
Abstract
A major challenge for healthcare quality improvement is the lack of IT skills and knowledge of healthcare workforce, as well as their ambivalent attitudes toward IT. This article identifies and prioritizes actions needed to improve the IT skills of healthcare workforce across the EU. A total of 46 experts, representing different fields of expertise in healthcare and geolocations, systematically listed and scored actions that would improve IT skills among healthcare workforce. The Child Health and Nutrition Research Initiative methodology was used for research priority-setting. The participants evaluated the actions using the following criteria: feasibility, effectiveness, deliverability, and maximum impact on IT skills improvement. The leading priority actions were related to appropriate training, integrating eHealth in curricula, involving healthcare workforce in the eHealth solution development, improving awareness of eHealth, and learning arrangement. As the different professionals’ needs are prioritized, healthcare workforce should be actively and continuously included in the development of eHealth solutions.
Keywords
Introduction
Healthcare systems throughout the world are endeavoring to rise to the challenges that result from aging population, prevalence of chronic conditions, rising life expectations, and multi-morbidity.1–3 The traditional healthcare delivery is unsustainable and is increasingly recognized that integrated care can significantly improve the quality and continuity of services. 4 With the focus on creating more efficient and cost-effective care, eHealth is seen as one of the key solutions. An EU report indicated that eHealth has the potential to be the third pillar in the health market, along with pharmaceuticals and medical devices. 5 The 2010 EU Citizenship Report underlined the role of eHealth in facilitating cross border healthcare. 6 Its focus is to advance and create new models for delivering better quality, more efficient healthcare services, and not to replace traditional ways of care delivery, such as face-to-face consultations.
According to the EU project “Chain of Trust,” which analyzed the experience of 6704 patients and health professionals who used eHealth, two most prominent topics were the confidence in health IT and health professionals’ skills. 7 Traditional curricula commonly do not equip healthcare workforce even with the basic health IT skills. Identifying approaches for achieving high proficiency in eHealth healthcare workforce including those working in public health, and allied professionals, is a key to healthcare transformation.
The need to improve the eHealth/IT competences of healthcare workforce has been frequently emphasized by policymakers at an international level. One of the projects aiming to identify healthcare workforce IT skills needs is the CAMEI project.8–10 It is a collaboration between the United States and Europe, which was initiated by the Memorandum of Understanding on Cooperation Surrounding Health-Related Communications and Technologies. 11 Other studies focus on some specific areas or workforce groups.12–15 In this study, we use the World Health Organization (WHO) definition of healthcare workforce as “all people engaged in action whose primary intent is to enhance health.” 16 The eHealth/health IT skills are defined as “any competence and knowledge deficiencies among all staff in healthcare delivery, management, administration and support to ensure universal application of ICT solutions in health services.” 17
To our knowledge, this is the first study that used a systematic approach in setting priorities for the IT skills competence development among healthcare workforce. A bottom-up approach, with collaboration between experts from diverse backgrounds in healthcare is the way to ensure the health IT skill issues faced by healthcare workforce be addressed appropriately. The objective of this study was to identify and prioritize the actions needed to develop the IT skills competence among healthcare workforce
Methods
The study was approved by the Bioethics Committee of the Medical School of the Aristotle University of Thessaloniki, Greece (approval no. 94/26-06-2014). Relevant information about the study was presented to the participants when asking for their consent of participation. The information covered the standard domains of identifying the researchers, the study purpose and procedures, confidentiality, and how to contact the researchers with any questions or to obtain study results. The way to use the participants’ response was also informed, as well as their impact on the results. Their response to the questionnaire indicated their understanding and willingness to participate in the study. Due to the various geographical locations of participants, the information was sent via emails.
Our research is about collecting basic and non-sensitive information. No harm is made to the participants. The collected data can only be used for research purposes and are stored accordingly to social science research guidelines. All the participants were not given any information about the data obtained from one another. All the data were analyzed anonymously. No comparison was made from one participant’s opinion to another. Taking into account the collected data, it was presented as it was without altering it to satisfy certain predictions. The participants in this study did not receive and were not promised any forms of compensation in return.
The Child Health and Nutrition Research Initiative (CHNRI) methodology for priority-setting was used to assist prioritizing actions in this study. 18 The process uses a systematic and transparent approach to assemble and analyze a wide spectrum of collective actions from an array of healthcare experts. Prioritization criteria relevant to the topic were used to score and rank the actions. The CHNRI methodology has been used previously to identify research gaps and resource priorities in areas such as birth asphyxia and mental health, and it is increasingly being used by policy-makers, large donors, and international organizations.18–20 Figure 1 illustrates the four stages of CHNRI methodology.
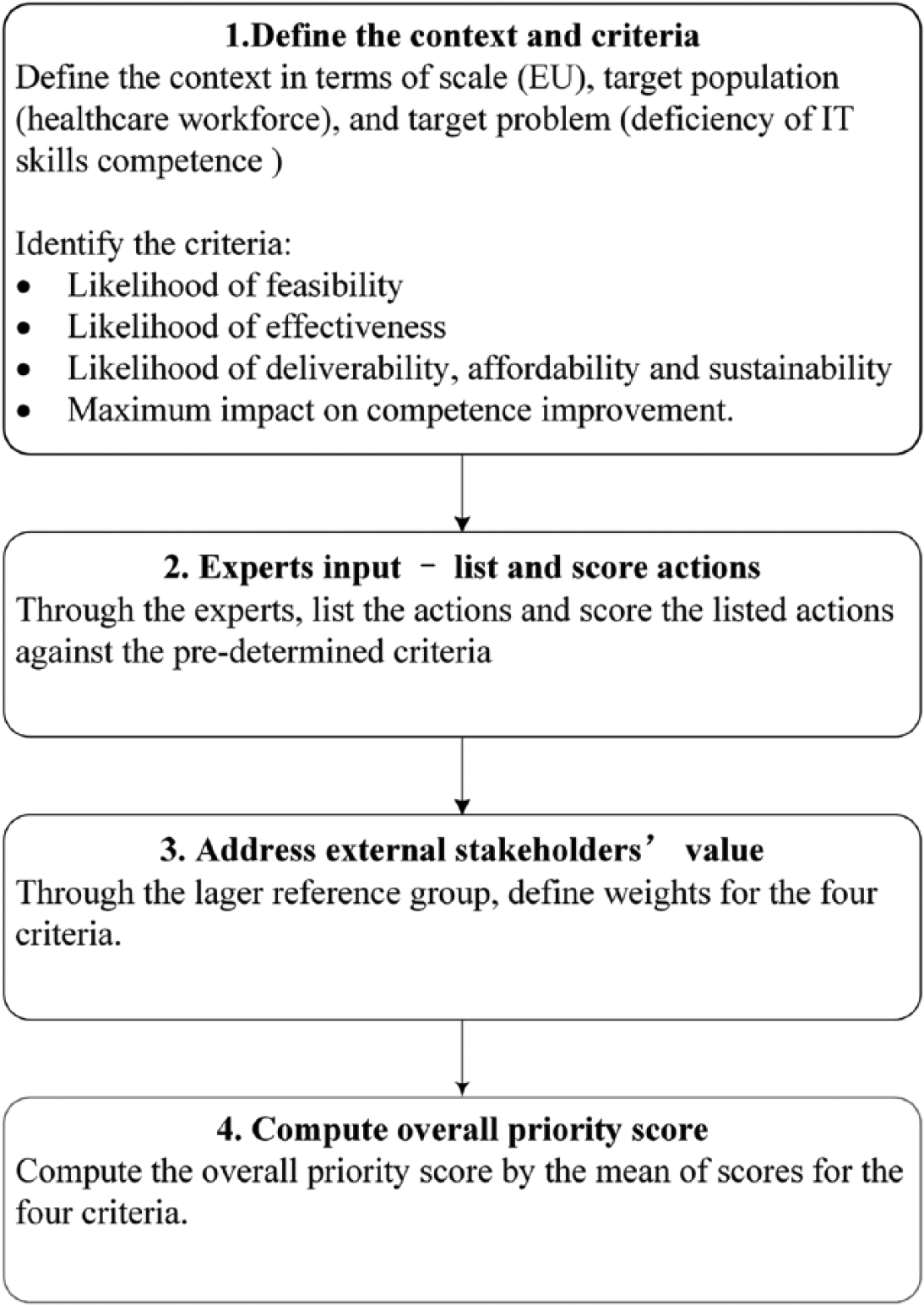
CHNRI methodology process.
Stage 1: define the context and criteria
Defining the context is a critical part of the CHNRI process as priority scores for many actions may strongly depend on the context in which the process takes place. The context for this study was specified as follows:
Scale of the study: EU;
Problem: deficiency of IT skills competence;
Target population: healthcare workforce;
Based on CHNRI’s conceptual framework, 18 four scoring criteria were identified: (1) feasibility; (2) effectiveness; (3) deliverability, affordability, and sustainability; and (4) maximum potential impact on competence improvement.
Stage 2: experts input—listing and scoring actions
A total of 46 leading experts, representing different expertise and geographical locations, were invited to participate on the basis of their record in eHealth or their membership in an international health organization, which mainly include the following:
American Health Information Management Association (AHIMA)
Computer-Based Medical Systems Committee (CBMS)
Standing Committee of European Doctors (CPME)
European Association of Hospital Pharmacists (EAHP)
European Federation for Medical Informatics (EFMI)
European Federation of Nurses Association (EFN)
Healthcare Information and Management Systems Society (HIMSS)
International Medical Informatics Association (IMIA)
Joint Information Systems Committee (JISC)
Medical Informatics Europe Committee (MIE)
Health Level Seven International (HL7)
openEHR initiative stakeholders
A total of 29 experts from 14 countries participated in the study listing actions via web survey in March 2015, whereas 34 experts from 19 countries scored actions via web survey from April to May 2015. There was an overlap of 17 experts who were involved in both processes, as shown in Figure 2. In the listing process, experts proposed actions that they thought were important to improve IT skills competence among healthcare workforce. The experts were from 14 countries, including the United States, the United Kingdom, Finland, Norway, Iceland, Switzerland, Denmark, German, Spain, Czech Republic, Ireland, Austria, Belgium, and the Netherlands. Among 29 experts, 10 percent were academics or researchers only, about 69 percent were academics or researchers and belonged to a non-governmental organization (NGO), and 21 percent were from NGO only. The process was open-ended and all the proposed ideas from each of the experts were collected independently. The list of actions was compressed to highlight important gaps, yet still represent the range of possibilities to improve IT skills. Then, the final list of actions was reviewed by the authors to ensure that they were framed correctly and comprehensively to allow scoring.
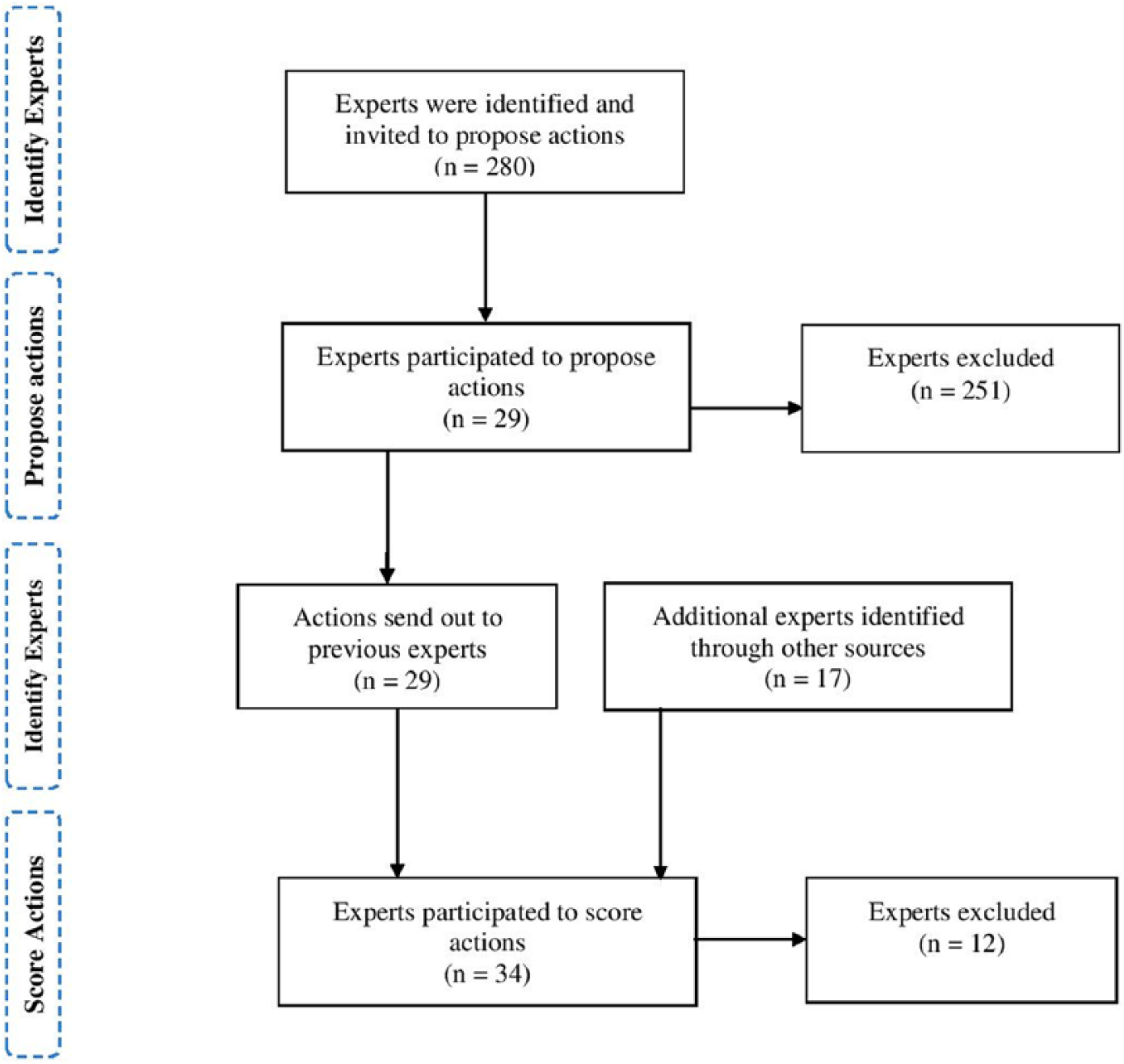
Experts’ recruitment process.
In the scoring process, experts evaluated the final list of actions independently according to the criteria as described in Stage 1. Every expert scored all four criteria, which limited potential impact of any single expert on overall scores. In this way, the listed actions received four “intermediate scores,” ranging from 0 to 100 percent. These values represented a direct measure of the collective optimism of the experts. In addition to the 14 countries in the listing process, more experts from Sweden, Greece, Kosovo, Slovenia, and Bulgaria participated in the scoring process. Among 34 experts, 17 percent of them were academics or researchers only, about 59 percent were academics or researchers and belonged to a NGO, and 24 percent were from NGOs only.
Apart from EU countries, experts from the United States were also invited to participate in the study due to the collaboration between the European Commission and the United States in actively addressing the needs for skilled workforce. 11 This was also necessary to make sure that identifying approaches to develop IT skills competence involved a diverse group of experts (rather than isolate EU experts only).
Figure 3 illustrates the expertise of participants in both listing and scoring processes, which mainly included the following:
eHealth: EHR, telehealth, clinical decision support, healthcare information system, and health knowledge management;
Health informatics: medical informatics, nursing informatics, and biomedical informatics;
eLearning and education;
Standardization: SNOMED CT and interoperability;
Clinical expertise: medical doctor, nursing, and pharmacy.
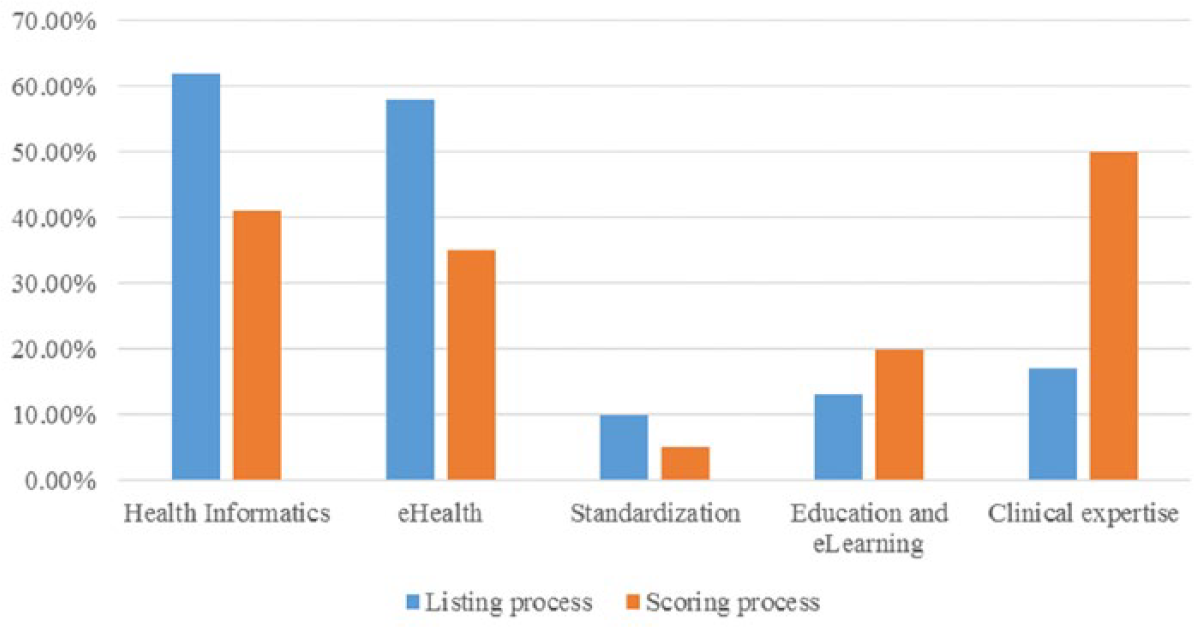
Experts’ expertise information.
A full list of experts with their expertise and affiliations are presented in Tables S1 and S2.
Stage 3: address external stakeholder’s value
The CHNRI methodology ensures the involvement of stakeholders in the process regardless of their expertise. The term “stakeholders” refers to all individuals and/or groups who have an interest in the prioritization of health research, therefore will comprise a large and very heterogeneous group (e.g. expected recipients of the research, taxpayers, medical students, health workers, journalists and media, and political experts). 18 They lack expertise to directly decide research priorities, but they can still weigh the chosen priority-setting criteria based on values assigned by them. 21 In this study, it was decided that the external stakeholder’s value will not be addressed and final rankings were based on the priority scores from the perspectives of experts.
Stage 4: compute priority scores and assign ranks
Each expert scored each action by answering one question per criterion. According to CHNRI framework, 18 the answers to each question are simply: “Yes” (1 point) or “No” (0 points). When the experts were sufficiently informed to answer the question, but can neither agree nor disagree, they were allowed to choose “Undecided” (0.5 points). Furthermore, when the experts did not feel they have enough knowledge to answer some questions, they chose “Unqualified to answer.” Thus, the listed actions got a score for each of the four criteria. The overall scores were calculated as the mean of the scores for the four criteria according to the below formula

Results
The full list of 23 actions and scores from each individual expert is presented in Table S3. The results exposed how actions can be prioritized depending on the criterion of feasibility, effectiveness, deliverability, and maximum potential impact on competence improvement.
Table 1 shows the 10 actions with greatest overall priority score. The action that achieved highest score was about integration of health information technology in curricula for healthcare workforce at different levels (85.1). In addition to that, other actions that focus on continuing training among healthcare workforce also obtained high scores. The action about ensuring the trainer competence was ranked second (84.5); training on patient-centered eHealth services was fifth (83.6); training on role-specific IT skills was sixth (80.3), and training on the development of processes and activities supported by IT solutions was tied ninth (75.6).
Ten actions with greatest overall priority score.
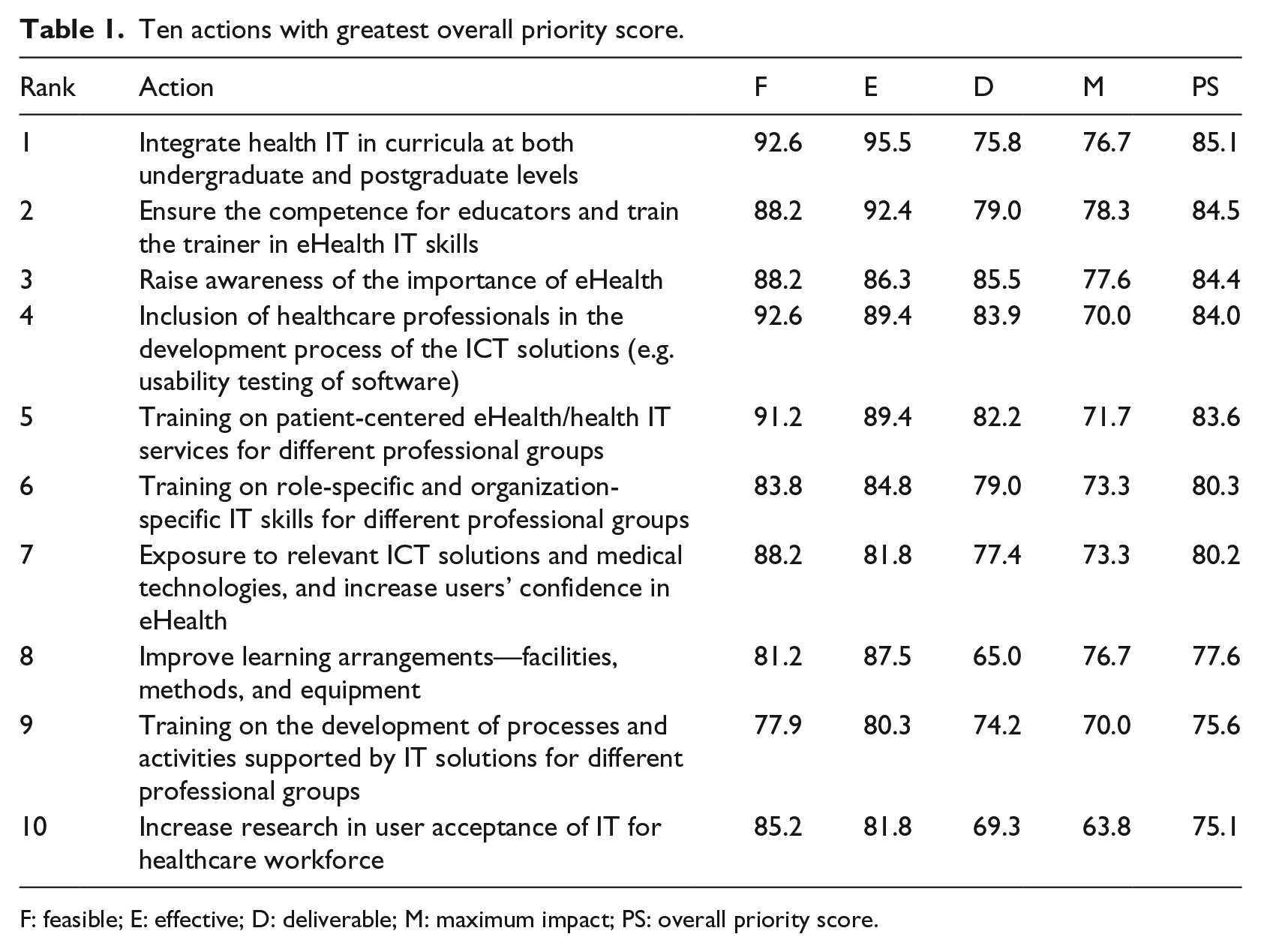
F: feasible; E: effective; D: deliverable; M: maximum impact; PS: overall priority score.
Two high-scoring actions were related to improve the workforce involvement: inclusion of healthcare workforce in the development process of eHealth (ranked 4th) and research in user acceptance (10th). High scores were also given to two related actions that identified education on eHealth, specifically for and improving awareness (3rd) and increasing confidence (7th).
Table 2 shows the 10 lowest-scoring actions. Concerns about feasibility were expressed for actions related to identification of IT skills competence needed at international level (ranked 16th, feasibility score: 74.2), evaluation of skills of existing and new staff, offer qualification procedure (19th, feasibility score: 73.5), and joint funding for training programs (20th, feasibility score: 66.7). For the effectiveness criteria, experts identified actions that introduce online training tools and in-house training for different healthcare workforce as less effective (14th, effectiveness score: 74.2). Other effective action was related to helping workforce recognize eHealth/health IT as a specialty (17th, effectiveness score: 68.1).
Ten actions with lowest overall priority score.
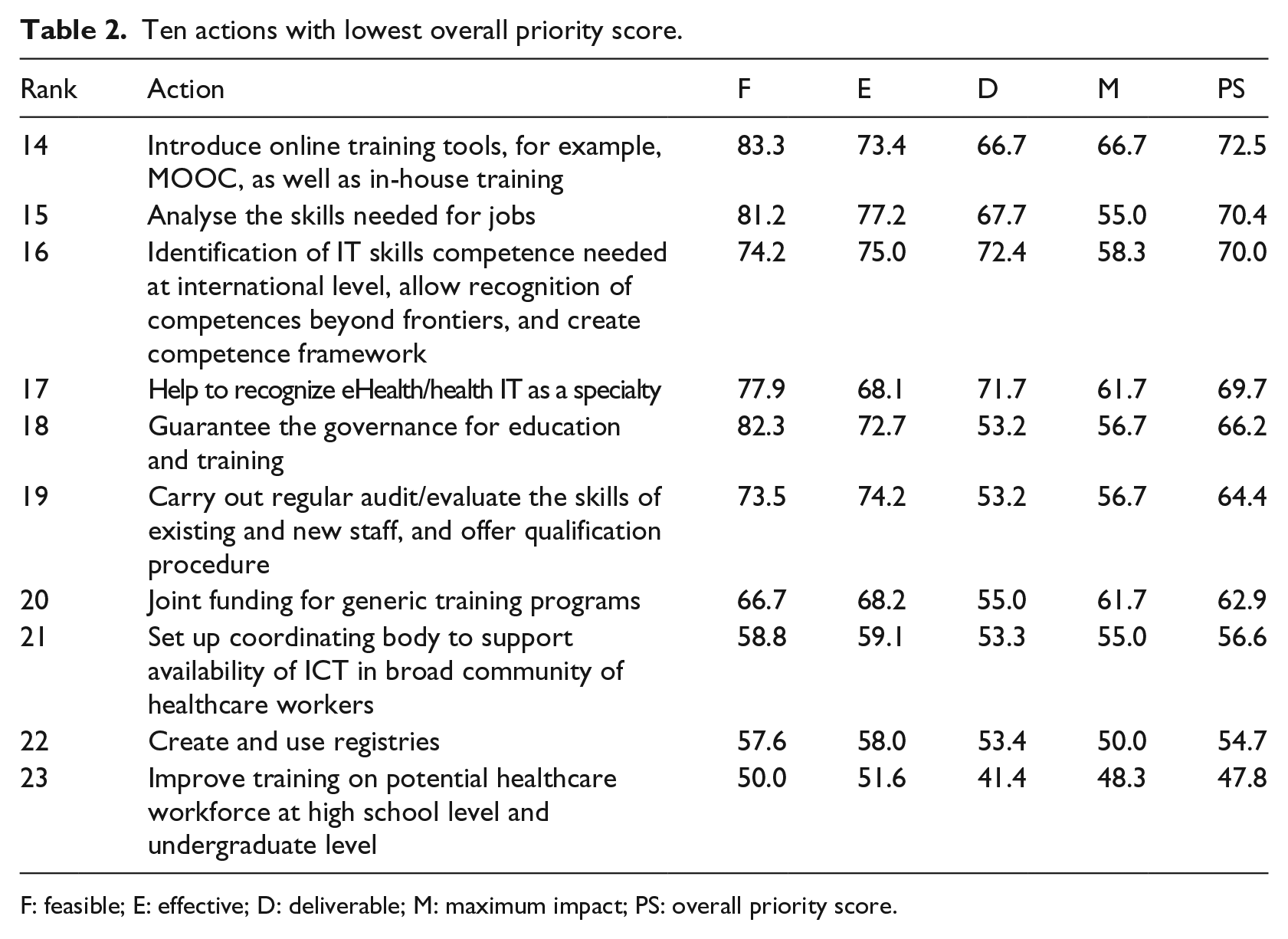
F: feasible; E: effective; D: deliverable; M: maximum impact; PS: overall priority score.
Several actions reached the bottom line because they had low scores in the likelihood that these actions could be deliverable, affordable, and sustainable taking into account the current resources. These actions included guaranteeing the governance for education and training (18th, deliverability score: 53.2), setting up coordinating organizations to support availability of ICT in broad community of healthcare workforce (21st, deliverability score: 53.3) and improving training on potential healthcare workforce (23rd, deliverability score: 41.4). Two actions that proposed to analyze the IT skills needed for jobs and create registries (15th and 22nd, maximum impact score: 55.0 and 50.0) received low-priority scores because they were perceived to have less impact on the improvement of IT skills competence.
To summarize, the action that proposed to integrate health IT in curricula was acknowledged as most feasible (92.6) and effective (95.5). Raising awareness of the importance of eHealth was considered to be most deliverable (85.5) while ensuring the competence for educators could mostly impact the IT skill improvement (78.3).
Discussion
Main findings
Prioritization mechanisms are necessary to facilitate the current demand for skilled healthcare workforce, particularly competence to support national eHealth work agendas.14,15 The overall message of this prioritization study suggests that actions to improve IT skills competence among healthcare workforce in the EU should concentrate on improving workforce training, the inclusion of healthcare workforce in the development of eHealth solutions, raising awareness of eHealth, and improving learning arrangements. The results are generally in line with the recommendations from a recent eHealth Stakeholder Group report 22 that focused on eSkills and health workforce.
Of the top 10 actions, 5 were related to training among healthcare workforce, which reflects the significance of continuous training in IT skills development since the gap between current curriculum and eHealth.23,24 The importance of training for healthcare workforce in the use of new technologies was also acknowledged in several studies, as well as a Green Paper on the EU health workforce.14,25,26 Moreover, the results showed the great need of involving healthcare workforce in decisions on introducing eHealth, as well as in designing, testing, and deploying eHealth. Similar results were also demonstrated in another study; user involvement is perceived as crucial to ensuring acceptance in the long term. 7 Furthermore, improving learning arrangements was considered as an essential approach to improve the workforce IT skills. It has been identified by Fields 27 that being limited or with not enough access to technology was one of the top 10 challenges faced by healthcare workforce.
The 2012 Action Plan for the EU Health Workforce from the European Commission 28 outlined three priority areas of actions to promote a sustainable healthcare workforce: forecasting workforce needs and improving workforce planning methodologies, anticipating future skills’ needs in the health professions, and sharing good practice on effective recruitment and retention of health professionals. However, the two actions related to identify the IT skills needed were not highly featured, despite being crucial for future workforce plan. These lower prioritizations were due to the concerns on the maximum impact on IT skill improvement.
Two exception actions addressed training issues: “introduce online training tools” and “training on potential workforce,” which ranked low priorities. Although a recent systematic review of the effectiveness of online eLearning suggested that eLearning is possibly superior to traditional learning, 29 experts probably feel that the actions were not deliverable, affordable, and sustainable.
Scores for feasibility and effectiveness of the 23 actions were relatively higher than deliverability and had maximum impact. For instance, while the action “Guarantee the governance for education and training” scored 82.3 percent on feasibility, it scored poorly on deliverability (53.2%). This illustrates the fundamental characteristics of health system delivery across the EU. Similar to the EU, the healthcare delivery system in the United States is facing critical challenges as each unit in health industry operates independently and focuses on its own performance. 30
Strengths and limitations
The main strength of the CHNRI methodology can be summarized as follows: (1) clearly defined context and key criteria that qualify some actions as a funding priority over the others, (2) transparent process for individual input and decision-making in priority-setting, (3) systematic way in scoring actions, thus limiting the influence of individual biases on the outcome, (4) prevent individuals from dominating the process, and (5) an intuitive quantitative outcome that is easy to justify and understand.
Still, the methodology is not free of some possible biases. Although the methodology attempts to involve a wide range of opinions from the participants, many good ideas may not have been included in the initial list of actions. The listing process ended up with open-end questions that may result in multilevel answers from experts. Although efforts were made to phrase the initial actions in a better way, the process was done only by the main authors and some phrased actions may be still confusing for experts. In addition, experts understanding in “IT skills competence” and “healthcare workforce” would be a bias on the outcomes.
Another concern over the CHNRI process is that the possible bias regarding the opinions of a very limited group of experts and the results from the choice of the experts. As the study was based on EU level, the participating experts in the study are only from 18 EU countries. The concept of “healthcare workforce” relates to a broad range of individuals with both clinical background and non-clinical background; 16 however, not every expertise was involved and balanced among experts. The number of individuals who possess enough experience, expertise, and knowledge on IT skills competence among healthcare workforce to evaluate the actions presented is rather limited.
Another bias could be the results from the scoring process. In order to improve the responsiveness of experts and decrease the burden of scores, a minor change was made to score the actions by answering one question per criteria rather than three questions according to the CHNRI guideline. It could affect the accuracy of results to some extent. As for the calculation of priority scores, the answers “yes” got 1 positive point, “no” got 0—no extra point, if it is “undecided,” a positive grade (0.5) is still added to the achieved sum. Nevertheless, compared to other priority-setting methodologies mentioned above, the CHNRI approach is prominently featured in the special algorithm and limits the individuals’ bias on the outcomes.
Validity
The fundamental principle of CHNRI methodology is “wisdom of crowds,” which refers to the process of taking into account the collective opinion of a group of individuals rather than a single expert to answer a question. 31 It has been shown that the average of collective guesses is often better than any expert judgment. By giving each individual the equal right and opportunity to express their own judgment, the personal biases that each one brings to the process tend to negate and diminish, regardless of the participant selection. Following the CHNRI guideline, the same action was scored by a larger group multiple times that improves the degree of accuracy.
Future work
The results from this study present a first step toward identifying the priorities of actions needed to improve the IT skills competence among healthcare workforce. Further research that includes experts with more expertise in healthcare is essential to better characterize all actions that needed for adoption of health informatics technology among workforce. One of the interesting approaches is to incorporate opinions from wider public who are interested in priority-setting in health area but lack of expertise to list actions. In this way, the final priority score for each action will contain the input from both experts and the stakeholders.
The CHNRI methodology ensures transparency in scoring process; therefore, it offers the potential to expose the points of the greatest agreement and the greatest controversy among the experts. 20 In this case, in addition to the information on how each action fulfills with the chosen priority-setting criteria, information about the amount of agreement between the experts on each action could also be obtained. Since the study context and other components of the contexts may change over time, actions can be taken so that research portfolio will continuously be adjusted to the context and aim, including (1) adding further actions to the list, (2) adding additional criteria, and (3) re-scoring all actions in the redefined context.
Conclusion
The growth of new technology, new medical appliances, and diagnostic techniques is leading to new ways of healthcare delivery, which requires a new mix of skills including technical and e-skills. Improving the eHealth IT competences demands concrete actions at an international level. This exercise has led to a concerted EU effort led by a group of experts, all of whom have eHealth-related experience, identifying the priorities of actions needed to be taken for IT skills improvement. The findings are a clear call for attention to integration of eHealth in current curricula, training for both educators and healthcare workforce, raising awareness of the importance of eHealth and inclusion of workforce in the development of eHealth solutions.
This study first explored the actions needed to develop IT skills competence among healthcare workforce using CHNRI methodology and systematically ranked priority list for generating specific suggestions. It is definitely clear that more researches in this field are required in order to provide comprehensive understanding of actions needed to foster IT skills competence for healthcare workforce at different levels.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by “CAMEI: Coordination Actions in the scientific era of Medical Education Informatics for fostering IT skills for healthcare workforce in the EU and USA” (![]() ), a project funded under the Seventh Framework Programme, as a coordination and support action (ICT-2013.5.1. G.A. no 611967).
), a project funded under the Seventh Framework Programme, as a coordination and support action (ICT-2013.5.1. G.A. no 611967).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.