
Abstract
Bringing virtual environments into cancer support may offer a particular potential to engage patients and increase adherence to treatment. Developing and pilot-testing an online real-time multi-user three-dimensional platform, this study tested the use of an early prototype of the platform among adolescent and young adult cancer patients. Data were collected with an online questionnaire and using ethnographic methods of participant observation. The adolescent and young adult patients tested basic features of the virtual environment and some conducted brief in-world interactions with fellow patients during hospitalization. They had no reservations about using the technology and shared their ideas about its use. Our pilot test pointed to a number of areas of development for virtual environment applications as potential platforms for medical or behavioral interventions in cancer care. Overall, the results demonstrate the need for high user involvement in the development of such interventions and early testing of intervention designs.
Keywords
Introduction
The virtual space, independent of its technological shape, is characterized by the possibility to navigate the borderlands between the actual and the potential. In the context of cancer therapy, this may carry a prospect of new forms of behavioral intervention. New online social technologies are creating novel opportunities for therapeutic and behavioral intervention with a positive impact on patient empowerment, knowledge, self-efficacy and pain control.1–7 Virtually mediated communication has the potential to transform our approach to patient education and interaction with the healthcare sector.8–11 This may offer new ways to approach the psychosocial support of adolescent and young adult (AYA) cancer patients.
Cancer is the leading disease-related cause of death in AYAs. 12 Each year, nearly 70,000 people in the United States between the ages of 15 and 39 are diagnosed with cancer. 12 In Denmark, where this pilot study was conducted, approximately 1500 people (in a population of 5.2 million people) between 15 and 39 years of age are diagnosed with cancer each year. 13 Even though increased survival has been documented among AYA cancer patients,14,15 a number of studies suggest that the survival of AYA patients still seems to be significantly lower than the survival of children with biologically similar cancer diagnoses.14–17 Likewise, the survival of AYA patients is lower than that of adults above 40 years of age.18,19 Several factors are believed to contribute to this disparity, including delay in diagnosis, suboptimal treatment adherence and physiological differences.16,17,20–22
AYA cancer patients are a particularly vulnerable group of patients as they are in transition between dependent childhood and independent young adulthood. 23 They fall in between pediatric and adult treatment protocols and have different social, psychological, biological and physiological needs and challenges than other cancer patients.12,24 Cancer profoundly disrupts the everyday and social life of the AYA patients and the availability of sufficient, appropriate support becomes crucial. However, studies have shown that the social support of AYA cancer patients is challenged by many different factors during treatment.25,26 Keeping up everyday life with regular activities such as school, sports and friends is difficult and in some periods impossible for patients in active treatment, as the very intense treatment protocols require frequent hospitalizations.
Computer games and other interactive, multi-media tools have been shown in previous studies to positively affect and change behavior in patients with chronic illness, increasing treatment adherence and self-efficacy, as well as relieving stressful aspects of the experience of illness.27–32 Social identification of self and other via avatars in virtual environments has been found to affect both virtual and real-life behavior, indicating that the vicarious reinforcement and identification with avatars can motivate behavior change that could have an impact on health.33–35 The avatar is in this study a graphical representation of the patient or user in a three-dimensional (3D) form. The simulation of events and effects found in computer games and virtual technologies make these technologies particularly suitable as educational tools to affect health and treatment behavior, beyond the traditional didactic methods.10,32,36 A virtual environment has the possibility of mediating the difference between the actual circumstances of a patient (e.g. a state of illness or pain) and a potentially new situation, demonstrating to the patient an opportunity to perform actions and engage in social interactions that are not possible within the actual everyday frame.2,4
At the same time, AYAs are very active and skilled users of media, both as consumers and as creators of content, 37 which makes it suitable to develop and assess media-based interventions to this group of patients.
As described, the social challenges facing AYA patients are significant. Finding ways to alleviate social isolation and sustain social interaction with peers in AYA cancer patients during treatments is of critical importance to assist their re-integration into everyday life after treatments. Bringing virtual environments into cancer support may offer a particular potential to engage AYA cancer patients and facilitate such a process.
The goal of this article is to present the results of a pilot study that tested an early prototype of an online virtual environment for psychosocial support of AYA cancer patients, focusing on areas for further development of the environment. The pilot study did not include or evaluate an actual intervention component at this time.
Methods, design and development
Setting
In February and March 2011, 12 young Danish cancer patients were recruited from the Youth Unit (YU) at the Department of Oncology at Aarhus University Hospital to test the feasibility of an early prototype of the online environment. The oncology department is one of five oncology treatment centers in Denmark that undertakes non-surgical cancer treatment and outpatient follow-up. The YU is part of an adult ward and comprises two 2-bedded rooms and a “youth corner” in the sitting room area. A small group of nurses are dedicated to the care of the YU patients. On average, the YU admits 8–10 new patients per year between 15 and 22 years of age. 23
Participants and procedures
Patients were recruited for the study by two of the researchers (M.T.H and P.R.O) following a weekly review through the 8 weeks of the planned patient flow in the YU. All patients eligible for treatment in the YU were also eligible for the study. All participants were in active treatment for their cancer. However, the status of each patient was assessed by the researcher (M.T.H) and clinical nurse specialist (P.R.O) and the YU nursing staff to protect the patients considered too vulnerable for participation. In the course of the 8 weeks, 16 patients were available for recruitment to the study. Four patients did not wish to participate. All participants were informed of the objectives and procedures of the study and their right to terminate participation at any time. All participants provided written informed consent to the study. The study was approved by the Danish Data Protection Agency and the Danish Regional Committee of Southern Denmark on Biomedical Research Ethics (S-20110037).
An appointment was made between the research team and the young patients as they were recruited for the study to introduce them to the virtual environment during the same hospital admission period in which they were recruited. Two participants were recruited and introduced to the virtual environment during an outpatient follow-up visit to the department. All patients received one session with a researcher. In one instance, two patients preferred to attend this researcher session together. The young patients were provided with a personal log-in to the virtual environment during this session and, if necessary, assisted to upgrade their browser software. The young patients were asked to test the basic features of the virtual environment, such as logging in, moving around their avatar and chatting with other patients’ in-world, if others were simultaneously online. Participants accessed the virtual environment using their own laptop or a laptop provided by the research team.
This served as part of a collaborative development process, where the young patients were encouraged to provide feedback on the use of the virtual environment to optimize and target the intervention to their needs and behavior. An interdisciplinary group of programmers, graphic artists and researchers with different social science and health backgrounds collaborated to integrate the responses of the young patients in the further development.
Design and development
This study used a web-based online multi-user 3D environment developed for the project between October 2010 and February 2011. The environment was designed with the low technical requirement of a modern web browser on the patient’s computer. The core idea was removing the friction of having to install a separate client or additional graphics drivers to participate, which traditionally had been a barrier to participation in 3D multi-user environments for non-technical users. The patient’s web browser acted as a client and contacted a single server administered by one of the researchers (E.C.P) to interact with the environment, similar to the design of many multiplayer games but all it would take to enter this environment was the click on a link on a webpage.
Through a standard web interface, patients could log in to their accounts, edit their profile information and enter the virtual environment. Patient profiles included options to customize their appearance through a set of pre-configured avatars. All user data, administrative data and logs were stored in the encrypted, password-protected database. The virtual world server, built upon existing open-source software for creating multi-user 3D virtual environments, 38 simulated the environment and allowed the users to interact.
To run within a web browser, the client software leveraged new browser technologies for graphics and networking. Interactive 3D graphics were enabled by WebGL, a system that provides access to the same graphics hardware used by games. To efficiently send and receive a constant stream of updates about the world, the client used WebSockets to access low-level networking functionality normally accessible only to standalone software. At the time of development, both technologies were still under active development but available in stable versions of the Google Chrome and Mozilla Firefox web browsers.
Theoretical and conceptual approach
Our thinking about developing a virtual environment for AYA patients took theoretical outset in an understanding of the virtual space as a space between the actual and the potential. 39 A space carrying a possibility to mediate the difference between the actual circumstances of a patient (e.g. a state of illness or pain) and a potentially new situation in the virtual environment, where the patient has the opportunity to perform actions that may not be possible within the actual everyday frame (reference 2–4), such as engaging peers in conversation or games. Taking an existential approach to the social interaction in the virtual environment, we drew on the thoughts of Arendt emphasizing the crucial role of being heard and seen by others for ensuring and maintaining “humanness.” 40 While undergoing cancer treatment, the AYA patients lose their ability to take part in social interaction with peers, to some extent depriving them of relationships with and recognition from others. The stories and interactions shared in a virtual environment are seen and heard by others and thereby constitute a common reality. Storytelling in this sense restores the viability of people’s relationship with others. 41 We become visible to others through our stories and position ourselves in the world. By focusing on the potential of the virtual environment in this study to create a sense of presence and social interaction between the AYA patients testing the features, we sought to be able to evaluate the potential of the virtual environment as a way to alleviate the social isolation that is often a consequence of cancer.
Data collection and measures
The endpoint for the study reported here was to evaluate additional technological and clinical areas for development of the virtual environment.
This study employed a combination of ethnographic observation and an online survey. The young patients completed an online questionnaire at enrollment in the study comprising socio-demographic questions as well as questions on diagnosis, medical adherence, use of the Internet and social network and support. No post-test measures were used, as the focus was not intervention outcome but the explorative endpoints described above. The data source for this study was the baseline questionnaire, completed by 10 of 12 participants and the ethnographic observations conducted with all participants.
An ethnographic approach 42 was taken to the interaction with the young patients in the researcher sessions. A researcher (M.T.H.) was present with the patient, observing in the actual physical space the use of and interaction with the virtual environment and taking notes of their immediate reactions to moving around in the virtual environment as well as their suggestions for alterations and improvements. In these sessions, a researcher avatar was further employed to interact with the young patients in-world. The same researcher who did the observation controlled this researcher avatar (Figure 1). The sessions were documented through fieldnotes.43,44

Screen shot of the virtual environment developed for the study. The avatars in this photo represent researchers working on the project in a testing situation.
To test how a small virtual community might be created, we asked the young patients to participate in a professionally facilitated group within the environment to connect with each other and the research team at four specific times, from wherever they might physically be present at the scheduled meeting time. These in-world group sessions were offered in addition to and following the initial researcher session.
Data analysis
Simple, descriptive analyses were conducted on the online questionnaire data, as the population size did not permit more advanced analysis. The ethnographic data were read and organized by categorical indexing 45 to disclose patterns of use and social interaction in the virtual environment.
Results
The young patients tested basic features of the virtual environment and conducted brief in-world interactions with fellow patients during hospitalization. They had no reservations about using the technology, and they shared their ideas about its use during the sessions with the research team.
Participant characteristics
Socio-demographic characteristics
The AYA cancer patients in this study were between 16 and 27 years of age and had been diagnosed with either bone sarcoma or a brain tumor. Two of the 12 participants recruited did not complete the questionnaire. These two however did engage in a session with the research team, testing the virtual environment. Both genders were represented in the group of participants, comprising seven young men and five young women.
The majority (80%) of participants were living with their parents at the time of study. A few indicated that they had temporarily moved back in with their parents during cancer treatments. A third of the participants were enrolled in school. From this group, however, only one was attending classes part-time during treatment, while the rest were on leave from classes. The majority (70%) of participants had full-time or after-school employment, but all were on leave from their jobs at the time of study (Table 1).
Socio-demographic characteristics of 10 AYA cancer patients in the virtual environment pilot study.
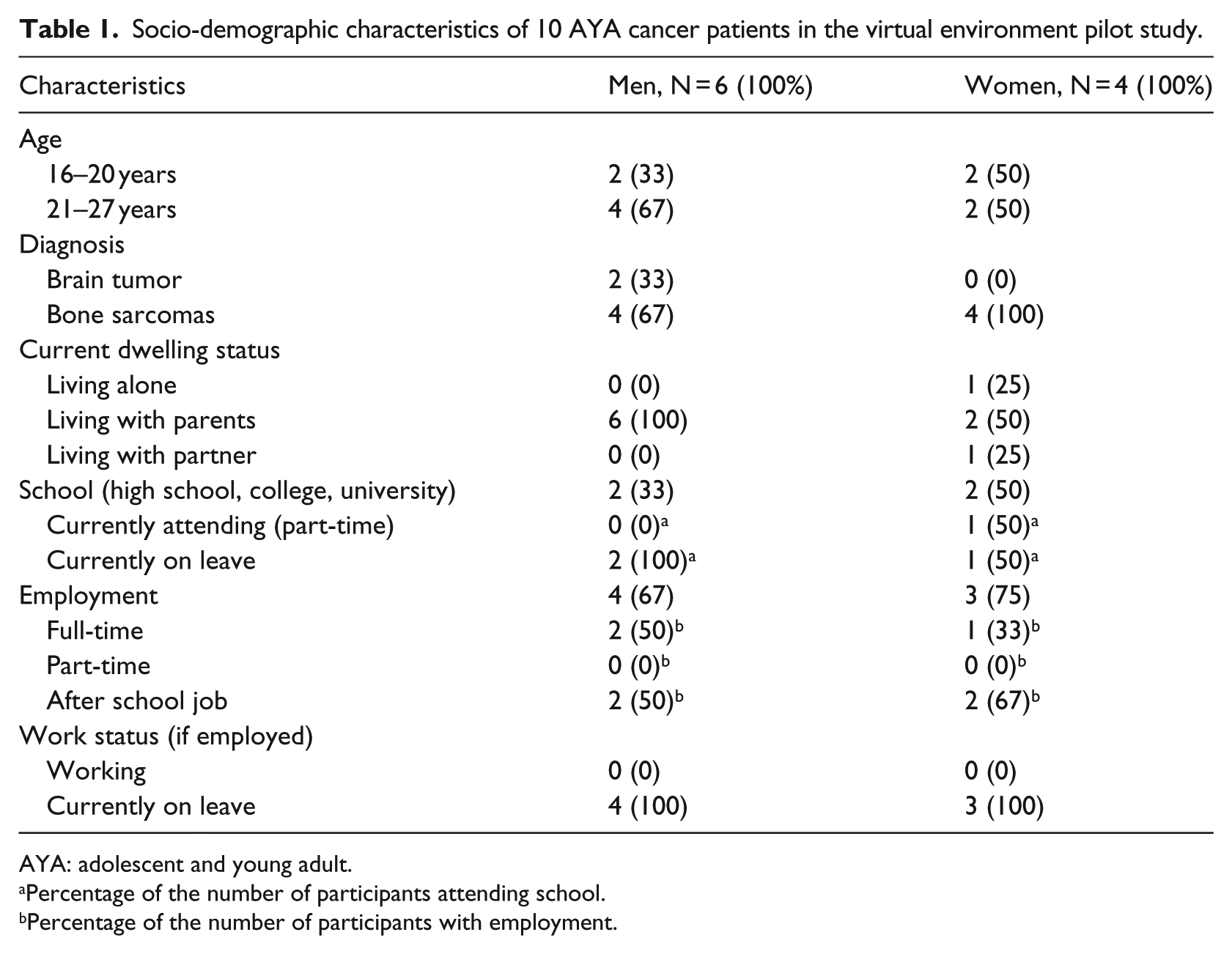
AYA: adolescent and young adult.
Percentage of the number of participants attending school.
Percentage of the number of participants with employment.
Furthermore, the AYA patients reported to have a comprehensive social network of family and friends that they felt able to ask for assistance in matters of practical challenges as well as to talk about their concerns with social and emotional issues of cancer.
Characteristics of Internet usage
All AYA patients reported to use the Internet, and 80 percent used it daily. Their main use of the Internet was to stay in touch with their social network (70%) and communication in online social media networks was the main task performed while online (80%). Furthermore, the main online tasks performed by participants were web browsing for information and writing email. None of the participants, however, participated in Internet discussion groups on cancer (Table 2). During the research sessions, several participants shared that they tried to research the Internet for information on their cancer but often found it very confusing and hard to understand and were generally not sure what to make of it. They had not found Internet sites dedicated to informing about cancer to their age group or with a focus on their special challenges and needs.
Reported Internet use of 10 AYA cancer patients in the virtual environment pilot study.
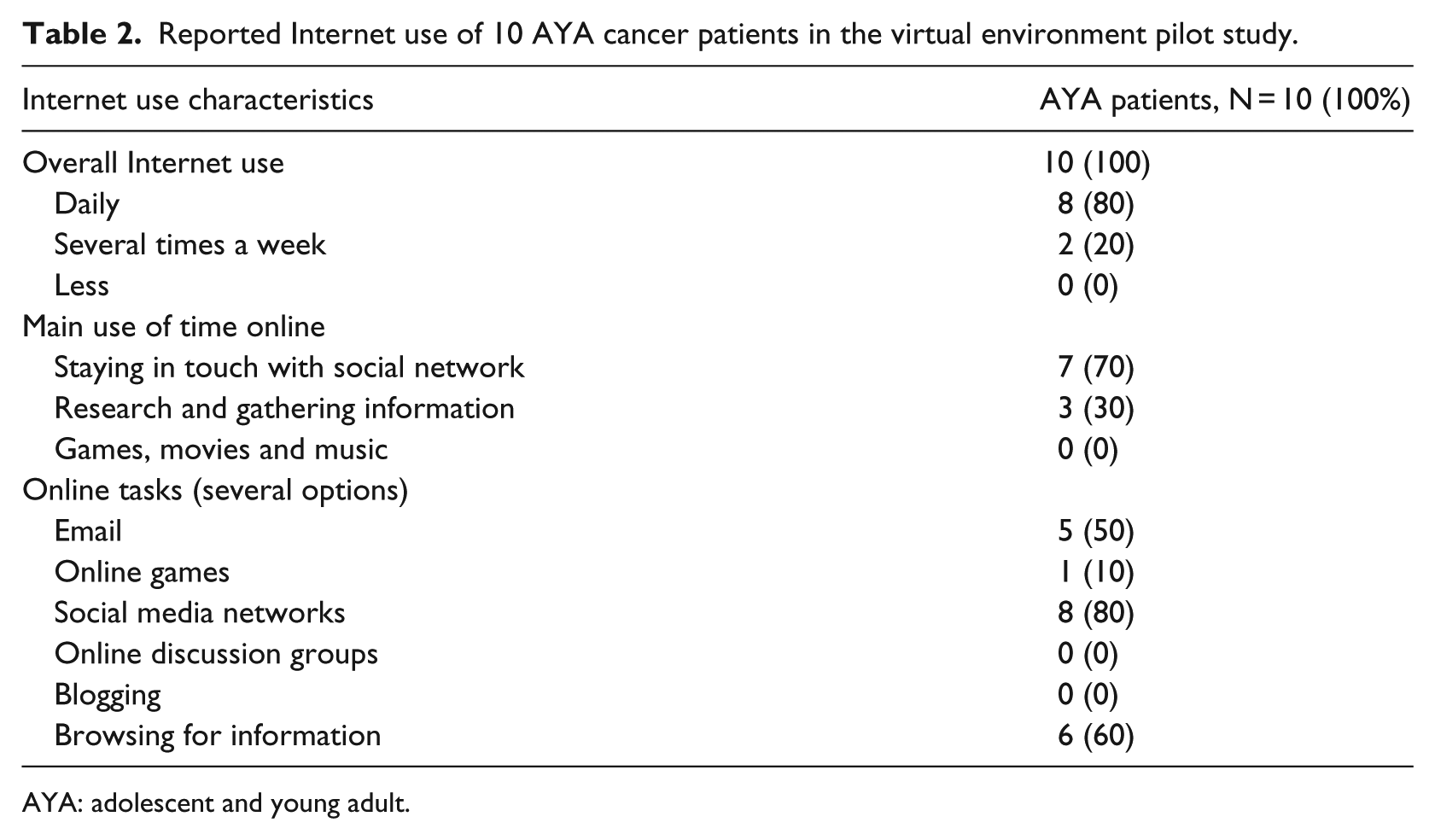
AYA: adolescent and young adult.
Interacting in the virtual environment
Most sessions were carried out with participants and the researcher (M.T.H) all physically located in the youth corner of the hospital ward sitting room. A few sessions were carried out at the bedside of the patient in the YU. No participants had problems understanding how to enter or navigate the virtual environment.
During sessions with the research team, participants engaged with the virtual environment and tested the functions of the avatar and the virtual space. After logging in, they moved around their avatar and interacted with the researcher avatar in-world. On three occasions, AYA participants interacted with each other in-world when more participants were admitted and present at the hospital ward at the same time. Those sessions were more playful and of longer duration than the interactions with the researcher avatar, as the AYA participants on those occasions took more control of the interaction. The few sessions engaging more participants provided a suggestion of the feasibility of the platform as a site for social interaction between AYA patients. The immediate feedback and response of participants were positive. They liked the idea of having access to a virtual space of their own, where they could engage with other AYA cancer patients.
To test the creation of a community in the virtual environment, as described above, the AYA cancer patients were asked to connect with each other and the research team and with a cancer counselor as facilitator within the virtual environment at four specific times from their actual location in or out of hospital. Meeting times were scheduled for late afternoons or evenings, as this would avoid interference with treatment appointments. However, these virtual meet-ups were not successful. Only two participants showed up, but not in the same session. Reflecting on their absence in later follow-up responses to the research team, the AYA patients conveyed that they had not had the energy to participate or it had interfered with other appointments they had had with friends or family.
Adverse effects of the use of the virtual environment
We did not register any adverse reactions to the engagement within the virtual environment.
Future directions for development of the virtual environment
The AYA patients made numerous suggestions to the further development of the virtual environment. The key issues of use that emerged from the interactions were concerned with integration with mobile platforms. Most AYA patients had brought a personal laptop to the hospital; however, the device that was always present with them was their mobile phone. Some participants suggested that accessibility would be higher if the virtual environment offered a mobile integration.
Also, participants suggested that a further development of the avatar animations would make it more engaging to move around. In particular, they would be interested in funny animations that would allow for jumping, hugging and dancing.
Exploring the types of interactions favored by the AYA cancer patients for future developments of the virtual environment, participants suggested mundane interactive games over more advanced educational or informational games. Well-known board games (like backgammon or chess) brought in-world were perceived as possible site-s of action to share and meet around, providing an opportunity to talk while playing, but not demanding continuous talking to share meaningful interactions. A few participants also suggested in-world poster boards for sharing photos, notes or poems.
Discussion
The AYA cancer patients in this study were strongly engaged with online media as part of their everyday activity and embraced the potential of an online virtual environment for social interaction when introduced to the idea and testing the virtual environment. The platform, however, did not integrate with the online spaces where the young patients were already present and interacted, such as Facebook. This may have limited the perceived accessibility. Also, it was accessible only through a web browser and did not support a mobile integration. Our observations revealed that the device constantly present with the young patients were their mobile phones, which suggests that a mobile platform may speak more to their use of technology. A future integration with Internet sites that already channel activity from the AYA patients may help drive more activity to a platform like the virtual environment. With the high demand on time and energy made by cancer treatment on the AYA patients, we found that they required additional motivation to check in on the virtual environment. Feedback from the patients suggests that additional information or entertainment might attract them to visit the environment more consistently.
Communication in the virtual environment was strictly synchronous, meaning that it only facilitated communication between users who were present in the environment at the same time. The suggestions made by AYA patients, to include features in a future development that would allow for posting images or poems, are clearly requests for other asynchronous methods of interaction. Such options would make it easier to build up a community within the virtual environment and achieve the critical mass necessary for a virtual environment to be dynamic, as it sustains an imagination of community without requiring simultaneous presence. The integration of asynchronous interactions could increase the success of future group meetings in-world, for example, by developing long-lived connections to the platform and notification services, where a user is still connected though not actually present and can be notified to log in when something happens. Such reminders and services might drive further participation and ensure co-presence in-world.
A crucial point for future design and successful implementation of virtual environment on browser-based platforms and applications is the support of the various devices and operating systems that different patients use. This is an extremely complicated task and a big barrier to applications like these. However, the limitation to a single device or operating system will limit the accessibility and use, as the request for mobile integration in our AYA population suggests.
Most existing studies of the online use and interaction of cancer patients have focused on the Internet use of adult cancer patients,1,46–50 documenting an extensive use of online cancer support groups in the adult cancer population. Although it is not possible to generalize on the Internet use of the AYA cancer population based on our study, it is interesting to note that no participants in this study reported to use Internet cancer support groups, which may suggest that other types of web-based interventions are more suitable for engaging this group of patients.
The generalizability of this study is limited by the small test population and the specific environment of testing. Also, the AYA patients in this study may have been a selected group of patients with more comprehensive social networks than the general population of AYA patients, if we compare them to reports in the literature.24,51 This may have affected their lack of perceived need for the social interaction offered in the four in-world group sessions. However, the study provides a first step in the development of the virtual environment technologies to target and serve the particular and specific needs of the AYA cancer population. It is to the best of our knowledge the first study to test the use of online 3D virtual environments with AYA patients. In this sense, this study offers a valuable first step in the use and design of virtual environments for personalized therapeutic treatments.
As was documented by Tsangaris et al. 51 in a study of the supportive care needs of AYA cancer patients, the social needs of patients are often not well met. Participants in this study in general reported to have comprehensive social networks and the majority was living with their parents. It may however be difficult for the AYA patients to sustain such a network and its support throughout treatment, as shown by Zebrack et al. 24 Systematic work with network-focused nursing to facilitate the involvement of the social network of AYA patients has been shown in previous studies to strengthen the AYA patient’s sense of self and help them navigate their interactions with family and friends.23,25
Although our pilot study was not successful to drive activity to in-world group sessions, the one-on-one researcher test sessions with AYA patients suggested a potential for further developing and using virtual environments in behavioral interventions with AYA patients. Such interventions could benefit from how the virtual environment makes it possible to simulate certain interactions in cancer treatment. This could increase knowledge and understanding in the individual patient of his or her situation, possibly affecting adherence, as has been documented in game-based interventions. 32 Furthermore, the AYA patients were highly motivated by thinking of social interaction features that would make it possible to just hang out and play together in-world. A supplementary approach to strengthening the social network and support of AYA patients may be a further development of the potential of the virtual environment interactions that may serve as a platform for alleviating social isolation by interacting with peers. The importance of such social integration has previously been documented in text-based Internet interactions.1,52–56 The continuous input from AYA patients to further and future development of such technologies is crucial to ensure they are perceived to be useful in terms of providing spaces for social interaction.
The user-test of the online virtual environment in this study encourages further work with similar types of virtual platforms and interventions as personalized treatment options. This may help to meet the needs of the AYA patients and strengthen their involvement in their care and follow-up. A particular focus point for such development may be to use in-world simulations as personalized intervention strategies to engage patients and increase their adherence to treatment.
It is an important finding of this study that AYA patients are motivated and eager to participate in the testing and development of interventions and technologies, which will serve to increase and ensure that they meet the needs of this particular patient population, as has also been argued in previous e-health development projects. 57 Online virtual environments may offer a particular potential in the future development of comprehensive healthcare programs that address such needs for personalized medicine and care, holding a particular potential for engagement and social interaction.
Conclusion
Our pilot test identified a number of areas of development for virtual environment applications as platforms for medical or behavioral interventions in personalized cancer therapies. Overall, the results demonstrate that engaging the user in the development and early testing helps identify the needs of the intended population, pointing to additional technological areas for development, such as integration with a mobile platform and asynchronous methods of interaction.
Moving toward-s employing such virtual environments in cancer care, issues concerning design, presence and usability are important to consider, as they situate and affect utilization and potential future health outcomes.
Footnotes
Acknowledgements
The virtual environment and the study design were developed in collaboration between Department of Computer Science, Stanford University; Katalabs Inc.; Center on Stress and Health, Department of Psychiatry and Behavioral Sciences, Stanford School of Medicine, Stanford University; and the Pediatric Oncology Research Laboratory, Bonkolab, at the Pediatric Oncology Unit at University Hospital Rigshospitalet, Denmark. The authors wish to acknowledge the valuable input in this process from Professor Kjeld Schmiegelow, University Hospital Rigshospitalet. The authors further wish to acknowledge the unique support and collaboration with Department of Oncology, Aarhus University Hospital, in implementing the pilot test and recruiting patients. The authors wish to thank the young cancer patients who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was generously funded by the Danish Child Cancer Foundation (Grant Number: 2010-12) and the Danish Agency for Science, Technology and Innovation (Grant Number: 10-098405).