
Abstract
The development of eHealth is dramatically changing the way healthcare is provided and organized. eHealth applications are used not only by healthcare professionals but also by patients specifically to self-manage their health condition. The development of eHealth applications requires a new methodological approach, departing from the more conventional methods dedicated to designing health information systems. There is a gap between theories to design persuasive eHealth applications and practices. In the Netherlands, eHealth innovation emerges from three areas. In research, the development of eHealth application often remains in a pilot phase. Healthcare organizations are also keen to innovate but do not always have the know-how. We further witness technology push from business and industry, undermining the co-creation process of the innovation. We consequently advocate an integrated, systematic and practical but scientifically based methodology to design effective persuasive eHealth applications. This approach is being successfully embedded in our educational health informatics program.
Introduction
Several factors in the Netherlands influence the development of persuasive self-health management systems, namely, a changing population, governmental policies and technological developments. The Dutch population is rapidly aging and has a rising prevalence of chronic conditions resulting in high costs of healthcare. 1 Both trends are intertwined and need to be addressed. The Dutch government actively encourages elderly people to stay at home longer rather than move to a retirement home. Furthermore, Dutch hospitals are looking for ways to diagnose and treat people closer to their homes by opening up small-scale local care centers. The idea is that care should increasingly take place at or near home and should be carried out by relatively inexpensive caregivers or by patients themselves. One of the main approaches to address this problem is a greater emphasis on self-management whereby patients have more responsibility and take over care actions from their providers. 2 Living with a chronic condition is for an important part lifestyle dependent, requiring patients to change their behavior, incorporate new routines in their daily life and to be motivated to do so. 3 Self-management as promoted by the Dutch government tends to create a new kind of patient: the do-it-yourself (DIY) patient who takes charge of their own health. This coincides with a change of focus from illness and care (of patients) to behavior (prevention) and health as laid down by the Dutch Council for Health and Care 4 and inspired by the new definition of health by Huber. 5
In this context, eHealth 6 already plays an important role to facilitate and catalyze self-management.7,8 The current situation regarding eHealth and its use for self-management in the Netherlands is described yearly in the eHealth Monitor. 9 eHealth provides a means to monitor patients at a distance, to consult a doctor online and/or to provide patient support. The Netherlands currently has approximately 85 broadband subscriptions per 100 habitants 1 and ranks 4th within the European Union (EU) as regards eHealth adoption.10,11 This puts the country in a good position to broadly stimulate the development and use of eHealth to provide more care services online and via apps. This may contribute to lowering the costs of care. In 2014, the Dutch Ministry of Health, Welfare and Sports formulated the following goals for 2020 12 to stimulate self-management behavior: (1) in 2020, 80 percent of chronically ill patients have online access to important parts of their medical record; (2) 75 percent of chronically ill patients and frail elderly people can carry out self-measurements, often monitored at a distance by a caregiver; and (3) everyone receiving care at home can communicate by video consult with a caregiver.
However, the use of self-management systems to support patients to change their behavior has to date lead to moderate success. 13 Patients report that they do not receive sufficient advice on using self-management systems, while their healthcare professionals think that they do. 9 Even though theoretical models to design the development of self-management are used, it remains rather ad hoc. Moreover, the complexity of communication that results from using these systems 14 and persuasive behavioral changes, for example, 15 remains a challenge in designing self-management systems. Furthermore, we witness a technology push from business and industry. This technology push often ignores the persuasive aspects undermining the co-creation process whereby patients are also co-developers of self-management systems. 16
The factors mentioned above create a gap between the theories used for development of self-management systems and a practical approach to help software developers and healthcare informatics professionals adopt evidence-based practices for support of an elderly population with chronic conditions. From an educational perspective, there are healthcare informatics educational programs available in the Netherlands although little attention is given to designing effective persuasive self-management applications. This article addresses this issue and proposes to bridge the gap between theory and practice through an integrated, systematic and practical but scientifically based methodology for design of effective persuasive self-management applications. Experience in embedding this integrated approach within our healthcare informatics programs of the University of Applied Sciences is also reported and discussed.
It should be emphasized that this article is a descriptive article, which gives an example application of the integrated approach. The article has two aims: to report on the integrated approach we have developed and how we have used it in our master program. These two aims are intertwined. The integrated approach has been developed from a didactic and educational perspective. It is hoped that this article will inspire educators on how to teach design of persuasive eHealth applications.
Material and methods
Selection of models for the integrated approach
Our motivation has been to develop an integrated approach, which is practical to use and scientifically based. eHealth solutions engage people in adapting their behavior without coercion. In this context, existing models of behavioral change and persuasive design technique are relevant. Application of these models to eHealth solutions provides the necessary sound foundations. The proposed integrated methodology makes use of existing models in the areas of eHealth development, persuasive design and behavioral change. These are, respectively, the CeHRes roadmap, the design features of Oinas-Kukkonen and the behavioral model of Fogg. From this perspective, our aim has not been to develop a new theory for designing eHealth self-management persuasive applications.
The CeHRes roadmap provides general guidelines on the steps to take in designing eHealth applications. It is up to the user of the roadmap to fill in the methods, which are found to be most appropriate for each phase. In our case, we make use of two models (see sections “Model of Oinas-Kukkonen” and “Model of Fogg”) in order to clarify aspects of behavior changes and persuasion important in designing dedicated eHealth applications.
CeHRes roadmap
The CeHRes roadmap 17 was developed by the University of Twente in The Netherlands (see Figure 1). It guides planning, coordination and execution of the participatory development process of eHealth. It takes a holistic research and development approach and consists of five main iterative phases. The first phase is contextual inquiry (CI) and focuses on understanding the targeted users and their context. The next is the Value Specification phase, where the users’ needs and wishes are translated into requirements. Based on the requirements, a prototype is developed (the design phase). During the operationalization phase, the eHealth application is implemented and put into practice. Finally, the eHealth application is assessed in the Summative Evaluation phase. At this point, an evaluation is made into how the eHealth application is used and its effect on patients and healthcare.
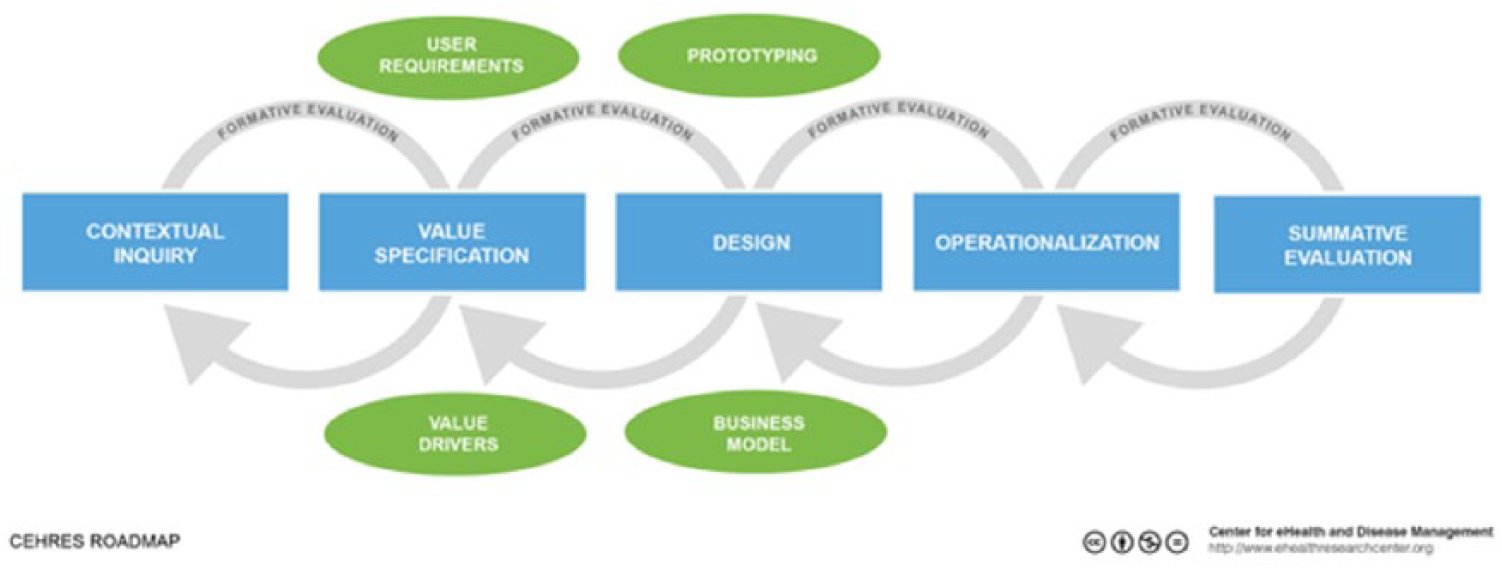
CeHRes roadmap.
The CeHRes roadmap has a number of advantages: first of all, it has the structure of an action plan with its various phases. Furthermore, there are no pre-required methodologies attached. Instead, it provides a certain flexibility in choosing which methods are most suited to the development of the eHealth application. For example, one may decide to use a focus group instead of an online questionnaire during the contextual enquiry phase.
The CeHRes roadmap is mostly used in academia for undertaking research projects. For example, the development of an eCoach for people with diabetes 18 or an eHealth intervention to help dementia patients stay at home longer. 19 As a teaching instrument, the roadmap is integrated in the bachelor and master educational programs of the University of Twente. In other Dutch universities and universities of applied sciences, it is to our knowledge scarcely if not taught at all.
Model of Oinas-Kukkonen
The model of Oinas-Kukkonen includes principles for persuasive design and describes the key issues behind them (see Figure 2). 20 The model allows defining the persuasive context, describing the targeted users, their goals, intentions and technology use. The model also defines a set of persuasive design features, which may be embodied in an eHealth application. Features include support to the primary task the user should accomplish, the dialogue with the user, the credibility of the application (e.g. the quality of information being conveyed) and social support related to reinforcing connectivity with the user.
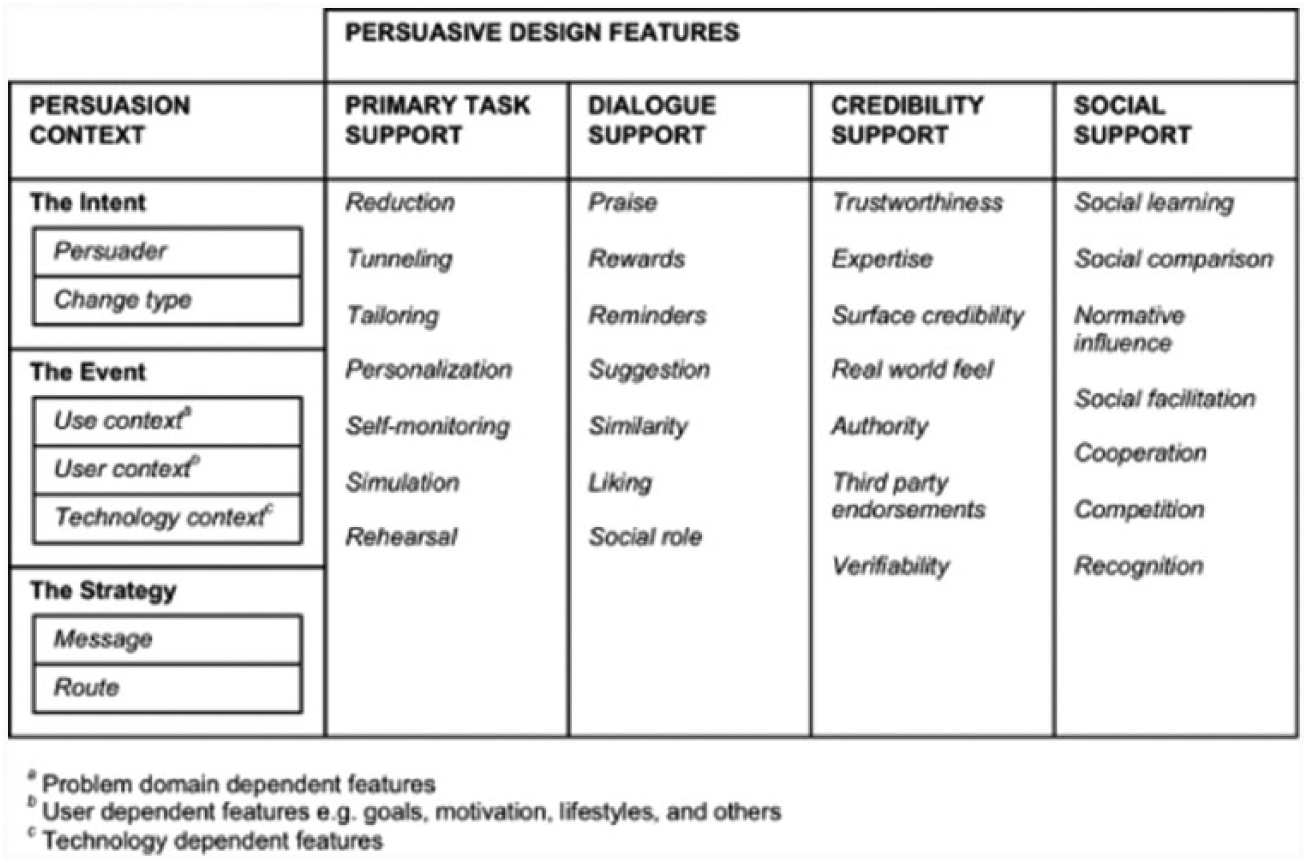
Model of Oinas-Kukkonen.
The model is relevant to the development of eHealth self-management systems. Studies such as Lehto and Oinas-Kukkonen 21 indicate that the primary task support is applied relatively widely for web-based self-management. The various components of the primary task support are used to various degrees. Self-monitoring is utilized more than tailoring, for example. Another study 22 shows that task support is also used for self-management via mobile apps and that system credibility ranked high as a persuasive feature.
Model of Fogg
The Fogg Behavior Model shows that three elements must converge at the same moment for a behavior to occur: motivation, ability and trigger (see Figure 3). When a behavior does not occur, at least one of those three elements is missing. The model is useful for understanding human behavior and to operationalize the factors related to it. In this sense, it is also applicable when designing persuasive technologies. 23
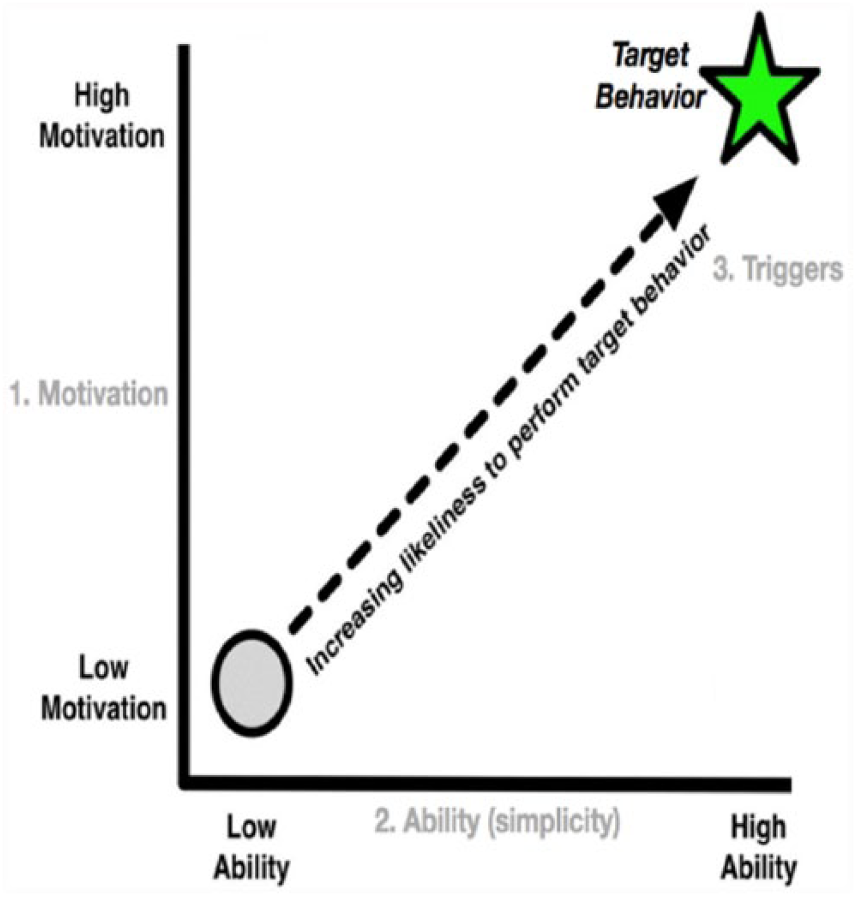
Behavior model of Fogg.
Core motivators include pleasure, joy and acceptance (their opposites are demotivators). Ability follows the power of simplicity principle. Simplicity factors may be influenced by (lack of) time and money or from requiring too much thinking among others. Behavioral triggers include elements such as facilitator and signal.
The model of Fogg is relevant when developing eHealth self-management systems since behavioral changes reside at the core of such systems. For example, it has been used to support the development of self-management promotion. 24 Another study has used the motivators from the Fogg model to design a self-management monitoring system for young patients with type 1 diabetes. 25
Integrated approach
The CeHRes roadmap is the starting point for the integrated approach. The roadmap provides the practical steps needed toward development of a persuasive eHealth self-management system. The models of Oinas-Kukkonen and of Fogg are included at various phases of the roadmap as explained below.
CI and persuasive context
The first step of the roadmap, namely, CI, makes use of the persuasive context from the model of Oinas-Kukkonen (see 1 in Figure 4). During the CI phase, an inventory of the stakeholders of the application is made. While not all stakeholders will use the application, it is important to identify them all in relation to the applications targeted users. The persuasive context helps to acquire a deep understanding of the targeted users. In particular, it includes the user, the use context, the technology context and the messages to be sent to the user. In this phase, these components are being used as a guideline for the stakeholder analysis defining the problems and needs of the targeted user. For example, problems the targeted user has may be linked to their technological context such as a limited access to a computer or low level of computer literacy. Similarly, the needs of the user are being addressed from point of view of the user’s context. For example, the user’s needs to take their blood pressure on a daily basis but with little motivation to do so. Knowing that the patient has little motivation will influence the way messages are being directed.
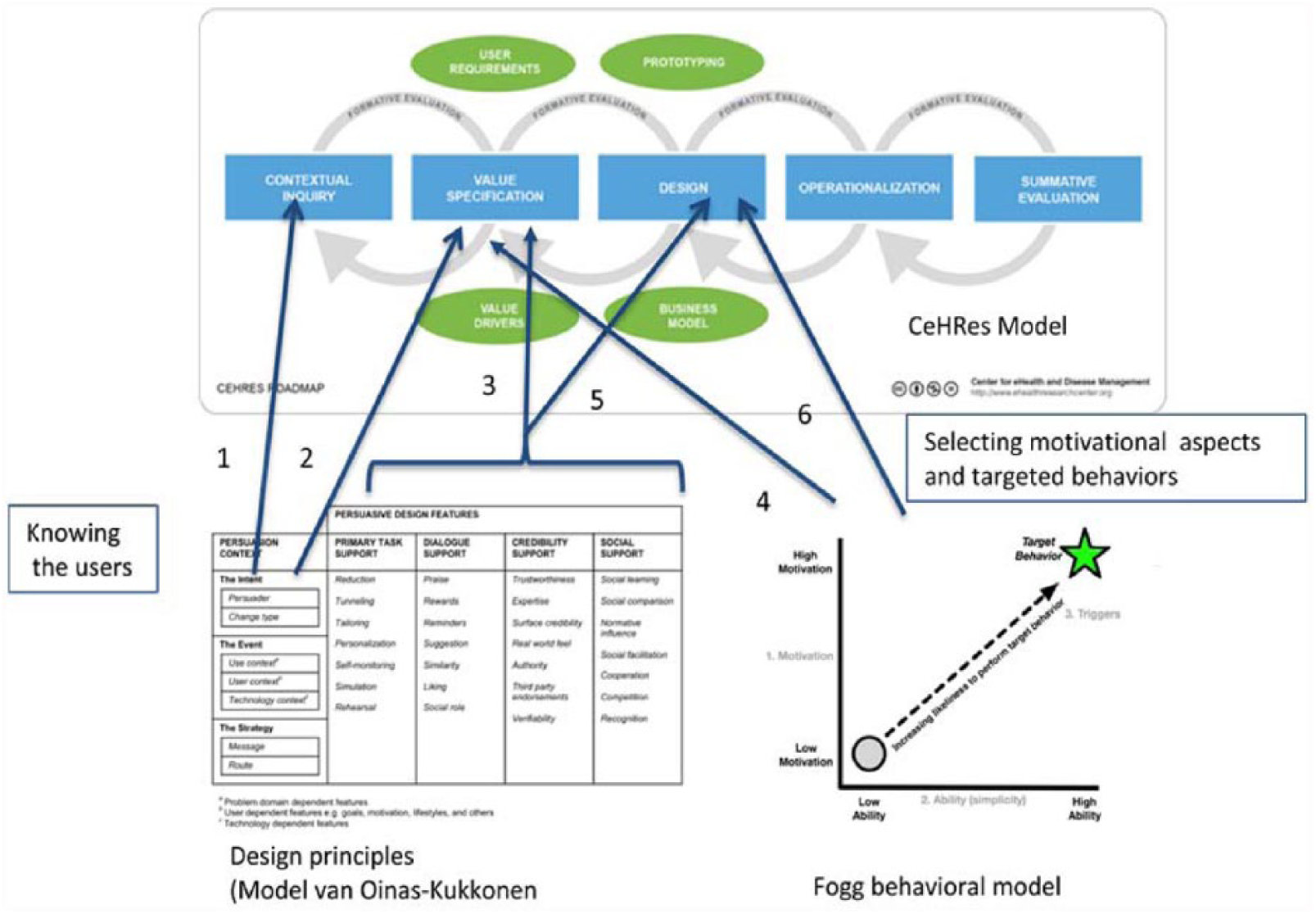
Integrated approach.
Value specification and persuasive context
The second phase of the roadmap involves defining personas, scenarios and requirements based on the results from the CI phase. The phase of value specification uses the persuasive context from the model of Oinas-Kukkonen (see 2 in Figure 4). Methods based on interaction design such as “About Face” 26 are used. “About Face” supports the process of interaction, goal-directed and user-centered design for describing the personas and for developing the scenarios of the user’s behaviors of the application. The personas and scenarios also include the user’s goals and how these can be achieved with the eHealth application. Each requirement to be defined is composed of an action, an object and a context. For example, “self-monitoring,” “blood pressure” and “daily at home.” The persuasive context in this phase serves as a guideline and ensures that the defined requirements take into account the technological dependent features of the context and provide a comprehensive overview of the requirements and factors involved. For example, the requirement “the application sends the patient a daily reminder to take his blood pressure” embeds a relevant technological context.
Value specification and behavioral change and persuasive design features
The behavioral model of Fogg is in phase 2 of the roadmap, pertinent to translating the user’s profile into behavioral variables, for instance, motivation and competencies (see 4 in Figure 4). In our given example, the ability to use a blood pressure monitor and the motivation to do so will be considered as two important behavioral aspects. These play a role in gaining insight into the design features, which may be suited for behavioral change (see 3 in Figure 4). For example, sending a reminder is a typical design feature to support user dialogue and is to be found in the model of Oinas-Kukkonen.
Design and persuasive design features and behavioral changes
Design of the eHealth application takes place in phase 3 of the roadmap. The model of Oinas-Kukkonen and the model of Fogg play a central role here in choosing the appropriate design features and targeted behavioral changes (see 5 and 6 in Figure 4). The elements of the persuasive context are providing an underlying structure for formalizing its primary user, the goal of the eHealth application, its context of use and the information to be conveyed. The persuasive design features serve as a checklist in order to assert (based on the information from the previous phase) which feature is best suitable. In our example, the task support features of self-monitoring and tailoring are good candidates. Dialogue support in the form of reminders is used to support addressing the therapy adherence of the user. With regard to the credibility design feature, non-biases and non-commercial-based advices on choosing blood pressure monitors make the eHealth application more trustworthy to the user. The social support feature in this example is not considered to align with the needs of the user and will not be included.
During the various phases of the roadmap, the user’s level of motivation and their ability to carry out a task have been identified. The behavior model provides the conditions under which the behavioral change is meant to occur. The behavioral grid (see Figure 5) is used in our integrated approach as a useful tool to pinpoint a suitable behavioral change. In our example, the user is already taking their blood pressure but not on a regular basis. From the grid, the targeted behavior change falls into the category “increase a behavior for a period of time.”
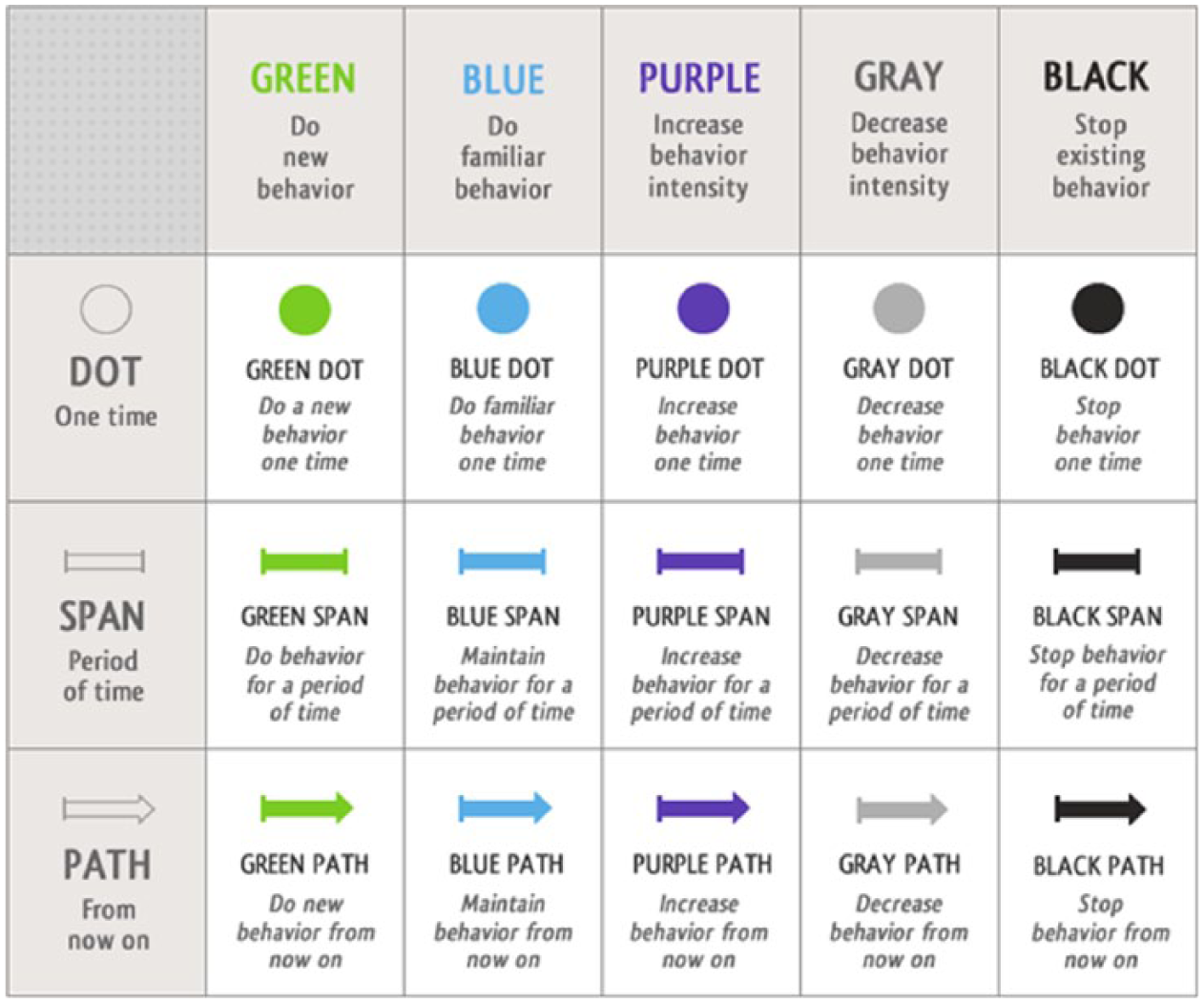
Behavior grid.
During this phase of the roadmap, the interface and interaction model are being constructed followed by development of a working prototype. These are driven from the selected persuasive context and persuasive design features. Required changes to these features elicited during formative evaluations means going back to the previous phase of the roadmap and determining feasibility and appropriateness.
Operationalization and evaluation
The phase of operationalization has to do with implementing the eHealth application in practice, for example, as part of an online intervention. This is followed by a summative evaluation. These phases close the iterative cycle of developing the eHealth application. The theoretical models of persuasive design and behavior changes are not required here.
Results
The master program advanced health informatics practice
The proposed integrated approach to design effective persuasive self-management applications is being used within our Master program “Advanced Health Informatics Practice” (MAHIP) at Inholland University of Applied Sciences. 27 MAHIP is a 2-year program targeted at professionals working in healthcare. The master program offers blended learning facilities: students attend the university every 2 weeks for a full day of lessons. For the rest of the time, they study at home and can use the online platform Moodle (https://moodle.org/) to access all information they need and to communicate with their fellow classmates and teachers. At the end of the master program, students become Healthcare Informatics Professionals (MSc). During the master program, the students learn to take an intermediary role in bridging the gap between healthcare and technology. Throughout their studies, the students learn different roles such as information and business analyst, system and solution designer, consultant, implementation specialist, project manager, information manager and researcher.
During their studies, students work on various assignments which are directly relevant and beneficial to their organizations. At the end of the first year, they work on an assignment to design an eHealth application. This assignment belongs to the module Persuasive design of eHealth.
Module persuasive design of eHealth
Contents of the module
Students learn how to create a conceptual design of an eHealth application, including a summative evaluation plan. This eHealth application must involve a patient-centered design and one or more (health)care interventions. To do so, the students use the integrated approach described in section “Material and methods”. This module covers the phases of CI, value specification, design and evaluation of the CeHRes roadmap, as well as the design principles of Oinas-Kukkonen, and the behavioral model of Fogg.
The operationalization phase of the roadmap is beyond the scope of the module persuasive design of eHealth. During this phase, the conceptual design of the eHealth application is translated into a technical specification and then into a working application. Furthermore, in this phase the application must be implemented within the organization. Although the implementation phase is not covered in the module persuasive design of eHealth, it is part of the module Implementation Management of the master program. Students make a strategic analysis of the implementation and change management aspects of an eHealth implementation and write an implementation plan. The realization of the implementation plan is not part of the master program.
During the past 3 years, several persuasive designs of eHealth applications have been developed by our master students. These include eHealth applications to promote a healthier lifestyle of youngsters with potential weight problems, to support monitoring and self-management of pregnant women with a heart condition, to support children with syringe anxiety, to support communication of patients on oxygen support at the intensive care unit (ICU), among others.
Methodology of delivering the sessions
The module includes nine lessons (90 min per lesson) over a period of 12 weeks. This includes the following: (1) introduction of the CeHRes roadmap and its phases, (2) domain analysis and preparing a business case, (3) user or patient analysis (persona design, scenario design), (4) requirements analysis, (5) persuasive design, (6) user interface design, (7) prototyping the eHealth application, (8) implementation of eHealth applications and (9) evaluation of eHealth applications.
Lessons are taught two times, one after the other on the same day. This option was taken as the module is also given as a master class to students who do not follow the full master program. In addition, it helps students to be really focused on the subject and work of their assignment.
Next to these face-to-face interactions (lectures), students can ask questions to and get feedback from the teachers and other students via the digital learning environment (being a complementary and an asynchronous facility). As a result, we use a blended learning approach for delivering the sessions. For this module, there is a team of two lecturers and a guest lecturer providing good didactic variation.
Collaboration between different educational programs
To translate conceptual design to technical design and a working eHealth application, we collaborate with another educational program, namely, the bachelor informatics course. Over 20 weeks, two groups of fourth year students from the Inholland bachelor informatics course develop the frontend application (the part that runs on a smartphone or tablet) and a supporting backend (the part that runs on the server side, for example, a database). The frontend group takes part in the course Mobile App Development and the backend group in the course Cloud Computing. The master student takes the role of contractor to those two groups. The result is a working prototype of the eHealth application, ready to be implemented as a pilot.
One example of this collaboration is the eHealth application supporting communication for patients on oxygen support on the ICU. The application was first programmed by the informatics students. It is currently being implemented in the ICU of the hospital where the MAHIP student works. The implementation and evaluation of this application will be the theme of the student’s master thesis.
Student’s example of applying the integrated approach
An eHealth application has been designed by one of our students aimed at promoting healthy lifestyles for overweight children. The student has now graduated and still works for the department of Children Healthcare Services in the area of Brabant. “Overweight among children” is one of the current difficult problems faced by the regional Public Health Service. It is beyond the scope of this article to fully detail all the steps which were taken to design the application, but selected aspects in designing the application are described here to give a look and feel of what the student had achieved in just a few weeks.
During the contextual enquiry, the student performed a stakeholder analysis, literature research, and conducted interviews with healthcare professionals, parents and children. Problems and needs of each stakeholder were elicited. For example, it became apparent from this analysis that children have little or no insight as to what healthy nutrition means. From this analysis and after having defined relevant behavioral variables (e.g. sports, knowledge about eating habits, computer usage) and user’s goals and activities, the student was able to construct personas. Figure 6 shows (translated from Dutch) the persona of the primary user. In this assignment, the persona “parent” was also included as a secondary persona since the parent is also involved in the child’s nutrition.
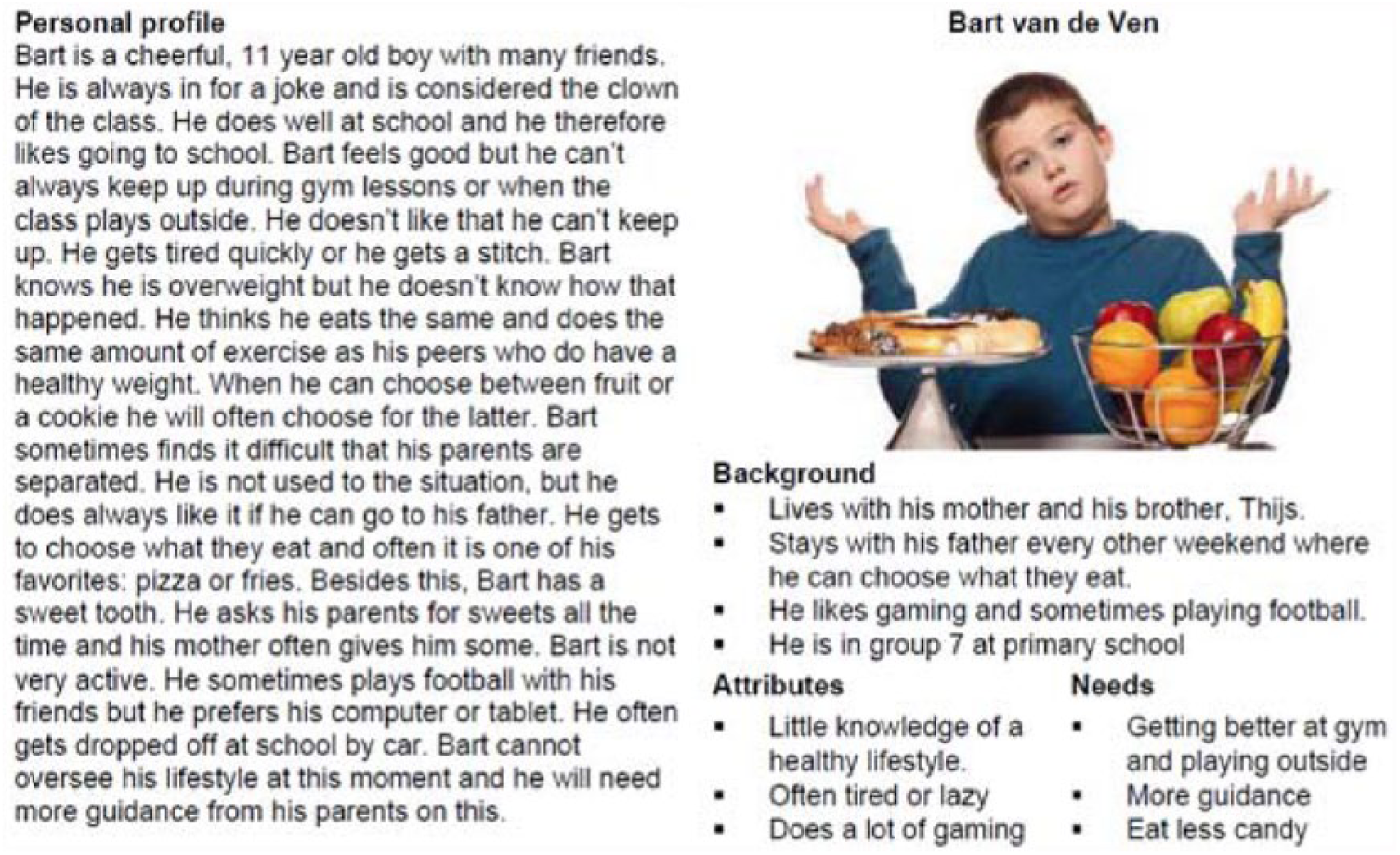
Primary persona.
A list of requirements was formulated. This included, for instance, that the application will give the child two nutritional challenges per week. With regard to the persuasive features, the student made a number of choices. For the design Primary Task Support, personalization with favorite topics and self-monitoring of the growth curve and progress of physical exercises were selected. For the design Social Support, the student included an element of competition with points scored during the past week.
The expected behavioral changes were focused on various span. The green span is relevant to start with a new behavior for a limited period of time such as keeping a diary of physical activities. The purple span is appropriate to increase a behavior, for example, having breakfast and eating more fruits during the day. Finally, the gray span is also important for decreasing a behavior such as eating fewer snacks in 1 day. The student created an interaction model. Figure 7 shows (translated from Dutch) an example of a webpage dedicated to information about eating breakfast, snacks, and fruits. The student also designed a mobile version.
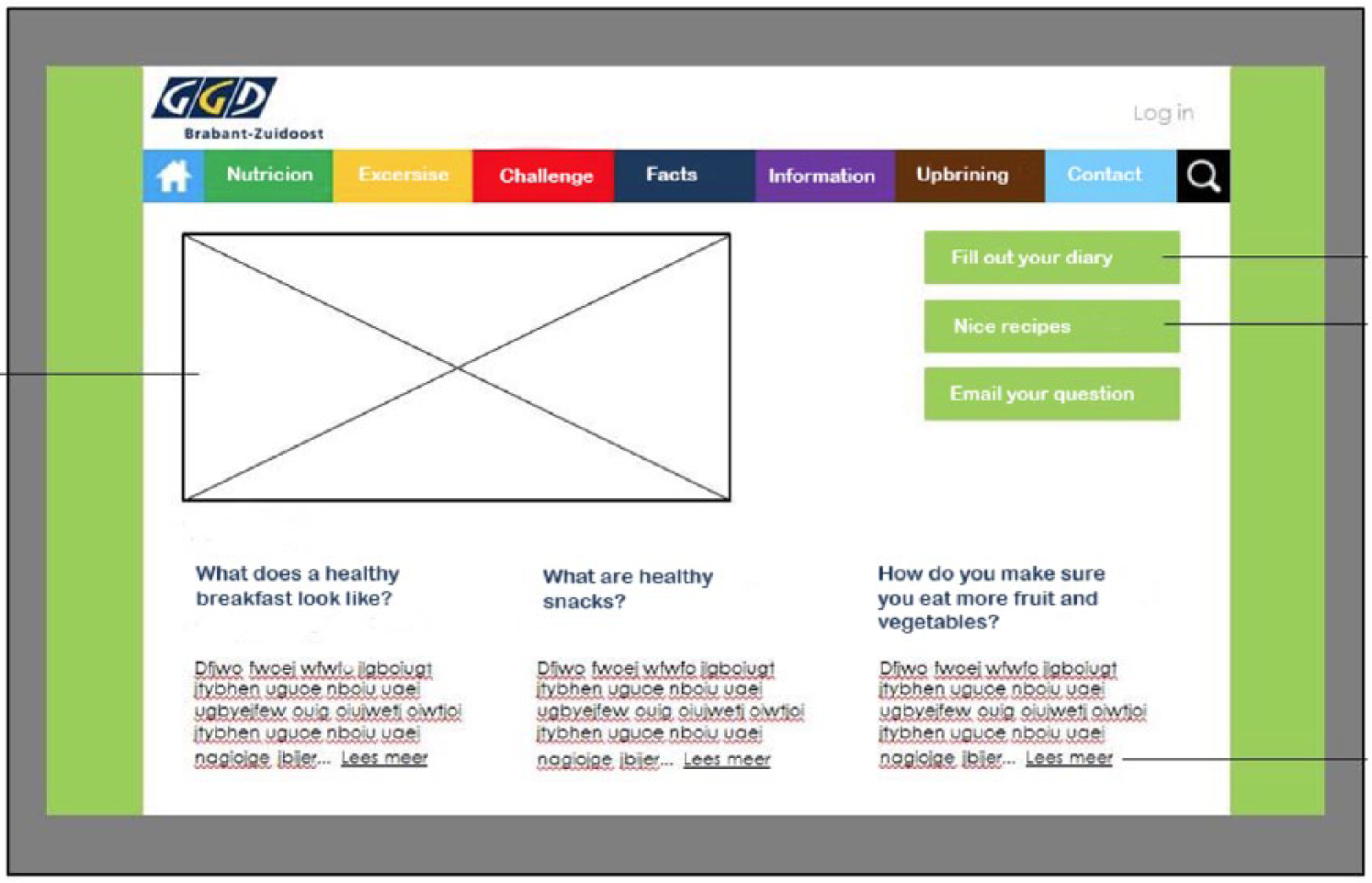
Interaction model.
The design of the application was developed further by a group of Bachelor informatics students from the university who programmed the frontend and backend of the app. The student acted as the contractor for the informatics students. Her employer currently plans to implement this app as part of one of its public healthcare services.
Discussion
In this article, we have presented an integrated, systematic and practical but scientifically based methodology to design effective persuasive self-management applications. The integrated approach makes use of three well-established theoretical models, namely, the CeHRes roadmap, the design principles of Oinas-Kukkonen and the behavioral model of Fogg. Results from applying this approach in an educational context have been reported.
The integrated approach
The choice of the models has been driven by their sound foundations and their practical usability in a teaching setting. The integrated approach can be viewed as a conceptual framework, a sort of analytical tool with several variations and contexts. It is used to make conceptual distinctions and organize ideas. A conceptual framework is aimed at capturing reality in a way that is easy to remember and apply. In our context, this has to do with capturing the process of eHealth design and the use of persuasive principles and behavioral changes for eHealth self-management systems. By no means do we claim that our integrated approach is complete. We do, however, view the proposed integrated approach as a first step that can be refined based on forthcoming assessments. To our knowledge, this integrated approach is a novelty (certainly in the Netherlands) within an educational context. Furthermore, it can be viewed as complementary to other current approaches such as design thinking. 28 The latter is for instance used at the Leeuwarden University of Applied Sciences for designing innovations (including eHealth) for the master Digital innovations in healthcare and welfare. 29
Didactic
At the time of writing, the integrated approach has been embedded into the MAHIP curriculum for the past three consecutive years. The students are adult learners and working as healthcare professionals. The integrated approach provides a number of didactic functions. As a cognitive function, it helps students to understand and learn basic concepts of the eHealth development process, persuasive design and behavioral changes. The formative function includes acquiring the skills to use these basic concepts. The instrumental function has to do with achieving the educational objective of designing an eHealth application. Finally, the normative function helps to attain the required result, in our context the assignment of designing an eHealth application based on the integrated approach.
Student’s perception and evaluation
The CeHRes roadmap helps the students in developing the eHealth intervention in part because it is less abstract compared to the other subjects taught in the previous period. The roadmap provides a step-by-step plan from which students can work. The module is often an eye opener for students. Designing an eHealth application is not just about designing an interface. The solution proposed and developed is well thought through and grounded in practicality.
The assignments students carry out are one indication of whether the approach is usable in a teaching setting and of its didactic added value. Until now, a majority of students (89%) manage to carry out the assignment successfully. Success rate is also dependent on the student’s own abilities and on the teaching support received. In any case, the results of the assignments provide good insight into the usability of and compliance to the integrated approach. The module persuasive design of an eHealth application is evaluated every year and changes are made accordingly. The changes made so far have been related to the composition of the lessons rather than to the integrated approach. An assessment dedicated to the integrated approach itself is one activity we plan to carry out in the near future.
Evaluation of the module is done after the last lesson (face-to-face evaluation) and is complemented with an online anonymous evaluation. In the 3 years which the module has been taught, only positive reactions have been received.
Problems encountered and shortcomings
Few difficulties were encountered while delivering the sessions. However, we can report the following:
Some students show a need for reassurance that they are applying the roadmap appropriately. This was noticeable during the lessons or via the digital learning environment where students can post questions and their work in progress.
Every student works on their assignment at their own pace. This means that some students are not always able to immediately apply what they have just learned. During each lesson, there is time for the student to work on their assignment alone or with another student. For example, let us say a student is still busy with defining personas and scenarios and the lesson of the day focuses on requirement analysis. In this case, the student may have some difficulty during the lesson on relating to requirement analysis for their eHealth application. This will be done when the student has reached the phase requirement analysis for his application.
Some students struggle at the beginning of the module in choosing the appropriate topic for their eHealth application. The application has to be developed in the context of a healthcare intervention. It is our responsibility as lecturers to guide students in making the appropriate choice.
Some of the shortcomings that have been noticed include the following: the time allocated for the module and for the assignments (in total 12 weeks) is too short. It is sufficient to understand the CeHRes phases, the design principles and the behavioral model. However, it is not sufficient, for example, to perform a detailed CI or to co-create with the relevant stakeholders. Timing is also an issue for inter-educational collaboration. Connecting the phases in the curricula and learning goals of different learning plans are challenges we face and need to be addressed. For example, whenever the courses Mobile App Development and Cloud computing start before the course persuasive design of an eHealth application has been completed, there are implications for the Informatics students who are being delayed in starting the programming of the application. Furthermore, we also notice a shortage of informatics students in taking up these eHealth-based assignments. The topics of the eHealth application do not always appeal to them.
Implications for best practices
eHealth provides a means to develop new healthcare models based for the largest part on patient autonomy, self-management and empowerment. Current trends in health as stated in section “Introduction” influence the way best practices are shaped and defined. Best (or good) practices for eHealth are often viewed from a broader perspective, involving for instance eHealth strategies, linkage to national health goals and priorities, governance and so on. The World Health Organization (WHO), for example, provides a national eHealth Strategy Toolkit, a practical guide that gives governments, their ministries and stakeholders a solid foundation and method for the development and implementation of a national eHealth vision, action plan and monitoring framework. 30 Moreover, one should not underestimate the potential of business models as part of a best practice when designing sustainable eHealth applications. 31
An eHealth application that is being successfully used and implemented is too often seen sufficient to be defined as best practice. However, persuasive design is one of the components for the best practice, which may or may not be accounted for when defining it. In order to gain more insights into the suitability of persuasive design for a given eHealth application, one may call on the law of attrition as proposed by Eysenbach. 32 Through the law of attrition, it is possible to define the attrition rate and factors in the users’ dropout of using the application. We argue that persuasive design for eHealth should be a more visible aspect of best practices. Visibility via educational programs and transferability through educated healthcare informatics professionals are a means which we advocate.
Finally, creating best practices for eHealth design and development present challenges for interdisciplinary work. As reported by Pagliari,
33
By sharing information about our research approaches and seeking to actively collaborate in the process of design and evaluation, the aim of achieving technologies that are truly user-informed, fit for context, high quality, and of demonstrated value is more likely to be realized.
We strongly agree with this view and through the (recently founded) Inholland Health and Technology Center (IHTC) 34 we provide a regional and national platform to stimulate and encourage partnerships in eHealth design and development between educational setting, practices and research. The proposed integrated approach based on persuasive principles and behavioral changes under a holistic process of eHealth development is part of the endeavor for integral best practices.
Conclusion
An integrated, systematic and practical but scientifically based methodology has been proposed to bridge the gap between theory and practice in designing persuasive eHealth applications. The integrated approach makes use of existing models in the areas of eHealth development, persuasive design and behavioral change, respectively, the CeHRes roadmap, the design features of Oinas-Kukkonen and the behavioral model of Fogg. Results and lessons learned in embedding this approach in our educational health informatics program have been reported and discussed. The road to creating best practices in persuasive design of eHealth and teaching those to healthcare informatics professionals remains a challenge. The integrated approach is a first step in this direction and further work in refining it will be undertaken in the future.
Footnotes
Acknowledgements
We wish to thank Inholland University of Applied Sciences for their support in preparing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.