
Abstract
Telemonitoring leverages technology for the follow-up of patients with heart failure. Limited evidence exists on how telemonitoring influences senior patients’ attitudes and self-care practices. This study examines telemonitoring impacts on patient empowerment and self-care, and explores adoption factors among senior patients. A longitudinal study design was used, involving three surveys of elderly with chronic heart failure (n = 23) 1 week, 3 months, and 6 months after beginning telemonitoring use. Self-care, patient empowerment, and adoption factors were assessed using existing scales. The patients involved in this study perceived value of using telemonitoring, did not expect it to be difficult to use, and did not encounter adoption barriers. There was a significant improvement in patients’ confidence in their ability to evaluate their symptoms, address them, and evaluate the effectiveness of the measures taken to address these symptoms. Yet, patients performed less self-care maintenance activities, and the capability of involvement in the decision-making related to their condition decreased. Telemonitoring can improve seniors’ confidence in evaluating and addressing their symptoms in relation to heart failure. This patient management approach should be coupled with targeted education geared toward self-maintenance and self-management practices.
Introduction
Population aging represents a worldwide phenomenon marked by an increasing proportion of people aged over 60 years, which is expected to triple by 2050.1,2 The decreasing potential support ratios (i.e. number of 15–64 year per one person 65+ years), 2 and increasing prevalence of chronic diseases, further complicates the situation and create a social and economic burden on patients and societies.3,4 Heart failure (HF) is a life-threatening chronic condition characterizing the final stage of most types of heart disease. It affects 23 million people worldwide, including more than 5.8 million Americans, 5 with a high prevalence among elderly, who account for 80 percent of HF-related hospitalizations and 90 percent of associated deaths. 6 HF management programs emphasize the role of structured follow-up, patient education, and symptom monitoring in improving patient outcomes and preventing exacerbations and costly hospitalizations. 7 And the Canadian Cardiovascular Society recommends multidisciplinary Disease Management Programs, including HF clinics, home care, and telemonitoring (TM) to address this condition. 8
TM represents remote, non-invasive patient monitoring 9 that employs telecommunication tools to transmit physiological data from a home setting to a health center for follow-up and treatment. 10 It supports effective patient management 11 and allows early detection of deterioration in a patient’s condition and timely interventions. TM may benefit a broad range of patients,11–13 particularly elderly patients, and it has been associated with reduced risk of suffering from HF, and lower costs and hospitalizations. 14 In an overview of systematic reviews on TM and HF, Kitsiou et al. 10 recommended assessing TM processes, comparing effectiveness among different patient groups, and identifying optimal strategies for its success. This is important given the variation in TM compliance 15 and the particular needs of elderly patients that may influence their TM use. 16
Prior TM research mostly focused on TM impacts on symptoms, mortality, and services utilization.10,17,18 Yet, no previous research has fully explored the adoption factors related to TM by senior patients and limited evidence exists on its effects on patients’ behaviors, in relation to empowerment and self-care, which is particularly relevant for elderly HF patients who often face self-care challenges. 19
Patient empowerment and self-care are important concepts for global healthcare policies.20,21 Patient empowerment manifests itself in patients successfully regaining control over their condition22,23 and indicates their ability to cope with an illness and self-efficacy in managing it. 22 Self-care is a decision-making process involving a choice of behaviors that maintain physical stability (“self-maintenance”) and respond to emerging symptoms (“self-care management”). 24 Previous TM studies have discussed self-care, 25 but except for a few exploratory studies,26,27 TM’s effect on self-care behavior is limited. Radhakrishnan and Jacelon 25 conducted a literature review of telehealth’s impact on HF patients’ self-management and called for studies with improved designs to examine its effect on self-care outcomes. 25
In addition, very few studies in the literature have investigated TM adoption by elderly patients with chronic conditions. 16 A survey of chronic patients by Peeters et al. 28 showed that perceived characteristics have a significant effect on system adoption and observed that telehomecare acceptance is higher when the patient lives alone and with fixed daily contacts with the telecare system. Van Offenbeek et al. 29 used qualitative case data and found ambivalent patients’ reactions toward telehomecare solutions.
In an attempt to unify prior literature on information technology (IT) adoption, Venkatesh et al. 30 developed the Unified Theory of Acceptance and Use of Technology (UTAUT) model consisting of four constructs related to individual IT adoption: (1) performance expectancy (perceived usefulness), (2) effort expectancy (perceived ease of use), (3) social influence (people important to users think the system should be used), and (4) facilitating conditions (= IT infrastructures to support system use). Only two previous studies have used UTAUT to gain insight into older adults’ intention to use e-health solutions 31 and mobile phones in general; 32 however, they did not focus on a particular IT-based solution such as TM.
This study addresses these areas and investigates how TM works for senior patients with chronic HF. Specifically, it explores the factors that affect its adoption by elderly patients (at home and in retirement homes (RHs)) and examines the impacts of TM on empowerment and self-care.
Methods
Study design
A longitudinal study was conducted, involving a triangulation of data sources including three rounds of surveys; vital signs transmission from patients’ residences to a central TM station at a local hospital; outcomes data on health services utilization. While TM has been conventionally investigated in the context of patients living within their homes, this study is the first to also include patients residing in RHs. RHs are flexible residences for independent seniors who desire an environment enabling interaction with people of their age. They simulate a home environment, where each individual enjoys privacy and usually lives in a separate suite, 33 but they also provide services that increase residents’ comfort (e.g. housekeeping, meals, transportation).
Overview of the technology
The University of Ottawa Heart Institute (UOHI) has a well-established TM program. All patients with a discharge diagnosis of congestive HF are automatically referred to the TM program. An advanced practice nurse reviews the referral against standardized acceptance criteria, and each patient is then either placed in the TM or automated calling program based on their clinical needs and ability to use the technology. The TM system consists of a user-friendly monitor connected to a cellular or telephone line. It supports daily data transmission from standardized peripherals (e.g. weigh scales, blood pressure cuffs, and ECGs) through direct download and is programmed to ask common yes/no questions that patients have regarding their care (i.e. medication concerns, symptoms, changes in weight). The data transmitted by the patients are received at a central TM station at the UOHI and reviewed by a nurse expert who does the follow-up with the patient as needed. The interventions are standardized protocols for the program, which can vary from education to titrating medications based on patient need.
Survey instrument and data sources
In order to capture and understand the elderly patients’ attitudes, which may account for the differential effectiveness and TM success, we assessed patient empowerment and self-care at three points in time using existing measures.
The Self-Care of Heart Failure Index 24 was used to measure self-care (self-care maintenance and self-care management). Self-care maintenance was assessed by five questions measuring the frequency of the patients performing certain activities (e.g. eating a low salt diet, participating in a physical activity) on a 1–4 scale. Self-care management was assessed using 12 questions, which varied in nature (e.g. likelihood of recognizing symptoms, likelihood of confidence in recognizing and addressing symptoms), and were mostly measured on a 1–4 scale (1 = not likely and 4 = very likely).Two questions related to the speed of symptom recognition and certainty that the remedies helped were measured on a 0–4 scale.
The patient Empowerment Scale 22 was adapted for the purpose of this study. Eight questions were included in the surveys that assessed patient empowerment (e.g. feeling involved in the decision-making process, capability to make decisions related to their condition) using a 1–7 scale (1 = strongly disagree and 7 = strongly agree).
Factors related to TM adoption were also explored using existing validated scales 30 (based on the UTAUT model), which were adapted to fit the context of this study: performance expectancy (3 items), effort expectancy (3 items), social influence (3 items), facilitating conditions (3 items), and behavioral intention to use the system (3 items). All questions related to the adoption factors were measured on a 1–7 scale (1 = strongly disagree and 7 = strongly agree). Health consciousness was assessed at baseline using four items on a 1–5 scale (1 = strongly disagree and 5 = strongly agree) adapted from Jayanti and Burns. 34 Data on services utilization (e.g. emergency visits) were captured at the TM unit at the UOHI.
Sampling
Over a 6-month period, the nurse expert, who usually initiates the technology with the HF patients, introduced this research to them and discussed the procedures above and beyond the TM process (i.e. completion of the surveys related to this study). Twenty-three patients were recruited for this study, with careful attention to identify elderly patients with HF who demonstrated physical and mental capability to participate. Recruitment considerations included dexterity, fall risk, mental health, and so on. We also included patients living in RHs due to limited research on the use of TM in this environment.
The patients included in this study received the usual standard of care, following their discharge with congestive HF, as per their placement in the TM program. The only difference in this research is the administration of the survey tools to the patients. Each home-based patient was given a monitor for daily data transmission. For patients residing in RHs, a central station was installed in the common area of the RH. Each patient had a unique swipe card to use for data transmission. An early demonstration of how the system works was performed to ensure that patients were capable and informed on system use. Informed consent was obtained from all patients and ethics approval was granted from two institutional review boards: the Ottawa Heart Institute Research Ethics Board and the University of Ottawa Research Ethics Board.
Data collection
Data collection was performed through self-administered surveys. The questionnaires were developed with attention to the layout and presentation of the questions (e.g. large font, ease of read, good spacing). Three questionnaires were mailed out to the patients at different points in time (Table 1): T0 (1 week after system use), T3 (3 months after system use), and T6 (6 months after first day of system use). Upon completing the questionnaires, the patients mailed the completed surveys back to the UOHI (TM unit) using stamped return envelopes. Data assessing TM adoption factors were collected at T0 and T3; 19 and 20 patients completed the surveys, respectively. Patients’ characteristics and services utilization data were obtained for all 23 study participants. Data on patient empowerment and self-care were assessed at T0, T3, and T6. Out of 23 patients, 17 (74%) completed both T0 and T3 surveys, and 11 (48%) completed both T3 and T6 surveys.
Survey constructs and data collection rounds.
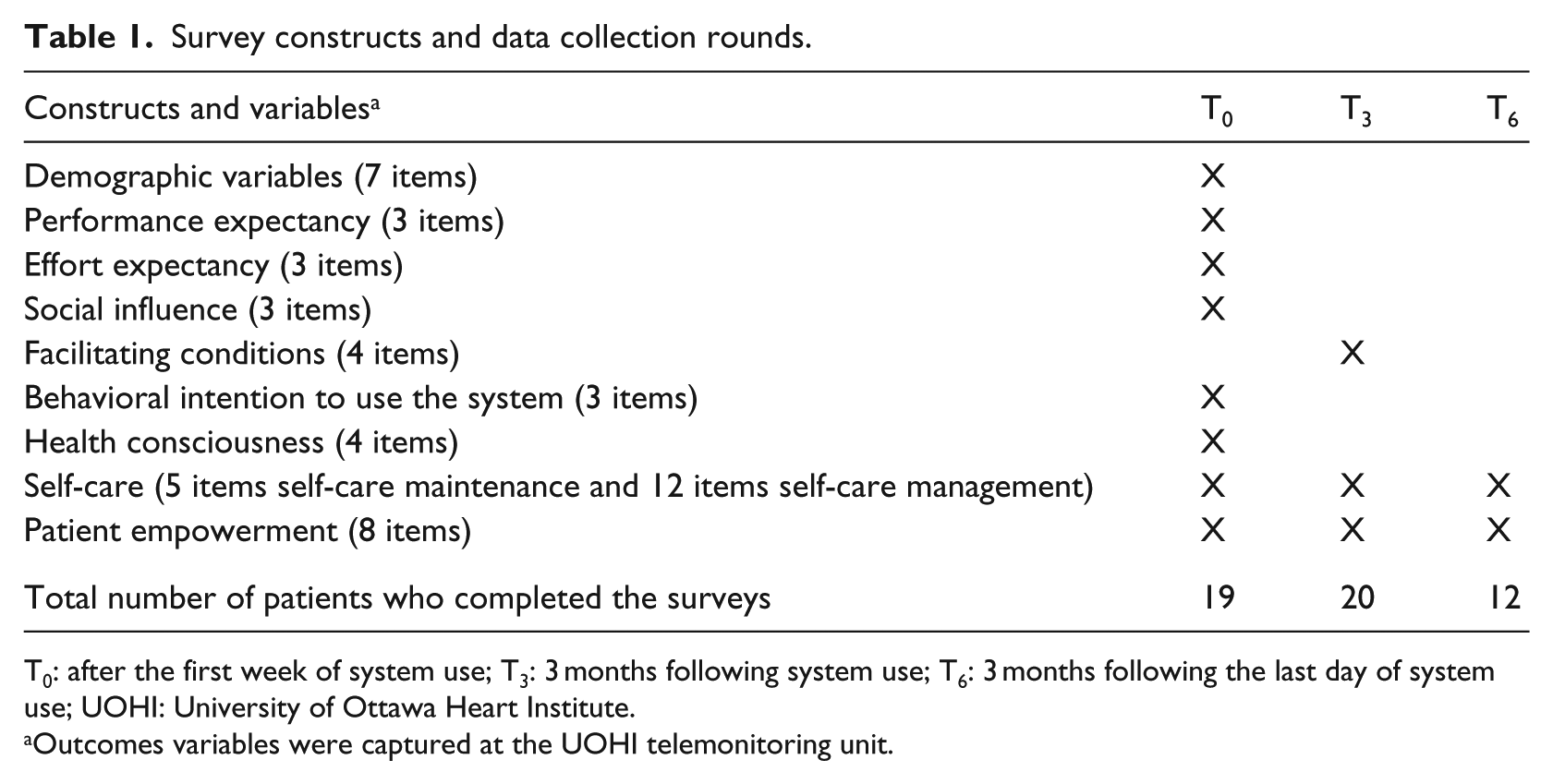
T0: after the first week of system use; T3: 3 months following system use; T6: 3 months following the last day of system use; UOHI: University of Ottawa Heart Institute.
Outcomes variables were captured at the UOHI telemonitoring unit.
Data analysis
Descriptive data analysis was performed to present an overview of patients’ characteristics, outcomes, attitudes, and contextual factors and to explore patient empowerment and self-care levels in the sample. The non-parametric Wilcoxon signed-rank test (i.e. rank sum test) was used to assess significant changes in patient empowerment and self-care over time.
Results
Sample characteristics and TM outcomes
The sample consisted of 5 RH patients and 18 patients residing in their own homes. The mean age was 75.2 years, most patients were married men, and the highest degree of education was high school/college (Table 2). The majority had chronic HF as a primary diagnosis and reported multiple comorbidities, mostly diabetes, and other non-cardiovascular diseases.
General patients’ characteristics.
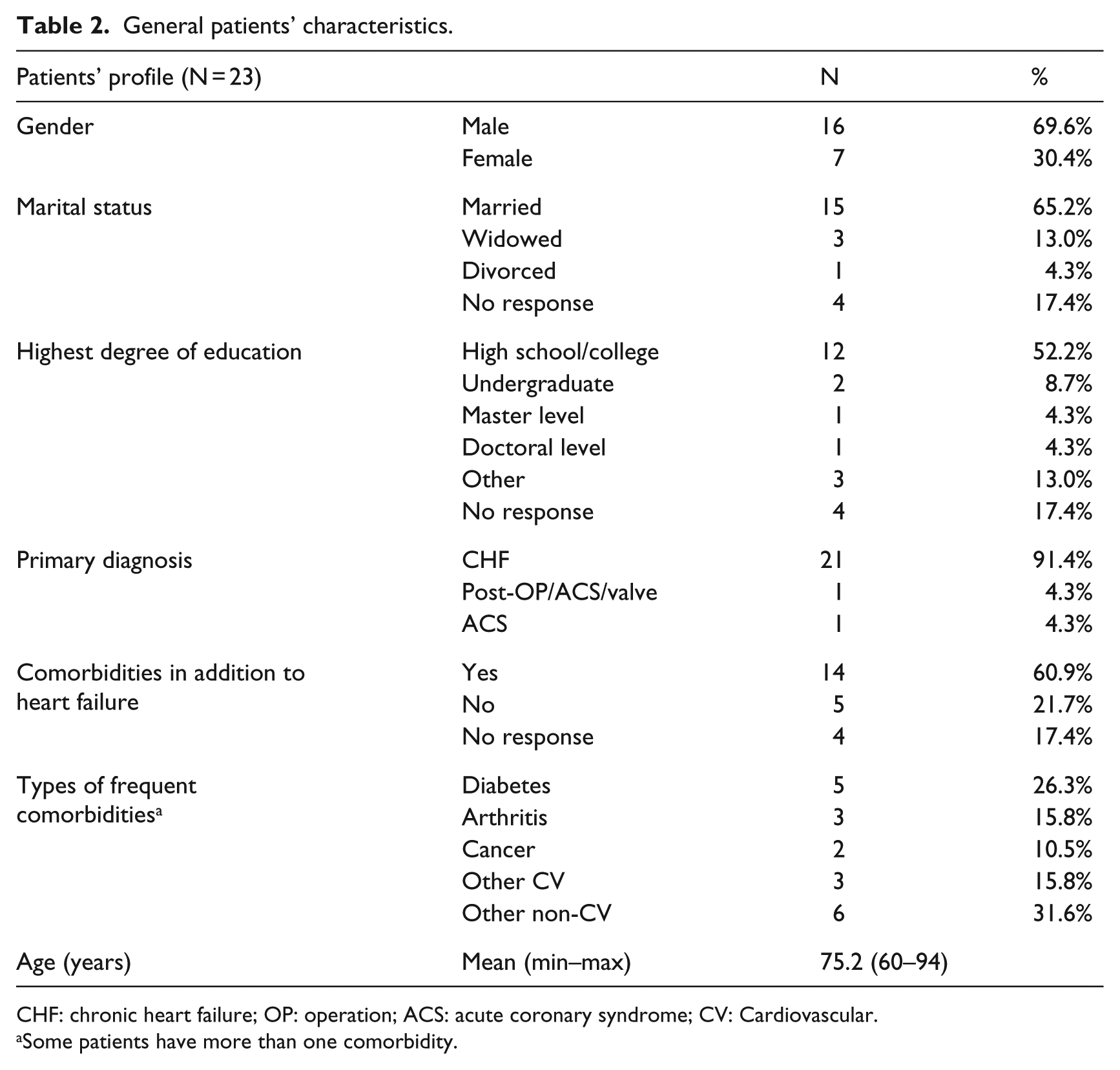
CHF: chronic heart failure; OP: operation; ACS: acute coronary syndrome; CV: Cardiovascular.
Some patients have more than one comorbidity.
The number of physician calls (mean = 0.7), emergency room visits (mean = 0.3), and hospital admissions (mean = 0.7) was relatively small and comparable between patients living at home and in RHs (Table 3). The number of HF medications adjustments, based on best practices, and diuretics adjustments were also comparable (mean = 1.4 for medications and 3.1 for diuretics).
Overview of telemonitoring outcomes.
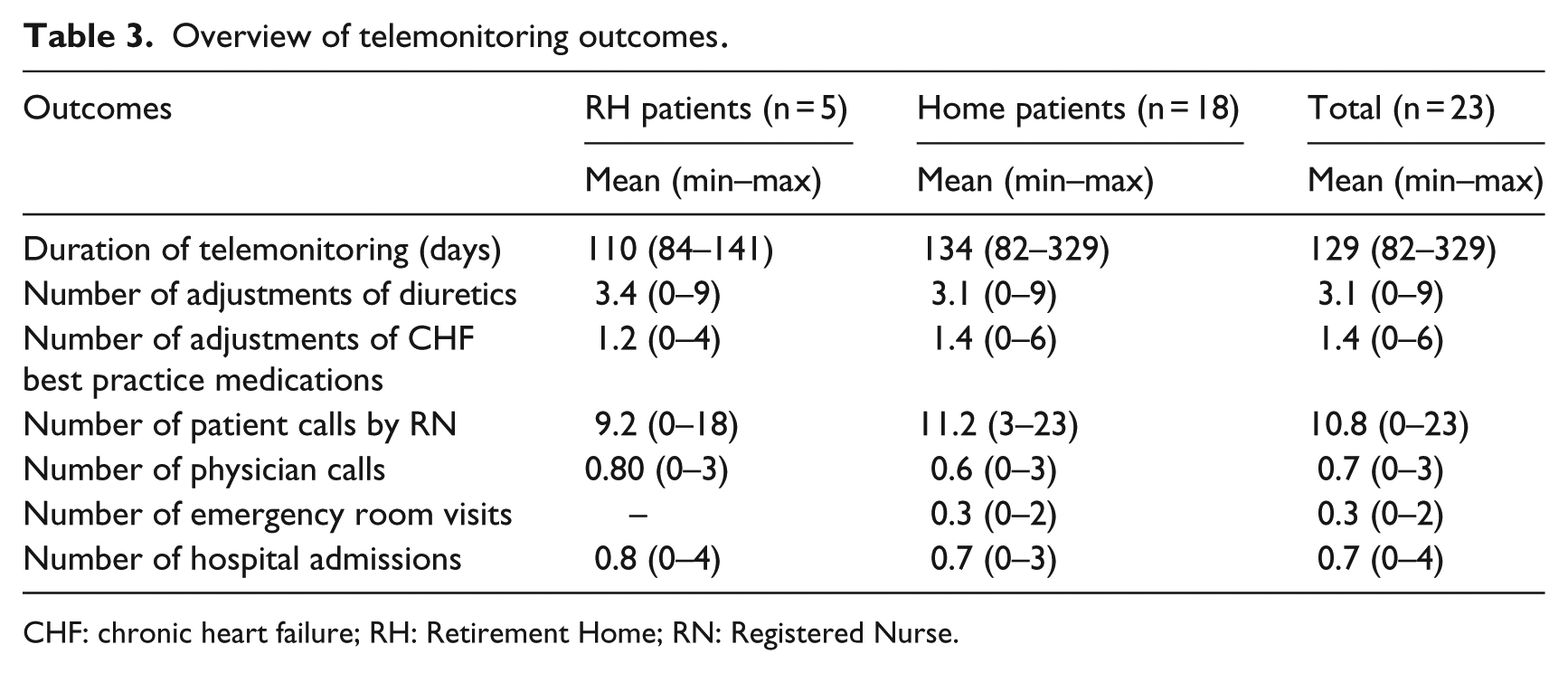
CHF: chronic heart failure; RH: Retirement Home; RN: Registered Nurse.
Adoption factors and health consciousness
On a 7-point scale, the 19 patients who completed the T0 survey perceived that TM would help them manage their condition (median = 6), monitor it (median = 6), and stabilize it (median = 5). They expected the system to be easy to learn and use (median = 7 for all three questions). They indicated that the people around them were supportive of this technology, and their intention to use TM over the next 3 months was very high (median = 7). Patients indicated some concern about their health conditions and high interest in getting information about their health and the management of HF (median = 4 and 5, respectively).
Twenty patients completed the survey at T3 (Table 4) and indicated that training was sufficient and the technology set-up in their residence was convenient. Technical support was also available (median = 7), and the patients indicated that people around them (e.g., friends, peers, nurses) assisted them in using the technology appropriately (median=7).
Behavioral/contextual factors related to TM adoption among elderly patients with HF.
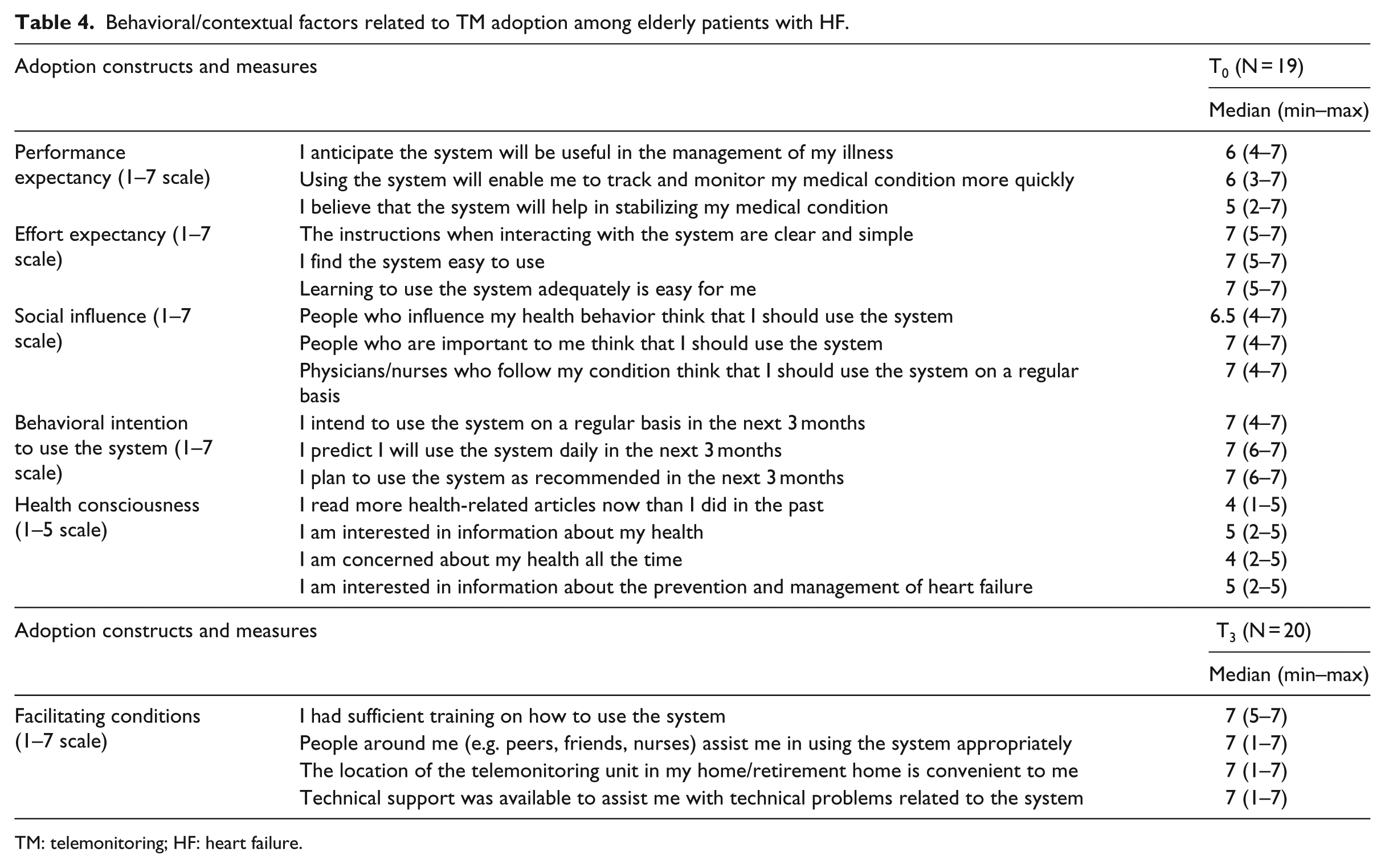
TM: telemonitoring; HF: heart failure.
Patient empowerment and self-care
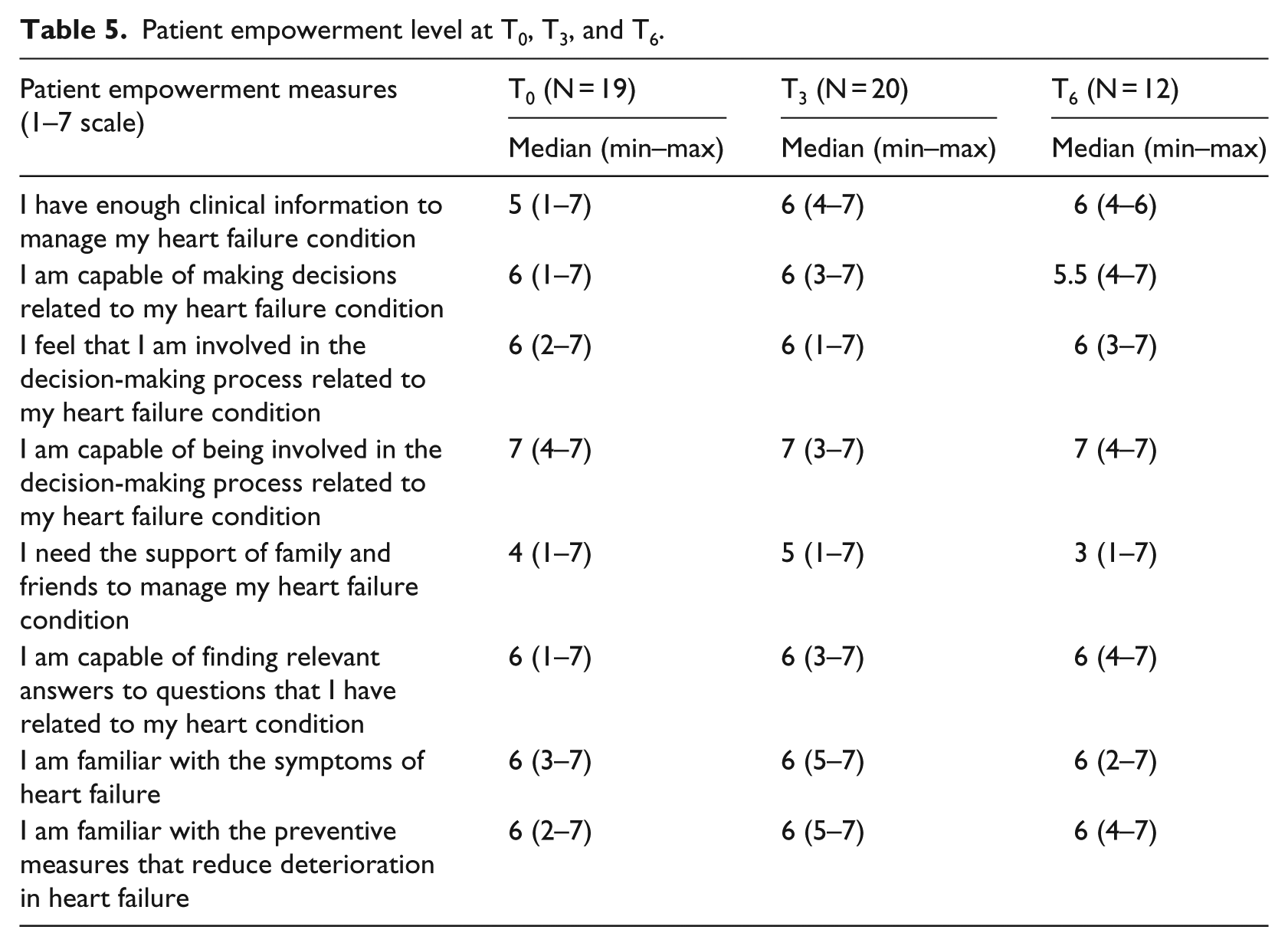
Overall, patient empowerment was moderate-high at all three points in time (Table 5). There was a slight increase in patient empowerment in relation to having enough information to manage one’s HF condition 3 months after using TM; yet this increase was not sustained over time. In addition, a decrease in the need for the support of family and friends in the management of one’s condition was observed and sustained at T3 and T6. Surprisingly, the Wilcoxon signed-rank test showed a statistically significant decrease in seniors’ perceived capability to be involved in the decision-making related to their HF condition at T3, 3 months after using the technology (Table 6).
Patient empowerment level at T0, T3, and T6.
Wilcoxon signed-rank test for significant differences in patient empowerment at T0, T3, and T6.
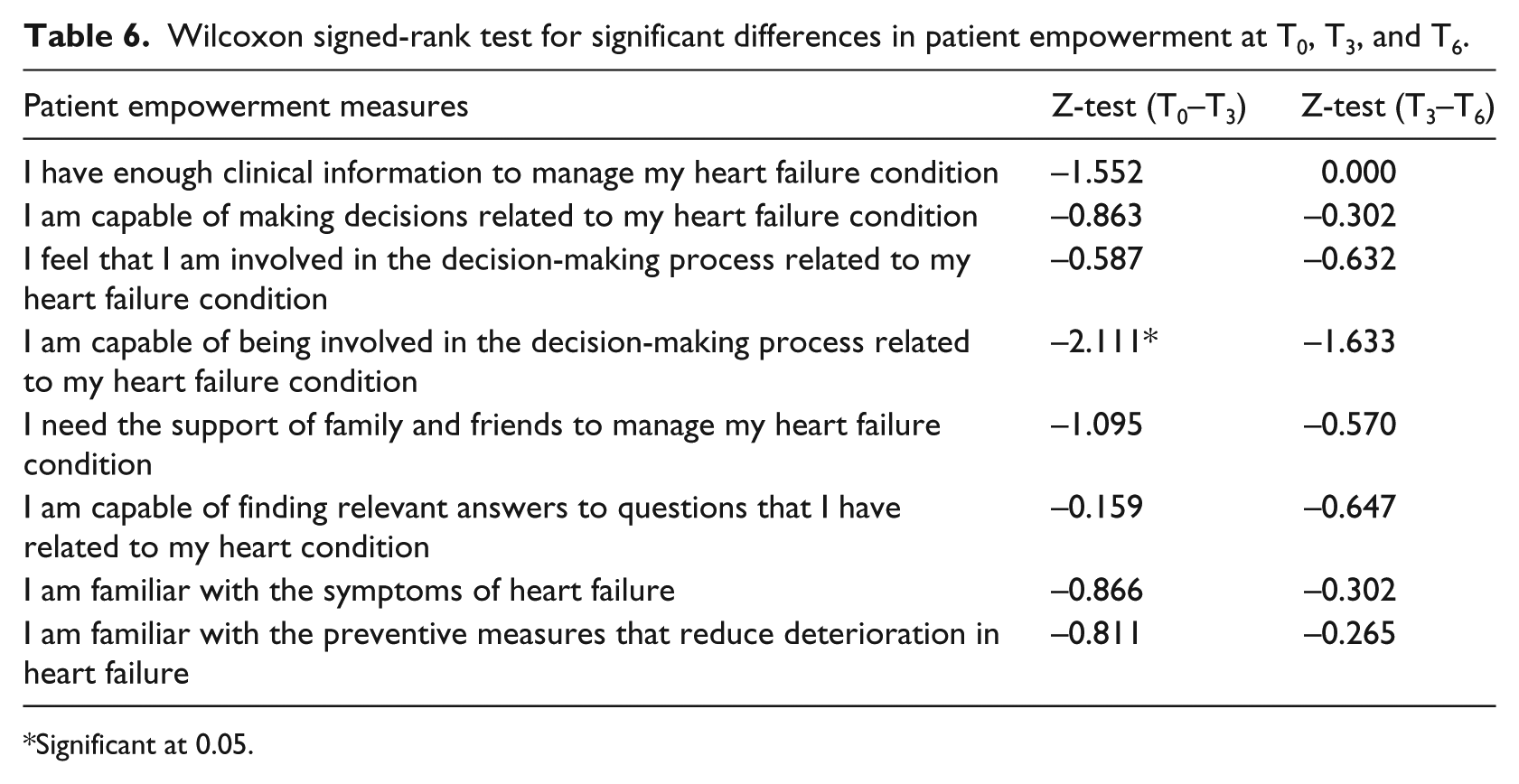
Significant at 0.05.
Patients reported relatively high frequency for the five self-care maintenance measures at T0, T3, and T6, despite a decreasing trend over time for one measure (Table 7). Interestingly, weighing oneself daily was the only self-maintenance measure that showed a statistically significant decrease in frequency over time at both T3 and T6 (Table 8). For self-care management, the incidence of trouble breathing and ankle swelling decreased over time at T3 and T6, which is indicative of symptom control and reduced exacerbations. The surveyed patients in this study also reported overall high scores on all self-care measures except on questions related to timely recognition of trouble breathing and ankle swelling as HF symptoms; reducing fluid intake or calling a doctor or nurse for guidance when these symptoms arise; and confidence that a used remedy actually helped. This was especially observed at T6. A trend of higher scores on some self-management indicators was observed at T3 as compared to T0 and T6; yet, this improvement in self-care management measures was not sustained over time.
Self-care level at T0, T3, and T6.
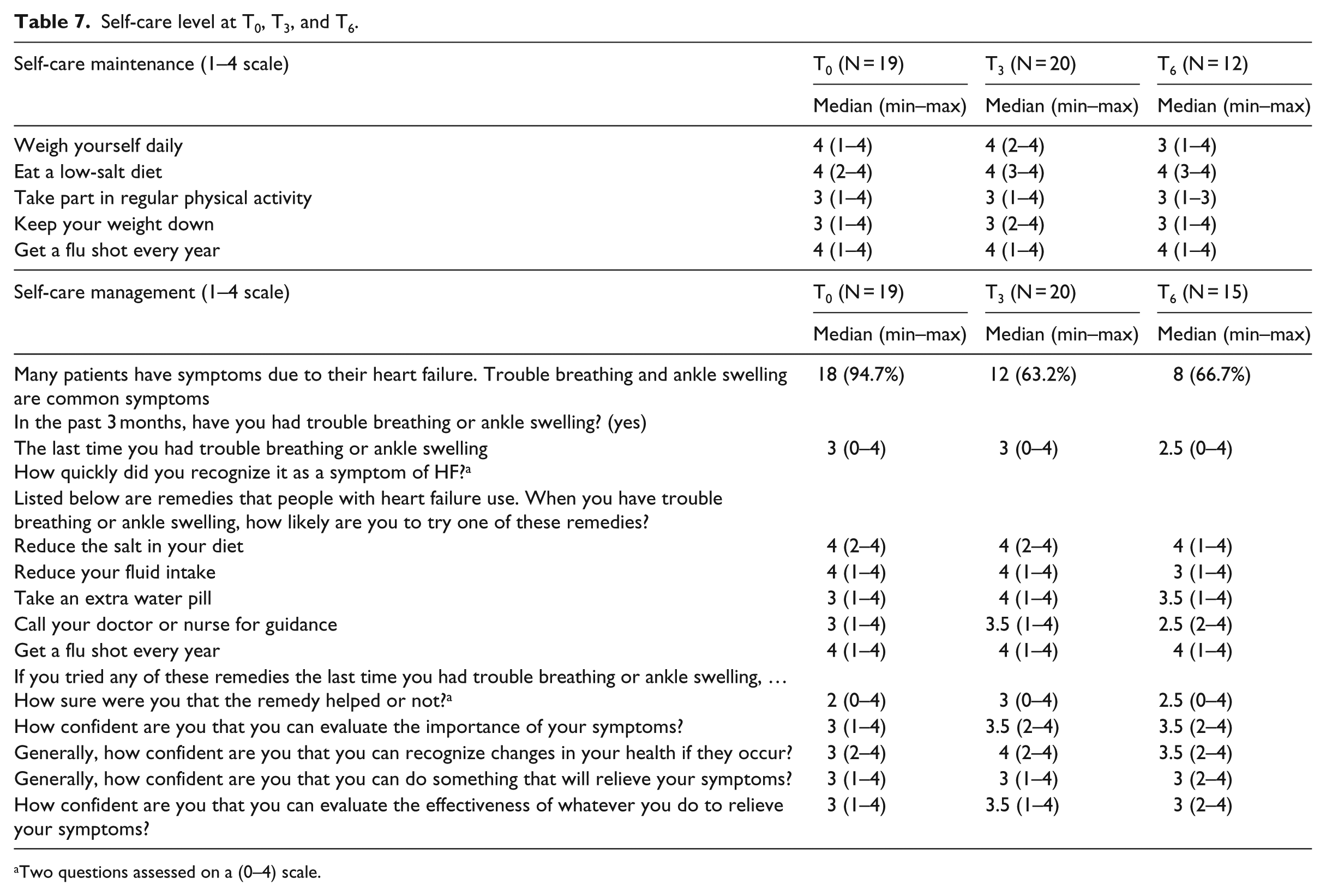
Two questions assessed on a (0–4) scale.
Wilcoxon signed-rank test for significant differences in self-care at T0, T3, and T6.
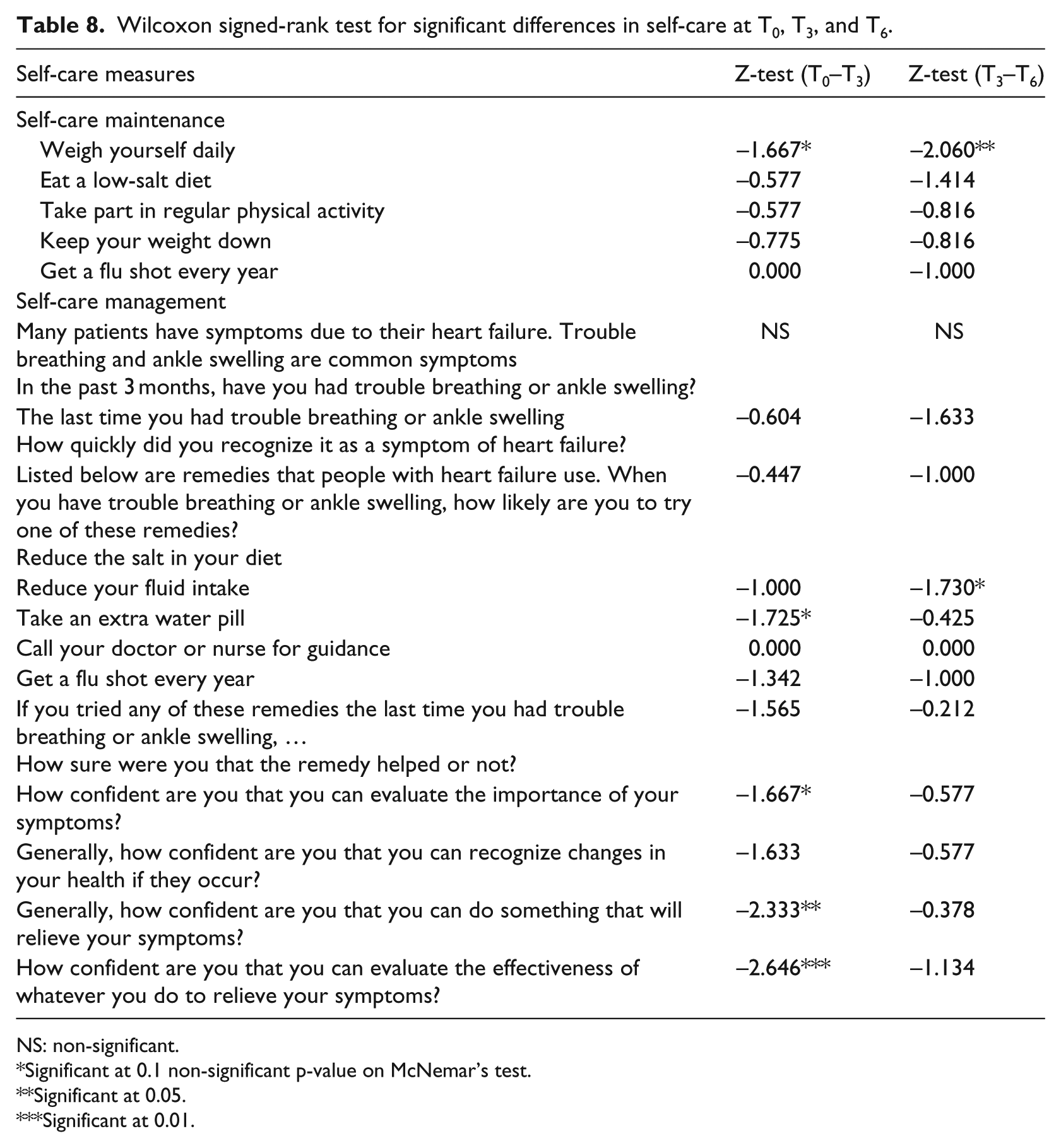
NS: non-significant.
Significant at 0.1 non-significant p-value on McNemar’s test.
Significant at 0.05.
Significant at 0.01.
The paired Wilcoxon rank sum test analysis revealed a statistically significant change on five self-care management measures (Table 8). The likelihood of trying an extra water pill as a remedy when having trouble breathing or ankle swelling, which was relatively low at the beginning of the study, significantly increased in the first period after TM started (T3). In addition, of utmost importance, a statistically significant increase in patients’ confidence in their ability to evaluate the importance of their symptoms, to take measures to relieve these symptoms, and to evaluate the effectiveness of such measures was consistently observed at T3. Finally, one surprising finding was related to the likelihood of reducing fluid intake when having trouble breathing and ankle swelling, which was statistically lower at T6 compared to T3.
Discussion
HF patients often experience quick deterioration in their condition accompanied by weight increase and symptoms lasting days before they seek care. 35 They are often readmitted to a hospital within 3–6 months after their discharge due to poor self-care and inability to detect early signs of deterioration. 36
Previous research on IT adoption by the elderly has mostly focused on the pre-implementation stage with limited available quantitative research post-implementation. 37 In a systematic review on the factors that affect the acceptance of technology for aging in place, Peek et al. 37 called for quantitative research involving technology for chronic disease management, especially in the post-implementation stage, and leveraging existing theories on technology use. In addition, limited research has been conducted on the facilitators/barriers for the adoption of telehealth by older patients 38 and the process by which it works to improve outcomes is also not well understood. This study, although limited by the small sample size, contributes to this area of research by leveraging existing models and scales to assess the adoption factors related to TM by elderly patients with chronic HF. It is the first to include patients living in RHs, who demonstrated similar pattern of adoption factors and services utilization as patients residing in their homes. Despite the small sample size included in this study, the longitudinal design, triangulation of data sources (i.e. survey on adoption factors, data extraction from patients’ records, three waves of survey of patient empowerment and self-care), and in-depth analysis allowed a comprehensive evaluation that contributes to this under-researched area.
Overall, our findings revealed that senior HF patients considered in this study perceived value in using TM and did not expect this technology to be difficult to use. The social influence of people close to them was positive and their intention to use TM was high, which was further enabled by supportive facilitating conditions. This is in line with the findings by De Veer et al., 31 who assessed the determinants of intention to use E-Health in general by older people and found that the majority perceived it easy to use and learn. 31 Interestingly, the participants reported lower levels of perceived usefulness at the beginning of the study, compared to ease of use and social influence, possibly reflecting a limited upfront knowledge about the ways TM can support the management of their condition.
Moderate to high levels of patient empowerment were. Surprisingly, patients’ capability to be involved in the decision-making process related to their HF condition significantly decreased at T3, although the reported feeling of involvement remained relatively high. This may be attributed to TM’s structured approach in monitoring symptoms and addressing them based on best practices and available guidelines. This may limit the patients’ perception of their involvement in decision-making.
In general, TM did not improve the frequency of self-care maintenance measures, which are indicative of behaviors necessary to maintain physical stability. A statistically significant decrease in patients’ weighing themselves daily was observed at T3 and T6. It is not clear as to whether or not there is a risk of patients relying on TM and acquiring a passive behavior toward monitoring their weight, which may persist with them over time. Alternatively, as a patient’s condition improves, there may be less attention to weight changes. This finding suggests that TM programs should continue to incorporate educational interventions to increase awareness among patients on the importance of weighing themselves to identify early HF deterioration.
High levels of self-care management after TM use were observed, except on three important measures. First, timely recognition of breathing difficulty and ankle swelling as HF symptoms was moderate, which stresses the value of TM in following-up these patients for timely detection of deterioration that may otherwise go unnoticed. Second, senior patients were not very likely to take an extra water pill when these symptoms appear, nor call a doctor or nurse for guidance. This further indicates the importance of connecting them with a provider before their condition worsens necessitating an emergency visit or hospital admission. Third, participants lacked confidence on the helpfulness of remedies. Therefore, we posit that a targeted patient education model focusing on these three areas might improve senior patients’ self-care.
The consistent impact of TM on self-care management was observed in relation to increased seniors’ confidence in their self-care ability. This is in line with recent studies that showed that the use of TM can educate patients and enhance their self-care skills.26,27 Specifically, patients reported higher levels of confidence in evaluating their symptoms, acting to relieve these symptoms, and evaluating the effectiveness of their actions. This is particularly important for senior patients, as it presents opportunities for leveraging TM to manage them at home while improving their ability for their self-care. This also addresses prior concerns about HF patients’ misconceptions and lack of knowledge about how to deal with their condition, which may lead to improper self-care skills and lack of confidence in these skills. 39
It is important to note some of the challenges and limitations associated with this research. Given the clinical nature of the population included in the study (elderly, multiple comorbidities), some of the findings may not be generalizable to all HF patients. The majority of the sample consisted of married men, which may not be representative of the overall population given the prevalence of HF among men and women. The longitudinal nature of the research also led to attrition and a decrease in survey response over time. The absence of a control group usually present in randomized controlled trials, despite the prospective nature of the study, precludes firm conclusions as to the absence of changes at the patients’ individual level, which may have also contributed to the observed changes. The implementation of TM programs can be variable among different organizations; hence, it is important to consider program structures and processes when applying these findings. We recommend that future research in other contexts (e.g. different countries, different healthcare systems) conduct similar studies to build more solid evidence in this area. In addition, future studies should also leverage qualitative research approaches to better understand patients’ experience with this technology and address questions related to their perceptions of adoption barriers and facilitators.
It is worth noting that patients’ expectations of the TM system are expected to evolve over time. Yet, these expectations are not anticipated to be associated with changes related to patients’ ability to self-care, as the TM system is only considered as a tool for the management of patients and not an intervention in itself. Importantly, TM appeared as a “new concept,” which was unknown for a lot of the RHs that we contacted for installing the TM unit. With a growing elderly population in Canada, programs (e.g. at local colleges) should be developed to train and inform administrators and employees at RHs on available technologies such as TM that may be useful and beneficial for their clients. This is especially relevant given the recurrent emergency visits of seniors to hospitals within the geographic catchment area of these RHs. Future studies may build on these findings and consider multiple community dwelling sites with a potential larger number of seniors patients.
In conclusion, elderly patients considered in this study were capable of using TM for HF management with no reported barriers. TM had a significant positive effect on these senior patients’ confidence in their ability to evaluate their symptoms, address them, and evaluate the effectiveness of the measures they take in relation to HF. We recommend combining the conventional TM approach supported with targeted education geared toward the importance of self-maintenance and self-management practices (e.g. recognizing major HF decompensation symptoms, understanding how certain remedies work, and assessing if they worked effectively). This will support long-term sustainability of the benefits associated with this patient management approach, especially for seniors who may be at higher risk of deterioration in their HF condition if their condition is not appropriately managed. In conclusion, this study concurs with previous research, 16 which shows that while remote monitoring creates new possibilities for HF patients, its success will require substantial and continuous efforts from healthcare professionals and staff and careful consideration to differences between patients, especially elderly patients with particular needs.
Footnotes
Acknowledgements
The authors thank Christine Struthers (APN Chronic Cardiac Care, Ottawa Heart Institute) and Maureen Taylor-Greenly (VP Patient Services and CNO, Queensway Carleton Hospital) for their support in the planning for this project. The authors also thank the administrators and staff of the RHs who facilitated the process of data collection from the residents.
Compliance with ethical standards
Informed consent was obtained from all patients and ethics approval was granted from two institutional review boards: the Ottawa Heart Institute Research Ethics Board and the University of Ottawa Research Ethics Board.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by the Social Sciences and Humanities Research Council of Canada (#410-2010-1760). This work was previously presented at the 50th Hawaii International Conference on System Sciences, 2017.