
Abstract
Mobile phones can produce detailed and personalized data to help diagnose, treat, prevent or rehabilitate women who are victims of gender violence. We sent automatic text messages, based on cognitive-behavioural therapy, to female victims of gender violence to assess the feasibility of the medium for mental health intervention. During the 28-day intervention period, each woman received four automatic text messages every day on a pre-established schedule. We evaluated symptoms of depression using the Personal Health Questionnaire-9. The Personal Health Questionnaire-9 decreased from an average of 14.8 at the beginning of the intervention, to 6.1 at the end of the text messaging period. All of the women reported that they liked receiving the messages, they found them useful and they felt that the messages had improved their health. Text messages are acceptable to women users who are recipients of public health and social services. Future research should focus more on the evaluation of the results and on how the specific content and aspects of text messaging improve health outcomes.
Introduction
According to data from the International Telecommunication Union, 1 there are 96.8 mobile phone subscriptions per 100 inhabitants globally. There are more mobile phones than there are people in developed countries (120.6 per 100 inhabitants) and almost one mobile phone per capita in developing countries (91.8 per 100 inhabitants). Mobile phones can become valuable tools in psychotherapies. They can produce detailed and personalized data to help diagnose, treat, prevent or rehabilitate socially excluded people. Mobile phones can collect objective data for psychological and social studies but they need to be understood as a work tool for the therapist.2,3 Several researchers have conducted experimental studies on cognitive-behavioural therapies (CBT) by sending text messages to mobile phones in various patient populations4–11 but not specifically with female victims of gender violence. This group has a high need for mental health interventions and could benefit from these technologies.
According to the World Health Organization, one in three women in the world has suffered or endured some form of violence in their childhood, adolescence or adulthood, an experience that affects their mental health, 12 and gender violence means any act of violence based on belonging to the female sex that has or may result in physical, sexual or psychological harm or suffering for women, as well as threats of such acts, coercion or the arbitrary deprivation of liberty. 13
This article is part of a broader programme of research focused on the design and study of an automatic system of remote psychotherapy for vulnerable people. We have previously reported the positive results of case studies with small groups of up to 21 vulnerable unemployed women for a continuous period of more than 12 months. Most women indicated that receiving text messages made them feel more connected to their social environment; they reported that the messages had improved their mood, and that they would like to continue to receive messages. 14 We discovered that 11 of the 21 unemployed women had been victims of gender violence. In the present article, we present the analysis of the results of the subgroup identified.
The objectives of our analysis are (1) to present the results of a systematic case study with long-term unemployed women who have suffered gender-based violence and (2) to reflect on the advantages and limitations of using mobile phones in psychosocial interventions with these vulnerable populations.
Material and methods
Our research involves an analysis of a text messaging-based psychosocial intervention for vulnerable, unemployed women who have been victims of gender-based violence in Spain. We decided to use text messages as a psychotherapeutic tool to improve the mental, physical and social health of a group of 11 women fitting this profile. All of the women had personal mobile phones and the skills to send and receive text messages.
The social services organization of the Autonomous Government of Galicia identified 40 cases of women who had been unemployed for more than 1 year, were living in poverty and had insufficient economic resources to support their families. These women resided in one of the eight municipalities that consented to participate and were located in the urban area of the city of Santiago de Compostela (in northwest Spain). All of these women were contacted by the researchers to request an in-person interview to explain the objectives of the study and 21 of them agreed to participate and provided informed consent. The meeting was arranged by telephone with the support of the municipal social services.
We conducted initial interviews in which we asked the women questions about their health status, current medical treatments, social and family relationships, professional activities, economic status and physical activities. The information obtained from each woman was complemented with information from her official social history records, for which we obtained prior informed consent from the women. From all this information, we identified 11 cases of female victims of gender-based violence. The entire process complied with the guidelines set out by the Bioethics Committees of the University of Santiago de Compostela and the University of California, Berkeley. The research, method, objectives and development were analysed and approved by the Bioethics Committees mentioned above.
We then contacted the 11 identified women to inform them that they would automatically receive personal text messages on their mobile phones, which they were free to answer when they deemed convenient. They were informed that we were not going to engage in personal dialogue through these messages, and that our goal was to follow, advise and improve their moods, as well as their physical and social health. With regard to the economic costs of sending and receiving text messages, all of the women were informed that the expenses would be entirely assumed by us, and that they would be absolutely free of charge for them.
These text messages were sent through mobile phone operators in SMS format, avoiding Internet messaging and, thus, ensuring that all of the participants received the messages on their phones regardless of their Internet connection. We observed that these women accessed the Internet from their mobile phones using free Wi-Fi systems in specific locations, days or times.
For 28 days, we systematically sent four text messages each day to the mobile phones of each woman at the following times: 09:00, 13:00, 17:00 and 21:00. We elaborated four message banks that focused on thoughts, health, physical activity and social relationships. An example message from each category is ‘Some thoughts can be unhealthy and pollute our minds; identify them and put them aside’, ‘How many enjoyable activities did you do today?’ ‘Maintaining a social life can make us feel better or worse. Try to identify the people who make you feel better’ and ‘What did you do today to take care of your health and well-being?’ In total, each woman received 112 text messages. We sent messages asking about, advising and orienting their daily habits with the purpose of improving and developing positive and healthy behaviours. The messages were based on the information collected from the interviews and the official social history records of each woman. We also based our messaging on previous experience of research with Spanish speakers suffering from depression. 4
To build an environment of trust and to answer any questions or concerns from participants, we had direct telephone contact with each woman at the beginning of the investigation, after 14 days and at the end. We dedicated an average of 15 minutes of direct telephone contact with each woman (5 minutes for each contact).
It is important to note that the automatic messaging system includes an alert system that automatically detects risks of potential suicidal or violent behaviour by detecting keywords in response messages (e.g. kill, suicide, die). We purposely did not notify women of this feature as we did not want it to be used to reach out and instead built it as a safeguard. We prepared an action protocol that was validated by the Bioethics Committee of the University of California, Berkeley, where if alerts were detected we would immediately communicate the information to the municipal social services, who would act accordingly. There were, however, no incidents of suicidal ideation or intent.
In terms of demographic and social characteristics, all participants had experienced gender-based violence as well as continued unemployment of at least 1 year, their average age was 40.5 years (standard deviation (SD) = 7.9; range = 29–50) and they had an average of two children (SD = 1.3; range: 1–5). Participants also reported cases of prostitution (9%, n = 1), drug addiction (18%, n = 2) and immigration from other countries (27%, n = 3) – with women from Brazil, Croatia and Colombia who had fluent written and spoken Spanish. Some participants reported diagnoses of mental illness that included anxiety, depression, recognized mental incapacity and/or under psychiatric or psychological treatment (45%). Most of the women were urban residents (73%). With regard to their educational attainment, 82 per cent had completed the primary level of education, 9 per cent secondary and 9 per cent had obtained a university degree. Most were divorced or separated (91%) and the rest were single and never married. It is important to stress that the majority (73%) of these women were engaged in informal work situations without legal recognition, such as working in elderly or disabled care, domestic or agricultural work and, in some cases, prostitution. In the remaining cases, the women received pensions or subsidies.
Measures
The main outcome measure for the study was the response rate to text messages and depression symptoms as measured by the Personal Health Questionnaire-9 (PHQ-9) at the beginning and at the end of the intervention period (28 days). The PHQ-9 questionnaire is a widely validated instrument. 15 We have also used this questionnaire in previous research 6 where each participant was asked to evaluate his or her experience. The questionnaire asked questions about the positive and negative aspects of the intervention, the perceived effectiveness, ratings of the number of messages received and whether they were interested in continuing to receive messages. In addition, we also assessed the response rates to the messages, as well as medication adherence.
We did not find significant correlations between the PHQ-9 results and age and between the PHQ-9 and the number of messages answered. The small sample size (n = 11) limited the statistical analysis regarding the correlation between variables or the paired simple test and other statistical comparison tests.
Results
All of the women participants (n = 11) responded to messages or phone calls: two women only answered telephone calls (18%) and nine responded through text messages and telephone calls (81%). All of the women received the same 112 text messages and the average number of messages answered per participant was 22 (SD = 25.7, range = 3–82). Participants who did not respond to text messages reported feeling unsure about answering, not knowing what to say or stated that the cost of sending the response messages was a barrier, even though they had been informed that these costs would later be repaid.
Symptoms of depression were assessed using the PHQ-9 and they evolved from an average of 14.8 at the beginning of the study (SD = 5.7, with a range of 3–19) to 6.1 by the end of the 28-day text messaging period (DS = 5.1, range 0–16). The difference between the two ratings was significant (t(11) = 2.22; p = 0.001). Scores of five represent mild depression and scores of 10–15 represent moderate depression. 15 We can highlight the fact that only two women (18%) had increased PHQ-9 values at the end of the intervention period (Figure 1). In both cases, we were able to detect problems with psychiatric medication adherence, drug addiction, prostitution, family conflict and social isolation.
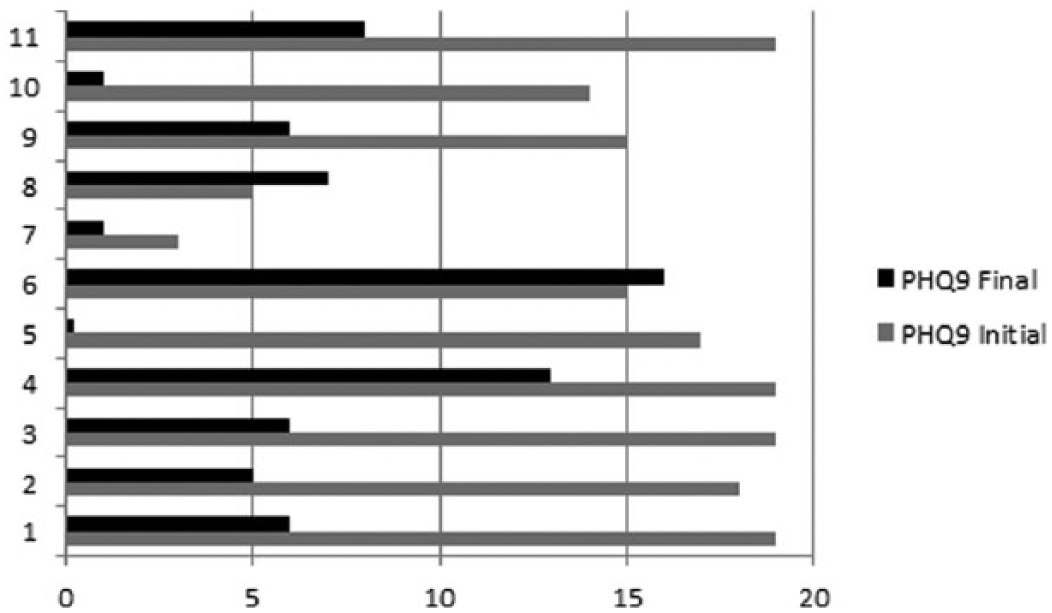
Representation of the initial and final PHQ-9 data.
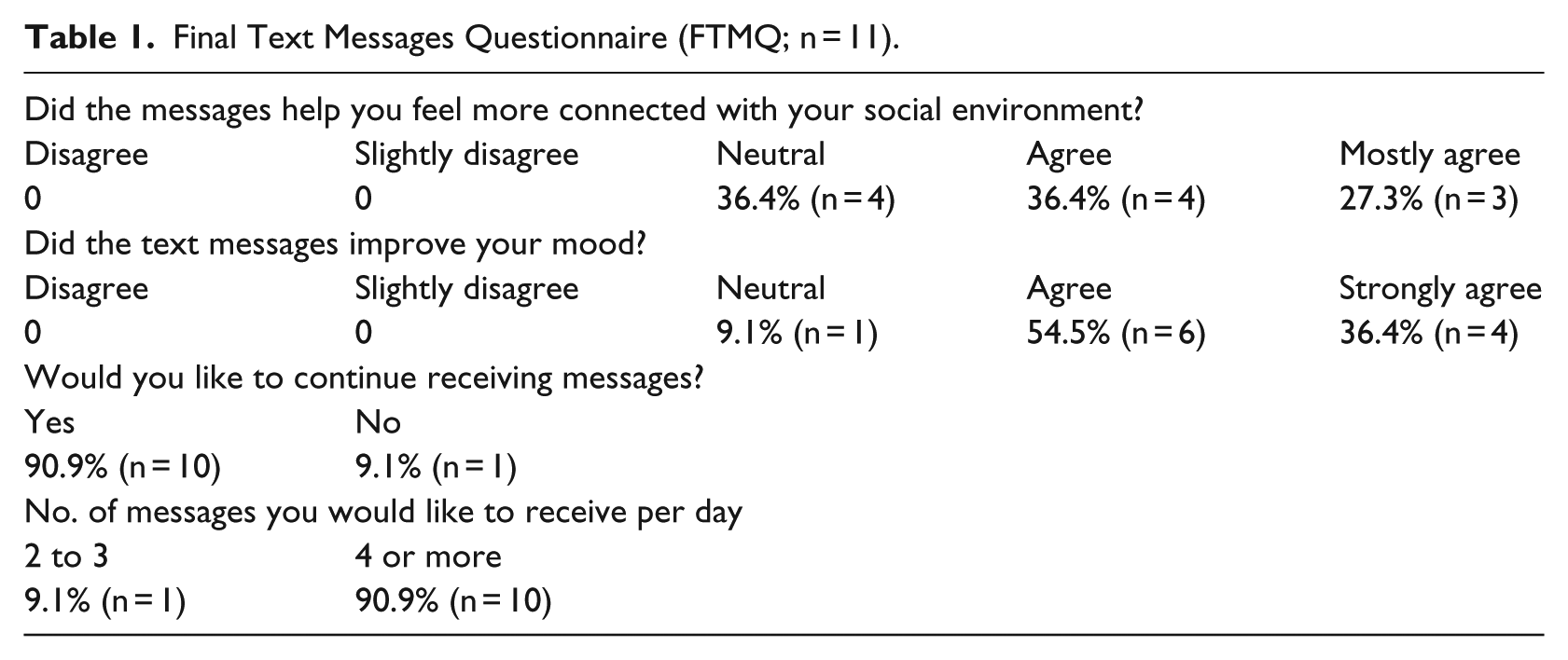
Most women indicated that the text message programme made them feel more connected to their social environment, answering that they agreed or strongly agreed with this statement, as shown in Table 1. Most women (91%, n = 10) agreed or strongly agreed with the statement that the messages had improved their mood, and that they would like to continue to receive messages (91%, n = 10) with a frequency and intensity of four or more messages each day (91%, n = 10).
Final Text Messages Questionnaire (FTMQ; n = 11).
Over the 28-day period, all of the women started and ended the experience at the same time and the response rate to text messages was 82 per cent (SD = 29.8%, with a range of 3%–95%, the IQR was 17 (20–3). With regard to suggestions for system improvement, one woman reported that the messages were sometimes repeated, and that she needed more time to reflect to be able to offer an answer. No problems were reported in terms of scheduling messages or message content. Five women (45%) mentioned that they saved the messages to personal files in order to read them on other occasions or to use them as a reference in their daily lives.
The women who participated were overwhelmingly positive in their responses to the messages. In general, they all stated that the messages had helped to improve their mood, to organize and plan their daily lives, had changed habits and attitudes, that they had felt accompanied and advised, and that they had improved their social relations. Two of the women commented that they also felt motivated to exercise or to improve their diets.
Discussion
Our results indicate that a group of vulnerable women who experience long-term unemployment and gender-based violence are receptive to a psychosocial text messaging intervention as part of their participation in social services. Text messages are acceptable to consumers of public health and social services and have the potential to improve outcomes at relatively low economic cost. Daily text messages guide, advise and reinforce healthy behaviours but further research is necessary to determine the influence of face-to-face interventions relative to text messaging interventions. It is possible that text messaging can enhance a face-to-face intervention 4 but there is a need for more controlled research that compares the results with standard face-to-face therapeutic interventions.
Cost may still be a barrier for the most economically vulnerable. Although receiving SMS is free of charge, sending SMS is not free of charge and is not included in most mobile phone plans in Spain. In our study, participants were informed that the researcher would assume the response costs but many still perceived the cost of sending messages as a barrier. This is an obstacle that needs to be overcome, perhaps via the use of mobile messaging apps such as WhatsApp and others. However, these apps can also be limiting for people with low economic resources who are forced to look for free Wi-Fi access spots, which costs them time and mobility.
Future research should focus more on the efficacy of mobile interventions with vulnerable populations. Mobile phones can collect daily data on mood, activities, geographical location, thoughts and feelings, social relationships, eating habits and so on, which may be accessed by health providers and integrated into healthcare and social services to improve outcomes. Interventions may also involve family members or key people in the daily lives of these vulnerable women, supporting efforts to improve their physical and mental health.
Limitations
Our analysis of the intervention is limited due to the small size of the sample. We cannot draw general conclusions based on the responses from this small group of women, particularly with respect to the cognitive and behavioural changes experienced. New research is needed to address the impact of specific life experiences and socio-demographic factors, such as gender violence, immigrant women, age, culture and mental health diagnosis. In addition, as we did not use a control group to establish comparisons, our ability to make causal claims resulting from the text messaging programme is limited. We need to design new research that includes a control group of women victims of gender violence who do not receive messages or other forms of intervention. However, the positivity of the responses is encouraging for the expansion and testing of text messages as a means to disseminate psychosocial interventions as a part of public social services.
Conclusion
Text messages are viewed positively and can be used as tools for the dissemination of psychosocial interventions with women who are victims of gender-based violence. Our results generate questions and highlight the need for new research to understand the efficacy and effectiveness of this and similar interventions. Our study has focused on unemployed women who have suffered gender-based violence but we do not know if the therapeutic benefits of text messages would be the same for unemployed women who do not suffer gender violence.
Text messaging systems could open the way to personalized attention, counselling, support and guidance for vulnerable populations in general. Using text messaging as part of social and healthcare services could help to maximize social service resources in a cost-effective manner. Given the accessibility of mobile phones and the relatively low cost of this form of intervention, more people could benefit from social and health interventions that encourage positive changes in their health behaviour. We have found that a reasonable combination of text messages, occasional telephone contact and personal, face-to-face interviews are feasible and accepted among users of public social services in Spain. We need more research and studies that assess mobile health interventions among vulnerable populations who may stand to benefit the most given the scarcity of resources available to them.
Footnotes
Acknowledgements
The authors are also grateful for the guidance and controls of the Bioethics Committees of the University of California, Berkeley and the University of Santiago de Compostela.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research would not have been possible without the support and collaboration of the General Directorate of Social Inclusion of the Xunta de Galicia, Spain.