
Abstract
Providing patients opportunities for self-management and education about their disease, asthma applications designed for use on an Android operating system can have positive health outcomes across the range of demographics who use mHealth applications. This study provides a content analysis of freely available Google Android Platform Mobile Applications for Asthma. A list of applications was collected on 26 October 2014, using the search feature of the Google Play Android platform and using the words and phrases “Asthma,” “Lung Function” and “Peak Flow.” Each application was coded for its approach to asthma self-management, based on categories adapted by Huckvale et al., which are based on the Global Initiative for Asthma and the National Asthma Education and Prevention Program. The characteristics of the 15 asthma applications are described. Most of the asthma applications’ primary function focused on patient self-monitoring and self-assessment. Using the HON Code, we found low health information quality across all asthma applications. Android asthma applications can have positive outcomes in helping patients as they provide opportunities for self-management and education about their disease. Future research should continue to monitor and evaluate the development and use of mHealth Asthma Applications. Based on these findings, and their indication of a gap in existing research, subsequent studies can continue to evaluate the development and use of mHealth Asthma Applications with increasing methodological consistency to improve the quality of in-app health information.
Background
As of the beginning of 2014, there were over 100,000 mHealth applications available on the Apple and Android platforms. 1 It is estimated that by 2015, there will be 500 million people around the globe using mHealth applications. 2 Fitness applications constitute over 30 percent of the mHealth market followed by medical references at 16.5 percent. Wellness applications represent 15.5 percent of the market and medical condition management represents 6.6 percent of the mHealth market. 1 Medical condition management applications help patients by displaying health parameters, medication intake for specific chronic diseases such as asthma, diabetes, and congestive heart failure. 1
In 2013, a study was conducted on mHealth applications using the World Health Organization (WHO) Global Burden of Disease to categorize mHealth applications. 3 The authors found that most studies for mHealth focused on chronic diseases such as diabetes, asthma, and depression. Although some work has been conducted around these three main chronic diseases, there remains a need for the development of more scholarly work about the quality of mHealth applications and their provided health information. 4 To address the dearth of scholarly analysis and evaluation of mHealth applications, and to examine mHealth practices with one of the aforementioned prevalent chronic diseases, this research will focus specifically on asthma mHealth apps available on Android operating systems.
Asthma is a condition characterized by an airflow obstruction for short periods of time that restrains airflow in the intrapulmonary airways. 5 Reports indicate that over 300 million people globally and of all ages suffer from asthma. 6 The type of asthma has a direct relation to the management, diagnosis, and potential prevention of the disease. A major factor in classifying types of asthma is the presence of underlying airway inflammation, which is variable and has distinct but overlapping patterns reflecting different aspects of the disease, such as intermittent versus persistent or acute versus chronic manifestations. Acute asthma usually arises from bronchospasm and requires and responds to bronchodilator therapy in a few hours, while the chronic inflammatory type usually responds to anti-inflammatory drugs over longer periods of treatment. 7
The principles of asthma pathogenesis are evolving and have been modified over the last three decades as many phenotypes for asthma are being defined and larger insight linkages are being found between clinical presentations of asthma and genetic patterns. 8 It is beyond the scope of our study to predict or correlate future changes in classifying asthma with mHealth apps. It is still important to note that as research deepens our understanding of the disease, it is integral that the management of diseases such as asthma through technology platforms continually must be re-evaluated and updated. This would ensure better patient autonomy and self-care practices in disease management with the assistance of easy to access platforms provided on mHealth apps.
It has also been observed that diseases such as asthma are considered to be a vastly variable. 7 This feature of variability is more commonly referred to as the “Natural History of Asthma.” One such example includes the progressive exacerbation of airway inflammation leading to airway change and remodeling. This may eventually lead to irreversible airway obstruction. 7 The onset, presentation and development of asthma are heavily dependent on the age of the patient. Studies revealed that the course of asthma is vastly different between children of a young age, children of an older age, adolescents, and adults.9,10 This is relevant when considering mHealth applications used in self-management with regard to disclaimers that should make users aware of age-appropriate measures in the apps. Access to care is an added issue, especially in developing countries, where people living with asthma do not have access to medical care and basic asthma medication. 6 Over 80 percent of deaths relating to asthma occur in lower-middle income countries.11–13
The understanding of the pathophysiology and pathogenesis of asthma tells us that airway inflammation in patients fluctuates based on the intensity, cellular/mediator pattern, and response to therapy. Analysis of these determinates helps in making treatment more specific and effective. 7 Advancement in the appreciation and effectiveness of treatment would help application developers around the world include these advancements.
Over the past few years, there have been research studies on asthma mHealth applications. Huckvale et al. 14 conducted a review of applications for asthma self-assessment. The authors identified 103 applications for asthma in English, of which, 47 were for asthma self-management. The authors conclude there are no applications that provide reliable and comprehensive conditions for self-management. Other studies have examined the impacts of mHealth asthma apps. Hyekyun et al. 15 developed a mHealth application for asthma monitoring of adolescents. The authors found that the application can help in the daily symptom monitoring and it was found easy to use by the participants of the study. 15
Another study was conducted by Ryan et al. on the use of mHealth applications for the management of asthma. The authors conducted an observational study using electronic peak flow monitoring and mobile technology over a 9-month period in a UK general practice population. The authors found that 74 percent of the participants determined mobile technology helped improve their symptoms and most were pleased with the technology’s ease of use. The mHealth applications helped patients to monitor and receive instantaneous feedback on their asthma control which would help patients to integrate management into everyday life, engage them more fully in their care and thus potentially improve their asthma control. 16
The National Asthma Council Australia (NACA) released an asthma application which became the most popular asthma management application for Australians in 2013. Over 2 million Australians suffer from asthma, making it one of the highest global prevalence rates. Australian figures, recorded in 2011, indicate that 386 people died from asthma. 17
Research has indicated that when asthma patients follow an action plan and are intimately engaged in their care process this results into fewer asthma attacks, reduced absence from work/school days, and decreased the use of relief medicine. Moreover, self-management plans help in reducing or avoiding emergency trips to healthcare centers and hospitals, leading to an increase in the quality of life for patients, their families and the community in general. 17
Asthma Buddy, the Android application developed by NACA, helps record patient medication plans, provides a what-to-do list in cases of emergency, facilitates communication with your doctor on the progress of your management plan, and records details of all emergency contacts and medical providers relevant to the patient in question. As more mHealth asthma applications are created, there is a need to evaluate their purpose and the quality of the health information they provide. The purpose of this work is to conduct a content analysis of asthma mHealth applications to assess the health information provided and their role in asthma treatment and self-management. In doing so, this article is a contribution in bridging the gap between innovative medical research for asthma management and the accessible platforms of technology used by diverse patient demographics around the world.
Methods
A list of mHealth applications was collected on 26 October 2014, using the search feature on the Google Play Android platform available at https://play.google.com/store/apps. The search was restricted to applications that are compatible with the Android platform. The phrases “Asthma,” “Lung Function” and “Peak Flow” were the search terms used in the query. The initial search identified 175 applications for the word “Asthma.” An additional 10 applications were found for the term “Peak Flow” and another 2 for “Lung Function.” Of the 175 mHealth applications, 165 were excluded for the following reasons: 61 applications were not in the English language (e.g. applications in Chinese, Arabic, Spanish and French), 34 applications were irrelevant to asthma (e.g. an application on coronary heart disease), 22 applications were physician focused and 41 were paid applications. In all, 22 applications made it to the next stage of the review.
After careful evaluation, another seven mHealth applications were excluded because they were not closely related to asthma. This final evaluation included checking whether the application includes at least three of the main eight approaches to asthma self-management, based on categories adapted by Huckvale et al., which are based on the Global Initiative for Asthma (GINA) and the National Asthma Education and Prevention Program (See Table 1). These eight information categories are: the inclusion of basic facts about the nature of the condition, information about the nature of treatment, information about allergens and trigger avoidance, instructions on how to use treatment, information about self-monitoring and assessment, suggestions on an action plan, recognizing and responding to acute exacerbations, and personalizing the definition of good asthma control. The analyzed sample consisted of a total of 15 applications.
Huckvale et al., GINA table.
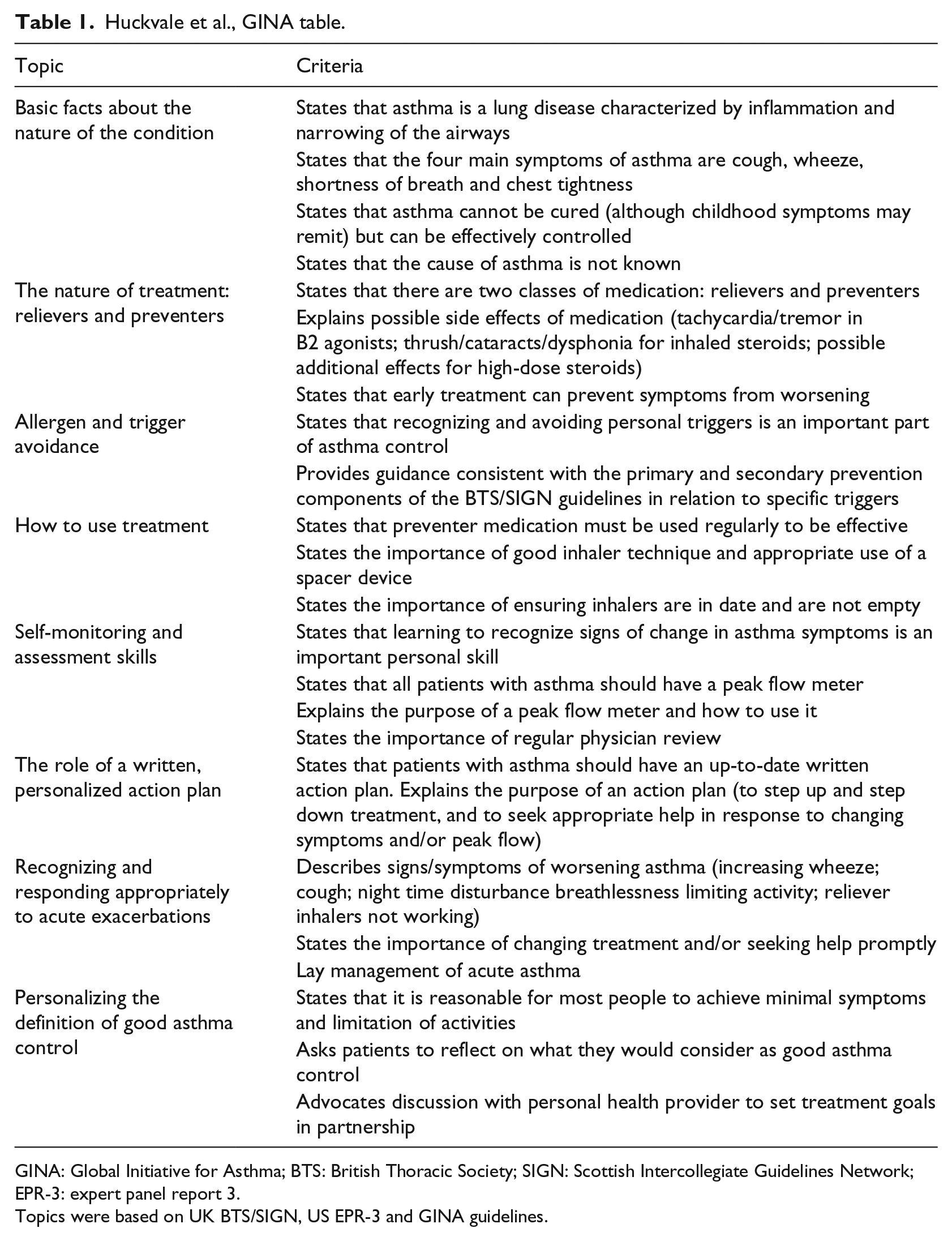
GINA: Global Initiative for Asthma; BTS: British Thoracic Society; SIGN: Scottish Intercollegiate Guidelines Network; EPR-3: expert panel report 3.
Topics were based on UK BTS/SIGN, US EPR-3 and GINA guidelines.
Each application was coded for its approach to asthma self-management, using the eight categories mentioned above. Each Application was coded into one of the following categories: (1) Basic facts about the nature of the condition; (2) The nature of treatment: relievers and preventers; (3) Allergen and trigger avoidance; (4) How to use treatment; (5) Self-monitoring and assessment skills; (6) The role of a written, personalized action plan; (7) Recognizing and responding appropriately to acute exacerbations; or (8) Personalizing the definition of good asthma control. Each application was coded by the researcher and cross-checked with another researcher. There were no disagreements between the coders.6,7,14
Asthma applications were also coded for their level of adherence to the Health On the Net (HON) Foundation principles for health information on the Internet as adapted by Huckvale et al. 14 The authors selected the HON Foundation principles since the Foundation is a leading not-for-profit organization founded under the Ministry of Health, Geneva, Switzerland, and aims at guiding both users and medical professionals to reliable sources of electronic health information. 14 Each asthma app included in the study, was coded into eight possible HON codes (See Table 2): (1) information must be authoritative; (2) purpose of the app; (3) confidentiality; (4) information must be documented, referenced and dated; (5) justification of claims; (6) application contact details; (7) funding and (8) editorial and advertising policy. 14
Health information quality criteria.
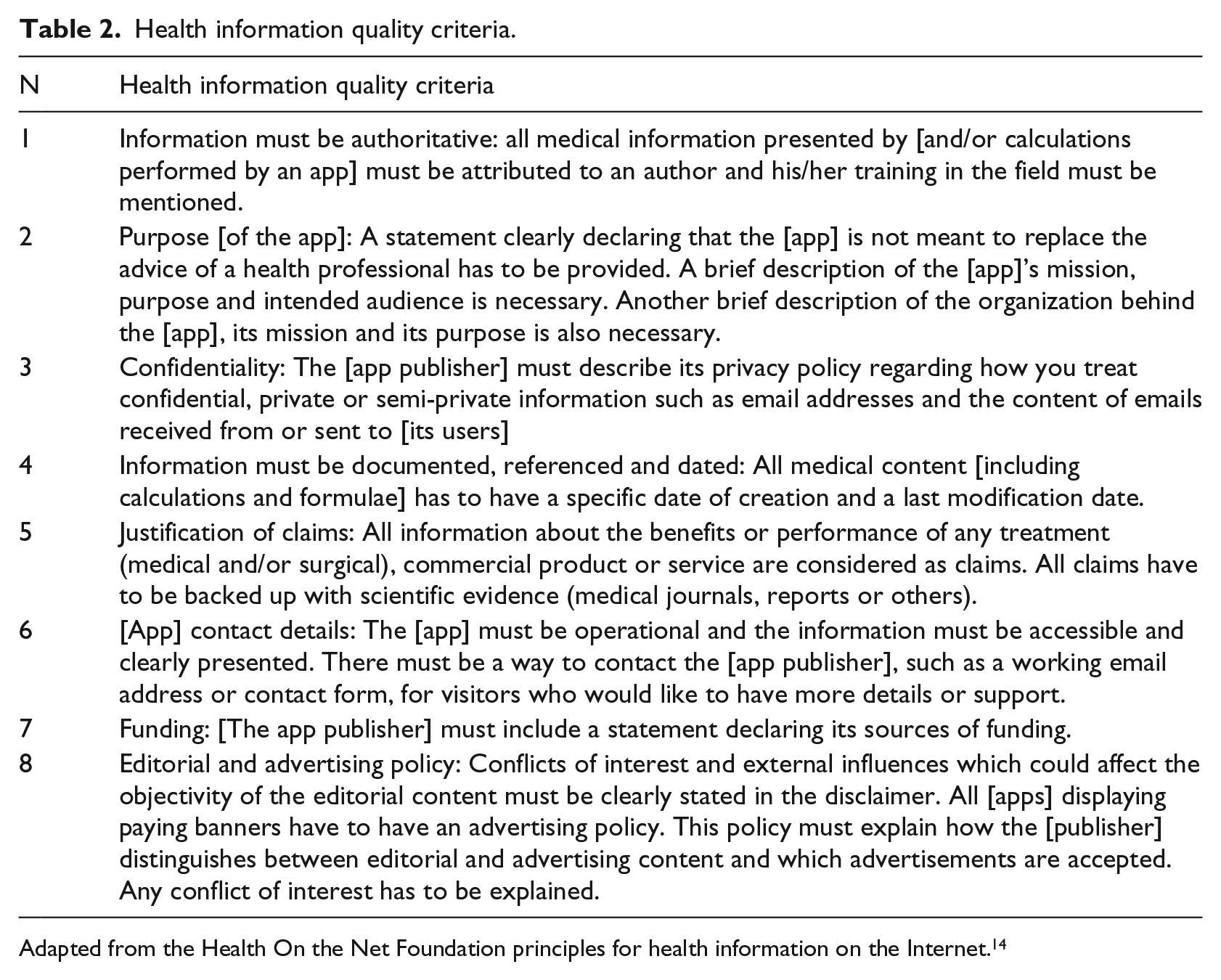
Adapted from the Health On the Net Foundation principles for health information on the Internet. 14
Each application was coded by the researcher and cross-checked with another researcher. Each application received a “0” or “1,” a “0” for not meeting the HON code requirement, and 1 for meeting the HON code requirement. For example, if the purpose of the application was not mentioned the application would receive a “0” code. If the purpose of the application was mentioned, it would receive a “1” code. Each application had to be explicit in mentioning, for example, the purpose of the application. If it was not clear, it would receive a “0.” Any disagreements were resolved between the two coders. The maximum score that each application could receive for meeting the HON code requirements was 8.
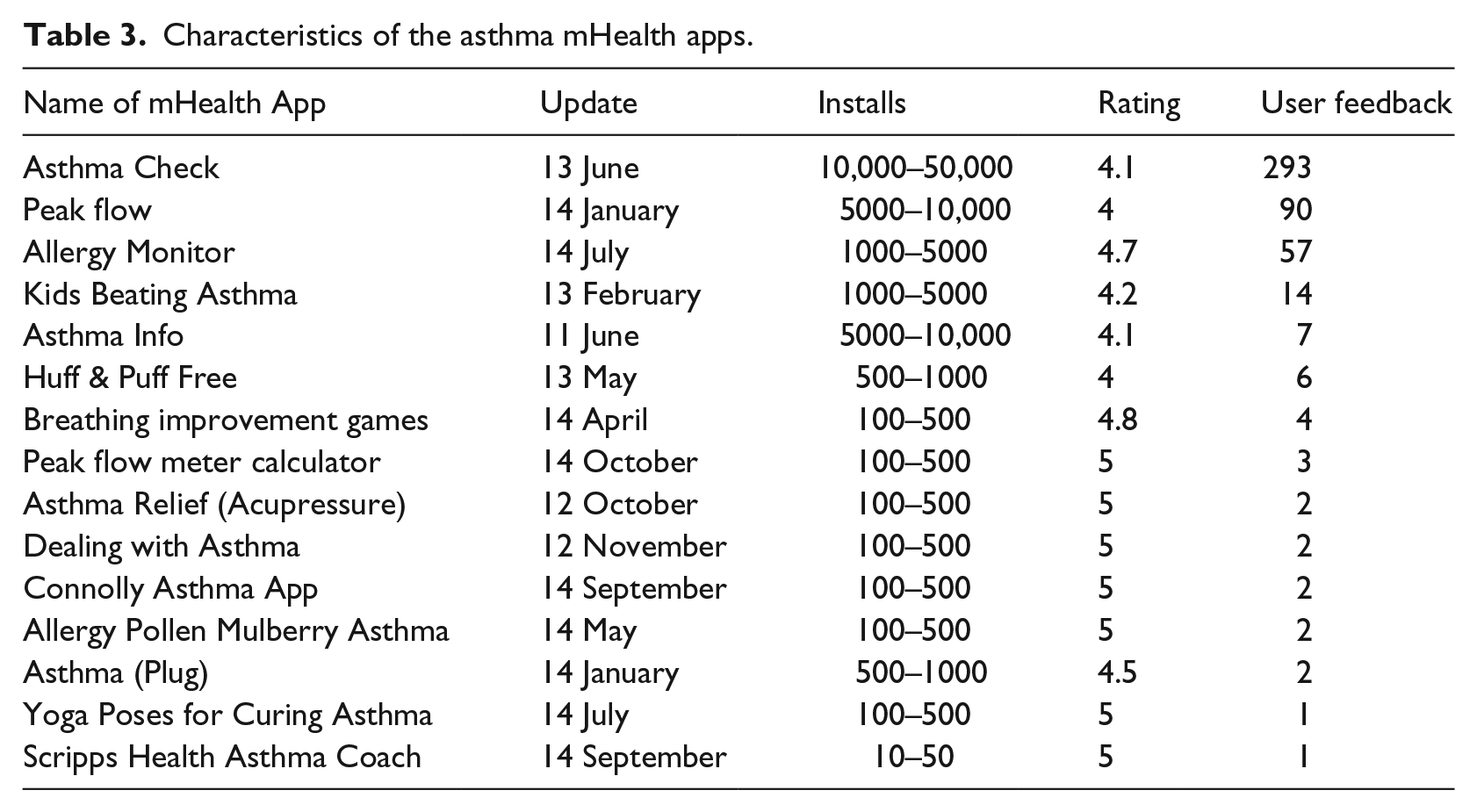
Other metrics were collected for each of the apps. Date of creation, number of times downloaded, rating, and the number of times it was rated by users of the application and their written feedback and reviews about the applications (See Table 3). The information was obtained for each application as of 26 October 2014. The information on each application was updated daily. The measure of number of times downloaded is indicative of the popularity of the application.
Characteristics of the asthma mHealth apps.
Data analysis and results
Descriptive statistics were used to summarize the results of the content analysis. The characteristics of the 15 asthma applications included in the content analysis are presented in Table 3. The dates of when the applications were created ranged between June 2011 and October 2014. One of the asthma applications had between 10,000 and 50,000 downloads. Two of the applications had between 1000 and 5000 downloads and another two applications had between 500 and 1000 downloads. In all, 47 percent (n = 7) of the applications had between 100 and 500 downloads.
The mean user ratings for the asthma applications were 4.6; the median was 4.8; and the mode was 5. The range of 1 and 293 was for the number of user rating responses for each asthma application with a mean of 32 user rating responses per asthma application.
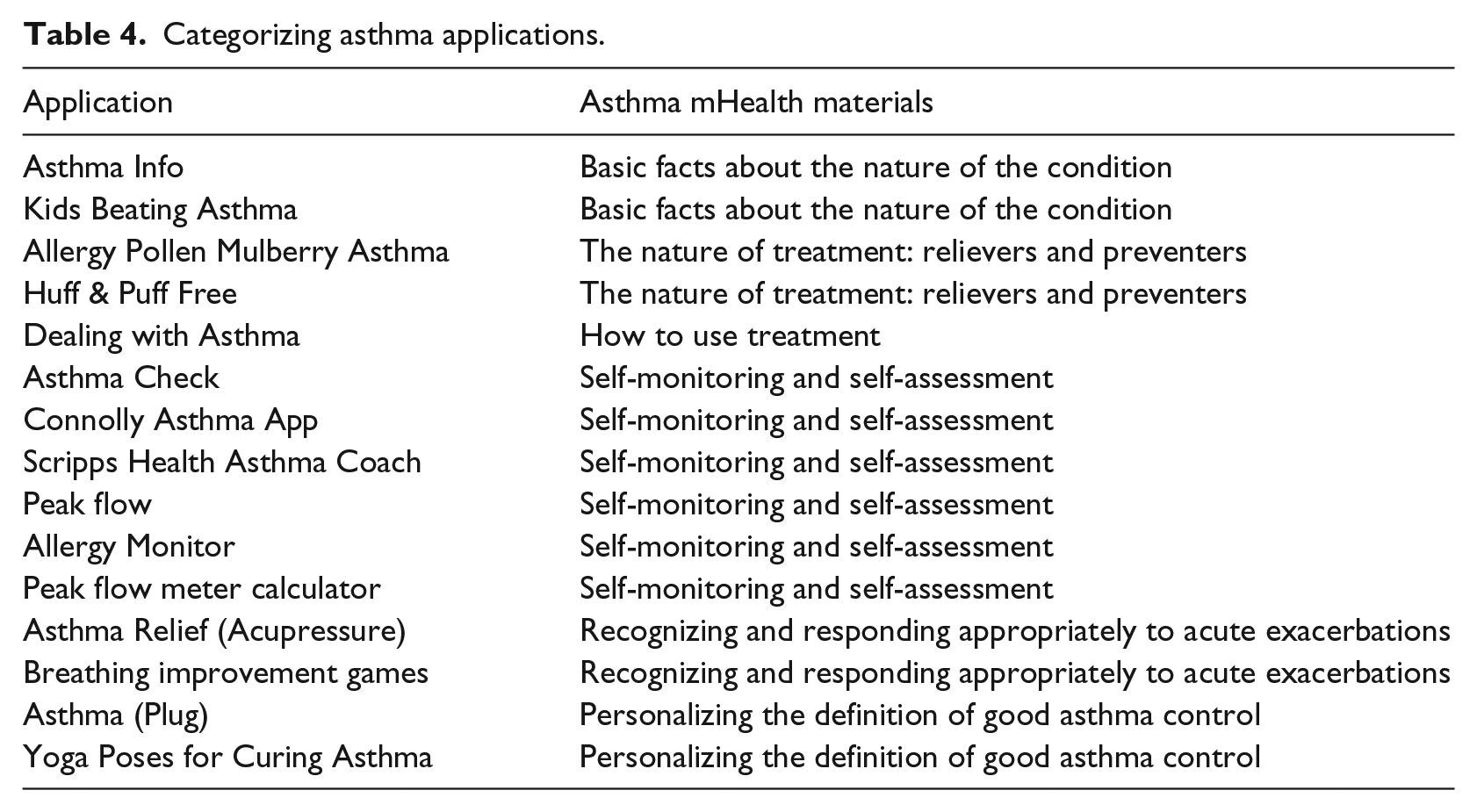
Each of the applications was categorized according to the GINA and the National Asthma Education and Prevention Program (See Table 4). Six of the applications’ primary function focused on “self-monitoring and self-assessment” of asthma patients. Two of the applications focused on providing asthma patients with “basic facts about the nature of the condition”; two of the applications focused on providing patients with “the nature of treatment: relievers and preventers”; two of the applications also focused on “recognizing and responding appropriately to acute exacerbations”; and two of the applications focused on “personalizing the definition of good asthma control.” Only one application focused on “how to use the treatment.”6,7 Detailed functions of examined applications are listed in Table 5.
Categorizing asthma applications.
Asthma applications detailed functions.
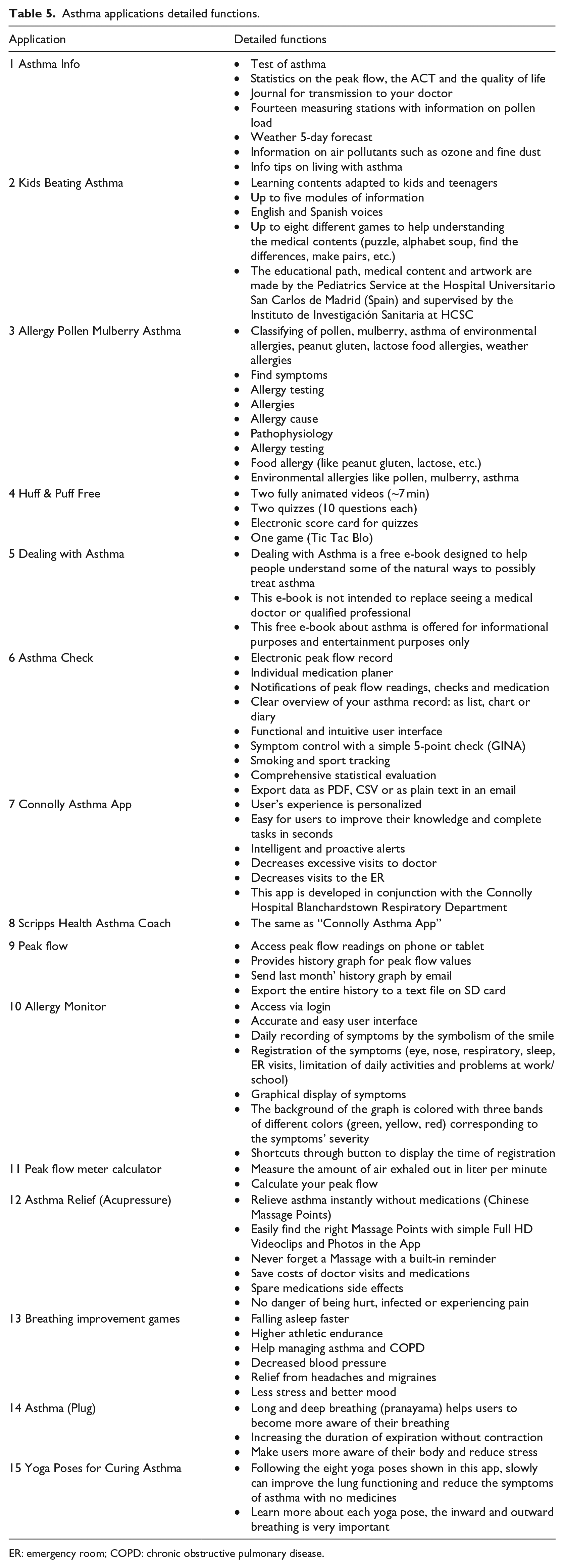
ER: emergency room; COPD: chronic obstructive pulmonary disease.
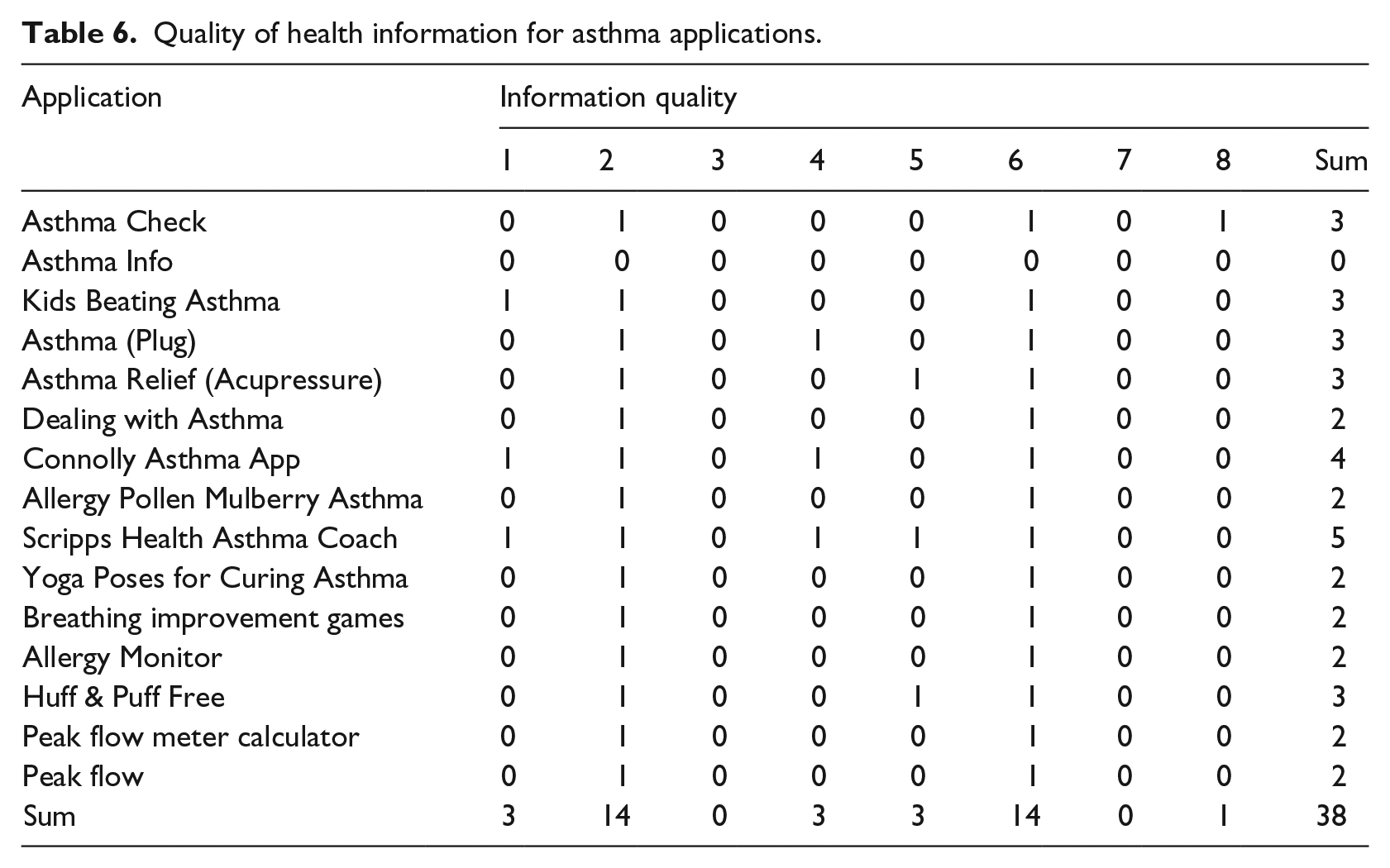
In addition to categorizing the type of asthma mHealth application, the study also measured the quality of health information provided by each application (See Table 6) based upon the HON Foundation principles (mentioned in Table 2). The sum of each of the eight categories coded for health information quality could have a minimum of 0 and a maximum of 8. The range of health information quality for all the asthma applications was between 0 and 5. The mean was 2.5 for information quality across all categories for all of the asthma apps. The median was 2 and the mode was 2. The highest rating was received for each of the applications stating their function and aim. In all, 14 out of the 15 asthma applications indicated the purpose of the application, and 14 of the 15 applications listed contact details. None of the applications clearly indicated how the application was funded. None of the applications discussed confidentiality or any of their privacy policies. Only 3 out of 15 applications attributed their work to an author. Only three of the applications documented and dated the medical information content. Only three of the asthma applications noted that the information presented in the asthma application was based on scientific evidence.
Quality of health information for asthma applications.
Discussion
Free Android applications for asthma have only recently been developed and made available online over the past 3 years. Some of the applications have not been updated for 3 years but are available on the Android market. Applications which are not being updated periodically, such as “Asthma Info,” “Asthma Relief” and “Dealing with Asthma” could be harmful due to outdated information provided in the asthma application. Only one of the apps, Asthma Check, had a high number of installs, while most of the asthma applications had a low install rate of about 100 to 500 downloads. The Asthma Check application also had a high number of user rating responses at 293 in comparison with other asthma applications that had user feedback of 1. These results show that the free Android market applications for asthma are still in their infancy when compared to the number of free applications for diabetes for example; over 1800 applications for diabetes compared to less than 200 for asthma. 3
Most of the free Android applications were determined to be for self-monitoring and self-assessment. Self-monitoring and self-assessment have positive outcomes for asthmatic patients and tools for self-management and self-assessment help in educating patients. 18 This may explain the higher number of self-monitoring and self-assessment applications for asthma patients. Of the sample, only one application was focused on how to use treatment, which indicates that there is little interest in applications that focus on teaching treatment methods.
The strength of this study is in the focus of systematically studying the content and types of free Android applications available to help asthma patients. Where there is a proliferation in the number of mHealth applications on the market, there is a need to systematically evaluate the content of such applications. Recent work is being developed to guide developers of mHealth applications to produce safer applications for the public. 19
Overall, the quality of health information for the asthma applications was low. Of the sampled applications, none provided indication of about protecting the confidentiality of the patients, no applications noted funding sources in detail, and only one of the applications attributed information to an author with noted credentials in the field. These findings are consistent with those of Huckvale et al. 14 These omissions present serious shortcomings of the free asthma mHealth applications. Therefore, more work is needed in the development of mHealth asthma applications that use high-quality evidence. It might be useful and maybe necessary that academic and professional healthcare bodies supervise or authorize the release of medical applications; this should also be supported by more strict regulations and legislations that govern the release of such applications to public.
There are several limitations presented in the research study. First, the content analysis included free mHealth asthma applications and not paid ones. The paid applications may mention funding sources, provide more evidence of the work and provide overall better quality. However, paid applications were not included in the review. It is also possible that new applications were created subsequent to the completion of the data collection process of this study. There may have been are other applications that were missed by not including other search terms. Furthermore, there was no clear evidence to the exact number of downloads for each asthma application; there was only an approximate range for each application. In addition, the user ratings for the asthma applications had to be at least four to be included in the review. It is not possible to know the source of rating such applications, which may bias the results relating to the inclusion of the application. Finally, only Android applications were included in the review, while other platforms such as Apple or BlackBerry were excluded.
Implications for practice
With their recent rapid development, mobile and electronic health have become beneficial tools that have not only reduced the financial costs, but have eased modes of screening and treatment. Applications for Android asthma can complement the existing systems of screening by engaging large numbers of diverse groups of users at one point in time. They can be used for educating patients about preventive and treatment remedies which can reduce the burden on hospitals and doctors. Android asthma applications do not only encourage the patients to remain particular about their health, they also keep patients updated about day-to-day advancement in the management of asthma. The main contribution to the literature is analyzing the content of one type of medical smartphone application, showing the existing gap between the medical research and available evidence gathered from a sample of currently available mHealth asthma applications. With these findings as a starting point, the benefit of the Health on the Net Foundation and the Global Initiative for Asthma’s principles are demonstrated to be a functional framework for evaluating specific aspects of mHealth applications. Further research can define the specifics of best practices in collaborative projects with application developers, medical professionals, and standardization organizations.
Conclusion
Android asthma applications show a promising future in helping patients suffering from asthma. The asthma applications provide an opportunity to reach a large number of asthma patients, which aids in educating them about their disease and in preventing possible hospitalization. Although there is potential for mHealth Asthma Apps in impacting the health of asthma patients, comprehensive work is needed to develop more evidence-based asthma applications that respect the privacy and confidentiality of patients. mHealth applications and research will continue to develop as described by a number of authors;20–23 however, this initial study recommends the quality of the content accords with to the International HON Code Standards.
Footnotes
Author’s Note
Mohamed Khalifa is now affiliated to Centre for Health Informatics, Australian Institute of Health Innovation, Macquarie University, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.