
Abstract
This study describes a unique approach to information transfer affecting the perceived value of this information and related impact on smoker behavior. Data were collected via survey, sampling approximately 120 participants. An online survey tool was used for the survey creation, data collection and monitoring. Another online tool was used by participants to create short animation videos as a means of increasing their engagement with information in an experiential fashion. Study findings included that the process experienced by the test group was influential and facilitated participants’ change of mind regarding enrollment in a smoking cessation workshop. This was partly attributable to the IKEA effect. The study provides evidence that a change in habits crucial to improve health and enhance positive lifestyle choices can be stimulated through active engagement with artifact creation in a technology-mediated environment.
Introduction
More than ever, awareness of health and well-being is a mainstream topic often viewed as a top priority in an individual’s day-to-day decision-making process. There is no doubt that health and well-being are indeed a matter of high value for the majority, yet many times achieving good health involves effort, such as sports participation, exercise, and a custom-tailored diet that require high levels of will and self-discipline. Moreover, when the will to lead a healthy lifestyle collides with bad habits, some individuals may find the bad habits with an upper hand. So, how does one decide to make the effort, if it requires altering one’s lifestyle? That is a question addressed by this study. We examine a critical factor that can motivate an individual to abandon bad habits and lead a healthier lifestyle. Our research examines how utilization of the IKEA effect increases the perceived value of information thus influencing smokers to register for cessation workshops at higher rates.
Literature review
Smoking and its implications are subjects of numerous research studies. This article draws on a subset of these and examines the reaction of smokers to smoking-related information. Among the areas considered are health hazards, social restrictions, economic implications, and cessation.
Health hazards
Smoking is a common practice around the world, known to be the province of over one billion people globally. Smoking is the single greatest preventable cause of disease and death in the United States. 1 In their research, Ryan et al. 1 review different groups within the smokers’ community categorized according to the volume of their daily smoking. Although health-care approaches result in several differences between groups studied, there is little doubt that smoking causes a multitude of health problems. This is not an isolated conclusion and is supported by major studies including those published by the US Surgeon General. 2 Many studies have found a strong connection relating health problems and smoking, ranging from cancers, 3 to respiratory and cardiovascular disease, 4 to various other disorders. 5 According to other research, a smoker’s chances to die by any cause are three times greater than a person who has never smoked. 6 Furthermore, the majority of deaths among smokers were caused by neoplastic, vascular, and respiratory diseases—all much less common in non-smokers. In addition, life expectancy among current smokers is more than 10 years shorter. According to Jha et al., 6 a current smoker’s chances to suffer from lung cancer are about 6.5 times greater than a person who never smoked. Furthermore, the chances for a current smoker to die from a respiratory disease are twice that of a non-smoker. The ills of smoking extend beyond individual health. Smoking is a common denominator in adverse effects in a variety of other realms. This makes health problems caused by smoking a mainstream topic. It is well-advertised and continuously broadcast in the media via different venues meaning most people are aware of its health risks.
Social restriction
Humans are not solitary creatures and tend to live in societies. This means their fates often are interrelated. Smoking provides an example. Although performed by individuals, it may take place in public, thus affecting not only the smoker but also passive bystanders. As a result, governments and municipalities have been obliged to constitute new rules and regulations, and law authorities have attempted to make adjustments regarding enforcement. As awareness of smoking hazards grew, so did the demand for smoke-free policies and stricter enforcement. 7 Over the past few years, this growing concern of the negative effects of passive exposure to tobacco smoke on the non-smokers’ health has increased. As a result, smoke-free policies have been designed. As might be expected, studies in China 8 and Germany 9 have indicated support for smoke-free policies in public places among non-smokers and people chronically influenced by passive smoking but not so much among smokers.
According to a study conducted in five European countries, 65 percent of the population are current or former smokers. 7 This study examined three smoke-free policies: (1) smoke-free public places, (2) taxation of tobacco products, and (3) regulation against the sale of tobacco products to minors. The results showed that current smokers were less supportive of smoke-free public places and taxation as compared to non-smokers and former smokers. The non-smokers group was more supportive of smoke-free public places and restrictions on sales to minors than on added tobacco product taxation. In addition, current smokers reported greater support for regulation against tobacco sales to minors than for smoke-free public places and added taxation.
Still, in spite of attitudes, compliance, and awareness, 10 tobacco use is related to millions of deaths worldwide, and the World Health Organization predicts that tobacco use will increase within many demographics in the coming decade. 11
Economic implications
In addition to health hazards of smoking, major economic consequences exist as well. Studies show that smoking affects economies worldwide since it causes extensive expenditures due to morbidity, medical care, premature mortality, and disabilities.12,13 Moreover, a study by Turner et al. 14 suggests the need to finance public health since its definition—“the science and art of preventing disease, prolonging life, and promoting health through the organized efforts of society”—clearly stands in conflict to smoking and its immediate effects.
Various policies have been enacted to reduce tobacco consumption through economic means. Examples include regulations and taxation on tobacco products used to increase prices either directly or indirectly. But, the economic impact is not limited to the tobacco user alone. In fact, society in general often bears the cost of regulation and enforcement.
Both direct and indirect costs result from tobacco consumption. According to Rice et al., 12 direct costs are related to hospitals and nursing home care, services of health practitioners, drugs, and tobacco products. Also included are indirect costs such as costs to quit smoking, those due to fires caused by cigarettes, and labor force expenses due to smoking-related illness. These indirect costs add to the total losses but are more difficult to calculate. Often, these costs fall on the individual or family and may include opportunity costs due to lost productivity and shortened life span.
In 1979, indirect tobacco costs were estimated to be about US$4–US$6 billion and direct costs in the range of US$29 billion in the United States. 15 Some of the expenses such as transfer payments from social security, pension and disability plan costs, and paid time off for illness were subsidized by non-smokers. The sum of indirect and direct smoking costs from all sources was calculated by Rice et al. as being approximately US$38 billion in 1980. 12 These expenses have greatly escaladed in recent years. According to Ekpu and Brown, 16 these costs are now half a trillion dollars globally.
However, cash flow created by regulation and taxation has also increased. According to a report issued by the Israeli Health Organization in 2012, the income from smoking-related taxation was 5.3 billion. In the municipality of Tel-Aviv, IL, fines due to smoke-free law violations reached to the sum of 1.66 million NIS. 17 In spite of added revenue, the new inflows do not offset the costs to society. 18
Smoking cessation
Smoking addiction presents challenges to those who seek a way out of unwanted habits. Various cessation programs exist: smoking cessation classes, incentive-based smoking cessation contests, self-help quit smoking kits, and many more. Other methods include using medications, alternate nicotine delivery systems and medical interventions. Some methods are considered more successful than others, but in total these programs yield a 21–35 percent success rate.19,20 According to some studies, smoking cessation requires particular abilities and environmental opportunities.21,22 Sometimes, brief advice from a professional appears more effective than volumes of information from other sources. For example, in a study conducted by Hjalmarson and Boëthiusb, 23 advice given by professionals led to a decrease in the proportion of people smoking by 2 percent, compared to those who received no advice from a professional. Other factors, such as spouse smoking status24–26 and household smoking policies, also appear to play important roles in smoking cessation. 27
In the field of health, there are fewer studies examining the cost-effectiveness of prevention programs (particularly, the cost-effectiveness of smoking cessation) than of those studying the treatment-oriented programs. A report by Altman et al. 20 examined the cost-effectiveness of three smoking cessation programs:
Smoking cessation class: The class included eight 1-h sessions, of which the first five were offered in consecutive weeks and the remaining three were once every second week. The cessation techniques included self-monitoring, deep muscle relaxation, goal setting, and group social support.
Incentive-based smoking cessation contest: This program lasted 6 weeks and was presented as a community smoking cessation contest. The program participants were asked to choose a day within the contest time frame to quit smoking. The contest was promoted through television, radio, newspapers etc.
Self-help quit smoking kit: The program was a four-step, self-quit kit. The kit contained four tips, comprising four double-sided pages: one side provided general information and the other provided specific tips on quitting and related action items. Once a participant completed a step, he or she could post it on the refrigerator.
The main variable was post program smoking status (smoker vs non-smoker). On average, participants of the first program quit smoking at the end of the fifth week, participants of the second program quit by the end of the fourth week, and participants of the third program quit by the end of the third week. In regard to the cost-effectiveness, the most cost-effective program was the self-help program and the least cost-effective program was the class. No long-term recidivism rates were included. 20
Other, more modern approaches to cessation programs exist. 28 Many of these are intended to reach large audiences made possible through Internet technologies. Using the World Wide Web, health-care information can reach anyone with access to mobile technology or computers, even in places where no smoking cessation clinics exist. The Internet has the potential to deliver behavior change intervention in a variety of ways related to health care.29,30 According to Civljak et al., 31 the uses of tailored or interactive Internet-based interventions are more efficient helping smoking cessation over a period of 6 months.
There are reasons why Internet-based smoking cessation programs appear to be effective. 32 Among these are the diversity of communication opportunities—the information is accessible everywhere right when it is needed. 33 The interaction is anonymous and in many cases, even automatic. 31 Although some reports suggest that the aspect of personal interaction is missed. 34 In other studies, encouraging cessation among young adults seems to be a priority in Internet-based programs. Furthermore, web-based cessation interventions as part of an online college life magazine increased the rates of quitting after a 30-week program to approximately 40 percent, which is higher than many other cessation programs. 35 Other research has indicated higher cessation rates for younger adults. 36 Although information regarding smoking effects and its hazards is accessible anywhere, and despite the increasing awareness of healthy lifestyle choices, many smokers continue smoking while others attempt but fail at ceasing.
Information search model
Modern forms of media come in different formats and allow immediate accessibility to information at all times. The search for health-related information has become more popular but amid the non-stop flood, finding relevant information has become difficult. In all areas of health care, there has been a shift in the way medical treatment information is received. Sometimes this shift is called health empowerment, defined as a combination of “knowledge, skills, and a heightened self-awareness regarding values and needs” to help patients reach their personal health goals. 37 Health empowerment has frequently been operationalized in terms of how much patients participate in the medical decision-making process 37 and how this motivates their decision-making process. Dupuits 38 suggest that informational media has a significant influence on patients’ empowerment and their participation in the decision-making process. However, in other instances, researchers ask whether high amounts of information are always beneficial. For instance, in a study of prostate cancer patients, Broom 39 says Internet health information has served as a source of empowerment for some and as a source of confusion for others. 40
Another topic to be considered in this area is the perceived value of information—a key factor in consumers’ satisfaction with the information search experience. Most people searching for health-related information do it for the sake of learning, so careful attention should be put into the layout and structure of information. In their study, Goetzinger et al. 41 examined the importance of the perceived value of information during a consumer’s e-health experience. They created a model of consumer e-health information search behavior that consisted of several elements. The net outcome was to increase the perceived value of received information. 41 Among their model’s elements were:
Information relevance: Is the online health information communicated relevant and are important details about health provided together with the data necessary to estimate ones’ health status?
Information clarity: Was it easy to follow the online health information? Was it presented clearly and the concepts and language used by the online health information sensible to the reader?
Utilitarian value: While searching online health information, did the reader receive exactly the information she or he wanted?
Epistemic value: Did the quality of online health information influence the readers’ knowledge of health and did she or he learn new things from online health information?
Satisfaction with online health information search: Were the readers satisfied with his or her choice to search for health information on the Internet?
Intention to repeat online health information search: How likely was the reader to get more health information online? How likely was he or she to use the online health information for most of his or her needs?
According to Goetzinger et al., the model provides the correct way for information sources to present consumers with information in a methodical structure that increase its perceived value and quality. Ultimately this results in consumers’ satisfaction and intention to repeat online information search. 41 Of course, this model is designed for people searching for information to expand their knowledge. When it comes to lifestyle choices and habit formation, this model can form a basis but changing habits also requires understanding a psychological dimension that can trigger the change. 42
The IKEA effect
Increasing the perceived value of a topic is a well-known method to change habits and lifestyles. The importance of perceived value has been researched and found to ultimately effect decision making. 43 One way to increase perceived value is via the IKEA effect. The IKEA effect is a phenomenon noticed by researchers which shows the impact of an individual’s labor on product valuation. This means when people imbue products with their own labor, their effort can increase their sense of valuation. 44 An example of the IKEA effect comes from the increase in perceived value demonstrated via origami figure building. Non-professional origami builders were asked to create origami figures while given origami instructions and then were asked to assess their creations by bidding on them. The experiment demonstrated how these non-professional builders assessed their creations as if built by professionals, while another group of non-builders have assessed them as amateurish creations. 45
Another example for the strength of the IKEA effect relates to instant cakes marketed in the early 1950s. Instant cakes were a part of a new trend aimed to simplify the life of American housewives. At the beginning of instant cake production, feedback from housewives using the product indicated the baking process was too easy, thus the cakes were unappreciated. As a result, the manufacturer decided to change the recipe to involve more effort by the housewives. The new recipe required bakers to add an egg and this resulted in a greater adoption rate. 45 In their research, Norton et al. 45 showed that labor leads to increased valuation only when labor results in successful completion of tasks. They concluded that labor increases valuation of completed products not just for consumers who profess an interest in “do-it-yourself” projects but even for those who are relatively uninterested. Another perspective for applying the IKEA effect is application to information gathering and self-schooling. In this case, the perceived value of information gathering holds a great deal of influence on consumers’ decision making. 46
Hypotheses
Many studies have examined the phenomenon of smoking, its effects, and ways that cessation rates might be improved. In spite of this, rates of quitting remain dismal. The current research is based in part on a general model developed by Goetzinger et al. 41 as a way to increase the perceived value of information related to cessation. However, an extra step was added to engage those receiving the information. Since nearly unlimited information flow and the ubiquitous nature of the Internet provides facts regarding the harmful nature of smoking both on personal and societal well-being levels, we believe more than just awareness is required, and we suspect that a structural and methodical presentation of information might not be enough to motivate smokers to achieve cessation. Therefore, in addition to the ideas suggested by Goetzinger et al., 41 we propose including the IKEA effect. Our research model and subsequent hypotheses, based on the reviewed literature, follow the structure in Figure 1.
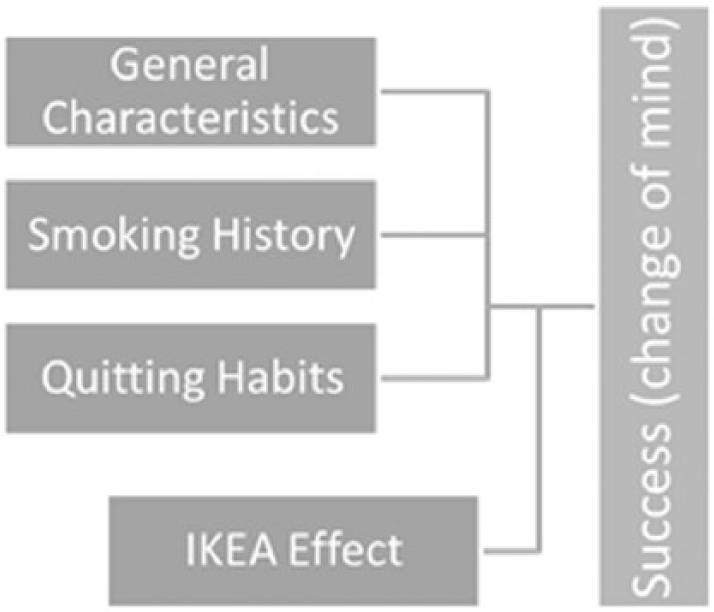
Perceived information value with IKEA Effect Moderation.
Tobacco industry views of young adult quitting behavior contrast with clinical practice. Tobacco marketers concentrate on recapturing young quitters, while organized smoking cessation programs are primarily used by older smokers. Young people have both the greatest propensity to quit and the greatest potential benefits from smoking cessation. 47 Therefore, targeted cessation programs for young adults are needed. Tobacco marketing data suggest that aspiration messages that decrease the social acceptability of smoking and support smoke-free environments resonate best with young adult smokers’ motivations. 48 However, the wide availability of information about the harm associated with smoking may go unnoticed unless young adults become part of the process related to information conveyance. We believe that the IKEA effect may impact their decision to enroll in a smoking cessation program. Therefore, our first hypothesis is
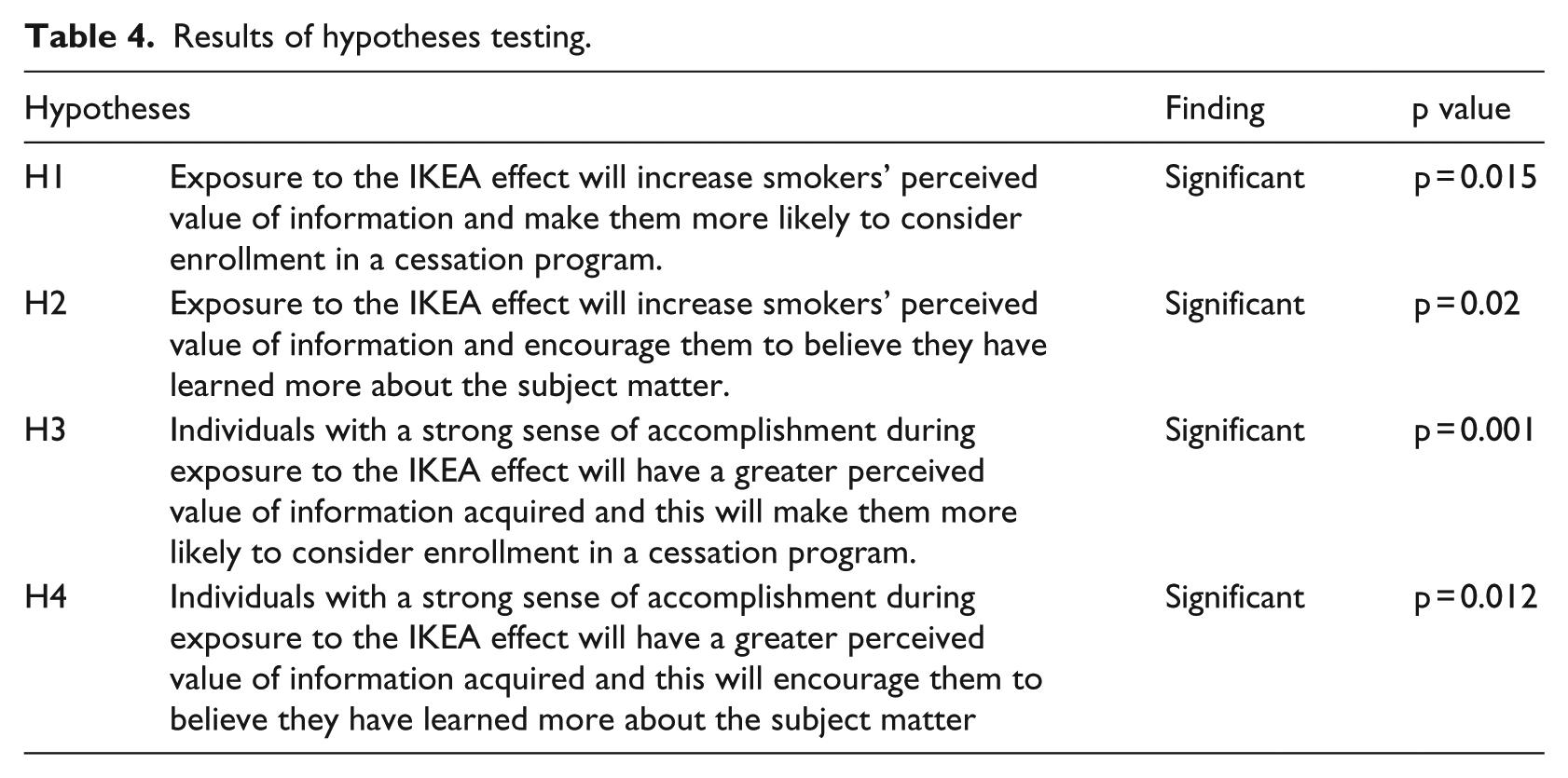
H1. Exposure to the IKEA effect will increase smokers’ perceived value of information and make them more likely to consider enrollment in a cessation program.
Smoking cigarettes has many health risks for everyone. However, starting at a younger age can result in more problems later. People who start smoking before the age of 21 years have the hardest time quitting. As reported by the US Surgeon General,
addiction caused by the nicotine in tobacco smoke is critical in the transition of smokers from experimentation to sustained smoking and, subsequently, in the maintenance of smoking for the majority of smokers who want to quit.
49
Further facts make this even clearer; for instance, 50 percent of adult smokers’ transition to regular, daily smoking before they turn 18 years. More than 75 percent transition to regular, daily smoking before the age of 21 years. Some students quit smoking before leaving high school but most will fail. According to a 2013 national survey by the US Centers for Disease Control and Prevention (CDC), 48 percent of current high-school smokers tried quitting but three out of four continue to smoke into adulthood, even if they intended to quit. 50
Although smoking cessation is essential and highly recommended, it is almost never determinant and smoking relapse tends to occur. Studies indicate that smoking cessation is not always permanent and one might go back to old habits by simply being in the presence of another smoker or smoking paraphernalia. 51 Bliss et al. found that most relapses occur within the first month after cessation and examined possible determinants of coping with the difficulty. We believe that participation in creation of smoking cessation material will make young adults more likely to change their minds about the importance of relapsing after cessation and therefore be more likely to take cessation efforts seriously. We believe that by participating in the creation of smoking cessation material, young adults are more likely to learn new information about smoking and its effects. This leads to our second hypothesis:
H2. Exposure to the IKEA effect will increase smokers’ perceived value of information and encourage them to believe they have learned more about the subject matter.
We also believe that the IKEA effect will have more impact among those who most strongly identify with the activity used for engagement and find it enjoyable as opposed to frustrating or unpleasant. For this reason, we also hypothesize in H3 and H4:
H3. Individuals with a strong sense of accomplishment during exposure to the IKEA effect will have a greater perceived value of information acquired and this will make them more likely to consider enrollment in a cessation program.
H4. Individuals with a strong sense of accomplishment during exposure to the IKEA effect will have a greater perceived value of information acquired and this will encourage them to believe they have learned more about the subject matter.
Methodology
Sample
The overall sample for this study consisted of Israeli smokers (n = 120). Of the 120, 60 were initial participants (known as the test group) and 60 were friends contacted by the participants (known as the control group). To ensure an even comparison, researchers made sure each of the 60 test group members was able to recruit a friend. Members of the test group were chosen randomly, without consideration of their personal characteristics, beside their status as a regular smoker. Several others chose to leave the study during the experiment. In all, 4 participants chose not to continue – 1 from the test group and 3 from the control group.
Procedure
Test group members were offered two options of receiving smoking-related information. The first option was to read articles related to smoking topics (health hazards, financial effects, and smoking cessation). The second option was to watch animation videos made by the researchers. These videos were created using a special video and presentation platform, relying on information from the same articles offered to the participants. These videos were validated by experts. The information videos that were pre-made can be viewed in the following links:
Health Hazards (https://www.youtube.com/watch?v=KmdwkfsH4uw)
Financial Costs (https://www.youtube.com/watch?v=UuTzBNaOiD8)
The Benefits of Quitting (https://www.youtube.com/watch?v=aDtNw_MJRMA)
All members of the test group chose the video option. After watching, subjects answered questions in a short online survey sent to their personal email. The next step for the test group was for researchers to apply the IKEA effect. In much the same way that past IKEA effect experimenters asked participants to create physical artifacts such as origami figures, 45 we asked our test group subjects to create their own short video using an online animation tool. This resulted in digital artifacts. Group members were given instructions to create a video about smoking to deliver a message of their choice. Since self-creation has been shown to be a key element in the IKEA effect, we determined that the participants needed to decide what message should be delivered. We did not want to direct their focus in any particular way. Following completion of their personal video, subjects were asked to obtain email addresses of friends who smoke and share the new video with them. The friends who agreed to participate in the study became the control group (57 of 60 friends). During this same time period, following artifact creation, each test group member was emailed a second survey with different questions about his or her will to cease smoking.
The control group first received a survey sent directly via email with their referrer’s personal video attached. The video included information about smoking much in the way that the control group received information prior to building an artifact. The survey was identical to the test group’s survey for easy comparison. Next, the control group received their own unique personal follow-up survey a few days after filling out the first survey. This survey inquired whether the control group’s participants desired to cease smoking and other questions. Since the control group had not gone through the IKEA effect process, we expected little indication of change within this group. Table 1 provides a summary of the activities in the experiment and the order in which they were completed.
Activity comparison between test and control groups.
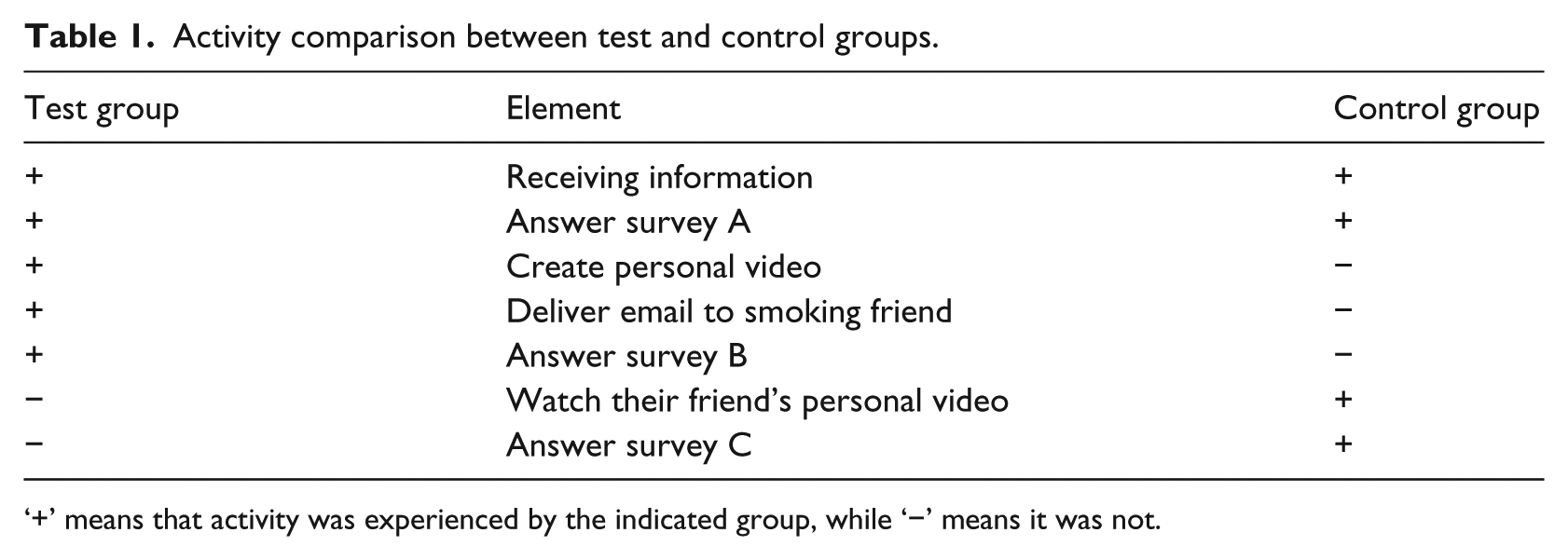
‘+’ means that activity was experienced by the indicated group, while ‘−’ means it was not.
A primary goal for this study was to determine whether the IKEA effect impacts behavior, particularly related to smoking habits and attitudes about smoking. For that reason, researchers induced behavior in the test group that should result in the IKEA effect as reported in past research. 45 As mentioned previously, the effect was stimulated during creation of short, personal animated videos. The videos were created with a popular online presentation and animation tool called PowToon. The tool has functionality similar to Microsoft Office PowerPoint and has a relatively low learning curve, but enough of one to engage the subjects, in the same way that increasing the complexity of an instant cake recipe tended to induce a greater sense of satisfaction in the housewives. 45 Each video consisted of various slides constructed and arranged by the test subject as a their personalized message. Eventually, the user was able to share her or his creation via online video sharing websites, such as Vimeo and YouTube. In some instances, the personal video was exported to social media platforms such as Facebook. Examples of the personal videos can be found in the following links on YouTube:
Figures 2 and 3 provide a glimpse of the PowToon interface. In Figure 2, the user is able to monitor the timeline, the screens of the video, and the name of the project and insert any desired text. In addition, on the upper right side, the user can export the video to YouTube or Vimeo. In Figure 3, the user is able to choose the way she or he wants the text to appear during the video. In addition, the user can use the tool bar on the right side to select any feature that will help create the video. Figure 4 provides a look at the PowToon layout screen. Figures 5 and 6 illustrate study participants working on video creation.

PowToon tool edit screen.

Video edit screen during creation of an animation.

The PowToon layout.

Creating the video in order to create the IKEA Effect in the test group.

Creating personal videos in order to stimulate the IKEA Effect.
Survey instruments
The surveys for this study were created using the Qualtrics platform. Once a survey was filled out, it automatically was saved on the Qualtrics online survey platform, which allows monitoring and analyzing of the respondents’ replies. The Qualtrics tool enabled designing and building the surveys with a logical flow. The stored data were exported to IBM SPSS version 20 and SAS 9.4 for analysis.
In general, the surveys were developed to appeal to the users. In the same way that the animations provided a message with a personal touch, the surveys were designed to avoid sounding clinical or formal using everyday language and incorporating a sense of humor.
Data items
The survey questions in this research were grouped into three categories. These categories included the following:
General characteristics
Smoking history
Quitting habits
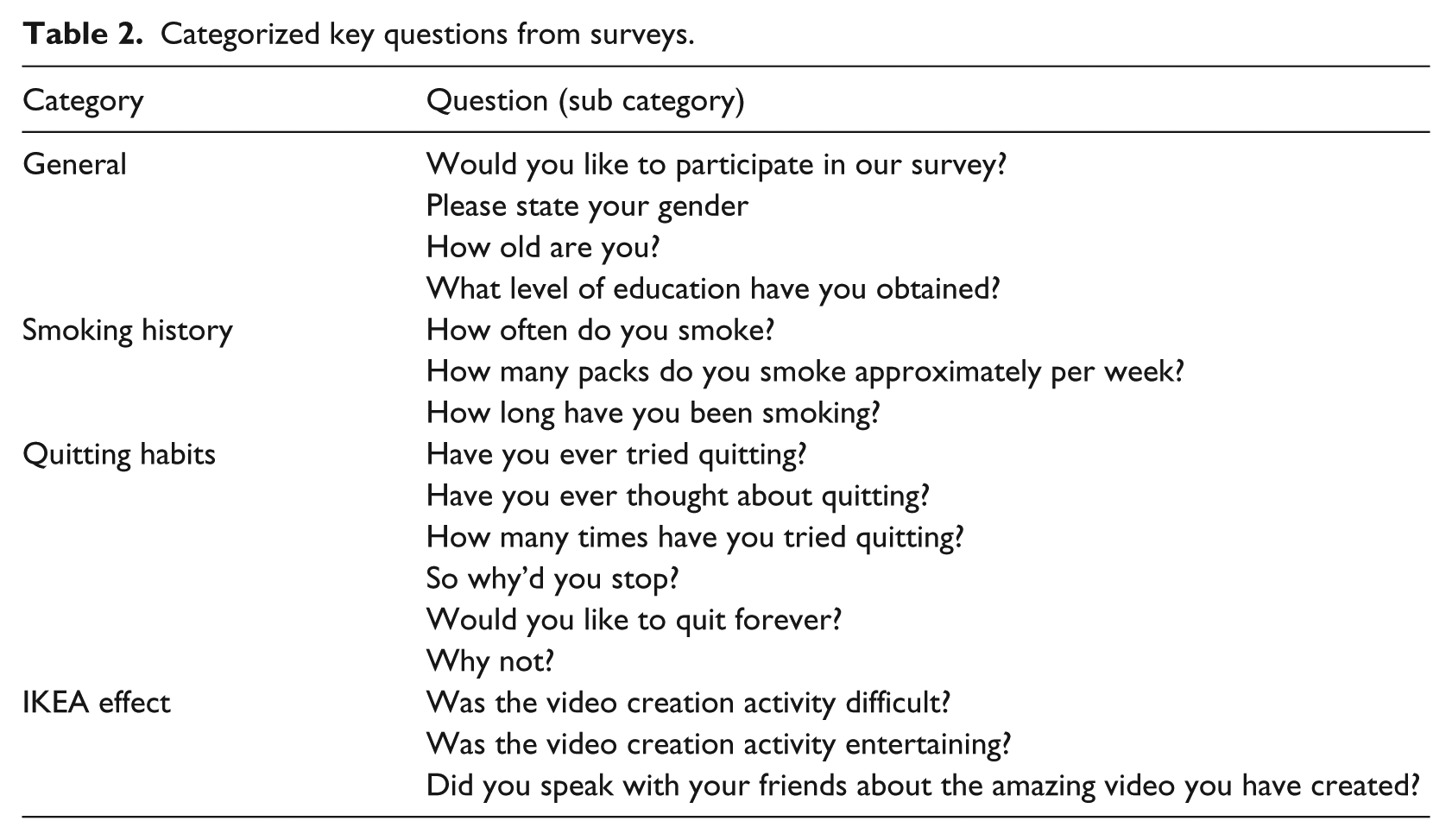
General characteristics refer to personal attributes of the research population. These items were collected using four questions for both the test and control groups. These questions were used to describe the research population and included gender classification (male/female), age (scalar), and education level (PhD, master, bachelors, high school or equivalent). Smoking history was defined in three ways: the frequency of smoking (occasionally or every day smoker), the amount of tobacco products being smoked per week (in amount of packs), and the number of years the participant has been smoking. These questions defined participants’ current smoking status and habits as well as personal history regarding the usage of tobacco products. 52 Quitting habits refer to the history of a participant’s quitting process and was determined by six questions shown in Table 2. This set of questions was derived from a prior study and asked to determine the participant’s past will to quit, 52 although other factors are known to exist. The strength of the IKEA effect also was measured among test group subjects. The IKEA effect questions were derived from Mochon et al.44,45 The effect was measured with three scale items which can be seen in Table 2.
Categorized key questions from surveys.
Results
Demographics
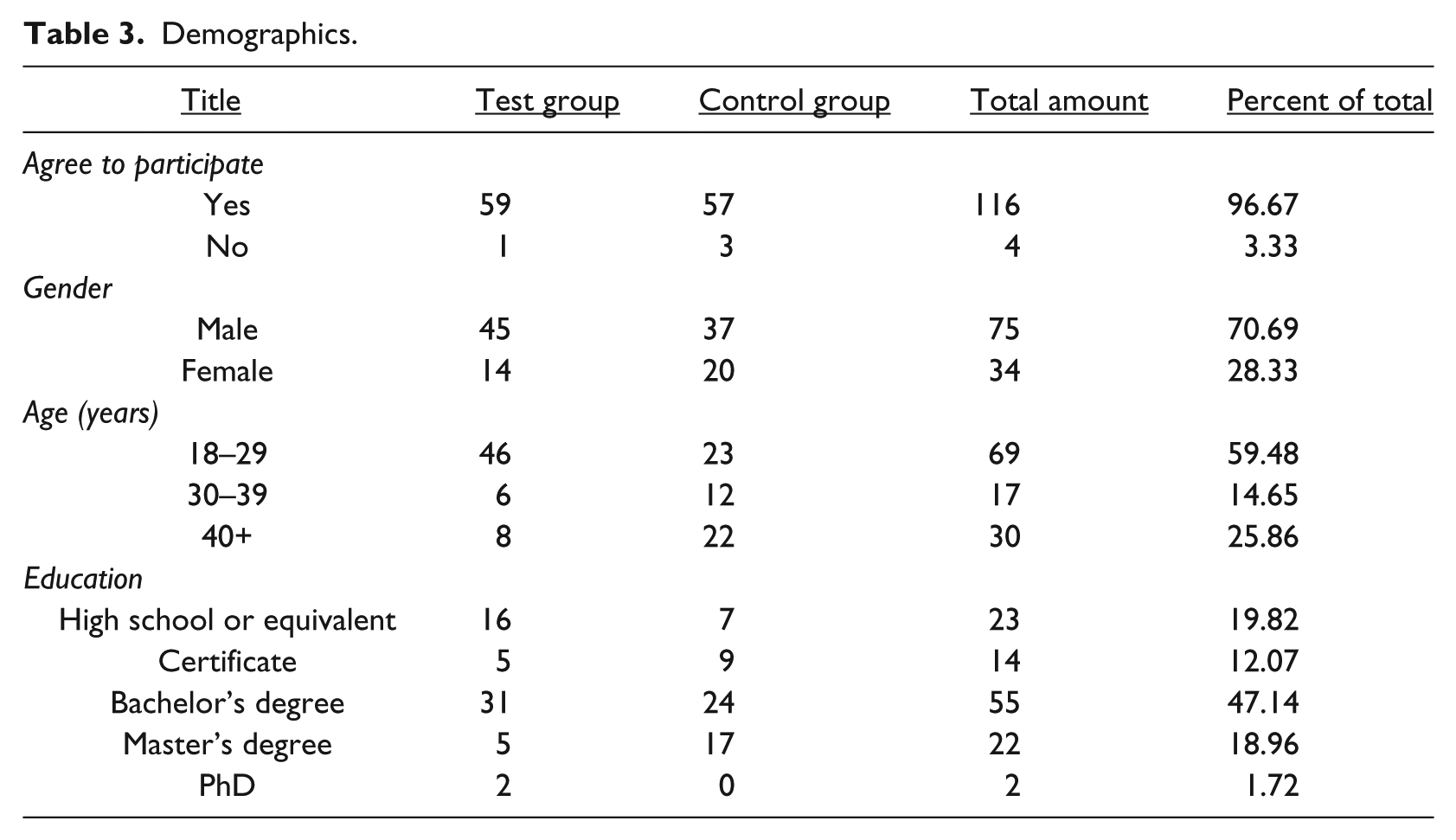
The data were collected and analyzed with IBM SPSS 20 and SAS 9.4 as mentioned earlier. There were no missing data in the dataset due to respondents being forced to answer each question in the survey. Table 4 shows the demographic characteristics of the respondents. Almost 60 percent (59.48%) were between 18 and 29 years of age, 15 percent (14.65%) between 30 and 39 years, while 26 percent (25.86%) were over the age of 39 years. The majority of respondents were male (70.69%). Almost all of the respondents had at least some college education (47.14% bachelor’s degree, 18.96% master’s degree, 1.72% PhD, and 12.07% professional degree). Some respondents had a high-school education or equivalent (19.82%). Several t-tests were conducted to determine whether significant differences existed between the composition of the test group and the control group. No significant differences were found due to demographics or general smoking characteristics. Table 3 provides a breakdown of both test and control group members.
Demographics.
Hypotheses testing
Statistical analysis was performed on data in support of the main hypotheses using SAS Version 9.4. Comparisons used the McNemar test which can be described as a cross classification of matched responses to a dichotomous item.53,54 The McNemar test is a type of chi-square test that uses paired data from a non-parametric sample. In this study, most of the data are binomial (e.g. yes or no answers to questions). McNemar also is recommended for use with samples that are not normally distributed. 54 The McNemar test also applies to multiple group designs and is well-suited for detecting significant changes in pre- and post-test scores for hypothesis testing. 55
Hypothesis 1
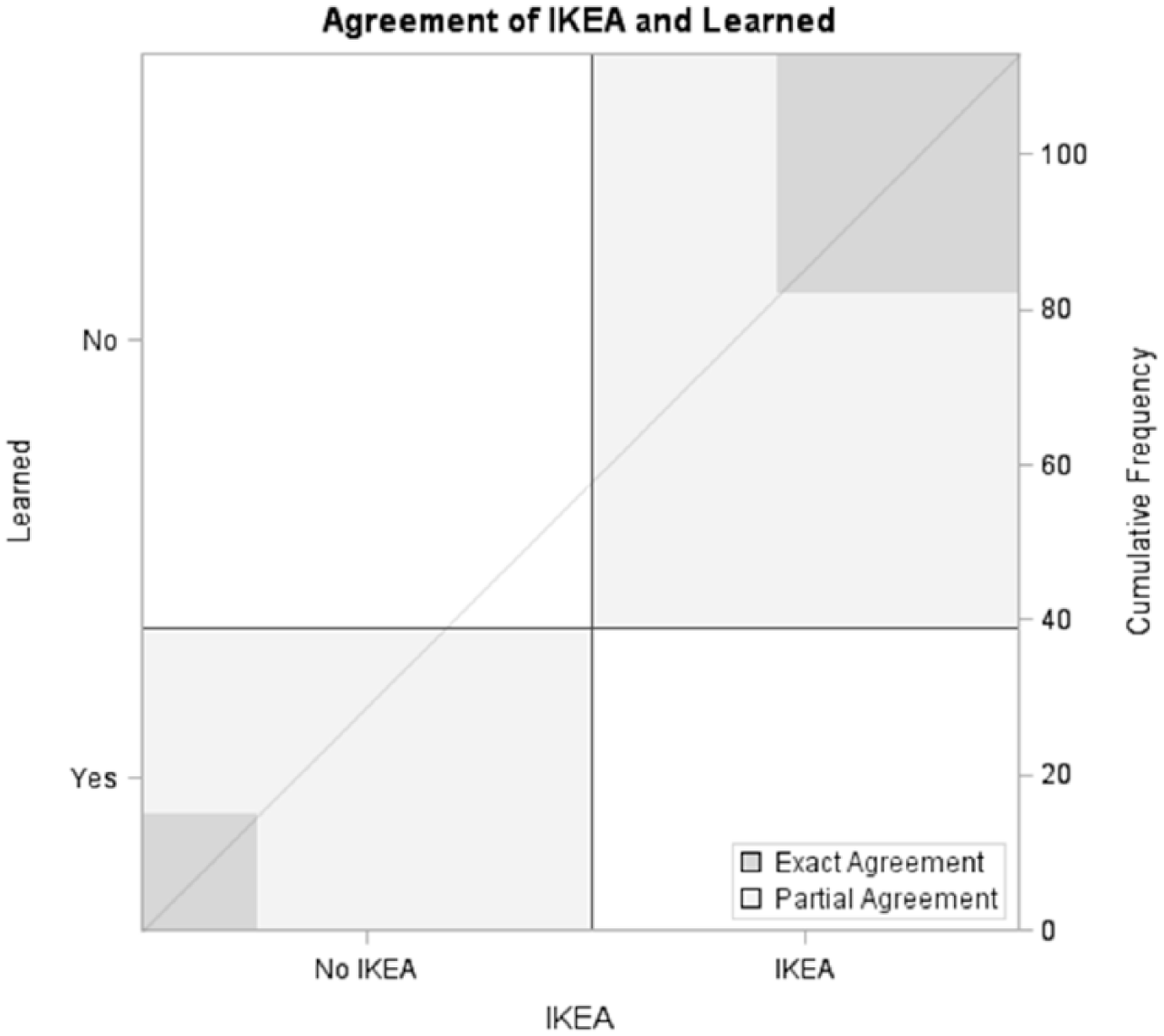
First, the data for H1 were examined to determine whether exposure to the IKEA effect increased smokers’ perceived value of information and made she or he more likely to consider enrollment in a cessation program. This analysis compared the test and control groups. The results were significant with McNemar’s chi-squared = 5.92, degree of freedom (DF) = 1, and p value = 0.015. Therefore, H1 was accepted. More subjects were willing to sign up for a cessation session if they had experienced the IKEA effect. Figure 7 provides a graphic view of the test result.

IKEA effect and likelihood of registering for cessation class.
Hypothesis 2
The data for H2 were examined to determine whether exposure to the IKEA effect increased smokers’ perceived value of information and made them feel as though she or he had learned something new related to smoking. This analysis compared the test and control groups. The results were significant with McNemar’s chi-squared = 5.39, DF = 1, and p value = 0.02. Therefore, H2 was accepted. Subjects who had been exposed to the IKEA effect were more likely to feel they learned something new about smoking. Figure 8 provides a graphic view of the test’s significance.
IKEA effect and perception of learning something new about smoking.
Hypothesis 3
The data for H3 were examined to determine whether perceptions of IKEA effect strength moderated smokers’ perceived value of information and made she or he more likely to consider enrollment in a cessation program. This analysis compared subjects within the test based on whether their composite score on the three items related to IKEA effect strength was high (e.g. above 6) or low (e.g. below 7). The results were significant with McNemar’s chi-squared = 10.9, DF = 1, and p value = 0.001. Therefore, H3 was accepted. Strength of IKEA effect significantly impacted subject willingness to sign up for a cessation session. Figure 9 provides a graphic view of the test result.
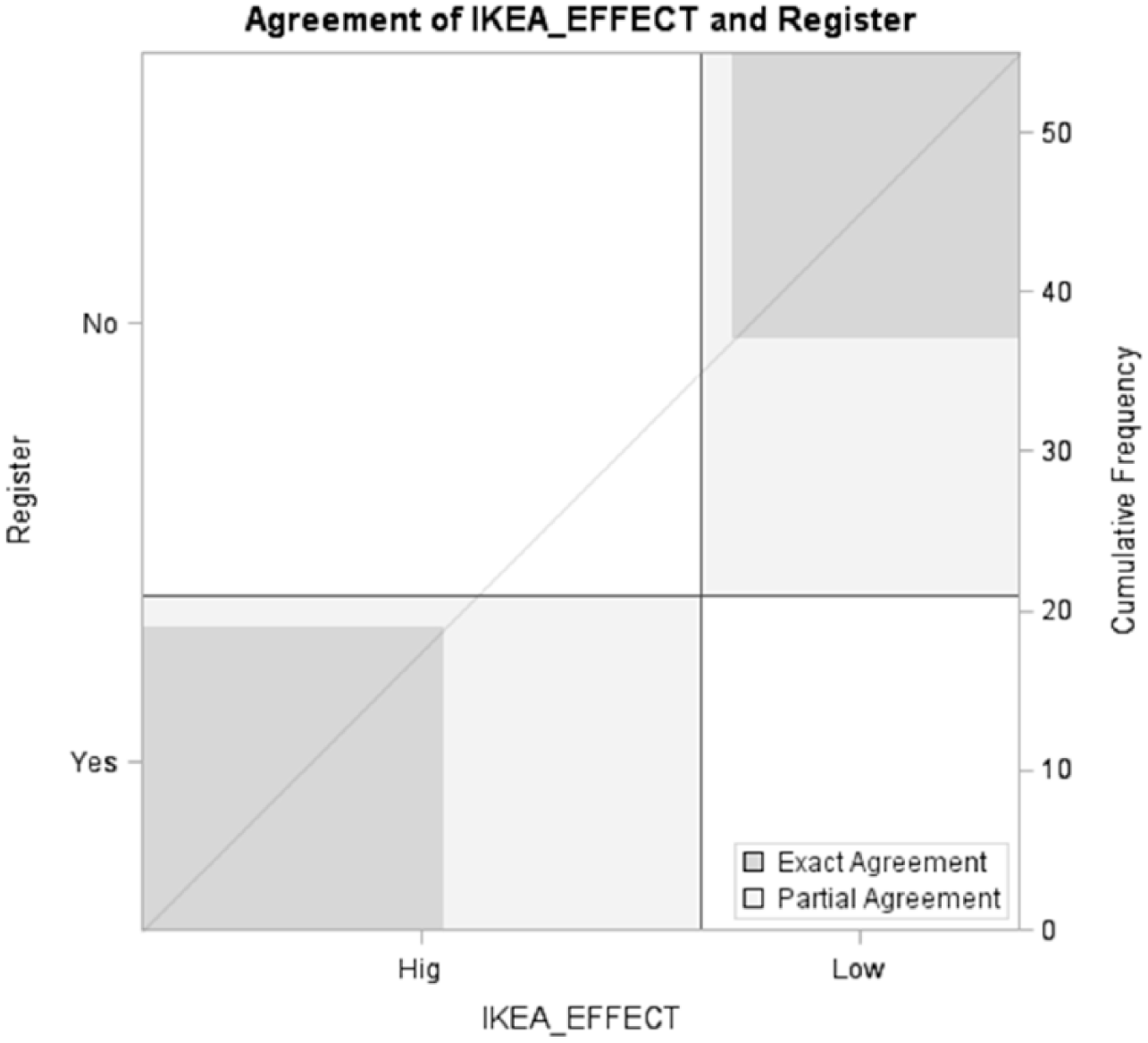
IKEA effect strength and likelihood of registering for cessation class.
Hypothesis 4
The data for H4 were examined to determine whether perceptions of IKEA effect strength moderated smokers’ perceived value of information and made them feel as though he or she had learned something new related to smoking. This analysis compared subjects within the test based on whether their composite score on the three items related to IKEA effect strength was high (e.g. at least a score of 7 out of 12) or low (e.g. a score no greater than 6 out of 12). The results were significant with McNemar’s chi-squared = 6.37, DF = 1, and p value = 0.012. Therefore, H4 was accepted. Subjects more strongly impacted by the IKEA effect were more likely to feel they learned something new about smoking. Figure 10 provides a graphic view of the test significance.
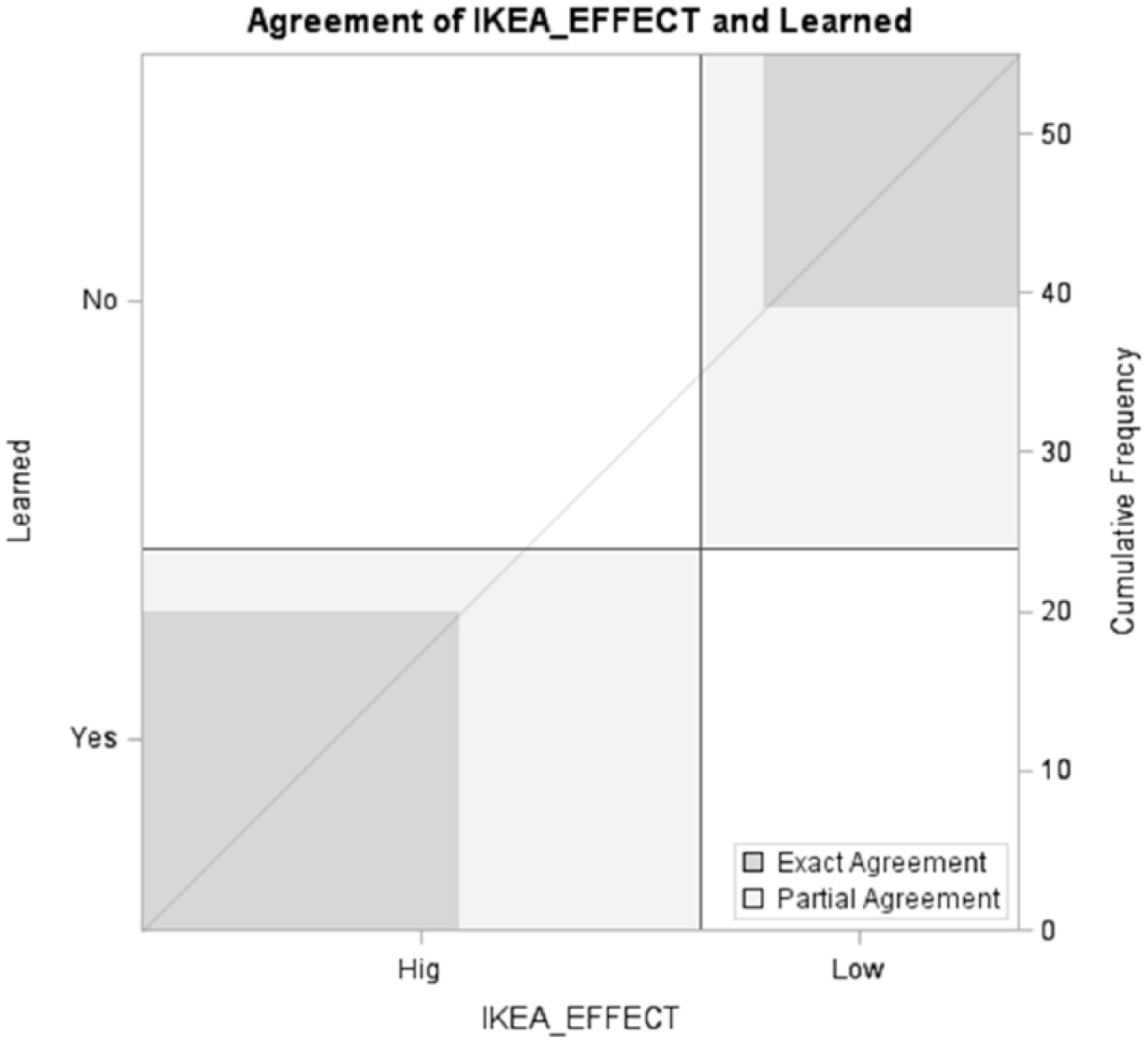
IKEA effect strength and perception of learning something new about smoking.
Table 4 provides a summary of the hypotheses testing.
Results of hypotheses testing.
Post hoc analysis
Past studies into smoking cessation have indicated that age may have a significant impact on outcomes.56,57 We conducted a post hoc analysis to determine whether that was the case in our collected dataset. We broke our sample into two groups: subjects 30 years of age or more and those below 30 years of age. No effect existed for age related to amount learned (p = 0.41) nor did it exist for willingness to register (p = 0.16). Several other age-related tests were conducted and none were found to be significant. The nature of the task may have been responsible for this outcome and may require more research to definitively understand this finding.
Discussion
The goal of this research was to investigate a novel approach for encouraging smokers to consider changing their habits in a way that results in better health. Prior research has indicated smoking cessation is a difficult process and involves many variables. While this study does not provide a panacea guaranteed to end smoking practices, it does provide another tool useful to health-care providers in their quest to convince the general public to make healthy choices. It also shows how current information technology can be used to effect change via the well-documented IKEA effect.
Our research study draws on the value-driven consumer e-health information search behavior model presented by Goetzinger et al., 41 and applies it to current needs for changes in modern health habits. This study incorporated the IKEA effect as a means of enhancing perceived information value by ensuring information that recipients became engaged in a creative activity. This helped inculcate the topic of smoking cessation and make the idea of smoking cessation more acceptable (H1). Likewise, in an information-rich society, it becomes more difficult to effectively acquire meaningful information due to surrounding ‘noise’ and information overload. We found that the IKEA effect focused information gathering, processing, and communication in ways that help the ‘creator’ acquire more knowledge on a subject—in this case smoking (H2). To ensure the IKEA affect was responsible for the outcomes, we ran additional tests to determine whether higher levels of engagement during the IKEA effect seemed to result in higher likelihoods of considering cessation program enrollment and learning new smoking-related information. In both cases (e.g. H3 and H4), this was found to be true. Engagement was measured with three questions: (1) whether the creative process of building smoking information was difficult, (2) whether the creative process was entertaining, and finally, (3) whether test subjects talked about the creative process with their friends. From prior literature on the IKEA effect, it was important not to direct the creative process too closely, nor was it advisable to select a process that was too easy. For this reason, the subjects selected a certain facet related to smoking and explained it. In many cases, we believed the subjects picked factors about smoking that concerned them and used the creative activity to explore and communicate what they had discovered.
With regard to Goetzinger et al.’s model, 41 information relevance and information clarity formed the approach to assigning the creative task to the test subjects. These concepts were used during the first stage of our research. The participants had to choose the way they prefer to receive the information—by reading articles related to smoking or by watching videos that were based on the same articles. All participants in the study test group chose video over articles and used this information in the creation of their PowToon artifacts. The data revealed the significance of the IKEA effect and how it affected change in the participants’ minds. The control group had access to the exact same information but did not engage in the creation process. As a result, they perceived less ‘new’ information and did not appear as willing to enroll in a cessation workshop.
We believe that our findings suggest that the combination of the normal information transfer techniques together with the IKEA effect can lead to a significant number of individuals being willing to consideration a cessation workshop. We do not suggest that consumer-created videos will influence others more than trusted public sources of information. Rather, we suggest that the act of creating an artifact from trusted information enhances its influence on the creators. Perhaps these results can also be applied to other related areas such as physical activity, better nutrition, and weight loss.
Research limitations
The composition of our test group was diverse but was drawn from a convenience sample of available subjects. Activities were held during different times of the day, and in different locations, such as homes, and university settings. Another potential limitation was the control group members. Since these individuals were recruited by the test subjects, we did not have complete control over their locations or demographics. Other limitations were related to the individuals themselves. The subjects came from a variety of backgrounds, households, and peer groups where smoking and cessation options might be influenced by factors unknown to the study. There were differences in the test and control groups related to gender, age, and education which also may have influenced the study outcomes. This was an exploratory study and therefore further rigorous investigation of the IKEA effect is recommended.
Future research
Many opportunities for future research exist. For example, it would be interesting to investigate whether the study subjects followed through and enrolled in smoking cessation workshops. If so, did they ultimately quit smoking? We also believe that further research on different behavioral habits and the affectivity of the IKEA effect on these habits should be investigated. In addition, we think that future research in this topic area should consider using a more controlled environment for the participants in order to avoid bias that might have been present in this study. Another potential research avenue would be to conduct similar research with test group participants divided into small groups. By adding a social dynamic to the IKEA, additional findings might be forthcoming.
Conclusion
Use of the IKEA effect can help an individual more carefully consider information related to his or her personal health. Our data support the idea that those more engaged in the creative process were more likely to perceive opportunities and available information in a way that can lead to better choices. Although the research focused on the health sector and smoking cessation in particular, we believe the use of the IKEA effect may be relevant to many more aspects of day-to-day life. We believe that the usage of the IKEA effect can increase the odds of success in many ways that need to be studied.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.