. 28 Identifying methods for integration of clinical pharmacy services into the provision of patient care services is also critical. Pharmacy IS alone is not the solution, but rather, it is a means to optimise service performance. However, numerous barriers exist, which inhibit pharmacists in proposing and/or implementing such systems. For example, Nanji et al. 29 examine barriers to, and facilitators of, the implementation of a pharmacy bar code scanning system. They identified three main barriers to pharmacy IS implementation: process (training requirements, process flow issues), technology (hardware, software, role of vendors) and resistance (communication issues, changing roles, negative perceptions about technology). They propose adequate training, continuous improvement and adaptation of workflow as strategies to overcome barriers. In addition, Holler 30 examines the role of IS in advancing pharmacy practice and improving patient safety, suggesting that pharmacists view technology as an opportunity to increase efficiency and to improve access to vital information. He suggests that pharmacy IS is considered as a means of improving patient safety, especially processes of care for threats to safety – something similar to the ‘Triangle Model’. 31 The Triangle Model acknowledges the interactions between technology, providers and organisations and their impact on patient-centric care. Within a pharmacy context, Siska and Tribble 32 performed a gap analysis based on the ideal future state of pharmacy IS. They identified that pharmacy requires mores service such as continuum of care, improved standardisation, interoperability, resource tracking, auditing and evaluation. In addition, Hudson et al. 33 propose that future pharmacist roles will adopt a ‘wider use of quality systems to address errors in prescribing and drug administration; the automation of systems of drug prescribing and administration and improved documentation of care’. Thus, the pharmacist will become a core treatment support for patients within both the hospital and community during their transfer of care.
A care pathway is defined as a multidisciplinary care plan that outlines the main clinical interventions that are carried out by different healthcare practitioners for service users with a specific condition or set of symptoms. They are usually locally agreed, evidence-based plans that can incorporate local and national guidelines into everyday practice.
34
Due to rising healthcare costs and increasingly limited resources, the development and standardisation of such clinical care pathways have been used to support quality management. 35 Furthermore, Pinder et al. 36 discover that ‘a critical and processual understanding of pathways might contribute to a more informed appreciation of their potential (and their limitations) as mechanisms for healthcare policy implementation’. Although clinical care pathways do offer a structured approach to guide clinical practice, the human-centric nature of delivering healthcare services often includes informal and undocumented processes that vary from organisation to organisation. For example, Pinder et al. 36 assessed competing variations based on assumptions about clinical care pathways for patients with cataracts. As they explain, despite obvious differences, there are also important underlying similarities, particularly the tendency towards simplification and abstraction. Thus, gaining an understanding of clinical, patient and management insights can provide vital clues as to how clinical care pathways are executed in practice. Building on what Pinder et al. 36 explain as ‘what had started out as a one-size-fits-all model of professionally-delivered care turned out to be dependent for its success upon a complex (and unmapped) network of relatives, friends and informal carers in the community’, this may also open up new opportunities for pharmacy IS. Therefore, the benefits of examining clinical care pathways and identifying inefficiencies in pharmacy include the opportunity to improve patient safety, improve the quality of care and reduce costs associated with dispensing medicine. In addition, in Ireland, the dispersed network of pharmacists across the country is a national healthcare asset. Coupled with our research, this presents a significant opportunity to redesign our national pharmacy healthcare model.
In summary, our exploratory literature research suggests that, to improve clinical pharmacy services, we must first identify what are the enablers for improvement and how we can eliminate barriers to improvement. Therefore, with the current clinical focus on patient-centric care, we posit that, while clinical care pathways are important from a policy perspective, they should be socially dynamic rather than static management structures.
Pharmacists are striving to improve pharmacy services on a daily basis. Although they neither have the qualifications nor expertise, we observed many situations whereby pharmacists are attempting to solve process and IS problems rather than pharmacy problems. In addition, many of these efforts are in silos and not adopted on a national scale. The introduction of a national medicine management strategy would provide pharmacists with the benefit of networking with colleagues and would also support process improvements such as developments in IS, thus providing a universal terminology to cater for a multi-stakeholder interdisciplinary approach towards healthcare services. Historically, pharmacy leaders have led cost containment strategies, which alone have been insufficient to advance pharmacy practice. 37 Pharmacy leaders must demonstrate value by affecting patient outcomes across the continuum of care while exploiting pharmacy ISs to manage the internal supply chain associated with medicine management.
The development of efficient and effective pharmacy ISs requires the pharmacists’ involvement in the planning, design and implementation of such systems. The success of adopting pharmacy ISs on a national level requires a balance between leaders who are knowledgeable about both pharmacy practice and health informatics. This is key to allow healthcare organisations to understand where improvements can be made from both the clinical and operations perspectives.
Opportunities for pharmacy information systems
Our findings suggests that there is a need for pharmacy ISs. For example, central access to medicine machine to support the availability of medicine in wards would be beneficial especially for high-risk medicines which should be available 24/7 as needed, requiring the introduction of robotic technologies for dispensing medicines. Our research confirms that there is a need for such technology to facilitate greater flexibility, with a need for more central access for high-risk drugs. This leads to risk in the provision of care. In addition, as part of an existing medicine management strategy, drug storage fridges are used, which are wired up to monitoring services in the event of a power outage or failure. Alerts are also sent to mobile phones if there is a temperature drop in the fridges. However, there may be a waste of resources when storing drugs, as a ‘just-in-case’ management approach rather than a ‘just-in-time’ system is adopted. Thus, there is a need to investigate whether new methods can improve the cost-benefit of inventory management and to examine the impact of new IS strategies such as ward-based medicine strategies. Designed to support pharmacists in achieving greater efficiency, reducing medication errors and providing documentation for regulatory compliance, these will extend the pharmacy system across hospitals. Central pharmacy systems can combine the power of pharmacy carousel systems and bar code packaging to automate the inventory ordering, receiving, stocking and picking processes. We learn that computerised provider order entry systems can facilitate pharmacists to allocate more time to clinical and administrative functions and increase the number of order actions processed per hour, thus enhancing workflow efficiency and productivity of the pharmacy department. 38 We also agree with Flynn and Stevenson 39 when they identify the need to move beyond department-level strategy to transform pharmacy practice. Instead, health system pharmacy leaders must explore opportunities for the implementation and use of pharmacy ISs for regional-, national- and international-scale analytics and IS initiatives.
The development of automated pharmacy processes would alleviate pressures on pharmacists and relocate them closer to the patient. Many existing pharmacy processes are manual, paper-based and laborious tasks that require numerous staff to check and sign-off on dispensed and/or returned drugs. These may have a knock-on impact on pharmacy performance, on other vital healthcare services and on patient satisfaction. One of the core problems appears to stem from assessing whether current pharmacy service can be dramatically improved. This may be due to the lack of clarity in purpose and feedback loops, , that is, staff do not know if and when they are performing satisfactorily (individually and as a team). We learned how demand on pharmacy often exceeds the flow capacity at different times of the day. The loss of flow capacity is often due to resource scheduling and highly variable productivity quotas among staff, for example, lack of pharmacy services availability during weekends. These factors motivate the need to examine how specific processes may be automated, for example, dispensary and quality control. Pharmacy IS solutions can ensure that the right medications are stocked in the right locations, and that security is maintained for controlled substances. A purposeful IS strategy for pharmacy should focus on transforming practice to improve care and exploit opportunities for more remote patient contact supported by new data sources. 39 This would suggest that IS is not the core challenge in pharmacy because such innovative solutions do exist. However, it raises critical questions regarding management strategy and pharmacy priority within the wider healthcare context.
Conclusion
In this article, we present an overview of the literature review. In addition, by undertaking three case studies in acute hospital pharmacy, we examined enablers to hospital pharmacy service processes and identified barriers that prevent acute hospital pharmacy service improvements. We explain how pharmacy IS solutions may address the problems associated with pharmacy mismanagement and inefficiencies. We also discuss how both pharmacy informatics and pharmacy IS innovation can generate improvements in pharmacy service operations and management. Thus, we have identified that there is a compelling rationale for pharmacists to re-examine clinical care pathways and identify service inefficiencies. The immediate benefits of doing so includes the opportunity to improve patient safety, improve the quality of care, reduce costs associated with dispensing medicine and encourage the adoption of a lean pharmacy service system. Thus, the pharmacist can establish a common understanding and vocabulary to drive action, improvement or change within a hospital pharmacy context.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.