
Abstract
This study explores the attitudes of elderly people to the use of electronic educational technology (e-learning) on drug utilization, with particular emphasis on the layout, usability, content, and level of knowledge in the tool. e-Learning modules were evaluated by a group of elderly people (aged ⩾65 years, n = 16) via a questionnaire comprising closed and open-ended questions. Both qualitative and quantitative analyses of the responses showed mostly positive reviews. The results indicate that the e-learning modules are a suitable tool for distributing information and education and that they can be managed by elderly individuals who are familiar with computers, allowing them to learn more about medication use.
Introduction
Medication is an important part of health care, contributing to an improved quality of life for many elderly people. In Sweden, most people aged 70–79 years use one or more medicines regularly, while about half of those aged 80–89 years use five or more medicines regularly. 1 The elderly often have complex problems associated with age-related changes in pharmacokinetics and pharmacodynamics, multi-morbidity resulting in increased sensitivity to drugs, and a greater risk of adverse drug reactions. 2 Special attention should therefore be given to the treatment of elderly people with medications. Drug-related problems cause unnecessary suffering in this age group and are associated with high costs to society. 3
The Swedish Council on Health Technology Assessment in Health Care and the Swedish National Board of Health and Welfare have stated that improvements are required in the prescription of medications for the elderly and in the use of medication by the elderly, and that education and information are one factor that could contribute to this.2,3
The proportion of elderly individuals in the Swedish population has increased during recent decades and will continue to increase. 4 Many elderly people in Sweden have access to the Internet at home and use computers. According to Statistics Sweden, 87 percent of Swedish men and women in the age range 65–74 years had home access to the Internet during 2014. 5 Age and education correlate with usage of the Internet; the older old (⩾78 years) use the Internet the least. 6 In the future, however, it is anticipated that older people will use the Internet and computers to a greater extent. 7
In the United States, a national campaign to provide information for the elderly and their caregivers has been introduced. It consists of web-based information, useful links, and slide shows about the use of medications by older adults. The website is titled Medication Use Safety Training (MUST) for Seniors, and the site was developed by the National Council on Patient Information and Education, Maryland, USA. The website encourages individuals to learn more about specific areas that interest them. 8 Alternative outlets for web-based information are electronic educational technology (e-learning) or multimedia education.
Several projects underway in Sweden have the goal of educating elderly people about medical treatment and related areas through e-learning and face-to-face meetings. The project “Awareness about medicines” (Koll på Läkemedel) is a collaboration between two pensioners’ associations (the Swedish Pensioners Association (Svenska pensionärsförbundet seniorerna (SPF)) and the Swedish National Pensioners’ Organisation (Pensionärernas riksorganisation (PRO))) and the Swedish national pharmaceuticals company (Apoteket AB) which allows older people to learn more about appropriate medical treatment. 9 The project “Feeling well with or without medicines” (Må bra—med eller utan läkemedel) focuses on the health and welfare of the elderly and is a collaboration among 10 municipalities in Sweden. This project uses face-to-face group meetings about different themes in the area of health and medication. 10
e-Learning sites about medication use that are designed for and adapted to the specific needs and requirements of the elderly are not very common. However, a study in elderly people (⩾65 years) in Korea showed that self-efficacy and knowledge about the safe use of medication were greater in those who used interactive e-learning techniques plus an information booklet than in those who only received the information booklet or no information at all. 11 Self-efficacy and knowledge about drug interactions were also better in a group with access to e-learning than in a control group without access to e-learning. 12
Many studies involving e-learning and multimedia have included participants of all ages, without being restricted to the elderly. 13 Positive results have been seen in this respect in studies of web-based interventions for patients with diabetes, HIV, or hypertension.14–16 e-Learning about medications seems to be more effective than usual care or no education at all, but further research is needed to increase confidence about the effects of different interventions, including e-learning, for educating patients about prescribed and over-the-counter medications. 13 e-Learning has been found to increase knowledge of heart failure treatment more than traditional teaching alone. 17 More extended studies are required in order to evaluate the retention of the new knowledge over time, although another study in patients with heart failure found that interactive e-learning was superior to traditional face-to-face education with respect to treatment knowledge after both 1 and 6 months. 18
Available education methods about medication for the elderly often entail face-to-face meetings in groups, which can be a problem for the elderly because of mobility problems, illnesses, lack of transportation, and scheduled meetings at times that do not suit. The advantages of web-based education methods are that it is easier to keep them up-to-date than written information and they are cost effective. However, it is acknowledged that some elderly people do not have access to the Internet at home, 5 which would tend to exclude these individuals from participating.
The purpose of this study was to explore the attitudes of elderly people to the e-learning modules in the field of drug utilization, with particular emphasis on layout, usability, relevance, and level of knowledge of the content.
Methods
This study evaluated e-learning modules that had been designed and adapted for use by the elderly. Initially, a prototype was developed, evaluated, and validated by a small test group. A revised version of the prototype was then evaluated by asking a group of elderly people to fill out a questionnaire.
The regional ethical board in Linköping, Sweden, approved the study (no. 2012/351-31).
Intervention and e-learning modules
The topics to be included in the modules were selected in collaboration with pharmacists by screening questions that were frequently asked by elderly patients in hospital wards or when visiting their pharmacy. The following topics were selected: Introduction, Over-the-counter medication and food supplements, Generic substitution, Different medication lists, The Pharmacy Benefit Scheme, Devices to help you administrate your drugs, Adverse drug reactions, Interactions, Questions to ask your doctor, and Frequently asked questions.
During the development of the e-learning modules, a participatory design was used; user representatives have been involved from the start both in the design process and in the evaluation process. The main focus in working with the user representatives was subjective satisfaction, which refers to how pleasant it is to use the system. 19 The choice of tool and design ofthe e-learning modules focused on simplicity and accessibility. It was assumed that the target group of elderly would not have a high level of digital skills and could have impaired hearing or vision. The e-learning modules were designed based on these assumptions, taking into account the size of the text, adequate color contrasts, and the addition of audio. The audiowas added to ease participation for those with problems associated with reading text on the screen. Guidelines from the Swedish Association for the Visually Impaired were used to help design the layout in the e-learning modules. 20
The first version was developed in Power Point (Microsoft, Redmond). This version consisted of slide shows about drugs and drug utilization, with informative text and pictures. In the next version, Slide Rocket (ClearSlide, San Francisco) was used to produce the presentations. WordPress (General Public License) was used to publish the final version of the material on the Internet, with the focus on appearance, web standards, and usability. The website housing the e-learning modules included a short presentation of the research project itself, an introduction on how to use the education tool and some useful links, as well as links to the slide show modules. Figure 1 shows a representative page from the website.
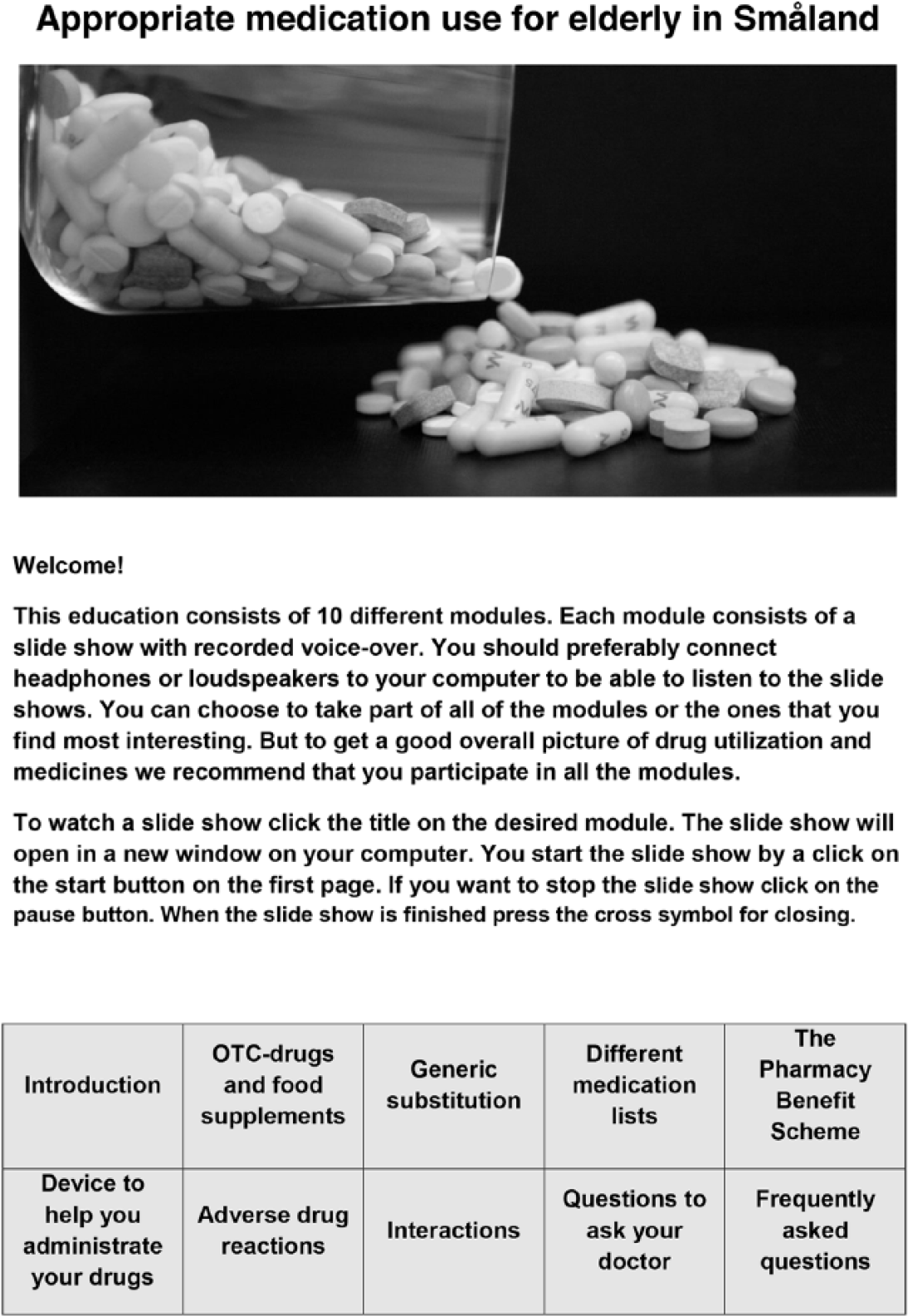
A sample page from the e-learning website.
The use of the Internet allowed flexible learning, that is, participants were able to choose the time and place that suited them, and to repeat the lesson as required. Thus, this tool requires access to a computer and the Internet.
The three County Councils in the southeast of Sweden were contacted to ensure that no interfering interventions were addressed to the target group (elderly people aged ⩾65 years; approximately 760,000 inhabitants).
Initial evaluation
After being published on the Internet, the e-learning modules were evaluated during a test period (February to March 2013) by four people (two men and two women) in the age range of 64–71 years. This test group evaluated the modules with a focus on usability, appearance, and relevance. Thereafter, experts (n = 5) in pharmacy, e-learning, health informatics, web design, and drug informatics also reviewed the content. Representatives from two pensioners’ associations also expressed their opinions on the content of the modules during the test period. The collected opinions were evaluated and included as appropriate in the e-learning modules.
Final evaluation
The revised e-learning modules were evaluated during the period from April to June 2013. Most of the participants (10/16) were using the modules at a center where they had access to computers. The researcher was present during the session and could observe that the participants actually used the modules. The remaining participants (6/16) used the modules on their own without superintendence. After studying the modules, the participants were asked to fill in a questionnaire on the content, layout, and level of knowledge of the modules, and on their computer skills and background data. Informed consent was obtained from the participants.
The participants were asked to fill in the questionnaire within 2 weeks of agreeing to participate in the study. However, illness, journeys, and changes of residency meant that the questionnaires were actually completed between 2 and 5 weeks from the date of inclusion.
Participants
The test group of elderly people was recruited from three sites: a patient association, a pensioners’ association, and a primary care center. A project member contacted the elderly individuals in person and asked them whether they would like to participate in the study. The same approach was used at all three sites. The inclusion criteria were as follows: age ⩾65 years and access to a computer and the Internet. Exclusion criteria were as follows: low vision, impaired hearing, poor understanding of the Swedish language, and cognitive impairment.
The use of an age of ⩾65 years to define the term elderly was based on the general definition of elderly in literature from the Swedish National Board of Health and Welfare. 2
Questionnaire
The questionnaire comprised 23 questions, including open-ended questions and questions on the participant’s background. A six-point Likert-type rating scale with each point labeled was used, where 1 represented “do not agree” and 6 represented “fully agree.” A “no opinion/do not know” option was also available so that the participants did not have to answer any question they were uncomfortable with. 21
During the initial stage, the questionnaire was evaluated with respect to content validity and face validity. 22 The initial test group were instructed to evaluate the appropriateness and relevance of the questions (i.e. content validity), and the appearance of the questionnaire in terms of readability by looking at formatting, layout, and clarity of wording (i.e. face validity). 23 Some small changes were made at this stage to the original version of the questionnaire.
Quantitative analysis
The results of the questionnaires were analyzed using frequency analysis on an ordinal scale. In order to enhance the readability of the results the six-point scale was collapsed to three categories when analyzed: disagree (1–2), neutral (3–4), and agree (5–6).
Qualitative analysis
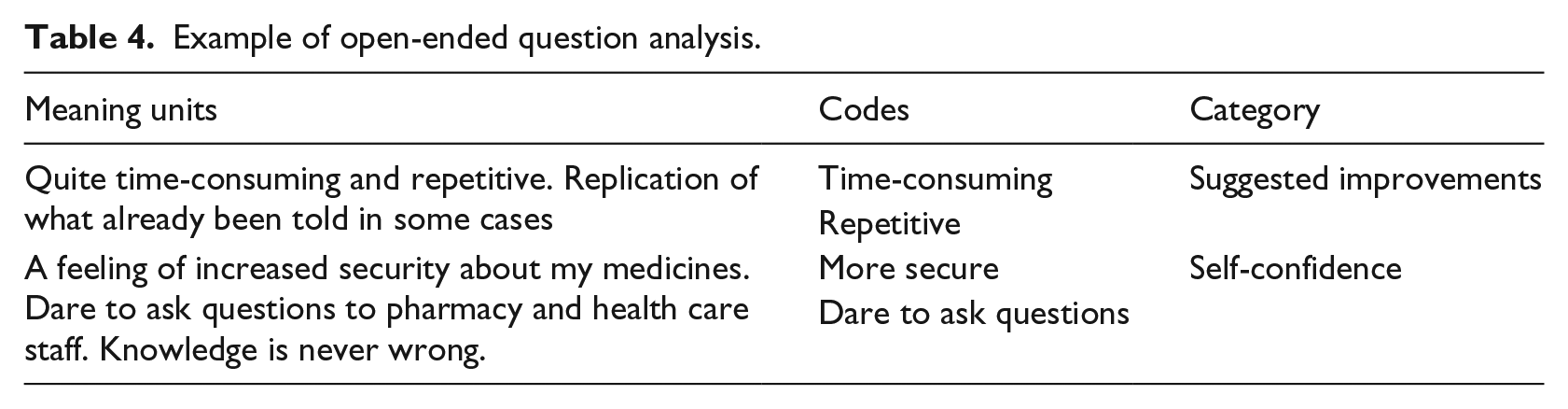
The open-ended questions were analyzed by qualitative content analysis in line with the conceptual framework developed by Krippendorff. 24 The manifest content in the open-ended questions was analyzed with an inductive approach which contained open coding followed by categorization and abstraction. The categories were stated with citations from the participants. 25
The entire text from each participant in response to the open-ended questions was regarded as a meaning unit from which codes and categories were constructed. The definitions of the text units (meaning units, codes, and categories) were defined according to Graneheim and Lundman. 26
After reading the text twice, the first author carried out the initial analysis and constructed meaning units, codes, and categories. Subsequently, the first and second authors read the text and discussed the coding and analysis decisions in analytical sessions to reach consensus. Finally, the fifth author checked the adequacy of the complete analysis.
Results
Study participants
A total of 53 elderly people were invited to participate in the study. Of these, 16 (3 males and 13 females) completed the education modules and the questionnaire, corresponding to a response rate of 30 percent. A participant flow diagram is presented in Figure 2.
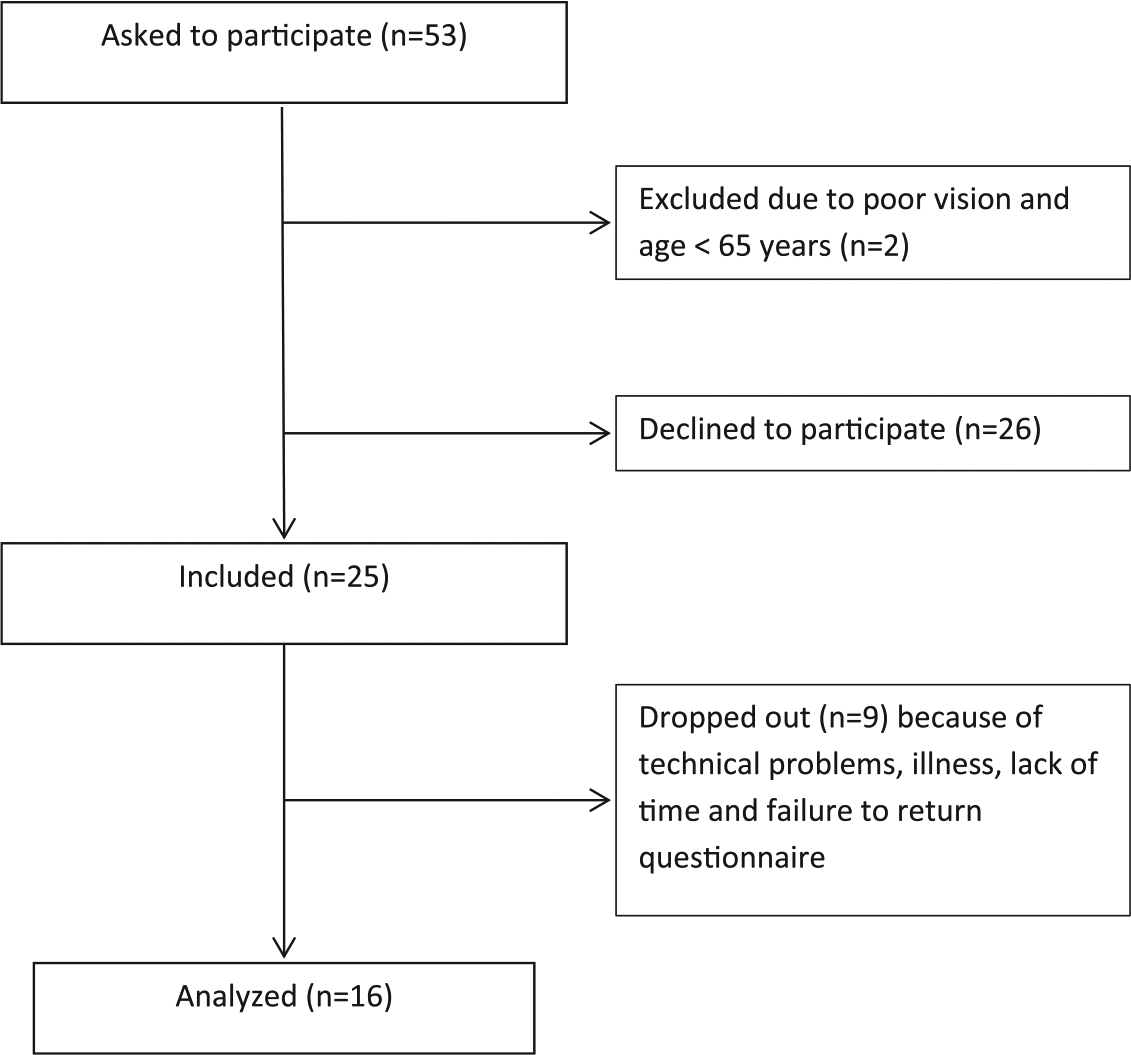
Flow diagram showing the participants in the study.
The age distribution among the respondents was as follows: three aged 66–70 years, five aged 71–75 years, five aged 76–80 years, one aged 81–85 years, and two aged 86–90 years. The mean age among the men was 79 years and among the women was 75 years. The highest levels of education among the respondents were as follows: seven left after primary school, six left after high school, two achieved college degrees, and one attended another education facility. The median level of education was equal between the men and the women. Nine of the 16 participants did their banking on the Internet, while seven did not.
Although they were not required to provide the information, some of the invited 53 elderly reported their reasons for not participating in the study: lack of access to a computer and the Internet, illness, lack of computer experience, lack of time, and no requirement for further information or education about drugs.
Quantitative analysis
Layout
The responses from the completed questionnaires are summarized in Table 1. A majority (81%) of the respondents agreed that the text was easy to read, 75 percent agreed that they could hear the information clearly, and 88 percent agreed that the images were easy to understand. The participants had different points of view in the question concerning the length of the information: half of the respondents disagreed that the education course was too time consuming.
Summary of responses from participants (n = 16) showing the frequency and proportion of agreement (on a six-point Likert-type rating scale) with 12 statements concerning the web-based education tool, where 1–2 represents “disagree,” 3–4 represents “neutral,” and 5–6 represents “agree.”
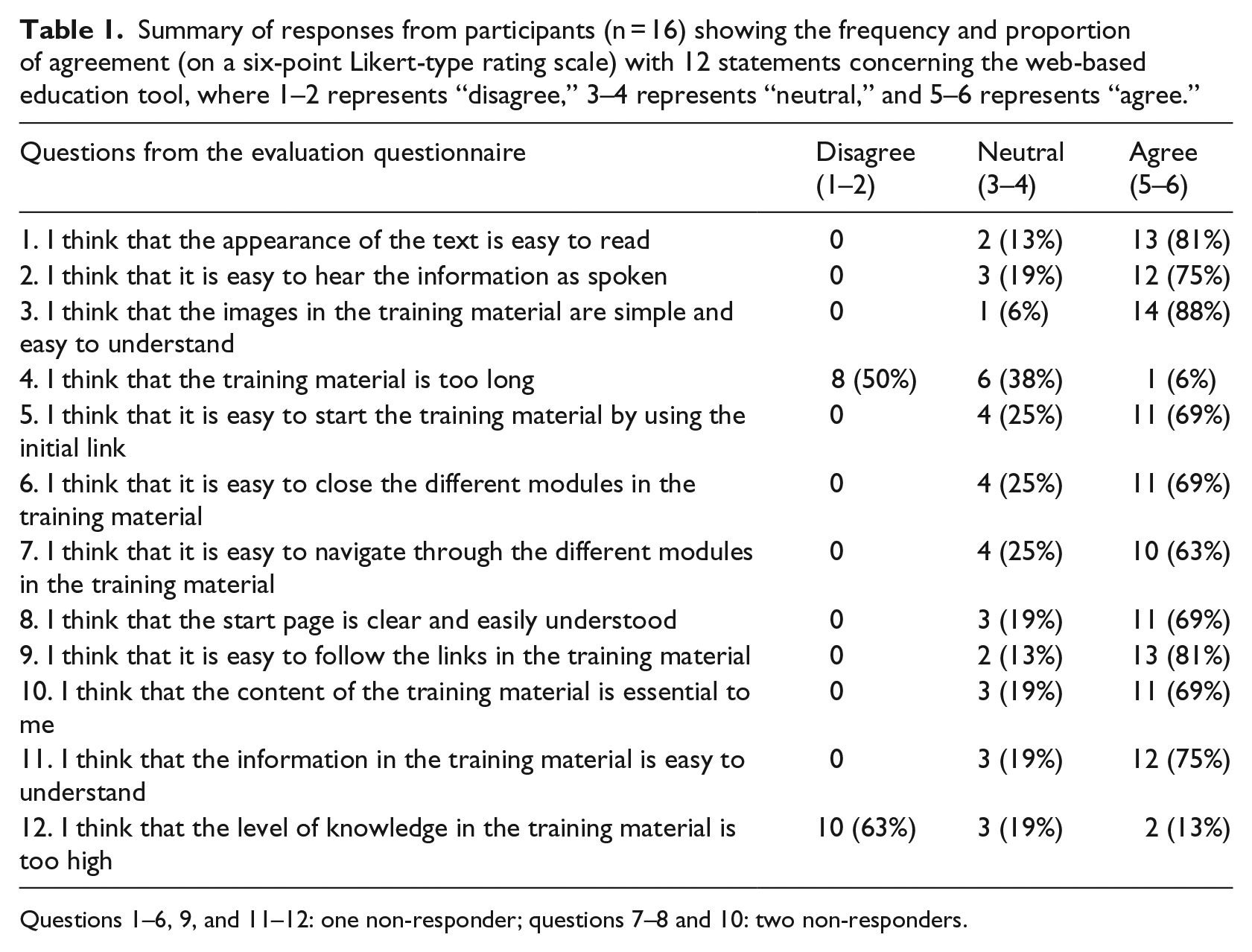
Questions 1–6, 9, and 11–12: one non-responder; questions 7–8 and 10: two non-responders.
Usability
The attitudes concerning the usability of the link to open the education site varied among the participants. A majority (69%) agreed that the link was easy to use, 63 percent agreed that it was easy to navigate through the different modules, 69 percent agreed that the start page was easy to understand, and 81 percent of the respondents agreed that it was easy to follow the links in the education.
Content and level of knowledge
A majority (75%) of the respondents agreed that the information was easy to understand and 69 percent agreed that the training material was essential to them. A majority (63%) disagreed that the level of knowledge was too high. None of the participants answered “no opinion” to any of the questions in the questionnaire.
Analysis by age
To visualize the responses in relation to age, the respondents were divided into two groups based on age Group 1, ⩽75 years (n = 8, range: 66–74 years) and Group 2, >75 years (n = 8, range: 76–89 years). The responses from the questionnaires are summarized in Table 2. There were minor differences in the responses between the two groups. There was a slight tendency that the degree of agreement was lower among Group 2, but due to the low number of participants, this was not statistically tested.
Summary of the responses from the participants (n = 16) is divided into two groups based on age: Group 1 and Group 2.
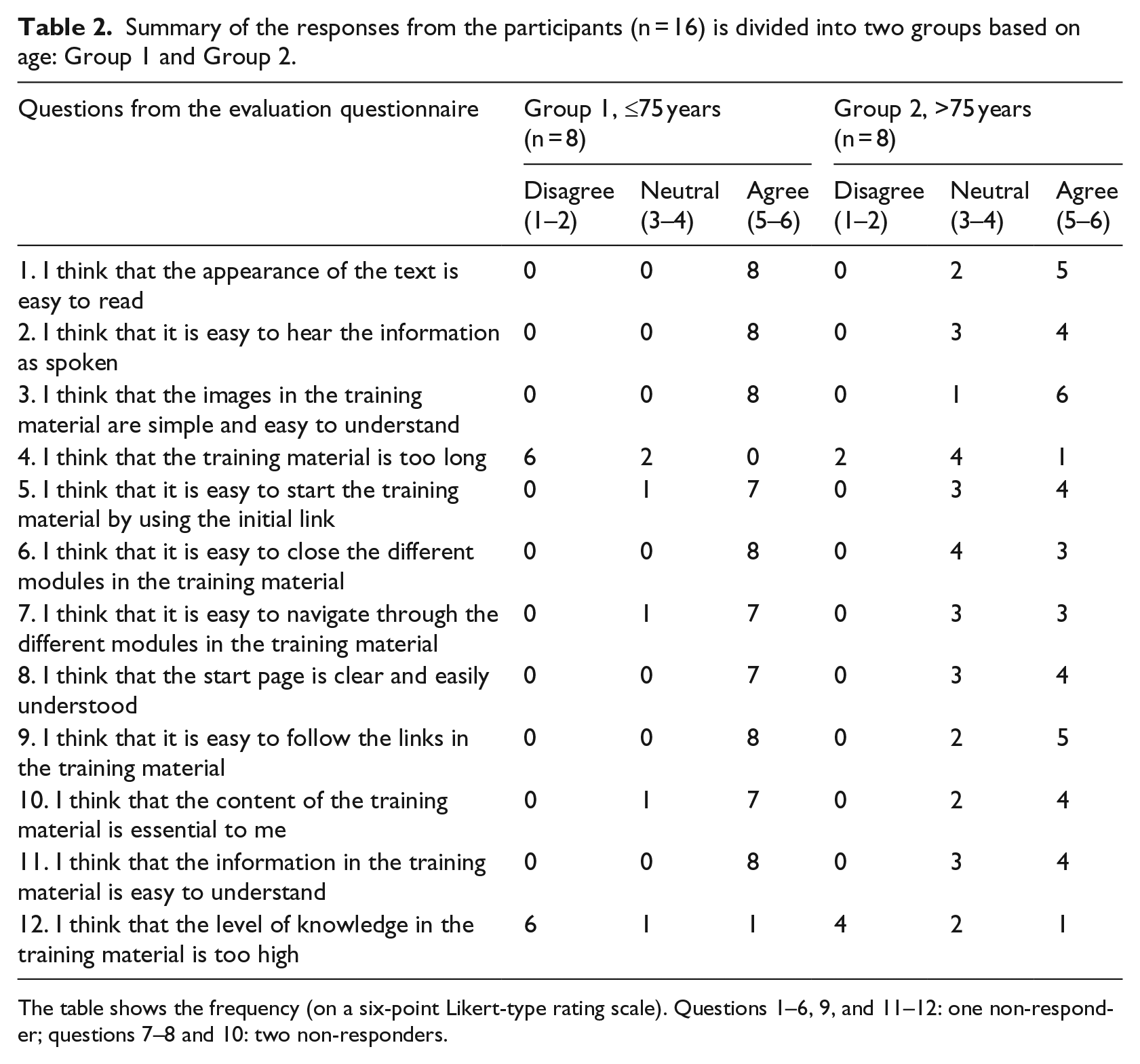
The table shows the frequency (on a six-point Likert-type rating scale). Questions 1–6, 9, and 11–12: one non-responder; questions 7–8 and 10: two non-responders.
Qualitative analysis
Six categories were used to describe the participants’ opinions of the web-based education tool from the questionnaire’s open-ended questions (Table 3): (1) layout and structure, (2) content and relevance, (3) distribution channels, (4) self-confidence, (5) drug-related problems, and (6) suggested improvements. The categories self-confidence and drug-related problems were from the participants’ personal experiences and beliefs, and the other categories were related to technical issues in the e-learning modules. See Table 4 for an analytical overview.
Five open-ended questions in the evaluation questionnaire.
Example of open-ended question analysis.
Layout and structure
The participants regarded the appearance of the website as good. Likewise, they regarded it positive to be able to take in the information at their own pace, and that it was easier to understand than receiving only verbal information.
The participants proposed traditional lectures followed by group discussions as an alternative to the web-based information:
Easier to understand the information on your own than verbal information only. (Participant 8)
Content and relevance
The participants regarded the topics on the site as relevant. The topics most appreciated were according to the open-ended questions the Pharmacy Benefit Scheme (the Swedish Government subsidizes prescription drugs for residents of Sweden), drug interactions, and medication lists. One participant regarded the information as a good way of supplementing, asking questions about medications at the pharmacy or at the doctor’s office. The participants regarded the content of the modules as good or okay:
Everything felt good and relevant. I saved the information to be able to look at it again. (Participant 4) I did not lack anything on the education site. (Participant 21)
Several participants wanted more information regarding specific medicines; in particular, they wanted more details and information on how they interact with other medicines:
I would like more information about specific medicines on the education site. (Participant 4) The education site lacked details about what drugs you can combine or not combine. (Participant 15)
Distribution channels
One participant suggested using a TV commercial as an alternative for distributing some of the information currently on the education site. The lack of access to computers among the elderly was seen as a problem with the web-based education site:
All the telephone numbers that are mentioned on the education site, as well as the information about the Pharmacy Benefit Scheme, would be great as a commercial on TV. Many of the elderly don’t have access to a computer. (Participant 21)
Self-confidence
Some participants reported a feeling of increased security about medication and increased self-confidence when asking questions about drugs and drug treatment:
A feeling of increased security about my medicines. Dare to ask questions to pharmacy and health care staff. (Participant 24)
Drug-related problems
The participants felt that the research about the elderly and medications was good and that knowledge can help to avoid many mistakes and misunderstandings:
The elderly might be a little reserved and not ask questions. Many mistakes and misunderstandings could be corrected with more knowledge. (Participant 24)
Suggested improvements
Some participants regarded the education tool as rather time consuming and repetitive. The opinions varied on the voice options used in the education tool:
Quite time consuming and repetitive. Replication of what we’ve already been told in some cases. (Participant 3)
Discussion
We found that the prototype of the e-learning modules has the potential to be a useful tool for distributing information about medications to the elderly. Overall, the participants found the education process positive; nevertheless, there were comments about deficiencies in the layout, content, and method of distribution. The group varied in their preference for web-based information or traditional information.
In general, a lack of experience with computers could prevent elderly patients from participating in web-based education. Lack of access to a computer was a common problem among the people who were asked to participate and was a reason for not participating in the study for some. However, many of the participants were happy to be able to access information on the Internet at their own pace. These results are in line with earlier research. 27 Other participants preferred to access the information from traditional lectures and group discussions.
Most agreed that the content was essential for them. These results were an indication that the choice of topics was accurate and that these topics should be included in ongoing work on the education modules. Opinions about the length of the information varied among the participants. Because of this, it was difficult to judge whether it was too extensive. It is hard to develop an education unit that is short but also contains detailed, rich information. Different individuals seem to have different requirements, and all education modules cannot be expected to suit everyone.
There were comments concerning the necessity to include detailed information about medicines and drug interactions in the e-learning modules. However, at this stage, it is not feasible to include information about specific medicines because of the wide variety of medicines used by the elderly. In the future, it might be possible to direct the information toward specific target groups of patients with specific diagnoses.
When the participants were divided into two groups based on their age, there were minor differences in the responses between the groups (Table 2). Actually, there was a slight tendency that the degree of agreement was lower among Group 2, but due to the low number of participants, this was not statistically tested. If the number of participants had been larger, a statistical difference might have been proven.
In that case, a plausible explanation to the difference between the groups might be that the participants in Group 1 were more experienced with computers than Group 2.
It is also possible that Group 2 experienced age-related hearing loss and vision impairment to a greater extent than Group 1, which could affect the ability to acquire the information in the e-learning modules. Furthermore, there seemed to be an age-related difference in understanding the information. In the statement concerning whether the information was easy to understand, the younger group had a higher degree of agreement.
It is important that this type of software should be flexible and user-friendly. In this study, the participants were able to select any module according to their own interests, in any order. This was seen as a way of individualizing the e-learning modules for each user. This method of individualization means that the information is suitable for many different target groups.
The elderly participants managed the e-learning modules well, which indicates that this could be a useful tool for informing and educating the elderly. In the future, the proportion of elderly in the population will increase and each individual will probably take more responsibility for their own health. It is important to be able to find and understand accurate health information.
Previous research shows that the oldest people (defined as ⩾78 years of age) use the Internet the least. 6 A study from the United States suggests that older adults need to increase their general computer expertise. It is possible that this will be less of a problem when Internet users currently in their 50s and early 60s become older. The current generation of Internet-connected adults is unlikely to abandon their Internet use and is actually more likely to develop their computer expertise in the future. 7
Before the participants were included, we did not ask them about their current understanding and knowledge of medication use, which probably contributed to the different opinions about the prototype e-learning modules. If we had had that information, it might have been easier to find appropriate module subjects and levels of knowledge to satisfy the participants. It might have been preferable to include more participants, but we found the data to be sufficient based on the purpose which was to evaluate the modules in a pilot test.
The unequal distribution of men and women among the participants was an issue and might have biased the results. However, the mean age was quite similar between the two groups (men and women), as well as the level of education. It would have been preferable to include more men to achieve an even gender distribution. The results cannot be extrapolated to larger groups, in which opinions would presumably vary even more. The participants completed the study in 2–5 weeks. This variation in times for completing the questionnaires is thought not to have affected the results, but this cannot be excluded.
The elderly people who agreed to participate in our study were probably those with an interest in drugs and medical treatment who wanted to learn more. They probably already had good knowledge of the area prior to the education course, which limits the generalizability of the results.
This study used an inductive approach in the content analysis. Inductive content analysis is recommended when there are no previous studies dealing with the phenomenon or when knowledge is fragmented. 25 Trustworthiness is important in content analysis. Intercoder reliability (ICR) is required when more than one researcher is involved in the deductive analysis process. However, it has been suggested that in inductive content analysis, trustworthiness should be checked in the way that one researcher is responsible for the analysis and that other researchers carefully follow-up on the analysis process and categorization. 28 The analysis in this study was performed according to these suggestions. According to S. Elo and H. Kyngäs, authentic citations have been used to increase the trustworthiness of the analysis. 25
Based on our findings, the e-learning modules have been further developed: revision of structure and content, optimization of layout, and revision of the voice recordings. In an ongoing randomized controlled trial (RCT) study with a larger study population, the purpose is to investigate whether the optimized e-learning modules on medication really contribute to increased knowledge, that is, improved performance, perceived knowledge, and self- confidence about medicines, as well as general beliefs about medicines among the elderly. Nothing of this was investigated in the pilot study.
Conclusion
The results indicate that e-learning modules are a suitable tool for distributing information that can be managed by elderly individuals with access to a computer. The benefits of the course reported by the participants included increased knowledge and increased self-confidence about drug utilization, as well as the possibility of absorbing the information at their own pace.
Practice implications
e-Learning modules about medication utilization could be a useful tool for educating and informing elderly patients who are familiar with computers. e-Learning provides a flexible education option for the elderly to use at their own pace.
Footnotes
Acknowledgements
The e-learning modules were developed with the help of Alastair Creelman (expert in e-learning), Pia Gröhn (web designer), and Gun Hjortryd (photographer). All authors contributed to the conception and design of the study, and analysis and interpretation of data. Victoria Throfast drafted the article; Göran Petersson, Lisa Ericson, Lina Hellström, and Bo Hovstadius revised the article. All authors approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Kamprad Family Foundation (grant no. 2013-0065) and Linneaus University. The funders had no involvement in the study.