
Abstract
People living with Parkinson’s disease engage in self-care for most of the time but, two or three times a year, they meet with doctors to re-evaluate the condition and adjust treatment. Patients and (informal) carers participate actively in these encounters, but their engagement might change as new patient-centred technologies are integrated into healthcare infrastructures. Drawing on a qualitative study that used observations and interviews to investigate consultations, and digital ethnography to understand interactions in an online community, we describe how patients and carers living with Parkinson’s participate in the diagnosis and treatment decisions, engage in discussions to learn about certain topics, and address inappropriate medication. We contrast their engagement with a review of self-care technologies that support interactions with doctors, to investigate how these artefacts may influence the agency of patients and carers. Finally, we discuss design ideas for improving the participation of patients and carers in technology-mediated scenarios.
Introduction
People living with chronic conditions, such as Parkinson’s disease (PD), spend most of their days in self-care but, two or three times a year, they visit their doctors to discuss old issues, new challenges, and treatment adjustments. While consultations in chronic care are seen as collaborative, 1 there are different ways of participating in these encounters. 2 Some studies show that patients and doctors sit as equal partners in decision-making, in recognition of their specific expertise and commitment to an appropriate treatment,3–5 while other studies suggest that patients only provide input to the decisions of doctors.6–8 Either way, when given a chance to participate, patients and carers bring useful insights to the table and actively contribute to building a better quality of life for themselves. 9
The agency of patients and carers in care, or in other words, the ability to contribute, influence, and decide on treatment, is not dependent solely on their willingness to participate in interactions. As Suchman 10 explains, agency is inherently situated and tied to specific socio-material arrangements, which offer different capacities for actions. People living with Parkinson’s, for example, are usually motivated to participate in their care because of the ability to shape treatment according to their issues and aspirations. 11 Yet, their agency in care is often constrained by doctors who proceed under a paternalistic model 12 of care where patients are considered as mere informants incapable of participating in decision-making.2,13 Besides such prejudices of doctors, the agency of patients and carers is influenced by a multitude of human and non-human entities, which include the following: self-care technologies, information systems, standards, as well as everyday activities, clinical processes, and procedures. Together these entities form what we refer to as the healthcare infrastructure. 14
One factor that increasingly influences agency in care is new technologies. Since self-care technologies for interacting with doctors often introduce new care activities and redistribute existing ones, 15 they are likely to change the ways patients and carers interact with doctors. 16 Self-care technologies for interacting with doctors are defined here as tools that support data exchange or collaborative interactions between patients, carers, and doctors. There are self-care technologies that do not offer interactions with doctors, 17 but these are not considered in this article. Self-care technologies for interacting with doctors appear in the literature under different names, including Telehealth, 18 Telehealthcare, 19 or Telecare. 20 The term Telemedicine is also used,21,22 but the overlap is restricted as Telemedicine also includes tools for supporting collaborations between healthcare practitioners. By using the expression self-care technologies, we emphasise the role of patients and carers in medical care, in opposition to terms such as Telehealth or Telecare that suggest care is remotely provided to patients, driven from a clinical perspective.
Previous research in human–computer interaction (HCI) and computer-supported cooperative work (CSCW) has explored numerous self-care technologies to support interactions with doctors, from videoconferencing systems for interacting with doctors remotely,21,22,23 technologies for collecting symptoms at home, 24 and apps for learning about one’s body in everyday life. 25 Nevertheless, due to the complexity of this topic, HCI and CSCW researchers are still discussing how best to enable patients and carers to participate in their own care and what sorts of healthcare infrastructures could support more participatory interactions. 26
This article contributes to the discussion on the agency of patients and carers in technology-mediated care scenarios. In particular, we contrast the agency of people living with Parkinson’s within current healthcare infrastructures, with the participation that is promoted in self-care technologies for interacting with doctors. For understanding existing healthcare infrastructures, we draw on interviews, observation, and online ethnography, and for investigating the agency promoted by self-care technologies, we review technologies published in scientific venues and the iTunes App Store. Our findings show that patients and carers living with Parkinson’s are very proactive, and that they play an important role in defining diagnosis, medical decision-making, learning, and addressing inappropriate medication. The review of self-care technologies shows they have potential to improve the agency of patients and carers, but in some cases, also present obstacles to their participation. We use our findings to discuss the agency of patients and carers in healthcare infrastructures and present implications for design to promote an active participation in technology-mediated care scenarios.
Methods
This article draws on two complementary studies. First, we examined how patients and carers interact with their doctors in consultations and in an online community. Second, we reviewed descriptions of self-care technologies for interacting with doctors, in search for understanding the role patients and carers can play in their care using them. The goal was to contrast the agency patients and carers had in their care in different scenarios.
Ethnographic fieldwork
To better understand the encounters between patients, carers, and their doctors, we analysed two different settings in two distinct care contexts. The first one consisted of face-to-face consultations of people living with Parkinson’s with their specialist in a European city. The second consisted of online conversations between patients or carers with doctors in a US-based online community or forum. The choice of using different contexts and settings was motivated by the possibility to compare field data and thus improve the depth of analysis. As Glaser and Strauss 27 explain, maximising the differences between groups in the data collection can help uncover meanings or assumptions that might otherwise be taken for granted.
To understand the existing healthcare infrastructures and gain broader insight into living with Parkinson’s, we used observations and interviews.
Observations
To understand consultations of people living with Parkinson’s, we observed 14 sessions at a neurology outpatient clinic in a major hospital in Portugal (the observed participants are named using a code. For example, OP5 refers to the patient on the fifth observation). The observation spanned several days and was always held in sessions with the same neurologist. The 14 sessions were with participants we recruited from the waiting room while they were waiting to see this doctor, and who agreed to let us sit in on their consultation. As such, the observation was divided between two rooms of the clinic. In the waiting room, the participation level of the researcher was moderate, 28 balancing between being an insider waiting in the room, and being an outsider who asks questions to patients and carers who are about to see their doctor. At this point, discussions with the participants were captured in hand-written field notes. In the consultation room, the observation was passive, with the researcher behaving as a spectator and not interacting. The consultations were audio-recorded (5 h), and later transcribed verbatim for analysis. Moreover, we obtained informed consent from participants and ethical clearance from the hospital ethics commission.
Interviews
To complement the understanding of consultations, we interviewed another 10 patients and 10 carers living with Parkinson’s (the interviewed participants are named using a code. For example, IP1 refers to the first interviewed patient, and IP10_C1 to the first carer of the interviewed patient 10). The interviews were intense, 29 qualitative, and loosely structured. The interview guide covered issues such as diagnosis, treatment, consultations, and overall everyday life. The interviews were audio-recorded (20 h) and transcribed for analysis. Participants were recruited through a local chapter of the Portuguese association of patients with Parkinson’s in an urban town. We obtained informed consent from all interviewed participants.
To understand the interactions between patients, carers, and doctors in a different context, we used online ethnography 30 in an online community.
Online ethnography
The community chosen was the National Parkinson’s Foundation (USA) online forum that offers a range of different sections including the following: ‘Newly Diagnosed’, ‘Caregivers Forum’, ‘DBS Forum’, or ‘Ask the Pharmacist’ (available at: http://forum.parkinson.org/). For this study, we focused on the ‘Ask The Doctor’ section where patients and carers could ask questions about their particular case to a handful of specialised volunteering neurologists from the association. A total of 800 posts from the online community were read using a standard web browser, and when relating with data that appeared relevant, copied and coded in ScrivenerTM (n = 332). We chose to analyse older threads of the forum, with closed conversations, and thus screened posts from 2007 to 2012. The posts in the online forum were publicly available and the names of patients anonymised (appearing as Guest__*), so we present them as they were online.
The analysis of the fieldwork followed a constructivist grounded theory approach. 31 In particular, we coded iteratively, constantly compared different excerpts, and regularly wrote memos about the emerging themes. We used the Scrivener writing software for collating relevant excerpts and writing memos. The data from the different methods was initially analysed separately and resulted in larger categories such as becoming a patient, self-managing Parkinson’s, collaborating in self-care, learning to live with the condition, and interacting with doctors. However, as the theme around interacting with doctors grew overall, we decided to approach it more systematically and merge the codes from the different methods together. The codes emerging from the more selective coding coincide with the headings in the findings discussed below.
Review of self-care technologies
We contrasted the fieldwork with an analysis of self-care technologies for people living with Parkinson’s to interact with doctors. Our focus was on how these technologies promoted participation of patients and carers in these care scenarios. The idea was not to be comprehensive and include the whole spectrum of self-care technologies, but rather to acquire an overview of the potential offered by these technologies.
To locate relevant technologies, we used different search strategies:
We searched for ‘Parkinson’ in HCI Bibliography – the main index aggregating HCI/CSCW research – and also in relevant journals in (bio)medical informatics, including Health Informatics Journal, International Journal of Medical Informatics, Journal of American Medical Informatics Association, Journal of Biomedical Informatics, Journal of Biomedical and Health Informatics, Journal of Medical Internet Research, and Journal of Telemedicine and Telecare;
We searched for ‘telecare’, ‘telehealth’, ‘eHealth’, and ‘self-care technology’ in the archives of the Movement Disorders journal, the key venue for research on Parkinson’s. We also followed the citations of the studies that we selected;
We searched for ‘Parkinson’ on the iTunes App Store for capturing technologies, that while not published in academic studies, patients and carers could access on their smartphones.
The criteria for inclusion in the review were technologies for patients or carers living with Parkinson’s that supported face-to-face or remote interactions with their neurologists. Our analysis was based on the descriptions that the research articles or web pages made about the technologies. This included features, ways of operating, and the expected interactions between patients, carers, and their doctors; this all helped in getting an understanding of the potential agency that patients and carers would be able to exercise when using them. Moreover, in the case of self-care technologies described in research papers, we also analysed the findings related with their use, mostly in feasibility studies, as another source of input to understand agency in care. Analysing technologies by their description does not reveal the same results as observing their use in practice because users might appropriate the technologies in unexpected ways, consequently promoting or hindering the agency of patients and carers in care. However, in the absence of detailed pilot studies of these technologies, there is still much to learn from their descriptions, because technologies influence greatly how people can interact, and their potential to exercise agency in care.
Interactions between people living with Parkinson’s and their doctors
Parkinson’s disease is a progressive chronic condition that impacts the neurological system. 32 It is characterised by four main symptoms: rigidity in the muscles, slowness of movement, impairments in the gait, and the most well known, tremor. Non-motor symptoms are also common and include depression, pain, and sleep disturbances. PD does not have a cure yet, but there are some medications that can attenuate the symptoms of the condition. Living with Parkinson’s is complex and requires significant work. The self-care of Parkinson’s includes 33 taking a cocktail of medication at specific times, exercising to keep muscles fit and stimulate areas of the brain, adapting lifestyle to increasing disability, and accepting the current and future state of the condition.
Two or three times a year, patients and carers have a chance to discuss their issues with the neurologist and collaboratively adjust treatment. These occasions are critical for people living with Parkinson’s (we use the expression ‘people living with Parkinson’s’ in this article to refer to the collective formed by patients and carers. All of them live effectively with the condition, even if the carers do not experience it directly in their body 33 ) because changes in medication can promote or hinder patients from performing specific activities. As the medication for Parkinson’s is solely concerned with addressing the symptoms of the condition, being able to articulate well one’s issues and discuss possible solutions is thus key to achieve a life with the quality that one aspires to. The medical care of PD can involve doctors, nurses, therapists, and other healthcare personnel. However, in this article, we discuss solely the interactions with doctors as they are the ones involved in neurological consultations and, consequently, the potential users of technologies for that context.
In this section, we explore the interactions patients and carers living with Parkinson’s have with their neurologists. In particular, we refer to five different interactions: (1) making explicit issues of concern, (2) evaluating movement, (3) discussing treatment adjustments, (4) getting an understanding of what to expect, and (5) getting inappropriate medication revised. These categories will now be described in detail.
Making explicit issues of concern
Many symptoms of Parkinson’s can be softened or removed using the right medication cocktail, so patients and carers carefully monitor the issues that appear and, during in-clinic consultations, report them to doctors. Neurologists support patients and carers in this task by asking questions such as ‘How are you doing?’, ‘Can you do everything you need in your day-to-day life?’, and ‘Do you need help from others for performing specific activities?’. In online exchanges, patients and carers usually express their concerns in the posts they publish, but doctors also prompt for additional information about the everyday experience. In both cases though, patients and carers are the ones defining the focus for the discussion and diagnosis, or in other words, what is important to address (or not) by what they mention to doctors. The word diagnosis is used here to name the identification and investigation of the causes of patient’s issues. As Arriscado Nunes et al. 34 explain, diagnosis is not only about getting a name for the condition but also addressing the agenda that the patients (and carers) bring to the consultation. In the case of Parkinson’s medical care, finding out the condition name is usually an activity that is held in the first encounters, but after that is settled, diagnosis becomes about understanding which of the identified symptoms and signs is indeed an issue for everyday life, and what are the causes of such problems.
Knowing what is an issue for Parkinson’s is not straightforward. As Parkinson’s affects the brain, its symptoms and signs appear in multiple areas and influence different functions. Furthermore, people have to investigate the issues caused by the condition, as well as the side effects of the medication. Issues related with Parkinson’s include not only movement problems such as tremor, or gait impairment, but also depression, delusions, and impulsive behaviours that one would not normally associate with a ‘movement disorder’. Thus, patients and carers adopt an attitude of actively investigating the issues they are faced with to understand whether and how they can address them:
When I have a slow movement problem I cannot walk slowly in a crowd in front of me, but I can walk very fast around them and continue to walk at a rapid pace, if I slow down to try to walk normally I can only maintain a turtle pace. Is this a common experience in movement disorders in beginning Parkinson disease? (Guest__*)
This patient asked whether the gait issues they experienced when walking around others were caused by Parkinson’s. In the reply, the doctor confirmed that this was an issue of the condition and that it could be fixed with medication adjustments. Interactions like these were frequent in the forum. Posting questions in the online platform enabled the patient to get some sense of direction on how to act regarding this issue. However, it is important to note that writing a post was often the last of a long line of actions by the patient (or carer). Before that, we can assume that the person was carefully observing the issue, comparing different situations, and reflecting on whether it always happened at the same time. This investigative attitude was essential if patients were to have their treatment optimised to their needs.
Having identified an issue, patients and carers make their own judgment about whether it should be addressed with treatment changes:
OP5: I always wake up at 4 in the morning to go to the toilet. I have nights in which I have … My legs get very heavy, they hurt, and I have to get off the bed to cool them down. Then, I return to bed. Dr: And then you can sleep, right? OP5: I can sleep then. Dr: You can sleep then. OP5: These are little details. I don’t think it is worth changing the medication [because of them].
This patient has issues in the legs at night but does not think they are worth addressing with medication adjustments. At first sight, refraining from treating a disturbing symptom could sound masochistic, but on a closer look, the excerpt reveals great reflection about the leg issue. The patient knows that there is no ‘silver bullet’ in the treatment of Parkinson’s; adding more medication might improve the leg issues, but bring other problems as well. In the whole picture, the leg issues are minor problems, ‘little details’ as the patient calls them. She can still perform most daily activities satisfactorily, so trying out a new medication scheme does not seem like a requirement for her at the moment, especially when it might entail other consequences.
Evaluating movement: refraining from hiding symptoms and documenting unobservable issues
In complement to the issues reported by patients and carers, doctors also observe the body of the patient during consultations. Part of the observation is unstructured and happens throughout the appointment. However, at some point during the consultation, the doctor performs the neurological examination, a more structured movement assessment. The examination is not the same for every patient but usually includes walking along the corridor, being pulled backwards while standing (‘pull test’), moving the elbow back and forth, opening and closing the hands fast, touching the finger alternately to the doctor’s and one’s nose, and following the finger of the doctor with the eyes. While observing the patient move, the doctor evaluates the rigidity of the muscles, symmetries in the body, difficulties in coordination, presence of tremor, gait impairments, and other characteristics of the condition. The doctor guides the neurological examination, but patients play an active role by letting their symptoms be visible (symptoms they might hide in everyday life), and by complementing the assessment with verbal details that cannot be observed.
Some symptoms of Parkinson’s bring unwanted attention to the patient, so people learn to mask and hide their issues from others. Tremor is a common example of a symptom that people usually try to hide. However, during the movement assessment, people need to refrain from hiding their symptoms for the doctor to be able to observe them at their full potential:
Dr: Now let’s walk, with a fast pace, until the end of the corridor, ok? (OP8 walks) Dr: You can come back, now. OP8: This hand is misbehaving [trembling]. […] If I press my hand it stops. Dr: No, let yourself relax.
While walking, the hand started to tremble, and the patient began hiding it by pressing the hand. The doctor quickly asked the patient to relax and let his hand shake as she needed to observe the symptoms in all their strength. Here again, the contribution of the patient is essential to ensure that the doctor can gain useful information and that care is appropriate. Unless the person refrains from hiding the symptoms, the result of the movement assessment will be misleading. However, if the actions of both patients and doctors are aligned, the assessment can inform medication adjustments.
Signs and symptoms are not always easy to observe. Sometimes, they only happen in specific circumstances that are not available in the doctors’ office (e.g. walking around a crowd, as shown in the previous section). Other observation difficulties occur in the initial phases of the condition if Parkinson’s signs and symptoms are subtle:
Dr: There is something I would like you to tell me. Before taking Madopar or Sinemet, because they are equivalent, were you better or worse? OP2: You know … I was never very [better]. At least, it did not seem to me. Dr: So we are going to do it like this. I am going to remove the medication. You’re going to get off the medication around one week before the next consultation. I will make a plan to show you how to do it, ok?
The patient in the excerpt has some symptoms that could be caused by Parkinson’s, but they could as well be due to the medication she has taken for years for another mental illness. When faced with Parkinsonian symptoms, neurologists usually prescribe Levodopa to patients. If they get better, people probably have Parkinson’s. If they don’t, the condition might be a different one. In this specific case, improvements were not clearly visible to the doctor via the neurological examination. So, the neurologist asked the patient whether she had noticed overall improvements since starting the medication. This feedback was essential, as the doctor could not observe the subtle changes felt in the activities of daily life. The observations of patients and carers provided the information to make a decision, which in this case is to stop taking the medication and re-evaluate the symptoms in some weeks.
Discussing treatment adjustments
One of the most significant moments of consultations is the discussion of treatment adjustments. During this exchange, patients, carers, and doctors agree on the medication to take during the next months and, as a consequence, define the activities patients will be able to perform. Doctors propose treatment options considering the needs of the patient, existing medications, and their previous experience with other patients. However, these suggestions are carefully scrutinised as only people living with the condition can assess whether they make sense:
If I increase the dosage of Stalevo my movement problems improve, but I get dyskinesias. […] Because the 150 mg [pill] improves my gait significantly, but the problem is the dyskinesias. And so she [the doctor] reduced from 150 mg to 100 mg but shortened the intake period. I feel better with that [regimen]. (IP2)
In this excerpt, the patient reflects about two recent medication plans and concludes that he ‘feels better’ with the latest one. With that regimen, the dyskinesias disappear, and the walking is almost at its best. There are no straightforward treatment options for Parkinson’s. Choosing the right medication, as Solimeo
35
explains, is an exercise of finding balance in abilities and side effect that is different for everyone. In any case, people living with the condition will be the ones weighing the various options provided by the doctor and choosing which direction to follow. Sometimes, they will even choose paths that are against the doctor’s recommendation:
Dr: You have a big gap between 8:00 and 15:00. This is even shameful [for me], but that is how Sir […] likes to do it, right? OP3: I have been doing it as the doctor instructed me. Dr: No, I did not instruct you to do it like this. We ended up adjusting it in this way. This is a difference of 7 hours, right?
This patient has a large interval between two medication intakes. Instead of the typical 3–4 h interval to keep the effect lasting the day, this patient has 7 h between two of his intakes. For the doctor, this interval is too long and inappropriate. For the patient, however, the medication regimen works just fine. He can do the activities he wants, and the regimen fits well with his routines, so from his perspective, there is no reason for changing it. The doctor tried to give arguments for making an adjustment, but as the patient finds it appropriate, ‘and he is the one living with it’, the doctor refrained from further persuading the patient to change.
Getting an understanding of what to expect
In consultations or online exchanges, patients and carers try to understand and prepare for their future situation. This includes understanding how the condition will evolve, the potential a treatment has, and whether they will be able to pursue their activities in the future. Doctors provide information, but it is the people living with the condition who seek to inform and prepare themselves. The insights patients and carers acquire are valuable to them as they enable them to prepare their self-management for when these future situations arrive:
Guest__*: It seems to me that a lot of the PD meds cause drowsiness. Do most PWP [people with Parkinson’s] continue to work full time jobs while being on the meds or do you find that most PWP usually cut back on work dramatically or quit altogether? thank you, MJ Dr Okun: This is a mixed bag. Many PD patients continue to try to work but must reduce hours, stress and anxiety which can all make symptoms worse. Many PD patients also find it hard to work after the 5th year of the disease, but this is highly variable as I have patients still working at year 20!
This patient (or carer) went online to ask whether patients with Parkinson’s continue to work after starting medication. They know medication can cause drowsiness, and people might be too sleepy to concentrate or keep their eyes open. In reply, the doctor explained that some people quit their jobs while others continue with reductions in their schedule. Knowing this information helps this person prepare for the future. In case she is a patient, these insights help her in preparing to cut hours on her current job, or even finding a new one, should cutting hours be impossible. In case this person is a carer, knowing about these possibilities can encourage her to help the patient manage this loss and prepare for her own work re-arrangements. The question posed might be read as a general interest question, but the consequences of having it answered have a significant impact on daily life.
Besides the progression of the condition, people also try to understand what to expect from their treatments:
Guest__*: I’m currently taking .5 mg Selegi[li]ne 2×/day and 2 mg Requip 3×/day. I am not experiencing any noticeable side effects on this dosage. My Neurologist says we can increase the dosage substantially slowly over time. Is it likely that on increased dosages of Requip that I will experience side effects of the drug? Dr Fernandez: It is possible that you will experience side effects, but it is possible also that you will not. The only way to find out is to try it, right? I personally do not go lower than 3 mg three times per day with my patients. […]
The patient asked in the forum whether they would experience side effects with a larger dosage of the medication. In reply, the doctor put things into perspective and even mentioned that the patient was on a very low dosage, smaller than the one he would initially suggest to his patients. Side effects might never materialise, but reading medication leaflets packed with potential side effects might be daunting, and so referring to the forum was a way to get some answers quickly. In asking the question, this person received information that might help planning the future. Common to both excerpts is the agency of patients and carers in understanding and preparing their self-management for the future.
Getting inappropriate medication revised
The medication for Parkinson’s is very sensitive. Too little of it and the symptoms will not be softened, and if medication is too much, it can lead to side effects. For this reason, medication should be carefully adjusted. However, sometimes, the medication regimen will bring more unwanted than beneficial effects and need to be adjusted before the next consultation – up to 6 months away:
Guest__*: […] I use lately 2 mg Mirapex, 3× a day at each meal, breakfast, lunch, and dinner, for a total of 6 mg per day. I have lately developed strong swelling of the ankles. My question is: Can this swelling be due to the Mirapex? I have no heart problems and I am sure it is not due to the heart. Dr Rodriguez: Very likely is a result of the Mirapex and if bothers[o]me you will need to stop the medication or at least reduce the dosage (try 1.5 mg tid).
This patient recently increased the medication dosage and around the same time experienced swelling in the ankles. These events seemed connected, so the patient went to the forum looking for confirmation. The doctor explained that the swollen ankles could be due to the medication and suggested adjustments to ease the swelling until the patient could reach the doctor.
The Portuguese patients we interviewed and observed did not use online forums but had other ways of getting their medication adjusted:
We call the doctor and she … It is not easy getting her on the phone. But she [says:] take this or take that. She changes medication, over the phone, she does. (IP10_C1)
Also, in this case, people were able to get their medication adjusted before the next consultation. As the medication plan brought unwanted side effects, they phoned the doctor, discussed the adjustment, and implemented changes. The participants we interviewed also mentioned that sometimes they went directly to the hospital to address the problems in the medication. What is common between these examples is that patients and carers proactively created a way to access the doctor’s advice between consultations. By using the forum, the doctor’s mobile phone, or by visiting the clinic earlier, patients and carers created an alternative channel to access care and to ensure necessary adjustments would be timely.
Playing an active role within the healthcare infrastructures
The fieldwork showed that patients and carers exercised a very active agency in their interactions with doctors. They helped define diagnosis, engaged in discussions about treatment adjustments, directed learning to certain topics, and acted when medication adjustments were inappropriate. Their active agency was not a coincidence of circumstances, but rather a consequence of the socio-material arrangements where they acted.
While at home, patients and carers carefully investigated issues that appeared. They compared between different situations, reflected on their differences, and considered whether they were worth addressing with medication adjustments. Patients and carers also reflected on which activities and routines were important to keep, and which ones could be stopped or adapted. These engagements helped people enlist issues, priorities, doubts, or other topics to potentially bring up in consultations.
But to actually bring up these issues while interacting with the doctor required that the doctors provided an interactional dynamic that invited and enabled people to be able to raise issues, discuss solutions, and steer discussions to certain topics. Had doctors aligned with a more paternalistic model of care, these engagements would have been much briefer and disconnected from the agenda of patients and carers. It was also important that patients had access to the mobile phone number of the doctor or the online community to be able to adjust inappropriate medication.
Self-care technologies for interacting with doctors
Having analysed how patients and carers currently interact with their doctors, our analysis now shifts to self-care technologies for interacting with them. These technologies influence the role people can play in care, by the features, interactions, or roles they offer; thus, investigating them can help understanding the sort of agency patients and carers will potentially exercise if these technologies are integrated into healthcare infrastructures.
Overview
The review resulted in a total of 15 self-care technologies for interacting with doctors. From this set, eight were published in scientific journals and conferences from the years 2006 to 2014 and the remaining seven found through the iTunes App Store.
The self-care technologies in the review can broadly be categorised as either tools that enable remote consultations through videoconference or technologies that enable some sort of tracking practices and, for that reason, contribute to interactions with the doctor. Table 1 analyses the features of the technologies in terms of how they capture and present data, and how they facilitate sharing of data and interaction with the doctor. We go on to discuss how these technologies support some of the key aspects we found in the fieldwork for exercising agency: investigating issues, participating in discussions, and adjusting medications.
Characteristics of the self-care technologies for interacting with doctors.
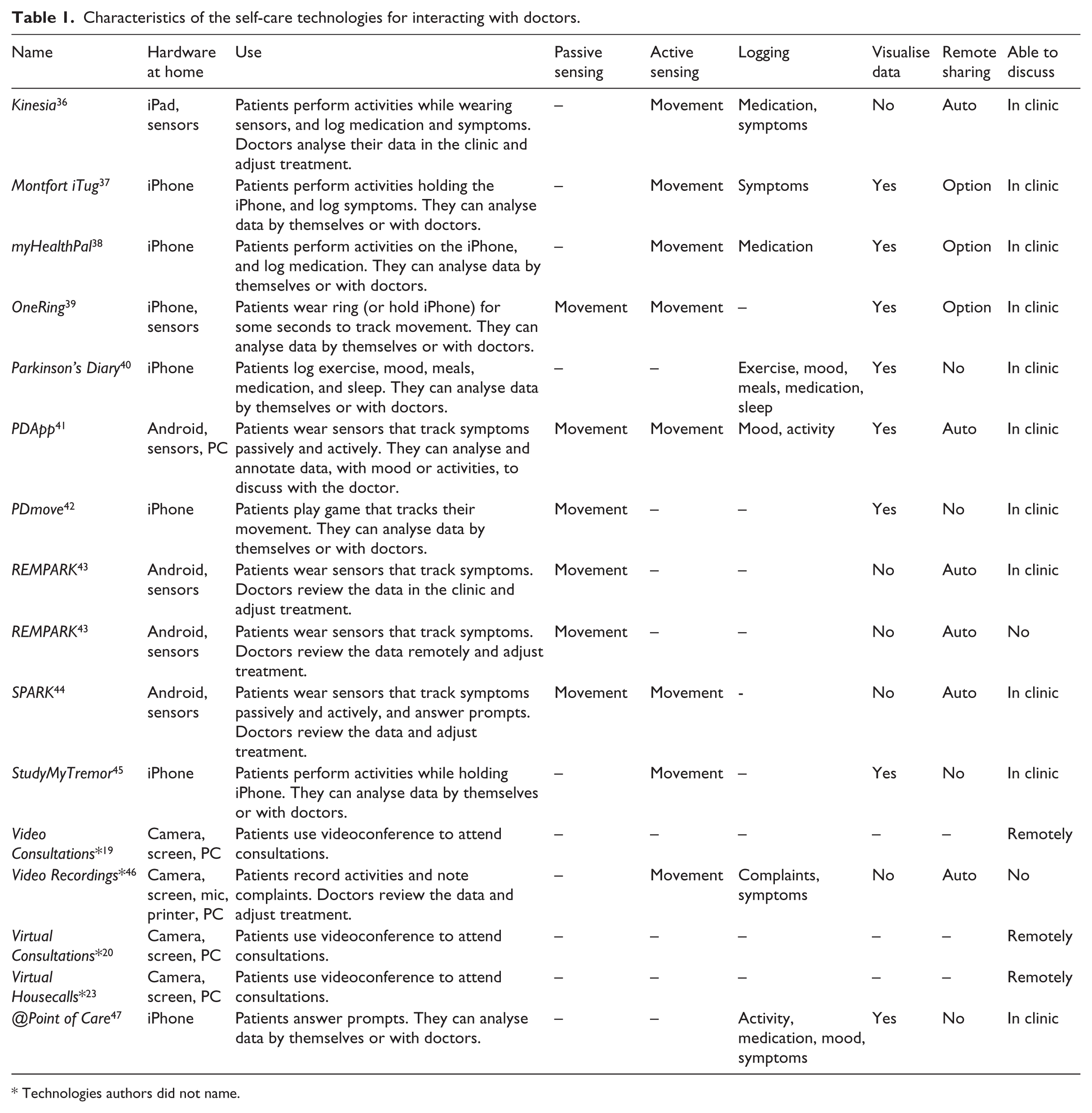
Technologies authors did not name.
Investigating issues
The self-care technologies for tracking, such as Parkinson’s Diary 40 and Montfort iTug, 37 were mostly targeted at helping people to learn about their body and condition. Since these technologies usually provide visualisations, they can potentially help patients quantify the severity of symptoms, identify trends, and overall collect issues that they can bring to discussion with their doctors.
Despite the potential of these technologies though, there are several characteristics that might hinder the patient from investigating certain issues. The most common issue is the lack of variety in tracking or logging features. While Parkinson’s affects numerous activities, logging is fixed on certain characteristics, such as medication or (motor) symptoms, and sensing is restricted to movement issues. The problem with the lack of variety is that it restricts the investigation of issues to a subset of Parkinson’s problems.
Another issue preventing technologies from enabling patients to investigate issues is the inability to visualise the collected data. While REMPARK, 43 Kinesia, 36 and SPARK 44 all enable patients to capture or report data about specific symptoms and signs of the condition, only doctors can visualise or analyse the data produced. Patients cannot access their own data, which defeats the purpose of investigating issues. Patients may still reflect about their condition each time they track a symptom or log an issue, but the opportunity for technology-mediated analysis is missed by not giving them the tools for reflecting more thoroughly on their data.
Participating in discussions
Most self-care technologies in the review potentially supported the discussions with doctors. In some cases, technologies enabled discussions to take place through videoconference, such as with Virtual Housecalls* 23 and Virtual Consultations*. 20 In other cases, self-care technologies could be used to feed discussions with issues identified while tracking or analysing data, such as with PDApp 41 and OneRing. 39 Participating in discussions about one’s health is essential to playing an active role in care, so it is positive that many of these technologies support and, in some cases, even potentially enrich the discussions with issues from everyday experience.
However, there were some cases in which the technologies eliminated discussions with doctors altogether. For example, Video Recordings 46 is a technology where patients answer questionnaires about symptoms and perform specific movements in front of a video camera. Once tracking and logging are complete, the data are transferred to the doctor who updates the medication plan without holding any discussion. Even though patients play a role in collecting the data, they are rendered as passive actors, who instead of contributing with their lived experiences only produce the data stream that informs the decisions of doctors.
Fixing inappropriate medication
The reviewed self-care technologies did not account for the possibility of getting inappropriate medication, since patients could not signal their need for treatment adjustments through the technologies. For example, the technologies for enabling remote consultations did not enable patients to initiate videoconference sessions. And while numerous self-care technologies enabled logging, it was not possible to report that medication needed revision. The inability to trigger medication adjustments through these technologies does not imply that corrections were impossible. One can extrapolate that patients would still be able to phone doctors or go to the clinic sooner as the fieldwork participants. However, by not providing direct paths within the technology, people might have missed a more straightforward process for adjusting medication.
Discussion
Our fieldwork showed that patients and carers were very proactive when interacting with doctors. Existing healthcare infrastructures enabled them to participate in diagnosis and decision-making, direct learning activities to certain topics, and adjust medication when it was inappropriate. Nevertheless, their agency might change if certain technologies that promote a more limited participation, as evidenced in the review, are integrated into healthcare infrastructures.
This article adds to the growing body of literature that describes the crucial role of patients and carers in making healthcare infrastructures work. Previous research had called attention to how they were essential in sending measurements remotely, 21 bringing medical exams, 48 and exchanging information between doctors. 49 With this article, we show the role patients and carers play in participating in the discussions that lead to appropriate treatment.
While this study is about people living with Parkinson’s, related studies of other chronic conditions argued that patients and carers similarly demonstrated active agency. For example, Cicutto et al. 50 described how people living with Chronic Obstructive Pulmonary Disease contributed to their diagnosis and argued for adjustments in medication timing to better fit their activities. Similarly, Funnell and Anderson 51 argued that doctors needed to work together with people with diabetes towards the goals they want to achieve, because that is the only way to reach appropriate treatment.
Acknowledging the active agency of patients and carers in medical care
Recognising the active agency of patients and carers has consequences for how we understand their role within healthcare infrastructures. For this reason, this section will now describe some properties that characterise the engagement of patients and carers when interacting with their doctors. Practical implications for the design and planning of self-care technologies and infrastructures will also be discussed.
Active role in diagnosis definition
Patients and carers played a critical role in the diagnosis definition. The neurological examination could easily become misleading if patients hid their symptoms, or if patients and carers did not describe the differences between the observation at the clinic and the everyday experience. Moreover, many symptoms, signs, and issues were brought up by patients and carers to the discussions; they were also the ones deciding how problematic each issue was.
This active participation contrasts with some perspectives on patient–doctor interaction (the expression ‘patient–doctor interaction’ undermines the key role that carers play in interactions with doctors. Still, as this is an expression commonly used in the literature, it is employed here) that expect diagnosis to be performed only by doctors after collecting issues and complaints. 6 Even the patient-centred care model, that advocates for shared decision-making, commonly understands the diagnosis and treatment definition as activities performed solely by doctors.7,8 Our fieldwork favours a more collaborative conception. Similar to Epstein et al., 52 our work shows that diagnosing is about understanding issues from the standpoint of the lived experience, together with other complex needs, fears, or expectations. The doctor’s role is thus not to decide but to help people reflect on their situation and priorities, so they can articulate what is most important to address. 3
In general, the reviewed self-care technologies promoted an active participation in diagnosis. By enabling people to track and visualise their data, the technologies potentially enabled patients to learn about their body and condition and thus elicit issues to discuss with doctors. However, there was an important obstacle preventing people from collecting issues to discuss, the inability to visualise the data collected. While most technologies enabled people to visualise their data, some did not and thus greatly reduced the reflection people could make of their data.
Recognising the active participation of patients and carers in the diagnosis motivates developing tools that enable people not only to track issues but also to visualise and analyse their own data. Without these, it will be hard for the tools to support people in investigating issues, and consequently bringing them to discussion.
Active role in decision-making
The fieldwork has shown that patients and carers participated actively in medical decisions concerning their health. While doctors suggested treatment adjustments, patients and carers scrutinised the potential of these to reach their needs and aspirations, and it was the collaborative engagements between all participants that resulted in appropriate treatment decisions. These collaborations were made clear with the excerpt of the patient with a 7-h interval between intakes, who kept to his own medication plan despite the doctor’s advice to change it, because it served him well and there was little to gain from changing.
Collaborative decisions were common in the fieldwork, however, as mentioned before, the literature on patient–doctor interaction often portraits these encounters under a paternalistic model, where doctors solely make decisions. The regular use of the terms non-compliance or non-adherence also indicates that medical decisions are not shared, because problems in implementing treatment or practical decisions are attributed to a willingness to go against the doctors’ ‘instructions’. As Funnell and Anderson 51 elegantly put it, non-compliance only exists when there are ‘2 people working toward different goals’ (p. 1709). Our fieldwork offers an alternative conceptualisation to patient–doctor interactions where medical decisions are collaborative. All participants sit as equal partners at the table, in recognition of their specific expertise and the mutual commitment to reach appropriate treatment.3,4 Making decisions collaboratively recognises that a treatment embodies both a clinical and a value judgment, and that the value judgement that matters is that of the patients and carers. 5
Most self-care technologies in the review supported discussions with doctors; however, there were some technologies that eliminated medical discussions. In fact, some technologies were designed for doctors to decide based only on the health data, which can be quite problematic. Based on symptoms alone, the patient with a 7-h interval would probably have had his medication changed, because that was the sensible decision to make with the available information. Yet, in changing his medication, the doctor would have forced unnecessary changes to the routine of a patient who does not feel like he needs them. Previous research also showed negative consequences of excluding patients and carers from the decision-making. For example, when patients with diabetes were removed from the interpretation of glucose values in a patient record, they felt frustrated because numbers did not explain their decisions or the context in which they acted. 53 In myRecord, 54 a technology where doctors could remotely diagnose and adjust an implantable pacemaker, the decisions became much harder after excluding patients to the point that they had to be later re-introduced. However, when patients and carers were indeed included, there were benefits to the care received. The doctors addressed issues after analysing measurements they did not consider before,54–56 and interpreted values differently after understanding the context in which they occurred.54,57
Recognising the active role patients and carers play in medical decisions involves developing tools that enable them to be ‘present’ when decisions are taken about their health. Even if the symptom data are sent remotely, collaborative discussions are the only way to ensure the treatment addresses the relevant concerns and fits with everyday life. Being face-to-face helps achieve this objective, but there might be alternatives, such as using videoconferencing19,20,23 or phone calls. 54
Active role in learning
The fieldwork has shown that patients and carers actively sought to learn about their condition, treatment, and prospects during interactions with doctors. They often raised questions and directed discussions to certain topics to get information from their doctor.
While patients and carers engaged actively in learning, literature usually refers to this activity as a passive one. The word used to name the learning that happens in interactions with doctors is usually patient-education, a concept that suggests that doctors educate the naïve patients who visit them. According to that perspective, patients do not understand the consequences of their choices, and so doctors need to educate and persuade them in specific ways. 58 However, this perspective does not adequately describe the interactions in our fieldwork. In fact, patients and carers were well informed about their condition, and that is why they raised issues in the first place. People sought advice on what to expect, what to look for, and what to consider, so that they could make informed decisions and prepare for the future.
As mentioned before, the reviewed self-care technologies could enable people to investigate their issues by supporting logging and tracking. These investigations would potentially raise doubts, problems, or other topics that people might want to discuss with their doctors. Nevertheless, there is an important obstacle that can hinder people from learning more: the lack of diversity of features that can be tracked or logged. Swelling ankles, pain in the legs, or problems walking around a crowd – all of which were mentioned in this article – could not be straightforwardly tracked or logged with the reviewed technologies. As the technologies focused mostly on motor symptoms, they fail to support the everyday experience and could restrict learning to certain aspects.
Recognising the agency of patients and carers entails offering them tools that support a rich investigation of issues. Making available self-care technologies that are open to capture different signs and symptoms without restriction to certain aspects or symptoms, as Storni 25 suggests, may be useful in enabling people to get in contact with more issues and thus better learn when interacting with their doctors.
Active role in adjusting inappropriate medication
The activities of patients and carers did not end when consultations finished. While at home, people carefully observed the effects of the updated medication plan in the patient’s body and activities. If symptoms became worse or unexpected issues appeared, patients and carers quickly went to the doctor, phoned their specialist, or went to the online forum, in search of a solution to their problem. These actions created ways to access medical care and ensured the disruptions were kept as short as possible.
However, the literature on Parkinson’s did not seem to discuss the experience of finding oneself with inappropriate medication. It was as if the treatment was always adequate or at least good enough to wait some months, because there were no mentions to having consultations or phone calls before the next appointment (in a focus group organised by Van der Eijk et al., 11 patients requested telephone consultations to follow up on treatment changes and asked for the email and phone contacts of their doctors. These requests suggest that those patients might have experienced the need to adjust medication before the next consultation, yet these practices were not documented in the article). In our fieldwork, however, it was clear that sometimes medication was not well received by the body and that medical care was essential before the next encounter. These urgent adjustments may also explain why patients and carers so often had the mobile phone number of their doctors.
Self-care technologies for Parkinson’s did not enable people to trigger the need for treatment adjustments. For example, in videoconference technologies, patients could not ask for having an earlier appointment, and in technologies that collected symptom data, it was not possible to signal inappropriate medication.
Recognising the role patients and carers have in addressing inappropriate medication changes requires technology or supporting infrastructures to enable people to signal their need for medication adjustments or advice on how to proceed.
Involvement of both patients and carers
Patients were rarely alone in their interactions with doctors. Most of the carers in our fieldwork accompanied the patients and engaged actively in discussions. Similarly, in the online community, both patients and carers asked questions to the doctors which give evidence of their collaborations.
The literature on Parkinson’s showed a similarly active engagement of carers. Both Pinder 2 and Martin 59 documented that carers accompanied the patients to the clinic and also that they participated actively in these encounters.
It is thus surprising to observe how often carers lacked a role in self-care technologies. Apart from one technology, carers were not even mentioned in the descriptions of the technologies, which lead us to assume they did not have a role to play.
Recognising the active agency of carers motivates the development of self-care technologies and infrastructures that enable carers to participate together with patients in their interactions with doctors. Otherwise, an important part of self-care may be disregarded.
Conclusion
This article has investigated the interactions of patients and carers with their doctors in different care scenarios. In particular, we have contrasted how patients and carers living with Parkinson’s act within the current healthcare infrastructures, with the participation that is promoted by self-care technologies for interacting with doctors. Our findings show that patients and carers play a very active role when interacting with doctors, and that technology has the potential to support or even enrich these engagements, provided some obstacles are eliminated. We discussed the implications of recognising an active engagement of patients and carers to the understanding of healthcare infrastructures, and propose practical implications for design. Our findings should contribute to the design of technologies that promote an active participation of patients and carers.
Footnotes
Acknowledgements
The authors would like to thank the participation of every patient and carer in the study, as well as all the help received from the Portuguese Association of Patients with Parkinson’s. They also acknowledge the neurologists Carolina Garrett and João Massano for facilitating access to consultations and for interesting discussions about Parkinson’s disease.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.