
Abstract
Over 90% of US hospitals provide patients with access to e-copy of their health records, but the utilization of electronic health records by the US consumers remains low. Guided by the comprehensive information-seeking model, this study used data from the National Cancer Institute’s Health Information National Trends Survey 4 (Cycle 4) and examined the factors that explain the level of electronic health record use by cancer patients. Consistent with the model, individual information-seeking factors and perceptions of security and utility were associated with the frequency of electronic health record access. Specifically, higher income, prior online information seeking, interest in accessing health information online, and normative beliefs were predictive of electronic health record access. Conversely, poorer general health status and lack of health care provider encouragement to use electronic health records were associated with lower utilization rates. The current findings provide theory-based evidence that contributes to the understanding of the explanatory factors of electronic health record use and suggest future directions for research and practice.
Introduction
Health information technology and health communication strategies are recognized as key tools to improve population health outcomes and achieve health equity. 1 Mapping out the progress toward these goals, the US national health objectives include the increase in the number of people who use electronic health records (EHR), feel capable finding information online, and use the Internet to communicate with their health providers. 1 In parallel with setting the goals for EHR use, a national program was created to provide incentives for the adoption and meaningful use of EHR systems by health providers and consumers. 2 The earlier aims of the incentive program supported by the Centers for Medicaid and Medicare Services have focused on creating data capturing infrastructure (Stage 1) and advancing clinical processes (Stage 2). Now approaching Stage 3, the meaningful use incentive program looks for further development of EHR into a tool for the improvement of health outcomes and health self-management.
Access to health information can lead to greater patient empowerment and better health outcomes. 3 Over 90% of US hospitals support online patient portals that provide patients with access to e-copy of their health records that contain laboratory test results, list upcoming appointments, provide summaries of past visits, and allow patients send messages to health care providers. 4 A sizable body of research looked at the uptake of technology for health communication and information seeking. The use of EHR creates opportunities for patient support and empowerment in complex medical situations, 5 such as cancer treatment. In the provision of care for cancer patients (i.e. those with the history of cancer diagnosis), EHR can be used to serve as quality control measures for discovering missed diagnosis opportunities, 6 create and implement comprehensive cancer survivorship care plans, 7 and provide a channel for education, communication, and information seeking for cancer patients. 3 Provision of and access to cancer-related information play a role in the support of effective coping with cancer and improved understanding of cancer disease management. 8 Despite its positive effects, health information can also lead to increased uncertainty about health status, recognition of the complexity of illness management, or diminished hope for a desired but unlikely health outcome. 9 Consequently, information behaviors can range from engaged information seeking to intentional information avoidance. 10 Dissemination of reliable information about prevention and treatment can also support uncertainty management associated with cancer diagnosis and recurrence. 11 EHR and patient portals are tools for information dissemination that afford patient empowerment, and their use can serve as its indicator. Patient empowerment can be defined as a greater participation of patients in health decision-making and self-management activities. 5 Going beyond deficit-model education approaches and support of treatment adherence, EHR can empower patients through personalization of information (e.g. by providing patients with convenient access to their test results and relevant health management and disease prevention tips). 12 It also supports collaborative communication enabling patient sharing of pertinent health information and active participation in the process of health management. However, despite the possible benefits and availability of EHR, only 27% of US health consumers regularly use this technology. 13 The lack of understanding of patient information-seeking behavior presents a significant barrier for the successful engagement of patients with the technology and its continued use. 14
The factors that explain information behavior and the use of different health information channels have been conceptualized within the framework of the comprehensive model of information seeking (CISM).10,15 The original conceptualization of CISM assessed individual and channel factors of information-seeking behaviors from communication with health care providers. CISM predicts that individuals’ predispositions to search for health information are influenced by demographics, direct experience, salience, and beliefs. Individual factors act as antecedents to information content and channel preferences. Prior research has found that demographic factors, such as age, sex, race, education, and income level, are associated with health information seeking, and disparities in access to information can contribute to the digital divide. 16 Although the number of Americans, including minorities, who access the Internet for health information continues to grow, some disparities associated with low socio-economic status are still prevalent. 17 Besides the demographic factors, prior experience with and general orientation toward online health information have been identified as precursors of EHR use. 17 Finally, health information behavior can be affected by the beliefs about access efficacy and cultural norms related to the desirability and necessity of the access to health information. 15
This article acknowledges the role of social factors and showed that channel factors should not be viewed in isolation but rather they should include social interaction. This means that the information management process as it relates to information seeking and repeat use of an information source is a social process. Such social information management allows formulating a proposition that information seeking is affected by both channel factors and social information management factors. CISM has been used in context of different online health information channels that present and passively distribute information, like online webpages. The first hypothesis, therefore, extends the application of CISM-defined individual factors for information seeking to predict the use of EHR:
H1. The level of EHR use among cancer patients is associated with the individual information behavior factors of demographics, prior experience, salience, and access efficacy beliefs.
The second group of factors identified by CISM is associated with the characteristics and perceived utility of access to a particular information carrier. Characteristics of access refer to the trust toward the information source, 18 which in the context of electronic transmission of information and EHR use has also been associated with the perceptions of information security. 19 The perceived value of accessing health information has been positively associated with patient-reported health status. 20 Carrier factors account for channel accessibility as well as information needs and preferences of health consumers. 11 Information needs of cancer patients have been shown to depend on the stage of cancer, 15 as well as their overall health status, which in turn determine the utility of an information carrier to a health consumer. Research on the information behaviors among cancer patients showed more broad and active information seeking among those in earlier stages of cancer and focused on direct communication with a health provider and limited additional information seeking by those with more progressed cancers. 10 Therefore, the second hypothesis extends prior research on the characteristics and utility of access to and use of EHR:
H2. The level of EHR use among cancer patients is associated with the EHR access factors of perceived information security and utility.
Methods
Source of data
The data came from the National Cancer Institute’s Health Information National Trends Survey (HINTS) 4, Cycle 4, which was collected via mail surveys (N = 3677) between July and November 2014 (National Cancer Institute, 2015). As with previous surveys, the sample included those who have had a cancer diagnosis (n = 542) and those who have not. Information seeking can vary greatly between those who have been diagnosed with cancer and those who have not; 10 therefore, only responses from participants who identified themselves as cancer patients were included.
Variables and measurement
Guided by CISM, individual information behavior factors included demographics, prior experience, salience, and access efficacy beliefs. Demographic variables included age, sex, race, income, and level of education. Direct experience was assessed with two questions that asked about the respondents’ use of email or apps to exchange medical information with a health care professional in the past 12 months. Salience and applicability of access to EHR were assessed with nine items that measured how interested participants were in exchanging information about appointment reminders, tips, medical reminders, lab/test results, diagnostic information, vital signs, lifestyle behaviors, symptoms, and digital images/videos with a health care provider electronically. The scale showed high reliability (α = 0.94). Finally, beliefs about the norm of EHR access were measured with responses to the statement, “You should be able to get to your own medical information electronically.”
Access factors included perceived security and utility of EHR use. Following the original conceptualization, the characteristics of information source were operationalized as the extent to which EHR is considered a secure source of information. Therefore, security perceptions toward EHR use were assessed by one question that asked whether respondents were concerned about the security of their medical information when it is sent electronically from one health care provider to another. In addition, because communication with health care providers can influence online health information seeking, the question asking whether a health care provider has offered access to EHR was included in the analysis to assess its impact on the utilization of EHR as a source of health information. Finally, CISM conceptualized utility of EHR to depend on the health status. Therefore, self-reported health status variable was included in the model.
EHR use behavior, the dependent variable, was measured by one question, “How many times did you access your personal health information online through a secure website or app in the past 12 months?”
Analytic procedures
A hierarchical regression was used to test the hypotheses. Individual information behavior factors were entered in the first block of the model and EHR use factors were entered in the second block of the model. Also, because the hypotheses focused on testing a previously developed model, weights for population-level estimates were not used.18,21 Results are reported as unstandardized coefficients with 95% confidence intervals.
Results
The level of EHR use was expected to be associated with the personal factors (H1) of demographics (age, sex, race, education, and income), prior experience, salience (interest in accessing health information electronically), and EHR access beliefs. H1 was supported, R2 = 0.28, F(7, 439) = 24.66, p < 0.001, and, as shown in Table 1, individual information behavior factors explained significant amounts of variance in the current use of EHR. Among demographic variables, higher income level was associated with more frequent use of EHR (b = 0.03, standard error (SE) = 0.02, 95% confidence interval (CI) = 0.001–0.06), but none of the other variables were significant predictors. Also, as predicted, prior experience (b = 0.95, SE = 0.11, 95% CI = 0.72–1.17), salience, (b = 0.14, SE = 0.05, 95% CI = 0.05–0.23), and access beliefs (b = 0.14, SE = 0.07, 95% CI = 0.01–0.28) were found to be significant predictors.
Regression of EHR use on personal information behavior and EHR access factors.
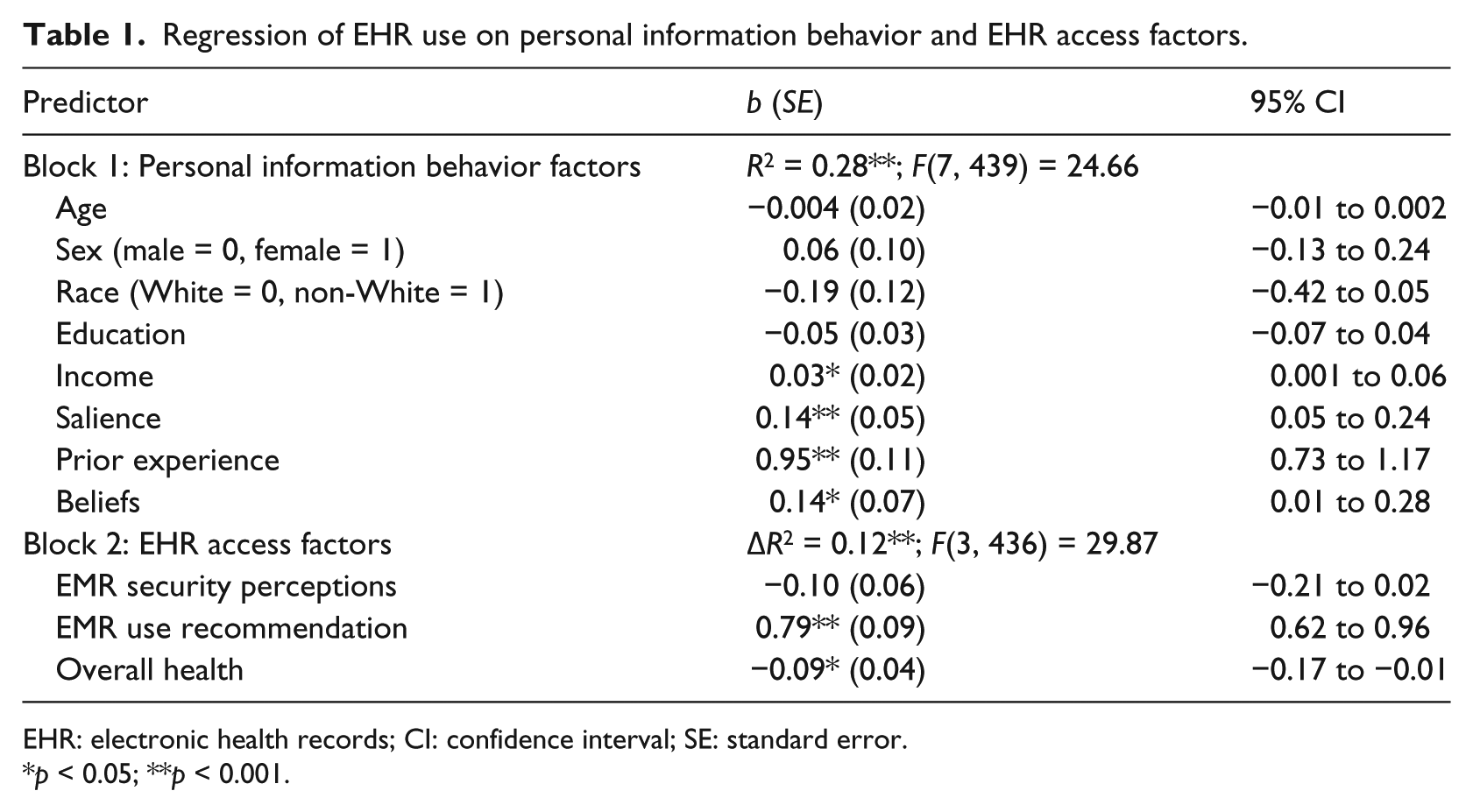
EHR: electronic health records; CI: confidence interval; SE: standard error.
p < 0.05; **p < 0.001.
The level of EHR use was also expected to be associated with the access factors of perceived security characteristics and utility of EHR (H2). This prediction was supported, and access factors have shown significant variance in EHR use, ΔR2 = 0.12, F(3, 436) = 29.87, p < 0.001. Specifically, general health status was a significant negative predictor of EHR use (b = −0.09, SE = 0.04, 95% CI = −0.17 to −0.01), and low health status rate was associated with less frequent EHR use. Furthermore, health provider encouragement for the use of EHR was a strong positive predictor (b = 0.79, SE = 0.09, 95% CI = 0.61 to 0.95). Although the perception of the safety of electronic health information sharing did not reach significance, its p value (p = 0.09), signals that health consumers could have concerns related to the protections of their health information.
Discussion
This study looked at the use of EHR reported by cancer patients who participated in the HINTS. Guided by the CISM,10,15 this article identified the factors that explain the use and barriers to greater adoption of EHR among health consumers. The results of this study showed that CISM is an applicable theoretical framework for the analysis of EHR use among cancer patients. The results of this study showed that CISM is an applicable theoretical framework for the analysis of EHR use among cancer patients. As predicted by CISM, salience of health information use online, prior experience using online health information, and beliefs about the importance of access to EHR serve as explanatory antecedent factors for EHR use.
This study has several notable findings. First, only income approached significance among the demographic factors. Although higher level of income was identified as a demographic predictor of EHR use, other factors that were previously associated with the digital divide, such as gender and age, 18 were not significant predictors of EHR use among cancer patients. Information-seeking behavior is dependent on patient characteristics, 22 and income emerges as a factor that acts as an antecedent for EHR use across the age and race groups of cancer patients and has been continuously identified as a significant predictor. 8 These findings correlate with other research that showed that the use of technology for access to health information is no longer dividing across the racial line, but the findings related to other demographic variables bring in new evidence that the use of health information technology (IT) is becoming widespread.16,23
Next, the importance of salience as a predictor of EHR use and high reliability of the scale used to measure it indicates that health consumers could be involved in health information exchange in a number of ways. Health behavior tips and lifestyle behaviors were among the types of health information types that were sought after by cancer patients. These information types are key in providing cancer education, and EHR could be used as a rich source of information exchange between health care providers and patients.22,24 While this study focused on cancer patients, future studies could assess the promise of EHR to provide cancer prevention and screening.
The findings also showed that channel and utility characteristic explain the use of EHR, and those who rated their health lower are less likely to access the information. This study has two theoretical implications related to the continued development of CISM as a conceptual framework. First, previous applications of CISM have looked at cross-sectional situations of information seeking, when a particular need for health information is either satisfied or not satisfied through information seeking depending on the personal and information carrier factors. 25 However, both personal and carrier factors affect continued use of technology for health information uptake. 14 This study extends the application of CISM to explain the differences in frequent repeat use of an information carrier channel. As a proposition, it could be stated that personal and information carrier factors are predictive of the initial and continued use of a health information channel. The second theoretical contribution made by this article is related to the application of CISM to an interactive information behavior. Previous applications have focused on non-interactive information seeking and the dimension of an information behavior that ranges from information seeking to avoidance.25,26 Applied to the EHR, which afford two-way communication, this study extended the use of CISM and showed that previously identified personal and information carrier factors form a stable predictive model. This finding could be formulated as a proposition that personal and information carrier factors are predictive of the use of information channels that afford interactive, two-way communication between patients and health care providers.
Applied to the practice of communication in health-related contexts and the support of greater adoption of EHR by patients, this study allows to provide two recommendations. First, the use of EHR is strongly associated with provider recommendation for its use. Health practices could capitalize on this finding by distributing instructions for EHR sign-on and its features in the office and with a personal message from a health provider. Similarly, focused campaigns that could include nursing staff, physicians, and their extenders could result in an increased uptake of EHR. However, these actions could lead to unexpected negative results if health care providers themselves do not hold positive attitudes toward the use of EHR. Receiving information about EHR use from health care providers was found to be the strongest predictor of EHR use. Future studies could assess whether reminders during office visits or targeted education campaigns through posters or brochures distributed in clinics could encourage greater utilization of EHR. Although provider attitudes toward the use of EHR might not predict their own EHR use, 27 consideration and caution should be exercised to account for the possible effect of provider attitudes on patient intentions to adopt and regularly use EHR.
Theoretical and practical implications of this study could be further explored in future research studies. First, as some consumers choose to avoid health information associated with cancer 25 and become overwhelmed by it, 28 future studies could assess whether EHR could be used to tailor the information based on patients’ preferences and be used as a mechanism to build patients’ self-efficacy and skills for information seeking. Second, active and interactive engagement with health information has been linked to more effective information management skills. The active styles of EHR screen sharing have been linked to greater patient engagement, while the passive styles have predictably resulted in lesser engagement. 29 Similar research is necessary to assess the effects of health care provider communication styles on the continuance and frequency of use of EHR by patients. Finally, future research should look at the qualitative properties of EHR use. Specific to the information needs of cancer patients, future studies could evaluate the patterns of use related to the diagnosis and office visits, the utility of sharing educational and health literacy information through EHR, and feasibility of collecting patient-reported outcomes.
Conclusion
The use of EHR can provide patients with access to health information, facilitate health self-management, and improve the quality of preventive health care. While personal beliefs in the importance of EHR use and experience looking for information online predict EHR use, encouragement from health care providers can further facilitate the rate of EHR adoption by health information consumers. Furthermore, EHR could also serve as a channel for the dissemination of health promotion and disease prevention information allowing tailoring of information to account for the needs of cancer patients with different health status. Existing theoretical frameworks, like the CISM, can inform the effective use of EHR as a channel for patient–provider communication that provides reliable and personally relevant health information within a secure environment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.