
Abstract
Pervasive mobile healthcare system has the potential to improve healthcare and the quality of life of chronic disease patients through continuous monitoring. Recently, many articles related to pervasive mobile healthcare system focusing on health monitoring using wireless technologies have been published. The main aim of this review is to evaluate the state-of-the-art pervasive mobile healthcare systems to identify major technical requirements and design challenges associated with the realization of a pervasive mobile healthcare system. A systematic literature review was conducted over IEEE Xplore Digital Library to evaluate 20 pervasive mobile healthcare systems out of 683 articles from 2011 to 2016. The classification of the pervasive mobile healthcare systems and other important factors are discussed. Potential opportunities and challenges are pointed out for the further deployment of effective pervasive mobile healthcare systems. This article helps researchers in health informatics to have a holistic view toward understanding pervasive mobile healthcare systems and points out new technological trends and design challenges that researchers have to consider when designing such systems for better adoption, usability, and seamless integration.
Keywords
Introduction
Modern societies are plagued with the continuous rising of fundamental health challenges, such as chronic diseases and a lack of medical professionals.1,2 The proliferation of chronic diseases is now a serious social issue in the world. The World Health Organization (WHO) report on non-communicable diseases (NCD) shows that chronic conditions are still a global phenomenon and prominent cause of death among the population. NCD deaths are projected to increase from 38 million in 2012 to 52 million by 2030, and are currently responsible for 82 percent of deaths. 3 Very often, failure to manage chronic diseases results in lower quality of life, increased economic burden, and social problems.4,5 There is an increasingly high need for cost-effective healthcare services that can be provided to everyone, everywhere, and anytime ubiquitously to support and monitor patients and to avoid expensive hospital-based care. 6
Pervasive healthcare (PH) is a new discipline involving the use of ubiquitous computing technology to provide emergency and preventive healthcare services. 6 It is an emerging area with the widespread plethora of health sensors, communication protocols, and intelligent context-aware applications. 7 PH systems aim in pro-active detection of significant vitals of patients, ensuring preventive care and continuous monitoring solutions, thereby improving both system reliability and efficiency. 8 There is growing evidence that the benefits and importance of PH are worth the effort and are beyond argument.9,10 The major benefits include its pervasive and assistive technology nature, self-management of conditions, remote monitoring, high-quality health assessment and medical service, and a significant reduction in escalating the cost of healthcare. Besides all these benefits, the patients can lead a normal life at their own convenience.9,11 Nowadays, most PH systems are making use of mobile technologies due to their high accessibility and various inbuilt sensors. There has been an exponential rise in PMHSs and their potential to alleviate the burden of health issues. Many works have been done till now, but there is still a high need to conduct a state-of-the-art review of PMHSs to investigate recent trends in PMHSs and derive current opportunities and challenges for future expansion of this emerging research area.
The remainder of this article is structured as follows: In section “Research methods”, a research methodology is presented based on Kitchenham’s guidelines to plan, conduct, and report the review. Section “Planning the review” presents the planning phase used to extract potential articles from IEEE Xplore Digital Library and points out the data sources, search terms, inclusion, and exclusion criteria. Section “Conducting the review” lists down the main steps that are used to conduct the review. Section “Reporting the review” presents the analysis of the publications exhibiting the inclusion criteria and reports the results by (1) classifying the 20 systems that were reviewed and (2) discussing the general results for each PMHS. Section “Discussion” discusses the 20 PMHSs at different levels in terms of node level, network level and human level. Section “Open research challenges” focuses on the potential research challenges and opportunities. Finally, section “Conclusion” concludes the article.
Research methods
In this article, a systematic literature review is conducted by identifying, evaluating, and interpreting all available research relevant to the topic area “Pervasive Mobile Healthcare Systems for Chronic Disease Monitoring.” The systematic review is undertaken to summarize existing evidence of the benefits and limitations of the study, to identify gaps and open challenges in order to suggest new directions for future research, and to provide a foundation for new research work. The systematic review is carried out in three phases according to the guidelines proposed by Kitchenham, 12 namely (1) Planning the review (2) Conducting the review, and (3) Reporting the review which are discussed further in section “Planning the review.”
Planning the review
In order to plan the review, a pre-defined protocol is used to determine an appropriate strategy to undertake the review, which consists of (1) the data sources to be searched (including databases, specific journals, and conference proceedings), (2) the search terms, and (3) the inclusion and exclusion criteria considered in the review.
Data sources
With the advance and prevalence of pervasive health, the number of publications related to PMHSs has risen significantly since the past few years. After exploring some databases to conduct searches, highest relevance of indexed papers was found mainly in IEEE Xplore Digital Library. Therefore, the IEEE Xplore Digital Library was selected for this particular review as it is more appropriate for PMHS-oriented topics.
Search terms
Articles were found via computerized search of the topic areas. In order to select typical PMHS and at the same time narrow down the selected publications in a reasonable range, the search term ((pervasive health system) AND (mobile) AND (chronic disease)) was used. The search was limited to the last 5 years, namely between 2011 and 2016. A detailed illustration of methodology for extracting articles is followed. The last update was on 12 March 2016.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were used to select and accept the published articles to review the state-of-the-art PMHSs for monitoring chronic diseases.
To be included in the review, a system had to exhibit the following characteristics:
Use of mobile phone and wireless infrastructure as an intervention,
Support for chronic disease monitoring,
Use of biosensors,
Articles published from 2011 to 2016.
Systems excluded from the review exhibited any of the following characteristics:
Articles that describe systems that do not contribute original research;
Articles that describe systems where the sole purpose is to educate the patient about the disease;
Articles that describe systems without an English-language user interface;
In the form of book chapters, guest editorials, unpublished working papers, master’s and doctoral dissertations, and article summaries
Conducting the review
The review was conducted according to the planning phase. Moreover, Mendeley was used for document management, and Excel was used for data extraction and analysis.
Selection process
The selection process follows the multistage process based on Kitchenham’s guidelines. Initially, key terms were searched in the data source whereby a total of 683 non-duplicated articles were retrieved. After exclusion of the articles based on the title, abstracts, and full texts, only 33 articles remained. Finally, after the exclusions based on papers exhibiting only the inclusion criteria, the systematic review resulted in 20 unique relevant solutions.
Data analysis
The results of the data analysis are reported in section “Selection process.” The results highlight the key features and requirements and identify research gaps of the 20 systems that were reviewed with the aim of identifying critical factors to improve the adoption, usability, and seamless integration of PHMSs in the patients’ life and in the context of the larger patient-centric healthcare system. The first section of the result classifies the 20 PMHSs into four major categories of monitoring, namely (1) self-monitoring, (2) assisted monitoring, (3) supervised monitoring, and (4) continuous monitoring. The second section includes the general results which comprise detailed analysis of the (1) target audience, (2) sensor types, (3) contextual information/parameters monitored, (4) architecture of PMHSs, (5) communication protocols, (6) incentives and motivations, and (7) decision-making techniques.
Reporting the review
The state-of-the-art PMHSs for monitoring of chronic diseases that have been reported in the literature were investigated. After analysis of the selected articles, the PMHSs were grouped into four main categories. The following section presents the results and classifies the PMHSs.
Classification of PMHSs
Depending on the use, complexity of the system, and whether intervention of health professionals is required, PHMSs are often classified into four main categories, namely self-monitoring, assisted monitoring, supervised monitoring, and continuous monitoring. The 20 PMHSs are discusses further in the section below.
Self-monitoring
Self-monitoring usually makes use of technologies that can support the shift from managing illness to maintaining wellness through preventive care. Technologies for self-monitoring usually include an integration of both invasive and non-invasive sensors, mobile applications that enable patients to gather, monitor, and manage their own personal health. Self-monitoring of diseases do not involve external caregiver but is rather focused on self-care, self-discipline, and self-confidence of patients. The self-monitoring systems mainly consist of a wireless body area network (WBAN) and a mobile unit (MU). The WBAN typically consists of a collection of low power, miniaturized, invasive, or non-invasive, lightweight devices with wireless communication capabilities that operate in the proximity of the human body to collect the patient’s physiological and contextual parameters. These sensors’ data are wirelessly transmitted to the MU which store, process, and analyses the physiological data in order to notify the patient through a user-friendly and interactive graphical or audio interface. In the systems reviewed (n = 20), the MU was either a smartphone (19) or a personal digital assistant (PDA, 1). Typical diseases that are usually self-monitored (Figure 1) are chronic obstructive pulmonary disease (COPD) and sleep apnea. The self-monitoring systems and the different criteria are presented in Table 1.
Self-monitoring diseases.
Self-monitoring systems.
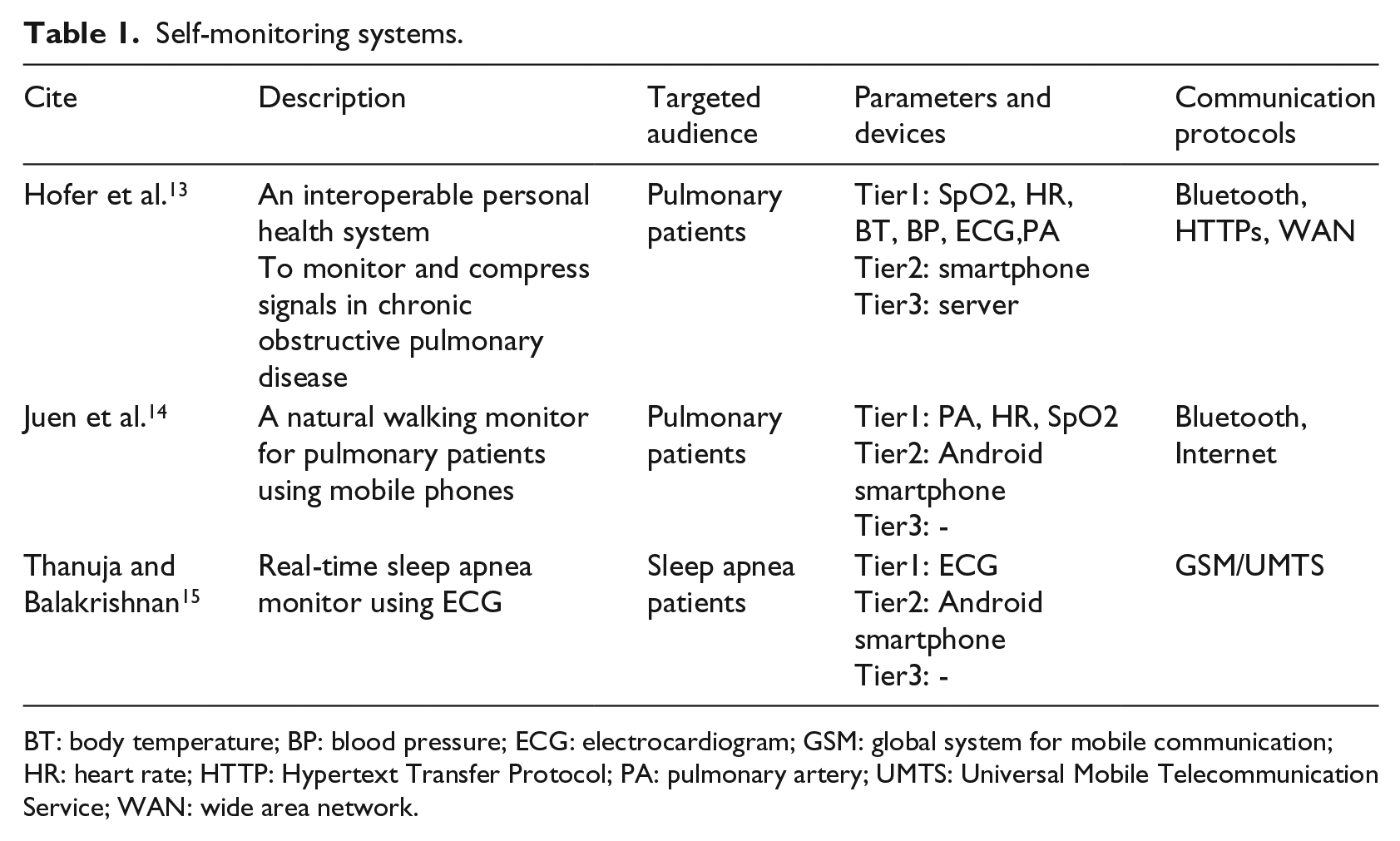
BT: body temperature; BP: blood pressure; ECG: electrocardiogram; GSM: global system for mobile communication; HR: heart rate; HTTP: Hypertext Transfer Protocol; PA: pulmonary artery; UMTS: Universal Mobile Telecommunication Service; WAN: wide area network.
Hofer et al. 13 propose a personal health system platform which uses Vital Sign Monitor1 (VSM1), a wearable medical sensor, to continuously monitor vital signs such as heartbeat, skin temperature, and movement/activity of patients with COPD. These sensor data are sent to an Android smartphone that acts as a data collector and are ultimately sent to an observation storage by means of interoperability standards. Compressed sensing techniques are also used to efficiently acquire and reconstruct each signal. Similarly, Juen et al. 14 developed a middleware software which runs on stand-alone smartphones with sensor chips similar to medical accelerometers to automatically detect the gait speed during natural walking to predict natural walking speed and distance during a 6-min walk test (6MWT) which is standard assessment for COPD and congestive heart failure. Thanuja and Balakrishnan 15 propose a sleep apnea monitoring system in smartphone using the matrix laboratory (MATLAB) tool. Electrocardiogram (ECG) sensors are used to record the heart activities and process the ECG signals to monitor obstructive sleep apnea episodes. The final output is then sent to Android mobile phone for alert.
Although some of the systems connect to a remote server to store and process the vital signs to notify the patients, they do not involve the interactions of healthcare professionals.
Assisted monitoring
Assisted-monitoring systems go beyond self-monitoring systems whereby the patients can request the assistance of an external health professional through SMS, phone calls, emails, and audio alarm in case of emergency. These systems usually consist of a WBAN, an MU, and a remote server. Most of the systems reviewed that provide assisted monitoring are focused on patients with asthma, risks of fall, cardiac disease, and any other chronic diseases (Figure 2).
Assisted-monitoring diseases.
Al-Dowaihi et al. 16 propose a prototype system whereby asthma’s patients can self-monitor and manage their health condition accurately, as well as informing the health professionals in case of emergency. The patients make use of a peak flow meter to measure the degree of obstruction in the airways, and these data are then sent to an Android mobile phone through Bluetooth. Then, the patient’s data are sent to the web portal. The medical staff perform daily check-ups and the health professionals monitor all the patients’ history, triggers, symptoms, and medications, and take appropriate actions.
Horta et al. 17 propose a system specifically for elderly patients suffering from the risks of fall. This system consists of three modules, namely (1) fall detection, (2) data processing and visualization of information from sensors, and (3) communication through web services with medical staff and external database storage. The built-in smartphone accelerometers detect the daily movements’ accelerations in order to detect user fall. The wearable body sensors (ECG, respiration, electrodermal activity (EDA), blood volume pulse, and electromyography) collect vital parameters and fall detection data that are sent to the smartphone through Bluetooth for biofeedback monitoring. The smartphone then sends the patient’s data to the web services that can alarm the medical staff.
Liu et al. 18 developed a novel family-based long-term healthcare monitoring system called “HealthKiosk” that provides rich contextual information and alerting mechanisms for any chronic conditions of elderly, children, and young fitness trainers. People suffering from any chronic disease can use their installed biomedical sensors (e.g. glucose meter, blood pressure, etc.) to take measurements. Then, the sensed data are sent to a small server or smartphone via existing communication networks like 3G, Wi-Fi, and Bluetooth. Afterward, the integrated data are sent to a backend support system where the clinical decision-supporting system processes the medical data and detects any deterioration to generate alert and invoke intervention of health professionals if needed.
The WellPhone presented by Moser and Melliar-Smith 19 is used as a personal health monitoring device which interfaces various health monitoring devices, such as blood pressure monitor, body weight scale, pulse oximeter, blood glucose meter, and accelerometer to the smartphone, and collects physiological data from those devices. This device provides feedback to the patients who are suffering from any chronic diseases by means of visualization and speech interaction, and alerts a health professional if needed.
SHARON is a novel tension-free mobile application system with implantable cardio defibrillator system and sensor mechanisms developed by Kumar and Ganesan. 20 It is specifically focused on people with cardiac diseases and uses built-in smartphone stethoscope. Alerts are triggered when patients reach critical level and an alarm is eventually initiated to be sent to the patients’ family members. The system also fixes appointment in the nearest hospital zone if necessary.
To summarize, these assisted-monitoring systems allow the patients to request the assistance of an external caregiver in case of emergency to whom only the data are forwarded (Table 2).
Assisted-monitoring systems.
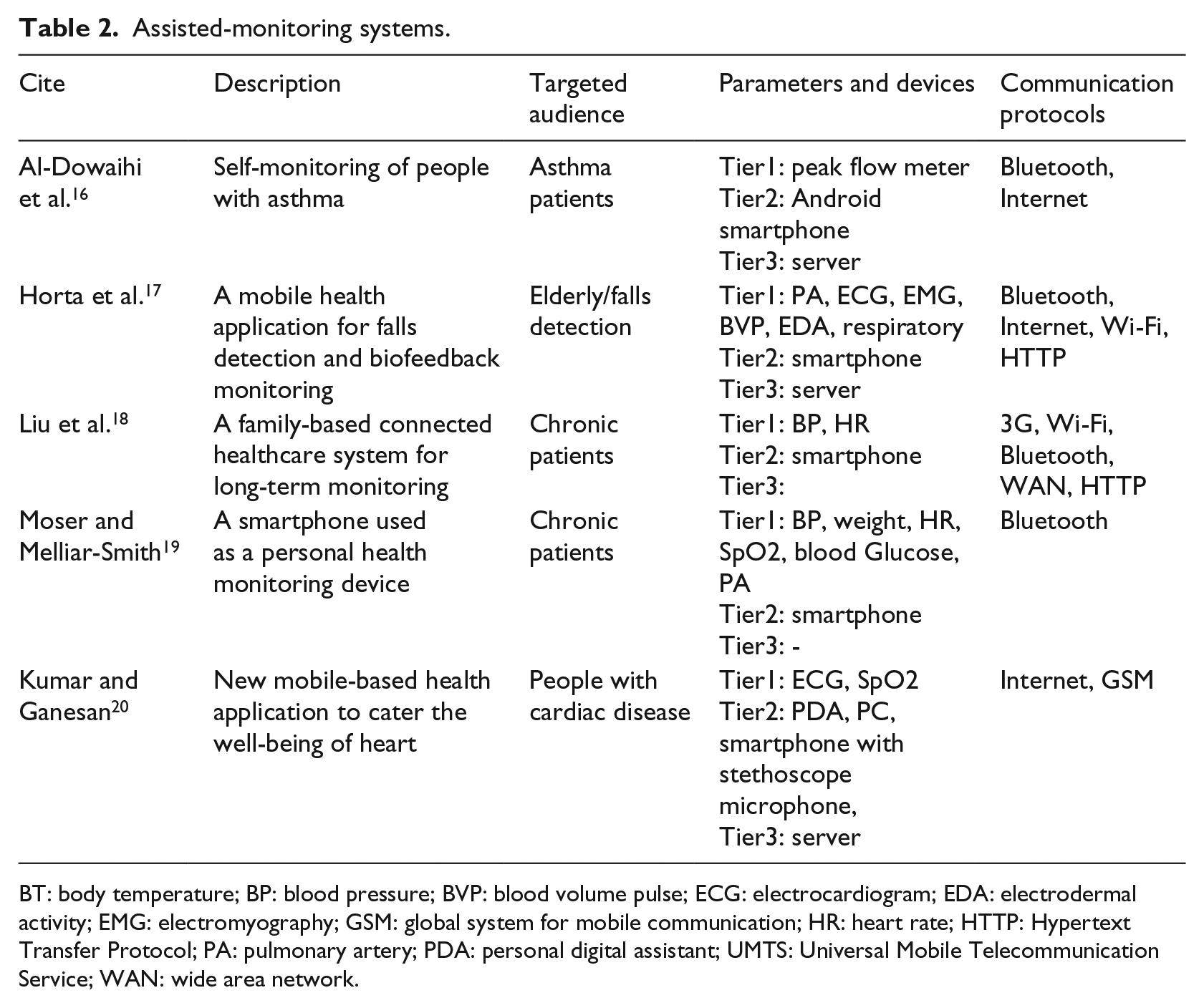
BT: body temperature; BP: blood pressure; BVP: blood volume pulse; ECG: electrocardiogram; EDA: electrodermal activity; EMG: electromyography; GSM: global system for mobile communication; HR: heart rate; HTTP: Hypertext Transfer Protocol; PA: pulmonary artery; PDA: personal digital assistant; UMTS: Universal Mobile Telecommunication Service; WAN: wide area network.
Supervised monitoring
Supervised monitoring goes a level beyond assisted monitoring whereby the health professionals not only intervene in case of emergency but instead all the physiological data are periodically sent and stored remotely for doctors, family, and friends to access the current and the past conditions of the patients or to configure the wireless body sensors remotely using a conventional web browser. Most of the systems are related to continuously monitor the health parameters of people suffering from cardiac diseases, hypertension, and any other chronic diseases (Figure 3), and they also include a component to manage emergency situations.
Supervised-monitoring diseases.
The system proposed by Nawka et al. 21 is either patient-driven or doctor-driven in case of emergencies, service-oriented, and provides a user-friendly interface for health management. It is based on ISO/IEEE11073 (X73) family of standards supporting high-quality medical sensors and uses the existing communication protocol for faster and reliable access to data. JavaScript Object Notation (JSON), a lightweight text-based open standard, is also used to represent data that are transferred between the system and remote server through the Hypertext Transfer Protocol (HTTP). The health professionals are connected to the remote server, and once the data are received, they perform their clinical diagnosis and transmit diagnostic reports with e-prescriptions back to the patients over HTTP.
Triantafyllidis et al.’s 22 system is based on unobtrusive vital signs monitoring through a non-invasive multisensing sensor, service-oriented architecture to handle any communication issues, and popular social service such as micro-blogging to share and discuss the recorded information within the patient’s community.
Rotariu et al. 23 propose a remote blood pressure and heart rate monitoring system for continuous long-time patient monitoring as a part of a diagnostic procedure. The patients can seek assisted healthcare if they are suffering from a chronic condition or supervised healthcare during recovery from any severe condition or surgical procedure. The system uses low-powered devices suitable for battery operation and high-peak performance. The PDA receives the blood pressure and heart rate values from the attached wireless blood pressure and heart rate monitor and sends alarms to the users (patient’s physician, healthcare specialist, ambulance center, or hospital) when these values exceed the preset limits. The PDA also communicates periodically to the central monitoring server through the Internet by using Wi-Fi or global system for mobile communication (GSM)/General Packet Radio Service (GPRS).
To summarize, in such systems (Table 3), once any abnormality is detected in the patient’s vital signs and behavioral patterns, a warning message is sent immediately to the health professional’s mobile phone in order to initiate the appropriate actions. A web-based interface is also used to synchronize data with the smartphone, to process and present data on a real-time basis so as to ensure a complete data analysis, precise health management, and on-time remote assistance for the patients by doctors and nurses.
Supervised-monitoring systems.
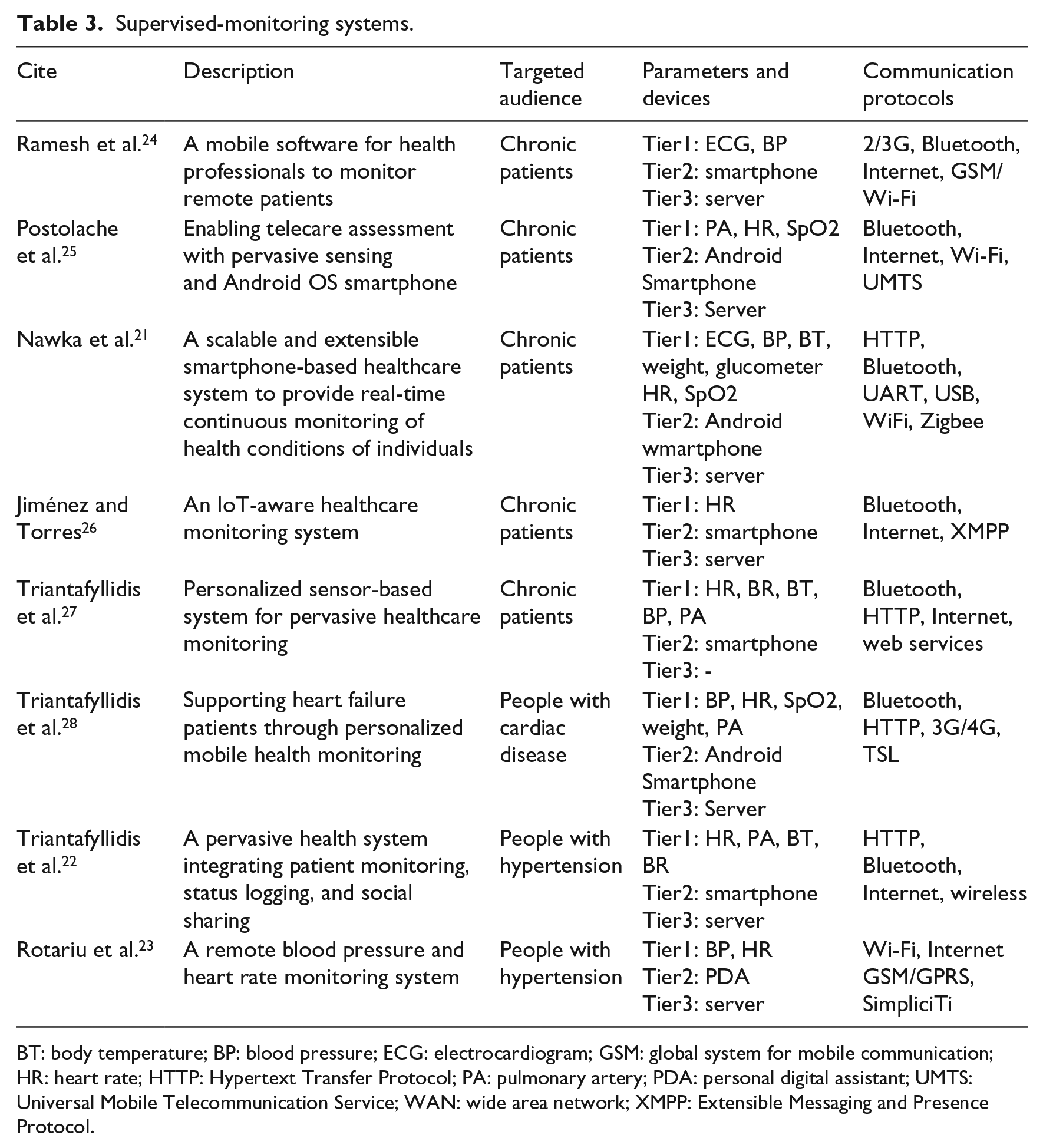
BT: body temperature; BP: blood pressure; ECG: electrocardiogram; GSM: global system for mobile communication; HR: heart rate; HTTP: Hypertext Transfer Protocol; PA: pulmonary artery; PDA: personal digital assistant; UMTS: Universal Mobile Telecommunication Service; WAN: wide area network; XMPP: Extensible Messaging and Presence Protocol.
Continuous monitoring
Continuous-monitoring systems not only include all the functionalities of self-monitoring, assisted monitoring, and supervised monitoring but also comprise of a shared approach between the patient and health professionals. Such systems collect and analyze physiological signs on a real-time basis using intelligent techniques which correlate data from multiple sensors in order to offer real-time assistance or preventive actions to the patients. These systems are devised specially for people suffering from stress, cognitive impairment, dementia, or Alzheimer who require real-time continuous monitoring and assistance (Figure 4).

Continuous-monitoring diseases.
Abbate et al. 29 proposed MIMS, a minimally invasive monitoring sensor, that provides comprehensive and customizable health monitoring services, especially to elderly patients suffering from cognitive impairment, risks of falls, dementia, and Alzheimer’s disease. MIMS offers active and passive 24×7 monitoring of patients’ physical activities and vital signs. The sensed data are analyzed preceding potential emergency events using advanced intelligent systems in order to predict them quickly.
Duarte et al. 30 developed a mechanism for indoor patient monitoring for medical purposes which rely on real-time continuous sensing algorithm to determine the location of a patient inside his or her home at each moment. Medical specialists continuously monitor the daily activities of patients and detect changes in the patients’ behavior that could be interpreted as early signs of any health-related issue.
Majeed et al. 31 proposed a mobile monitoring healthcare system for the chronic patients who need long-term nursing care and thereby decreases the need for patients to go to the hospital visits or stay. The system senses the patients’ physiological parameters, monitors the patient status, and ultimately notifies center and records the patients’ details that can be accessed by the physician from anywhere and anytime.
Zhang et al. 32 presented deStress, a mobile and remote stress monitoring system that monitors and manages stress. Patients’ psychological stress data are collected, analyzed, and shared with healthcare professionals. Moreover, a feedback approach is presented that is based on adaptive respiration to set the ideal personalized respiration parameters and consequently adjust the patient respiration frequency to alleviate the stress.
To summarize (Table 4), these continuous-monitoring systems use intelligent algorithms in order to provide continuous and ubiquitous information flow between the patients and healthcare professionals. These systems provide both real-time interventions in response to critical event alerts and also provide preventive customized feedback.
Continuous-monitoring systems.
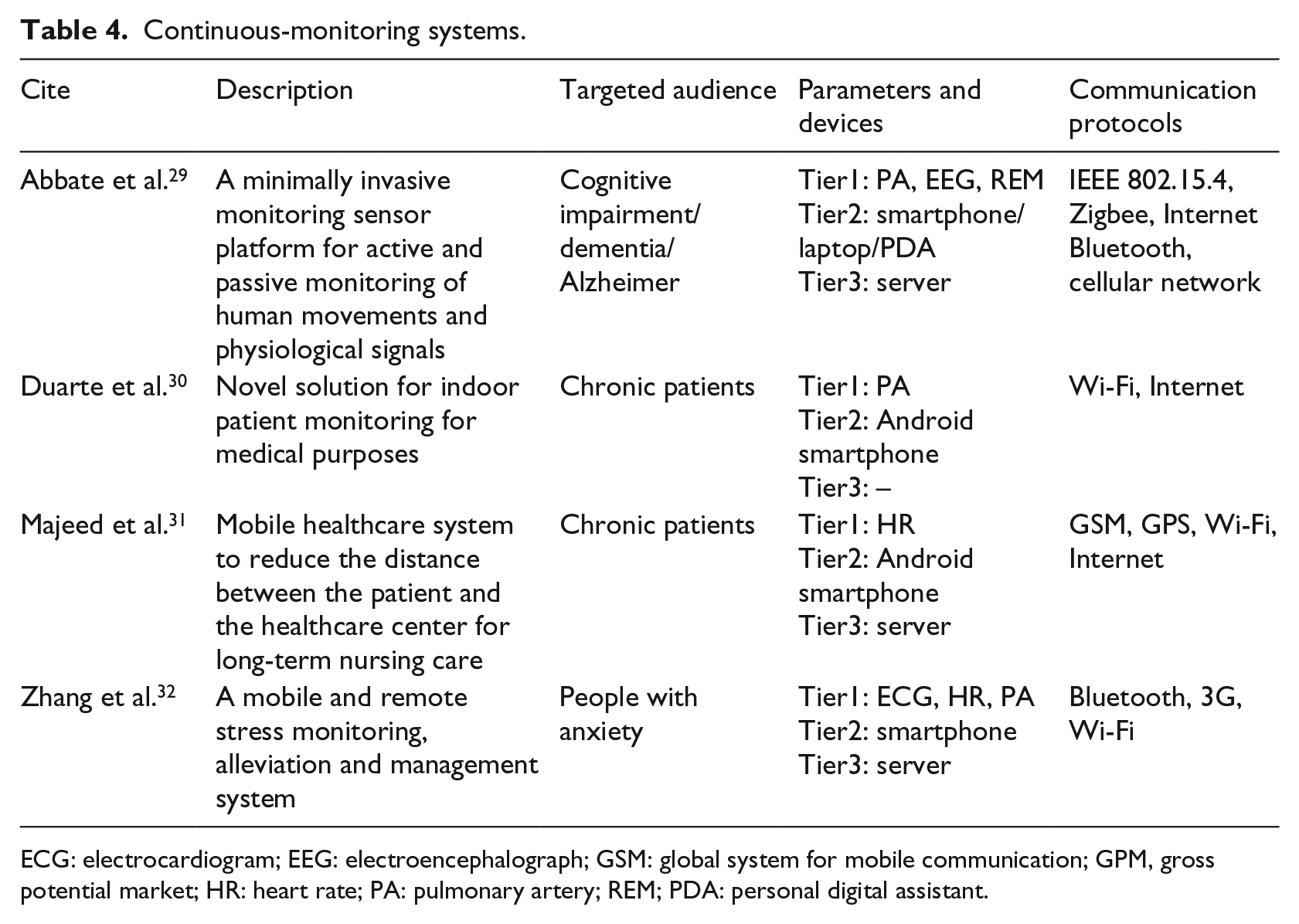
ECG: electrocardiogram; EEG: electroencephalograph; GSM: global system for mobile communication; GPM, gross potential market; HR: heart rate; PA: pulmonary artery; REM; PDA: personal digital assistant.
General results
The following section evaluates the 20 existing PMHSs and most of them are targeted toward chronic and elderly patients suffering from diseases. Most systems are developed on either wireless local area network or wireless personal area network. The PMHSs use various sensor devices and mobile phones to capture or transmit the physiological data. In order to transmit the data, common communication protocols, such as Wi-Fi, Bluetooth, Internet, 2G/3G/4G, and ZigBee, are used. Most systems are developed on architectures like client–server, web-based, or stand-alone. The user acceptance is usually influenced by specific motivations and incentives, and different decision-making techniques are used for intelligent decision making. The different aspects of the systems such as the target audience, the sensor types used, the types of architectures of the PMHSs, the communication protocols to transfer information, contextual information/parameters monitored, incentives and motivation triggers, and decision-making techniques in different PMHSs are presented and discussed.
Target audience
PMHSs are developed for a target audience of chronic or elderly patients suffering from illnesses like COPD, cardiac diseases, asthma, sleep apnea, hypertension, stress, cognitive impairment, dementia, Alzheimer’s, risks of fall, and many other chronic conditions. These PMHSs are mostly convenient to patients who prefer home and out-patient care rather than hospitalization. Many other patients are geared toward these systems since they can easily tap into patient-centric healthcare services whereby healthcare professionals can assist them in the diagnosis and treatment of their conditions and consequently adding value to their life. In fact, Boulos et al. 33 highlighted that the higher adoption rate of smartphones by elder people and patients with chronic disease will depend on cost, usability, awareness, and the type of technology.
Sensor types
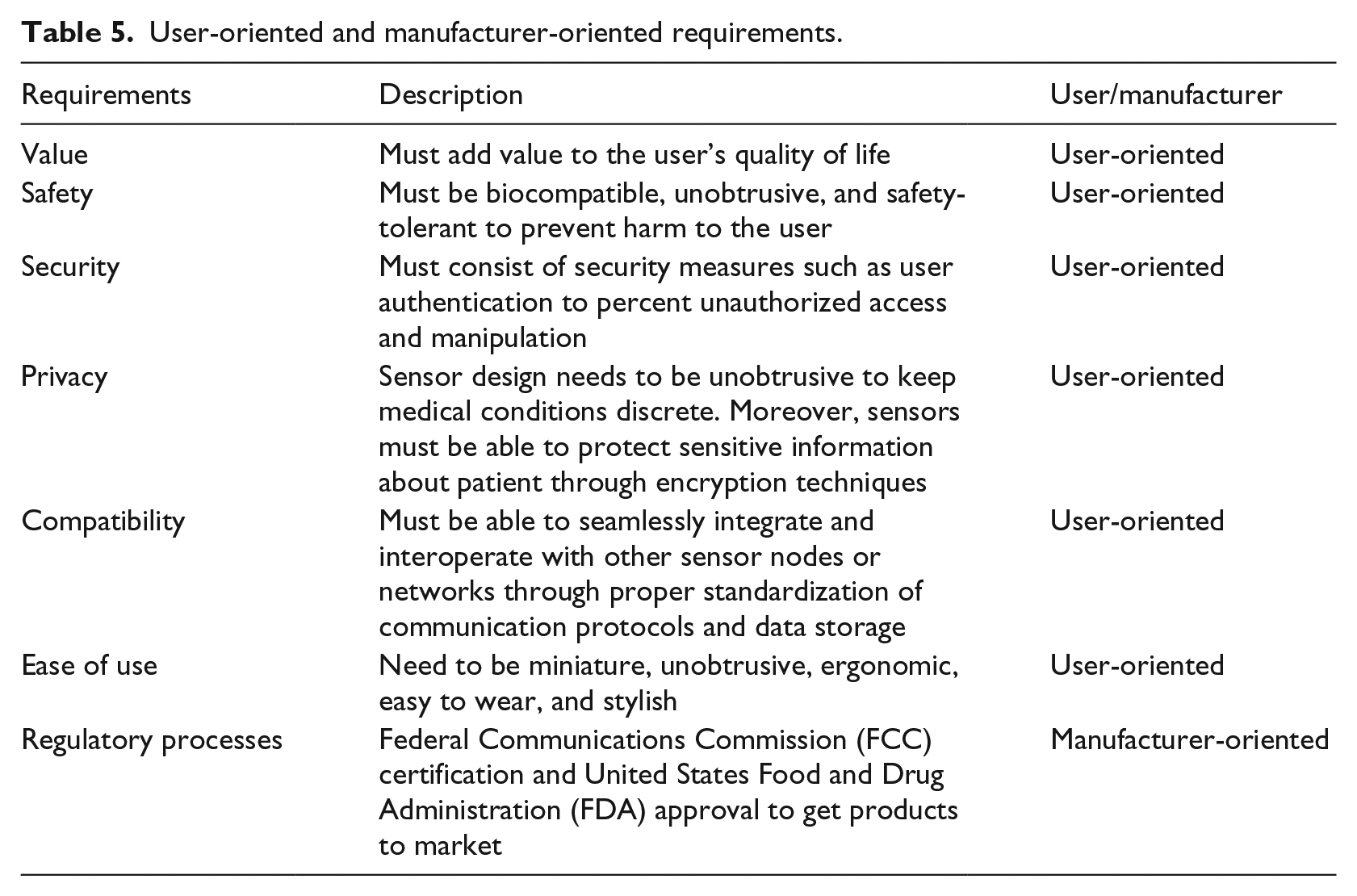
Sensor nodes are usually composed of either on-body or implantable nodes. All sensor nodes are equipped with wireless transceiver unit, mini processor, and energy supply device like battery. They sense, collect, and process various physiological vital signs of patients. These sensed data are then forwarded to an access point using a wireless interface. Widespread sensors’ adoption and diffusion depend on several factors 34 involving both the user and the manufacturer as shown in Table 5. Common sensor nodes used in setting up PMHSs are accelerometer, glucometer, blood pressure, respiration, ECG, electroencephalograph (EEG), electromyography (EMG), electrooculography (EOG), pulse oximeter, and body temperature.
User-oriented and manufacturer-oriented requirements.
Contextual information/parameters monitored
Wireless sensor devices are used to continuously collect and transmit the physiological vital signs so as to monitor health of patients and offer timely intervention and healthcare services. Out of the 20 studies that were analyzed (Table 6), most of them used accelerometers or mobile phone in-built accelerometers to measure the physical activity, heartbeat, and respiration of the individuals.14,19,32
Sensors and parameters monitored.
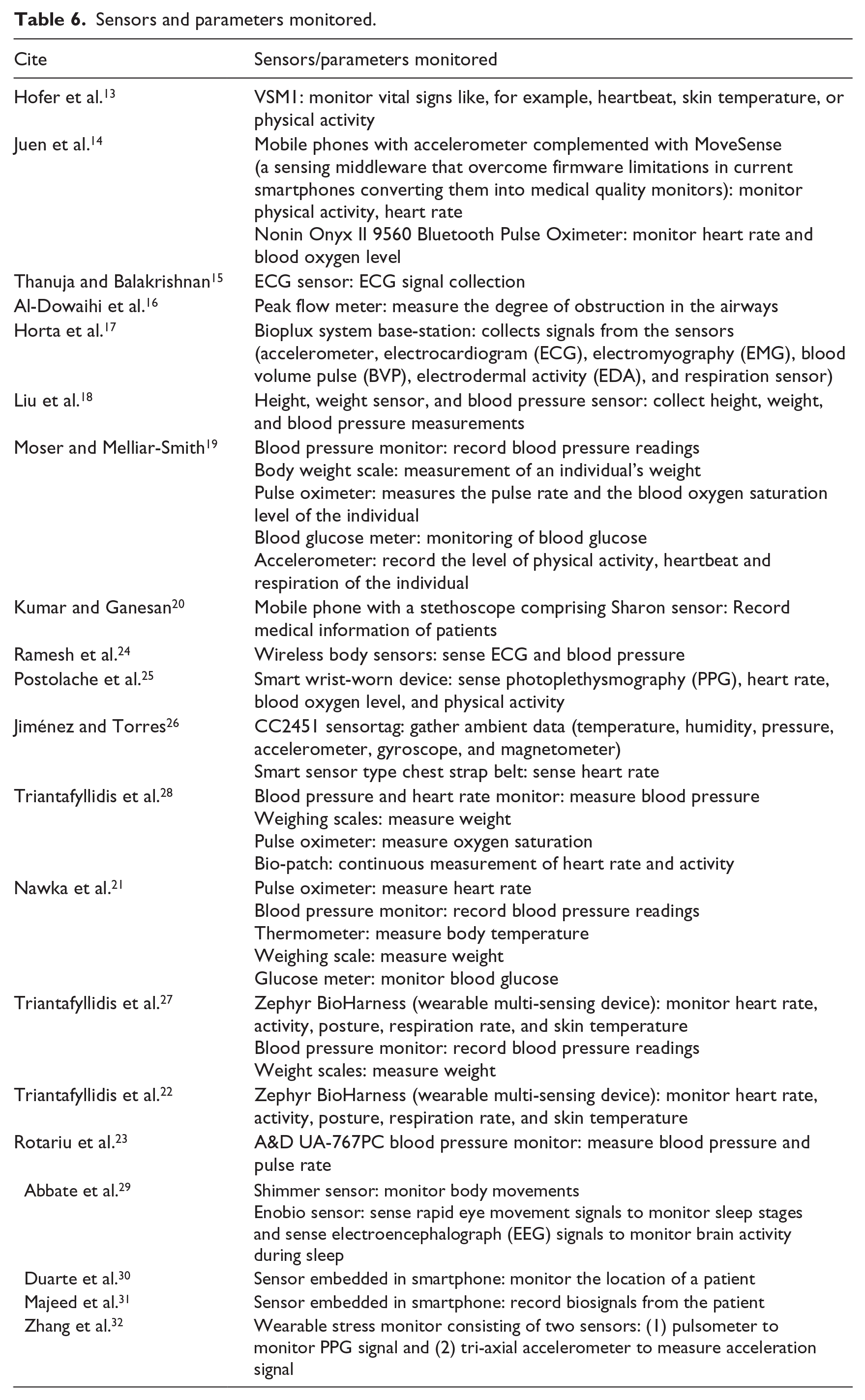
Pulse oximeters are also commonly used to monitor heart rate, ECG, and blood oxygen level.14,19,21,28 Height 18 and weight18,19,21,28 sensors are used to measure the height and weight of individuals. Thermometers are also used in the measurement of body temperatures. 21 A peak flow meter is used to measure the degree of obstruction in the airways, especially in asthmatic patients. 16 Blood pressure monitors are used to collect readings of the blood pressure18,19,21,24,27,28 and heart rate 23 of the patients. A blood glucose meter is essential to monitor the blood glucose level of patients.19,21
VSM1 is a wristwatch-type wearable medical device that is placed on the patients’ upper arm. It has sensors in direct contact with the skin and continuously monitors vital signs such as heartbeat, skin temperature, and movement/activity for patients suffering from COPD. 13 Smart wrist-worn devices are also used to sense photoplethysmography (PPG), heart rate, blood oxygen level, and physical activity for chronic patients. 25
Zephyr BioHarness is a wearable multi-sensing device that monitors heart rate, activity, posture, respiration rate, and skin temperature22,27 for chronic and hypertensive patients. The Bioplux system base-station is a device that consists of a big range of health sensors, such as the accelerometer, ECG, electromyography (EMG), blood volume pulse (BVP), EDA, and respiration sensor that collects the patients’ signals to detect risks of falls. 17
Jiménez and Torres 26 used CC2451 sensortag to gather vital data about temperature, humidity, pressure, accelerometer, gyroscope, magnetometer, and smart sensor type chest strap belt to monitor the heart rate of patients.
Abbate et al. 29 use the Shimmer sensor to monitor body movements of patients, and Enobio sensor that senses rapid eye movement (REM) signals to monitor sleep stages and senses EEG signals to monitor brain activity during sleep for patients suffering from cognitive impairment, dementia, or Alzheimer’s.
To summarize, it is of paramount importance that all the sensed contextual information or parameters meet the standards of quality of information (QoI) and which is ultimately essential for fast, reliable, timely decisions, and user acceptance.
Communication protocols
Sensor data from existing PMHSs are currently being communicated to the access point using various communication protocols such as 2G/3G, 3G/4G, Bluetooth, Wi-Fi, and GSM/Universal Mobile Telecommunication Service (UMTS), IEEE 802.15.4, ZigBee, UBS, and GPRS. Sensor data are often transferred to the remote station using Internet or Simple Object Access Protocol (SOAP) over HTTP. Since the PMHSs involve many biosensors, interactions with mobile phone, remote, and web servers, it is very important to consider the qualitative aspect of the communication protocol. The connectivity should be stable and without interference during any exchange of information so that the systems are efficient and performant.
Architecture of PMHS
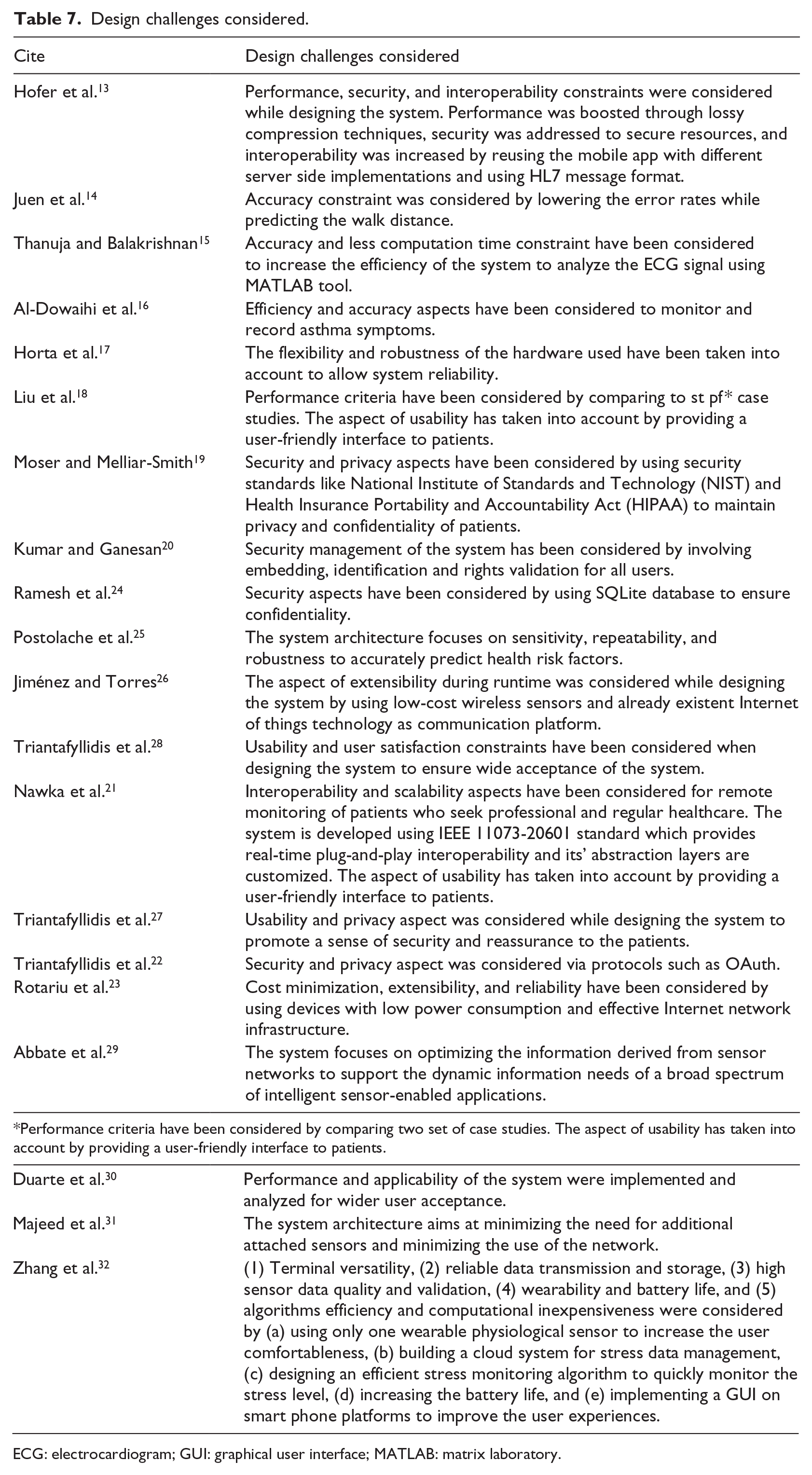
The commonly used architectures to develop PMHSs are client-–server, web-based, or stand-alone. Systems using a client–server or web-based share the same type of architecture and usually consist of three Tiers, namely Tier 1 (WBAN), Tier 2 (Access Point—AP), and Tier 3 (Remote Server). Tier 1 refers to the wireless communication between body sensor nodes and AP, Tier 2 is used to transfer the sensors data to the remote server using appropriate communication protocols, and Tier 3 refers to the remote server that provides just-in-time monitoring of received data. Stand-alone architectures use the mobile phone as both the sensor and AP. While designing the architecture of the PMHSs, several design challenges are taken into consideration (Table 7) to improve the adoption of such systems.
Design challenges considered.
ECG: electrocardiogram; GUI: graphical user interface; MATLAB: matrix laboratory.
Motivations and incentives
With the advancement and prevalence of PH applications, user acceptance has become a pertinent criterion that needs to be met besides the proper functioning of the system. Very few research focus on user acceptability and important factors that persuade people to accept and use health monitoring systems. 35
According to the study of Aflaki et al., 35 user acceptance is dependent on intrinsic motivations and extrinsic incentives. As depicted in Figure 5, intrinsic motivations are any activity that excite people to do something for the sake of enjoyment of the activity itself, whereas extrinsic incentives are external factors which are designed to influence behavior of people. Therefore, when intrinsic motivations match extrinsic incentives, that is, if what motivates people from inside matches facilities and supports provided externally, the system acceptance will be greater.
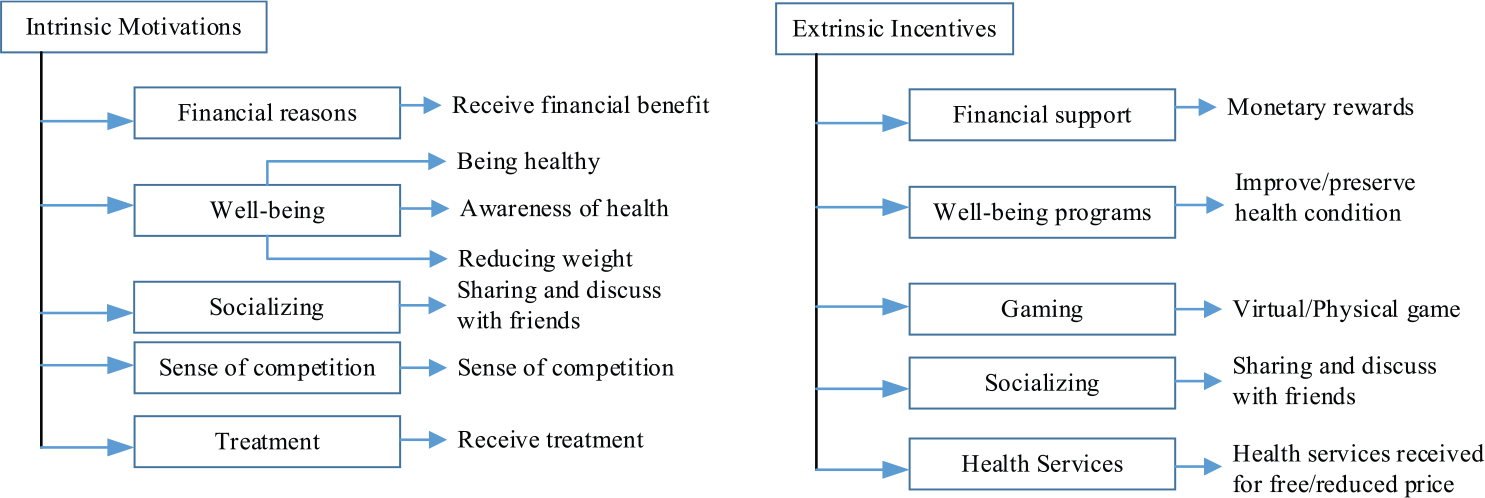
Intrinsic motivations and extrinsic incentives.
Motivations and incentives for self-monitoring systems
Table 8 shows that in self-monitoring systems, both intrinsic motivations and extrinsic incentive factors that influence patients’ behaviors are well-being programs whereby the patients self-monitor their health parameters to ensure a preventive lifestyle and early diagnosis to help them stay healthy and preserve their well-being.
Incentives and motivations for self-monitoring systems.
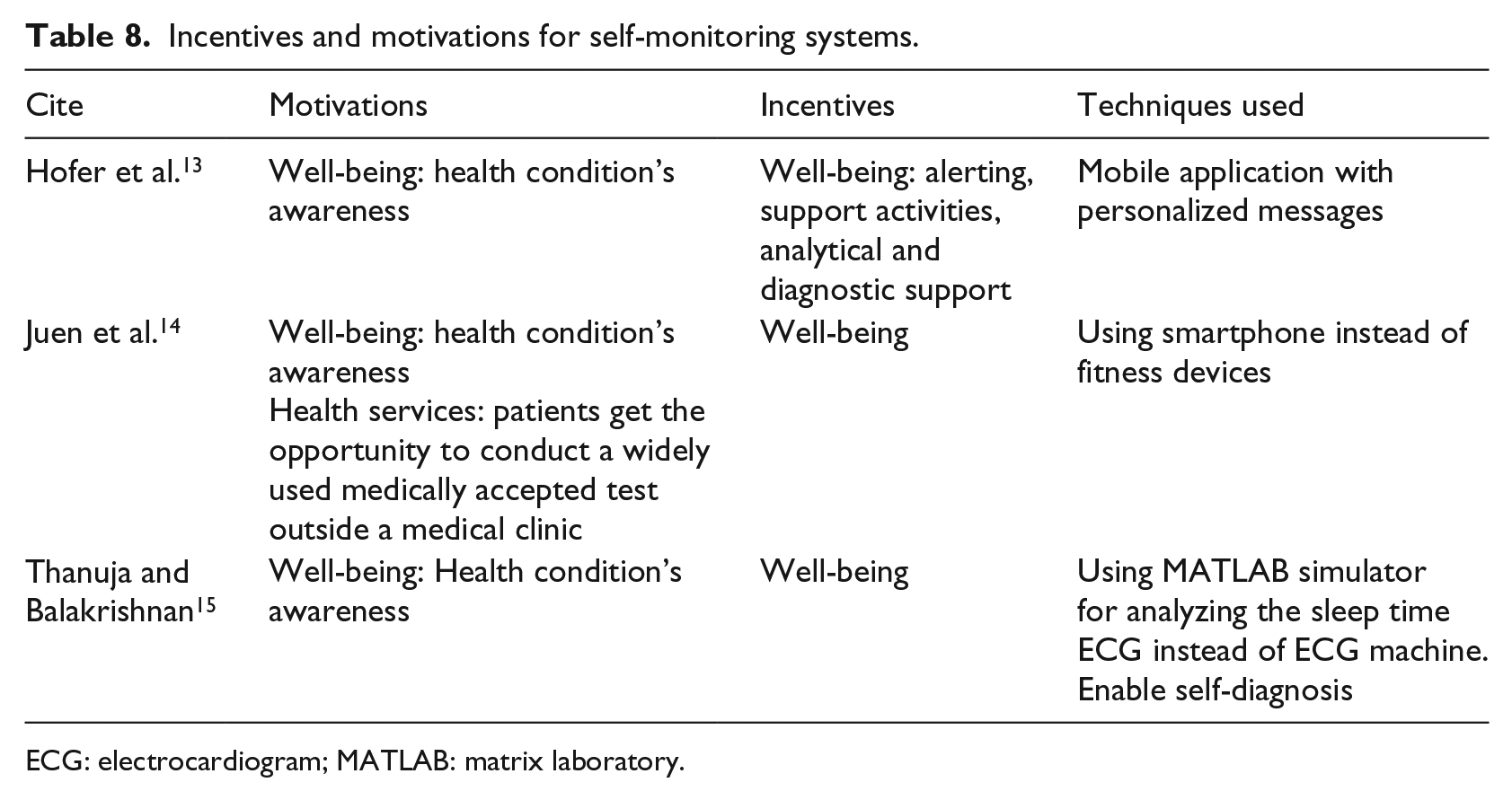
ECG: electrocardiogram; MATLAB: matrix laboratory.
Motivations and incentives for assisted-monitoring systems
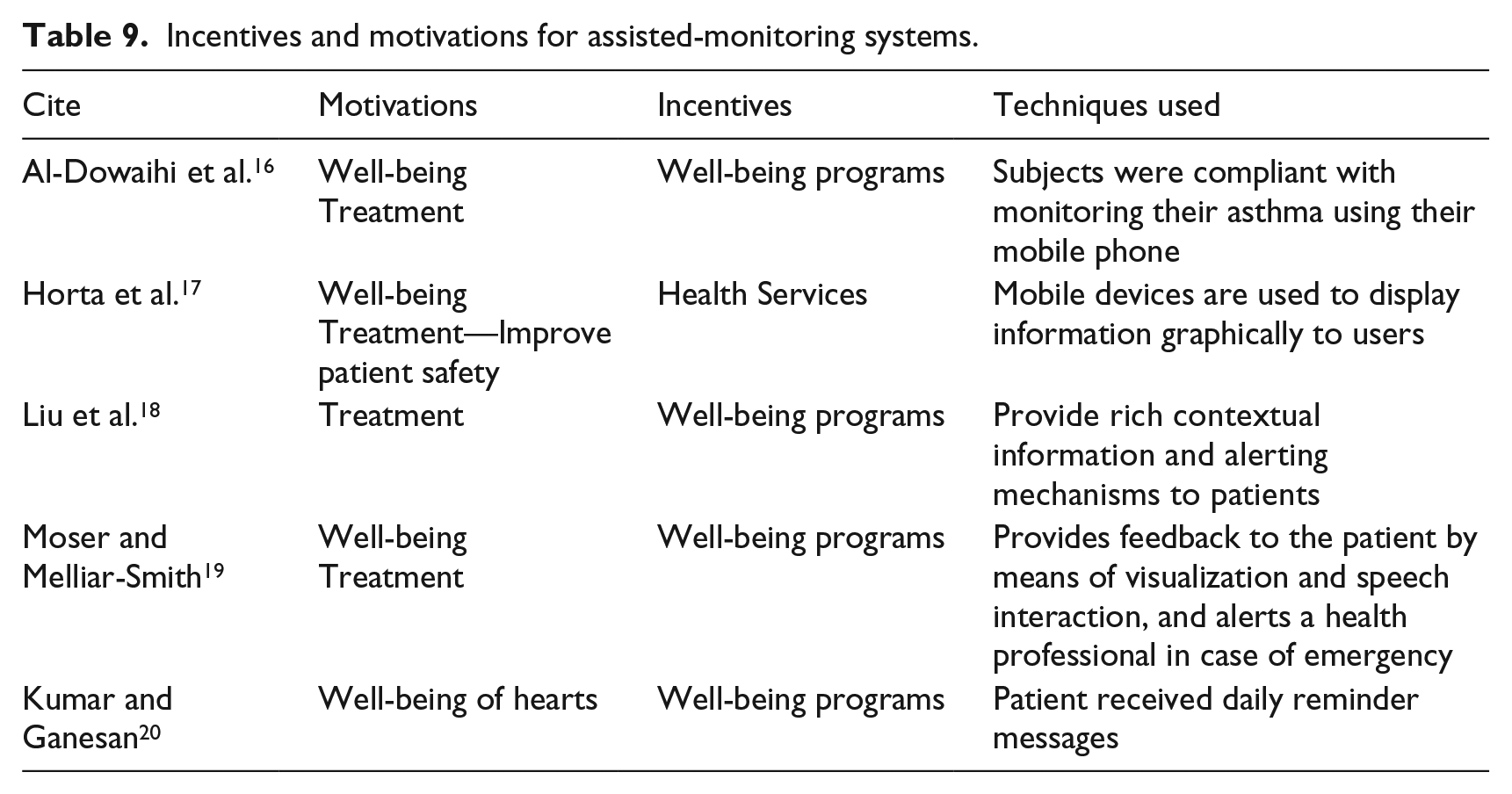
Table 9 shows that in assisted-monitoring systems, intrinsic motivations factors that influence patients’ behaviors are related to their well-being, such as awareness of their health conditions,16,17,19 well-being of their hearts, 20 and of the treatment16 –19 they receive based on the diseases they are suffering from. Most extrinsic incentives factors are related to well-being programs16,18,19 and health services for a free/reduced price.
Incentives and motivations for assisted-monitoring systems.
Motivations and incentives for supervised-monitoring systems
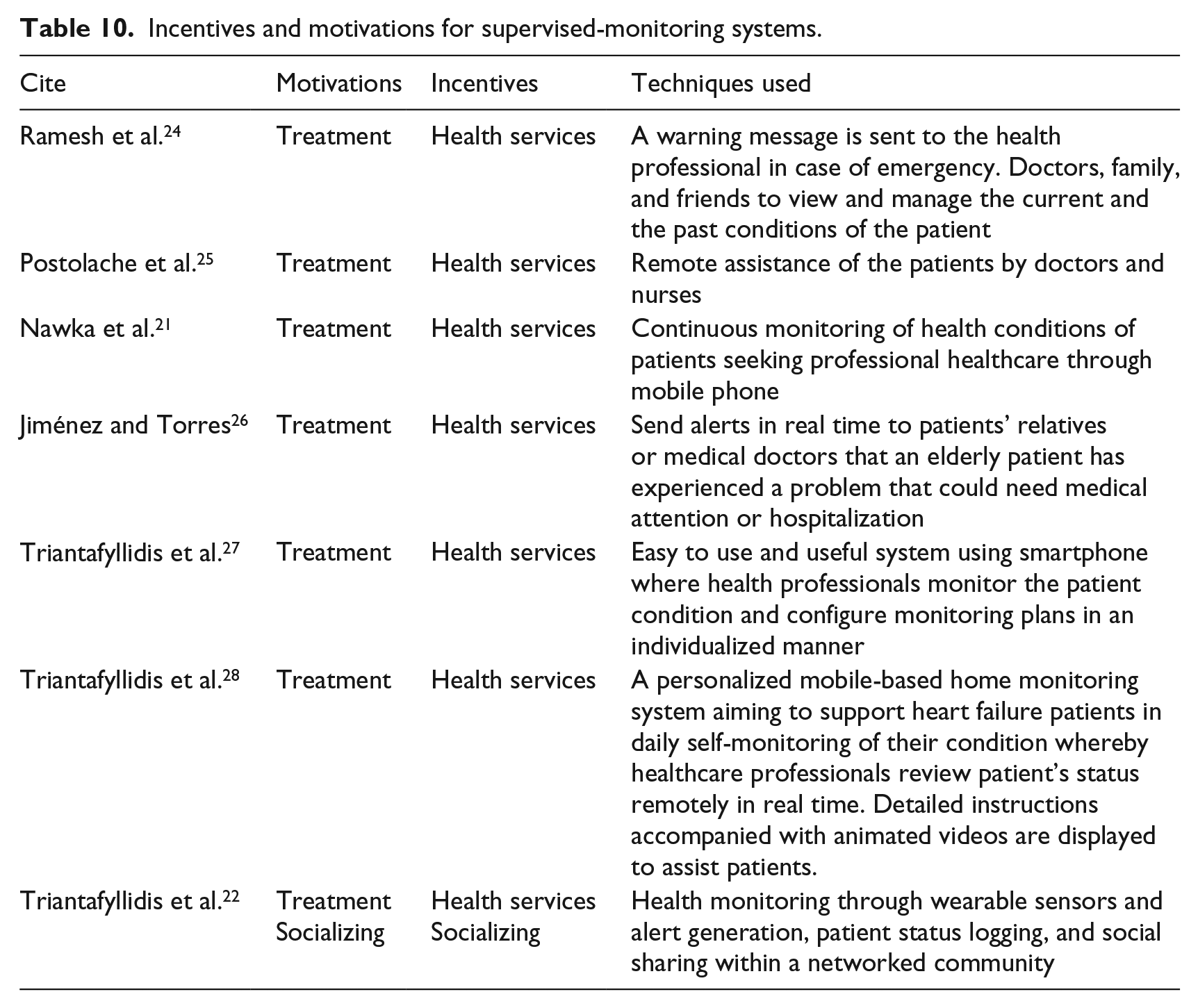
Table 10 shows that in supervised-monitoring systems, both intrinsic motivations and extrinsic incentives factors that influence patients’ behaviors are related to the treatment they are receiving for the diseases they are suffering from and the real-time health services they are provided with.21 –27 In Triantafyllidis et al.’s 22 system, the intrinsic motivation and extrinsic incentives are linked with social sharing where the patients can discuss their symptoms and health conditions with their relatives and community network for better health support.
Incentives and motivations for supervised-monitoring systems.
Motivations and incentives for continuous-monitoring systems
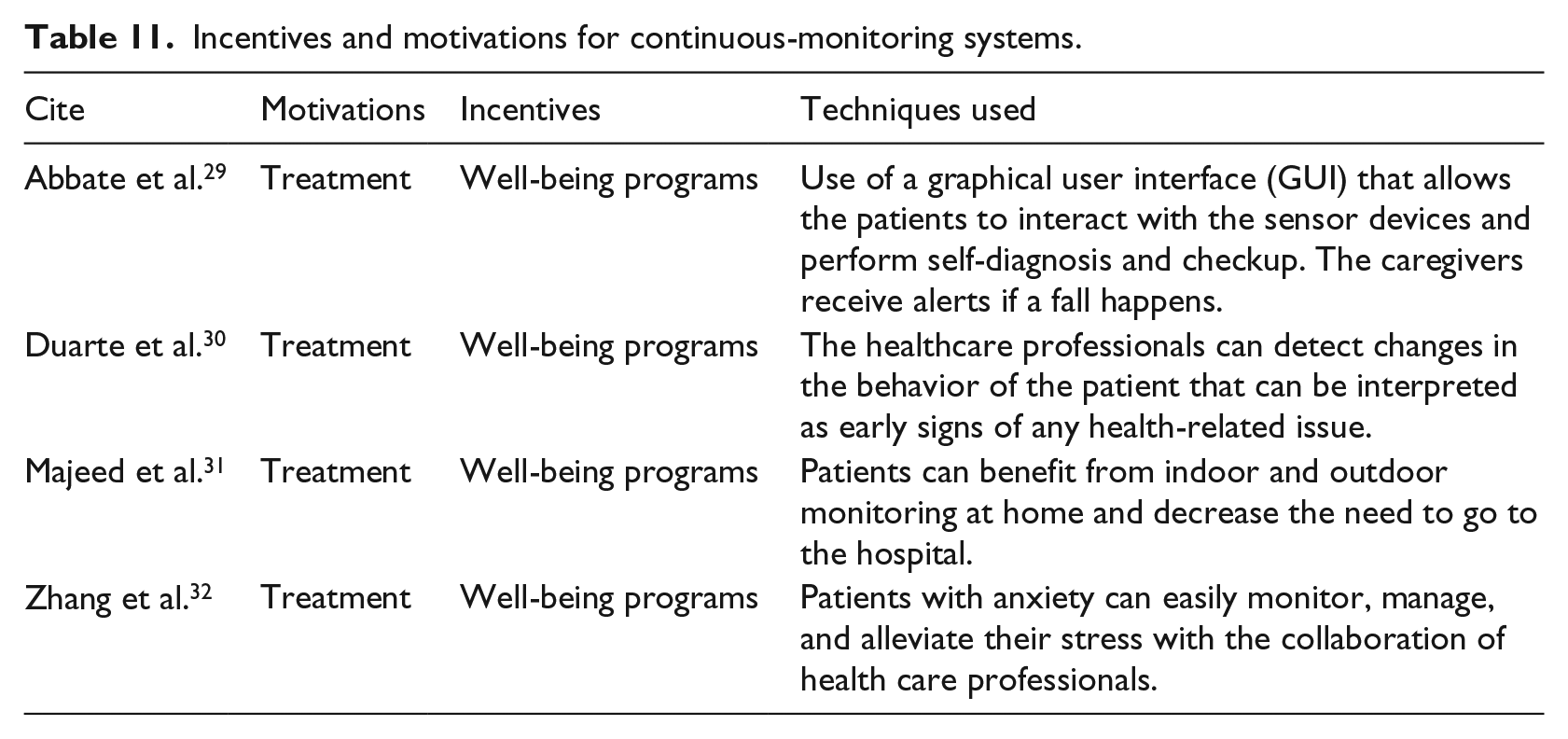
Table 11 shows that in continuous-monitoring systems, intrinsic motivations that influence patients are the treatment they receive and extrinsic incentives factors are related to their well-being whereby patients benefit from the two-way approach between patients and health professionals so that they receive a real-time continuous monitoring healthcare service and just-in-time intervention.
Incentives and motivations for continuous-monitoring systems.
Decision-making techniques
Data mining and machine learning techniques such as Decision Trees, Artificial Neural Networks (ANN), Fuzzy Logic, Hidden Markov Model (HMM), Support Vector Machine (SVM), Bayesian Classifiers, Bayesian Networks, and clustering techniques like k Nearest Neighbor (kNN) and k-Means are usually used in many research for intelligent decision making. 36
Abbate et al. 29 used the machine learning techniques, such as the Support Vector Machine (SVM), Bayesian networks, and reinforced learning, to develop an intelligent gathering module in the event classification algorithms. Juen et al. 14 used the Gaussian Process Regression (GPR) model for treadmill walking, a three-layer ANN using the genetic algorithm to minimize the mean square error and an SVM with Fisher’s linear kernel and an epsilon of 0.01 in the insensitive loss function. The HMM is used as a print proposed methodology in the research proposed by Kumar and Ganesan 20 and is compared with histogram recognition technique to evaluate the number of successful health transactions based on various timing intervals for sample training set.
Other data mining techniques such as dynamic assignment techniques have been used by Majeed et al. 31 to design and tune multimedia and also to ensure high-speed data transfer. Moreover, Liu et al. 18 proposed a lightweight process engine which runs a simple data processing logic and defines reusable data operations. The processing logic is composed of an aggregation operation to aggregate any received data, a transform operation to transform the combined data in a certain format, and a security operation for encryptions.
Discussion
In this section, the challenges of the 20 PMHSs are evaluated at different levels, such as node, network, and human-centric. Node-level challenges are related with the sensors’ design and energy consumption without violating their unobtrusiveness. Network-level challenges are related with data collection and transmission without violating the security and privacy. Finally, the human-centric challenges are related to (1) the degree of system acceptance, (2) sensitivity, and (3) mobility of sensors whereby a patient can access high-quality medical services anywhere and anytime, (4) standardization, and (5) interoperability.
Node-level challenges
Sensor technology
Despite the fact that there is a plethora of sensors, there is still a need for data integration models to be used in PMHSs so that one device can be used to monitor a patient for multiple conditions. 29 The sensor design is a key factor to improve PMHSs’ performance. Common sensors used are accelerometer, ECG, EEG, pulse oximeter, blood pressure, body temperature, respiration rate, and so on. Most patients also prefer wearable sensors over implantable sensors due to their high cost and the need of chirurgical operation.
Efficiency/power consumption
One of the biggest challenges and problems is energy consumption of sensor devices used in PMHSs. This has a high impact on the acceptance and compliance level of PMHSs. Low power consumption remains an important characteristic of wireless devices. 23 In Ramesh et al., 24 power consumption is estimated and then the energy is optimized to increase the battery life of smartphone by 6 h. Other systems 18 make use of RESTful design to collect data which reduce the power requirements on sensors, leading them to be more portable and energy efficient. Compressive sensing techniques are also used to reduce energy consumption. 13 Despite the use of low-power wireless devices, robust energy techniques and intelligent algorithms are still needed to sustain extensive power consumption during persistent communications. 22 Low-power monitoring sensors will attain importance as PMHSs evolve. Moreover, the energy techniques and other dynamic algorithms should be explored for greening the PMHSs. 24
Network-level challenges
Effective methods for data collection
Using optimized techniques for high QoI during data collection in PMHSs is crucial for correct diagnosis of the patients. Advanced signal processing algorithms associated with vital signs assessment are used for efficient data collection. 25 However, optimization of QoI for data collection in sensor networks remains to be further explored. In addition, time stamping and ordering of events, synchronization of different sensors are open problems for study and research.
Reliable transfer of data
Reliable data transmission is a key factor in PMHSs. Delayed sensor data can lead to incorrect diagnosis, inappropriate treatments, and untimely decisions. In Triantafyllidis et al., 27 sensor-specific APIs are used to transmit encapsulated sensor data in the response message to ensure reliable data transfer. Dynamic publish/subscribe mechanisms are used to ensure messaging reliability by publishing and discovering data automatically at runtime. 13 Moreover, low transmission power and small-sized antennae of wireless sensor devices usually result in reduced signal-to-noise ratios that consequently increase the bit error rate and reduce the reliable coverage area. Reliable data transfer should be investigated since it is still a challenge for PMHSs.
Security
Ensuring security during data collection and transmission from sensors to access point and from access point to remote server is highly critical for successful design and acceptance of PMHSs. Some systems19,21 have been using encrypted Bluetooth wireless communication, cellular telephony communication, and encrypted Internet communication to ensure data security and prevent possible data tampering or hijacking. To reinforce the need of secure PMHSs, security standards like National Institute of Standards and Technology (NIST) and Health Insurance Portability and Accountability Act (HIPAA) need to be followed. Moreover, very few systems are using encrypted or cryptography techniques to protect the data, so there is still a high need for such techniques to be developed and enhanced. 29 In Triantafyllidis et al., 22 protocols such as OAuth are used to ensure authentication. Other web-based PHMSs13,18 also make use of REST services to ensure authentication and authorization of users to login the system.
Privacy
Several studies have converged to the point that ensuring data privacy of patients is of vital significance in PMHSs.21,29 The physiological signal-based authentication method is proposed in Moser and Melliar-Smith 19 to ensure privacy of patients. In Triantafyllidis et al., 22 protocols such as OAuth are used to maintain privacy. Status alert messages are also used to notify physicians about patients. 27 Secure connection over an encrypted channel is established with the Server. 21 Very often, inadequate privacy protection consequently reduces the patients’ willingness to adopt PMHSs. Thus, privacy-preserving mechanisms should be developed for acceptance of PMHSs and to ensure data integrity.
Human–centric challenges
Technology acceptance
The technology acceptance of users is especially important for successful adoption of PMHSs. Triantafyllidis et al.22,27 surveyed the level of user-friendliness of their PMHSs with a limited number of subjects. Yet, it is crucial to explore the usability of the system with different groups of users since each user has a different kind of interaction with the system. Proper technical support and training are very essential to ensure broader acceptance of PMHSs, especially by elder patients and those with low technology literacy. Moreover, very few systems focus on the user-friendliness and natural interfaces with immediate response capabilities, and thus, there is a high need to perform more studies to assess the technology acceptance of PMHSs.
Sensitivity of sensors
The sensitivity of the sensor devices can be affected due to various environmental conditions, thereby reducing the sensitivity of wearable sensors or increasing the need of recalibration. Despite many systems are using sensors in the PMHSs, few of them happen to mention the importance of sensitivity. Yet, more exploration is needed in this aspect in terms of self-calibration algorithm, and sensitivity enhancement algorithm.
Mobility
Proper communication network is important to ensure that patients are connected anytime and anywhere with other devices, data centers, and healthcare centers. 31 The use of mobile devices, tablets, smartwatches, and sensors are important for mobility, especially during prolonged period.15,17,29,30 PMHSs can provide additional support to patients and promote mobility through unobstructed, ubiquitous, and continuous monitoring. 25 In Abbate et al., 29 multi-hop and ad hoc sensor networks are used to promote mobility.
Standardization
Nowadays, the development and adoption of standardization are becoming fundamental in all PMHSs so that these systems can operate in a multidisciplinary environment and be technology independent of their vendors. In Nawka et al., 21 Jiménez and Torres 26 and Abbate et al., 29 open standards such as IEEE802.15.4-based ZigBee are used to ensure low-cost and low-power short-range wireless communication networks. It is crucial that open architectures are adopted so that sensor node services are easily integrated with the existing medical services infrastructure.
Interoperability
A seamless flow of information among heterogeneous sensors over a network is of utmost importance for more accessible systems. To ensure interoperability, standard data format and protocols can be used. Continua Design Guidelines (CDG) are used by Hofer et al., 13 to some extent, due to hardware limitations. Medical Markup Language (MML) and Health Level Seven International (HL7) are used to define representations for physiological measurements.13,19 Different software and protocols are also used to address the issue of interoperability. 29 In Hofer et al. 13 and Nawka et al. 21 IEEE 11073-20601 specification has been used to provide interoperability between various health sensors. Thus, the propagating use of standards is crucial to address the aspect of interoperability in PHMSs.
Open research challenges
PMHSs have immense opportunities for monitoring chronic diseases, but at the same time, such systems give rise to several challenges. These systems are very critical and complex since they demand high dependability, reliability, security, and privacy for successful adoption and acceptability. Due to these complexities, many research challenges are still open. The challenges are discussed in the section below and are categorized under the node-level, network-level, and human-centric level.
Node-level challenges
Sensor technology
In PMHSs, wearable sensor devices are battery powered, and there are always design challenges from the hardware and software constraints arising from the form factor, lightweight, cost-effectiveness, energy efficiency, unobtrusiveness, sensing reliability, sensing and transmission coverage, and safety requirements for daily continuous health monitoring. So it is of high importance to consider safety and sustainability requirements while designing the sensors.
Efficiency/power consumption
Moreover, in order to address the issue of limited power resources, energy harvesting, an alternative to power sensor nodes, can be used to convert the ambient energy into electrical energy for optimized lifetime and performance. 37 Optimization algorithm using particle swarm optimization (PSO) can also be further explored and applied to a certain extent to address wireless sensor network issues such as optimal deployment, node localization, clustering, and data aggregation. 38 However, it is still crucial to evaluate the optimized algorithms using PSO for different network density. 39 Also, PSO usually needs a significant amount of memory for processing and is not very suitable for high-speed real-time applications. 40
Network-level challenges
QoI
Another challenge lies on the network level. Ensuring QoI during data collection, data processing, and data delivery in PHMSs is a major challenge as guaranteeing QoI in PHMSs is hardly possible. PMHSs need to satisfy the degree of confidence of QoI through various quality dimensions such as timeliness, accuracy, reliability, completeness, relevancy, usability, and confidentiality, so that relevant and timely decisions can be taken by patients and medical experts. Higher QoI in PMHSs will allow capture of regular measurements, thus promoting better day-to-day healthcare follow-ups through reliable diagnostics, monitoring, and clinical guidance. Thus, it is a huge challenge to ensure that the most significant data can always be delivered in a real-time manner due to frequent deep fading and packets loss.
Prathap et al. 41 highlight the importance of on-time and reliable data delivery at the network level. Moreover, several quality of service (QoS) parameters such as end-to-end packet delays, packet delivery ratio, average energy consumption per packet, and routing overhead for variable source traffic loads and wireless link bit error rates are considered in order to ensure high QoI. In order to improve the QoS, the study discusses about the commonly used routing algorithms, namely (1) energy-efficient differentiated directed diffusion mechanism (EDDD), (2) multiconstrained QoS multipath (MCMP), (3) multipath multi-speed protocol (MMSPEED), and (4) LOCALized Multi-Objective (LOCALMOR). EDDD is energy efficient but neither scalable nor adaptive. Moreover, the algorithms, MCMP and MMSPEED, consider link delay and reliability as routing decision parameters but not energy efficient. LOCALMOR achieves the on-time and reliable data delivery but it is not scalable.
Despite all the research being conducted, the challenge is still to design an effective routing protocol that uses a dynamic mechanism to automatically detect sensors in the network that remain static for long periods of time for data aggregation and propagation as a single transmission.
Security and privacy
Moreover, security and privacy constraints are an indispensable component that should be met for widespread adoption of PHMSs. Very often, authentication and data integrity are difficult tasks in limited resources of medical sensors. Fundamental security specifications, such as data confidentiality, integrity, availability, accountability, storage, and access control, are of paramount importance and are key challenges when implementing PMHSs. 42 Therefore, advanced algorithms, authentication protocol, encryption methods, and efficient cryptography methods should be further developed to prevent data tampering, hijacking, or any other attacks. 43 Other techniques like secure software protocols for routing and data aggregation can be implemented.
Human–centric challenges
Another major challenge often faced by PMHSs are human-centric issues. Since the PMHSs are usually used to target various aged groups with different diseases, it is essential that both technology-naive and technology-averse patients are able to use the PMHSs with ease. Concerning the sensitivity and mobility of sensors, it is equally important that users are seamlessly connected to the wireless network and they can move around freely anywhere and anytime despite any environmental conditions. 6 Novel link quality metrics and handover mechanisms should be further developed to ensure that sensor nodes are seamlessly connected to the access points. 44 Although Technology Acceptance models are available, user acceptance patterns should be further investigated, evaluated, and verified for PMHSs adoption. 45 Despite many PMHSs are on the shelf, extending the network lifetime in such systems remains one of the greatest challenges since wireless sensor devices are unable to operate for long time due to their limited power resources. Therefore, further research can be done with regard to energy harvesting to address the issue of energy consumption. 46 Moreover, reduction of motion artifact, low-power design, on-node processing, and distributed interference in wireless networks still need to be addressed to enhance the usability and functions of these devices for practical use.
The emerging deployment of PMHSs is triggering a worldwide paradigm shift from reactive to preventative healthcare whereby design considerations play a very important role in addressing the challenges outlined. These systems offer a variety of exciting opportunities from a healthcare perspective, such as encouraging self-healthcare, assisted healthcare, supervised healthcare, and continuous monitoring.
Conclusion
This article presented a review of state-of-the-art PMHSs that are widely used in medical applications, with particular focus on issues and challenges related to PMHSs. Given the fact that PMHSs are been introduced at an exponential rate to provide smart healthcare to different patients, researchers have started to explore technological solutions to enhance the provision of healthcare in a way which complements existing services. In this article, 20 PMHSs from 2011 to 2016 are evaluated to improve patients’ quality of life, and various prominent issues are outlined for design considerations during PHMSs development. A more significant data set from different medical informatics libraries (100 papers over a period of 10 years) can be considered as future work, and other criteria such as user acceptance, adoption, and QoI can be extensively considered. From the results, it is seen that common diseases such as COPD, heart diseases, asthma, sleep apnea, hypertension, stress, cognitive impairment, dementia, Alzheimer’s, risks of fall, and many other chronic conditions are monitored mainly for elderly or chronic patients. Moreover, client–server and web-based architecture appears to be the most common choice for the use of PMHSs. The systems make use of various wireless communication protocols to transfer sensor data from sensor devices to access points and also to remote servers. Various sensor devices are used in order to collect the vital physiological signs of the patient for disease monitoring. However, as pointed out, there are a number of challenges that remain to be tackled at the sensor level, network level, and human level. There are still many future works to be done to achieve a perfect compromise among all the design considerations when developing PMHSs. Despite all these challenges, a paradigm shift in healthcare delivery model from doctor-centric to patient-centric, from acute reactive to continuous preventive, and from sampling to monitoring is noticed in the trend. The confluence of PMHSs development can lead to exponential advantages in the healthcare sector mainly in continuous monitoring applications. In the near future, the evolution of PMHSs can significantly improve the health conditions and lifetime expectation for various patients. The current challenges faced when designing PMHSs were outlined, and the main areas that researchers should investigate further for successful deployment, adoption, and seamless integration of PMHSs in patients’ life were discussed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.