
Abstract
Asthma continues to be the leading chronic condition among US adolescents. Despite medical advances, many adolescents face uncontrolled asthma mainly due to insufficient self-management skills. Mobile apps pose a promising adjunct to in-clinic asthma care. However, little is known about the usability and effectiveness of such technology. In all, 20 adolescents participated in a 3-month trial to test an asthma app tailored to their age. Qualitative data on adolescents’ experience with the app were inquired. Overall, participants thought the app was functional and user-friendly. The majority expressed that the app assisted them with asthma self-management through tracking of asthma status and text reminders to test their peak flow regularly. They indicated external factors that limited app use and suggested improvements to make the app more engaging and appealing to adolescents. The tested app provides a feasible means to assist adolescent in developing self-management skills, tracking disease status, and communicating with healthcare providers.
Introduction
Self-management skills improve the asthma patient’s overall quality of life and are important in achieving controlled asthma, reduced exacerbations, fewer missed days at school, and reduced hospitalization.1,2 Research has shown that most cases of uncontrolled asthma stem from a poor adherence to the recommended treatment. 3 Coping with a chronic condition, such as asthma, can result in life-altering adjustments. For adolescents with asthma, the physical limitation and the treatment regimen may cause interruption with their daily routines such as sports activities and social interactions. These demands in behavioral adaptation along with adolescents’ eagerness for independence often lead to minimal compliance with the recommended treatment regimen. 4 Thus, effective patient education becomes crucial in the development of self-management skills. 5 Patient education tailored to the individual’s need and lifestyle, which incorporates personal goal-setting and positive feedback, was noted to improve patients’ compliance to treatment, specifically among adolescent patients.4–7 Furthermore, Robinson et al. 8 identified patient–clinician communication and support for self-management as key elements in patient-centered care that improves adherence to treatment. They further emphasized the significance of health education in self-management, specifically for patients coping with chronic conditions. According to the authors, effective education components include patient–provider interaction, non-face-to-face communication, and a care management plan.
The limited success achieved through traditional asthma education strategies, along with limited clinic-time devoted to addressing those strategies,3,9 suggests the need for innovative approaches to deliver asthma education for adolescents. As suggested by adolescents and healthcare providers, one viable solution that could meet the recommended patient-centered care elements stated above is the use of mobile technology.9,10 The use of mobile technologies is on the rise, particularly among adolescents. According to 2015 Pew Internet research, 73 percent of adolescents own smartphones and 58 percent own tablet devices; 11 these escalating rates make mobile devices a native and accessible medium in which adolescents are receptive to a variety of messages. Serving a major role in adolescents’ lifestyle, mobile technologies were identified as a convenient platform for adolescents to communicate with their healthcare providers, gain self-management skills, and track their treatment regimen and disease patterns.8,9 The use of mobile devices for the purpose of healthcare promotion is now known as mHealth. 12 Such technologies include text messaging, wearable devices, and mobile apps—the most common smartphone features used in mHealth. Recognizing the potential of mHealth in disease management, the number of health-related apps has been increasing steadily. In 2012, Malvey and Slovensky 13 reported the existence of approximately 40,000 health-related apps. More specifically for asthma, the number of asthma apps available through commercial app stores has doubled in the past decade. 14 In their current version, most asthma apps provide disease information and self-management tools such as diaries, recording of symptoms, and medication intake; some provide reports of pollen count and other environmental factors. 3 A small number of apps offer an electronic asthma action plan (AAP), one of which is interactive. 3 Although providing useful tools for asthma management, the majority of apps do not meet evidence-based recommendations for content or self-management strategies. Despite the potential inherent in mHealth, most apps do not address gaps identified in traditional disease care education that would ultimately facilitate better self-management practices (e.g. the use of AAP, positive feedback, and patient-provider communication). 3
Guided by the patient-centered approach, our interdisciplinary team gathered input from adolescents with asthma and their healthcare providers on an optimal asthma management app.9,10,15 Using these insights, we then developed an app prototype responsive to users’ preferences and informed by asthma treatment guidelines from the National Institute of Health’s (NIH) National Asthma Education and Prevention Program (NAEPP) Expert Panel Review (EPR). 1 Figure 1 depicts the features and functions of the developed app, which enable users to track disease patterns, symptoms, triggers, and peak-flow readings and then receive AAP feedback on their current asthma status. This study aimed to test the developed adolescent-friendly asthma management app; specifically, the purpose was to explore participants experience using the app and obtain feedback on how to facilitate its use. In addition, the study explored how app use influenced participants’ asthma self-management practices.
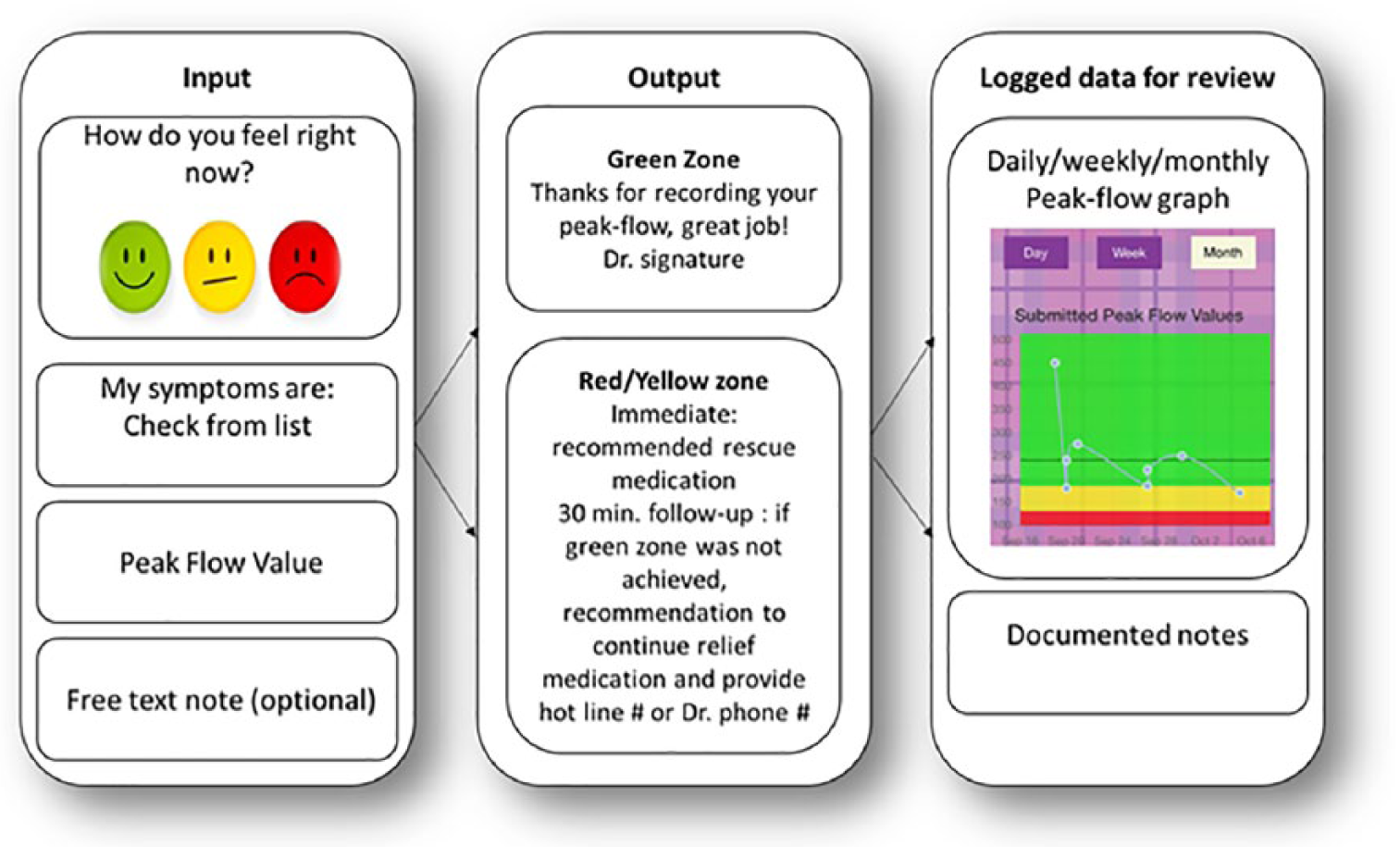
App features and functions.
Methods
Participants
A purposive sample of 20 adolescents with asthma was recruited through three university-based inner city pediatric clinics in the Tampa Bay area, Florida, United States. Clinic staff introduced the study to eligible adolescents during their scheduled doctor’s visit to the clinic. Eligibility criteria included being in the target group of adolescents (aged 12–17 years) and having English proficiency to enable reading of the app prototype. Participants had to be diagnosed with mild, moderate, or severe persistent asthma without a co-morbid chronic cardiopulmonary disease, removing confounding factors for determining the app’s impact on the adolescent’s asthma. In addition, participants were required to have access to a mobile device with the appropriate capacity to use the tested app and were given a peak-flow meter and trained on its use. Before entering the study, adolescents and their caregivers were informed of the study details, and both signed an informed assent or consent form. Demographic information was gathered during enrollment and is presented in Table 1. The study was approved by the University of South Florida Institutional Review Board (IRB# Pro00021447).
Participant characteristics.
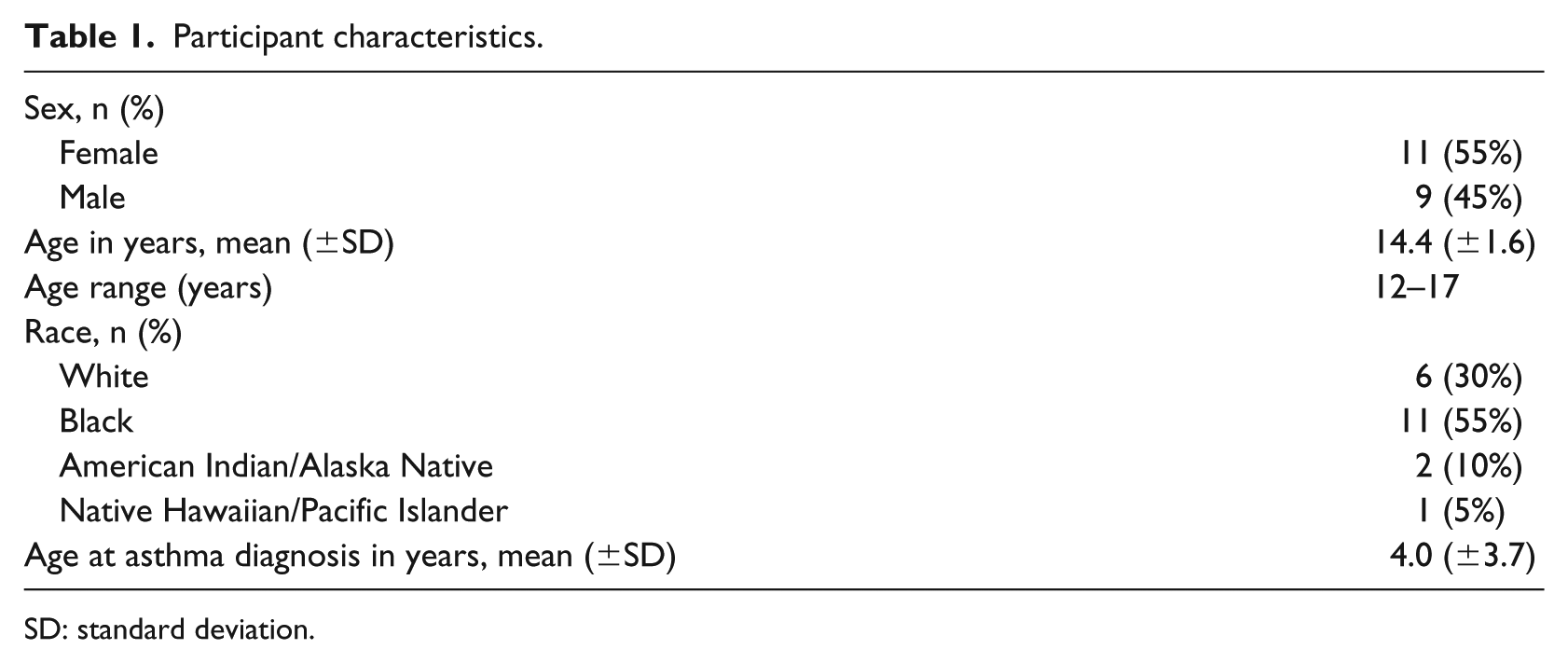
SD: standard deviation.
Procedure and methods
In this qualitative, exploratory study, the asthma self-management mobile app was tested for a trial period of 3 months. During this time, participants received two daily reminders that invited them to enter asthma symptoms and peak-flow values. The app would then determine NIH NAEPP EPR 3 asthma status of the participants based on their individual peak-flow goal and reported symptoms. Asthma status was color-coded to green (indicates 80%–100% of the individual’s goal peak-flow value), yellow (indicates 50%–80% of the individual’s goal peak-flow value), and red (indicates less than 50% of the individual’s goal peak-flow value) zones. 1 For each zone, the participant received a recommended action that followed their personal AAP treatment plan. Although participants were prompted to use the app twice daily, they could adjust the reminder to their preferences and use the app as frequently as desired.
In all, 20 adolescents participated in the study; of which, 11 were females and 9 males; 30 percent were White and 55 percent were Black, which reflects the clinic population. Semi-structured interviews were conducted with each participant at mid-point (via phone) and the completion of the trial period (in-person) by trained study investigators. During the 3-month trail, one participant was lost to follow-up and two more were not available for the mid-point interview; therefore, a total of 37 interview sessions were conducted. Interviews intended to capture participants’ experiences related to usability of the app and its influence on their self-management practices. Interview questions solicited input on the app in general and specifically on each app feature. Each interview lasted 30–40 min; participants received a stipend of US$20 after the final interview and US$10 after the midterm interview.
Data analysis
To capture participants’ perceptions, thematic analysis was employed in two phases. First, two of four analysts listened to each interview recording; interviews were summarized in a matrix to capture the main elements. Quotes that clearly highlighted the identified elements were transcribed and added to the matrix to support the findings. In this phase, a priori codes were guided by the interview questions. Second, analysts combined midterm and endpoint interviews matrices for each participant to detect any changes in perception throughout the trial period. They then conducted a second phase of coding using ATLAS.ti© (version 7). For this phase, a codebook was created including codes’ names, definitions, and examples. Applying the constant comparative method, 16 analysts discussed emerging themes and addressed any inconsistencies in the coding throughout the process; additional codes emerged while others were refined or eliminated. To better tailor the app to certain subgroups, design questions were examined across gender (male/female) and age groups (early adolescence (12–14 years) and middle adolescence (15–17 years)).
Results
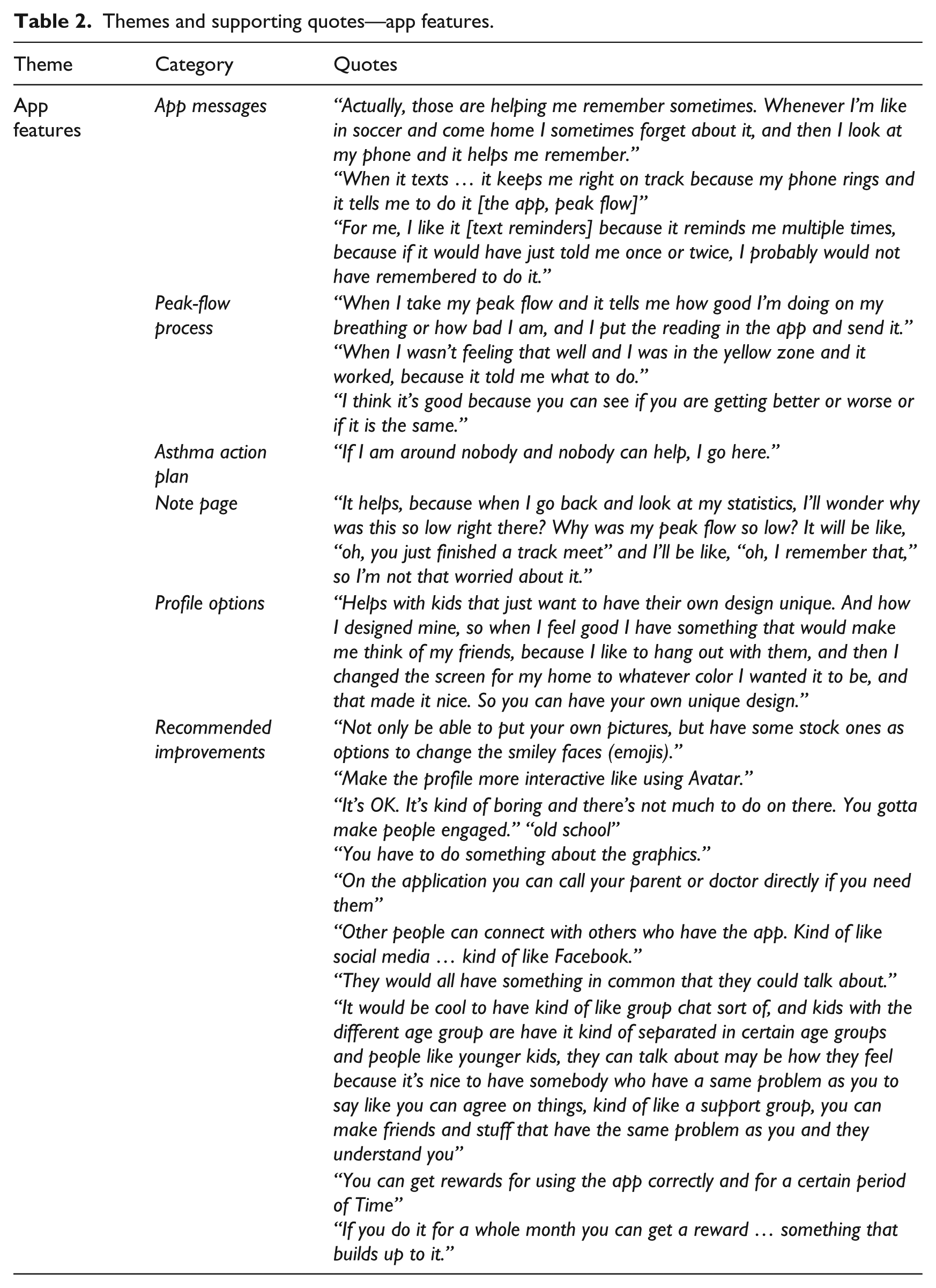
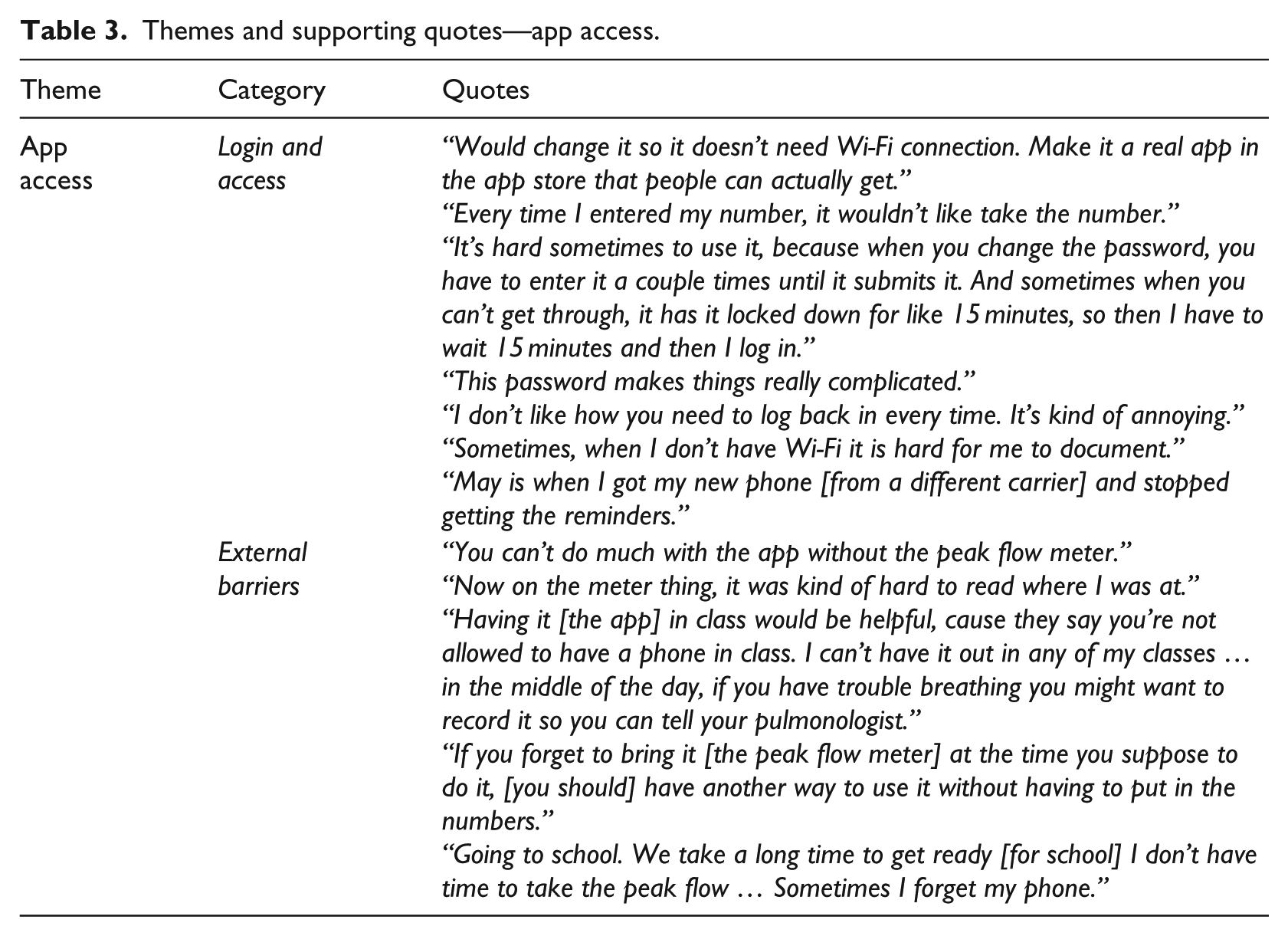
Through an inductive process, study personnel classified the codes yielded by the thematic analysis into three themes: app features, access to app, and asthma self-management. Tables 2 to 4 present the identified themes and supporting quotes.
Themes and supporting quotes—app features.
Themes and supporting quotes—app access.
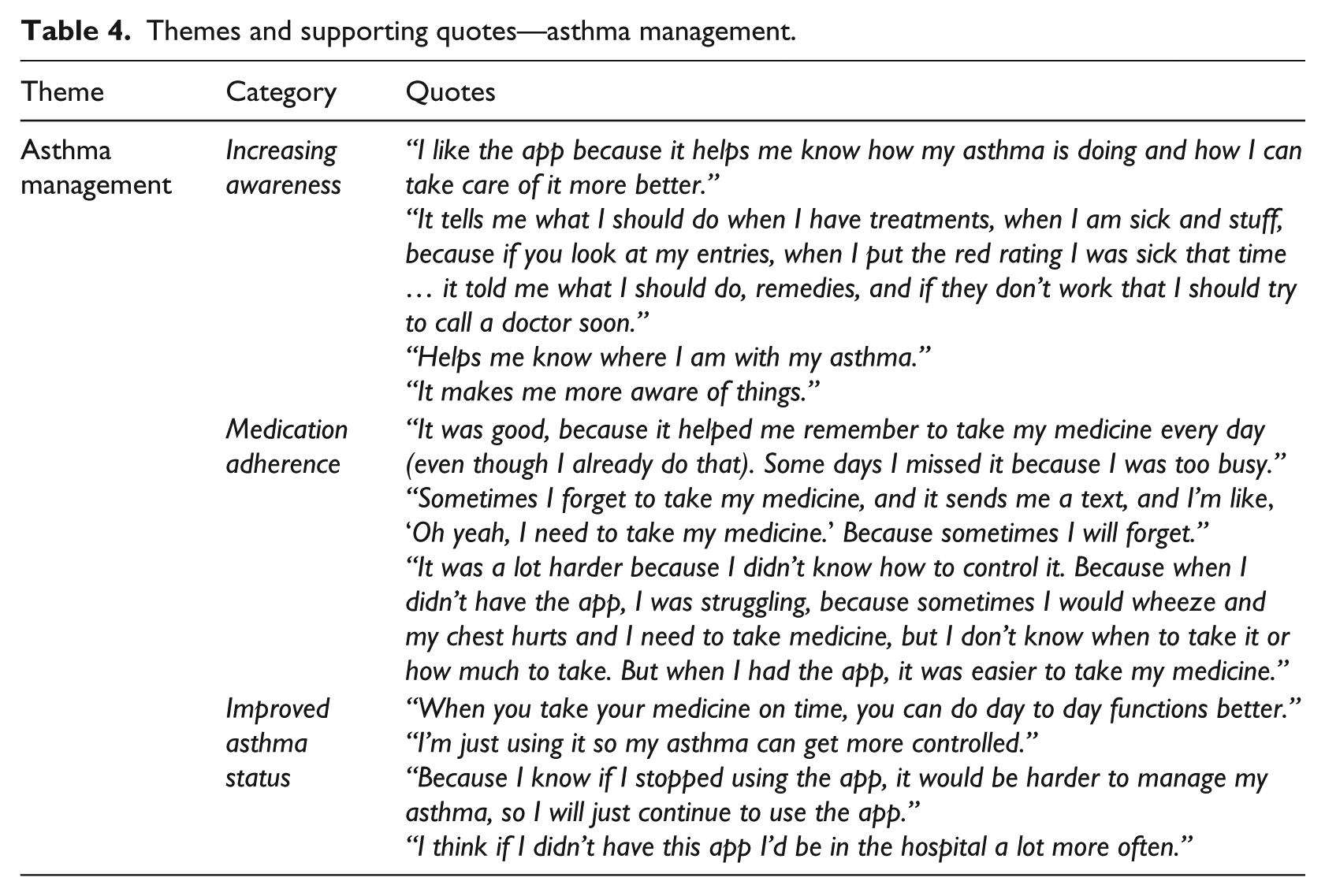
Themes and supporting quotes—asthma management.
App features
System messages
Participants received three types of messages through the app: twice-daily reminders to use the app, reminders after low readings, and inspirational messages.
The majority of participants (n = 18) thought receiving twice-daily reminders prompted them to take their medicine and to check their peak flow, actions that without the reminders they would have probably forgotten. A few (n = 3) also stated that they only use the app when their reminder comes. Participants also liked the frequency of the reminders and ability to schedule them at convenient times. Five participants, however, thought that there were too many reminders to check peak flow and found them to be “annoying” rather than helpful. Furthermore, participants requested additional reminders for the times they were scheduled to take their prescribed medications.
Reminders to follow-up after a low peak-flow reading were perceived as beneficial; these recommendations helped the participants know what to do next. Some (n = 2) participants thought the advice could be clearer. With respect to the inspirational messages, three participants could not recall receiving any. Of those who recall receiving them, participants thought the inspirational messages are useful; they suggested increasing the pool of messages to avoid repetition.
Peak-flow process
To comply with the recommended standard of care, multiple elements were integrated into the peak-flow entry progression. As portrayed in Figure 1, the user (1) enters how they are feeling (i.e. good, okay, or bad) by selecting a corresponding emoji faces (i.e. green, yellow, red), (2) selects relevant symptoms, (3) provides a current peak-flow value, and (4) writes a note if desired.
Based on the users’ report and their individual AAP, users receive a message guiding them how to manage their asthma.
With respect to this series of features, participants perceived the peak-flow entry process as the main way they used the app. Some (n = 9) particularly liked noting their symptoms using the notes functionality to write how they were feeling at the time of the reading, mainly to explain low readings. Participants liked the integrated navigation of this process; most importantly, the integration of AAP recommendations into the peak-flow entry process. Out of 20 participants, 8 specifically appreciated the advice on how to improve their peak-flow value and when to take emergency medications and 9 noted liking the “emoji” faces reflecting how they feel and think in terms of green, yellow, and red readings. Although users could visit their notes and AAP pages outside the peak-flow process, most (n = 11) did not use these features. The majority (n = 13) did, however, value the option of revisiting or sharing their notes with the physician to explain asthma patterns. The main barriers in these features were related to technical problems with submitting a peak-flow entry.
An additional feature was the goal tracker. Peak-flow values were stored in a graph, enabling users to compare their latest value with previous values and their personal goal. Those who expressed liking the goal tracker feature (n = 18) said it was most helpful for them viewing asthma patterns over time. Many (n = 11) said the graph’s use of the colored zones to indicate their peak-flow measures (as seen in Figure 1) helped them visualize if their asthma was “better” or “worse.”
Profile options
Whereas most (n = 18) participants only used the profile page minimally, many (n = 11) expressed that they appreciated having the option to change the wallpaper color and designs on the page and customize the “emoji” faces to express how they feel at the time of data entry. Participants liked having the option to customize their profile picture, yet the majority (n = 12), specifically older participants (aged 15–17 years), did not use this function.
Recommendations for improvement
When asked about recommendations for design or functionality improvements, participants stated that the app is good in its current version and provides the basic functionality needed for them to track their asthma. Overall, participants felt that the app design is outdated and could be improved by adding a larger variety of colors, backgrounds, font options, and graphics. They suggested that the app include more customization options to make it look less medical, such as allowing the upload of any picture and making the profile more interactive with a customizable avatar.
Participants also suggested new elements to include in the app; overall, similar patterns were observed among the younger and older participating adolescents and across genders.
First, participants expressed their interest in receiving training material through the app, mainly in the form of short video clips. Recommended training topics included a tutorial on how to use the app, information on strategies to self-manage asthma, or general information about asthma. Other suggested elements included incorporation of role model (celebrity/athletes) testimonials on how they cope(d) with asthma, as well as live video chats with healthcare staff to train on asthma management activities and communicate asthma information.
Second, communication was mentioned in several levels: communication with tech support, app team, healthcare staff, parents, and finally, other teens with asthma. Participants of all ages expressed interest in having a two-way interaction option with the healthcare providers. Three further suggested communication with app team through video chats that would reach out to people using the app, similar to the video tutorials. They also suggested sending periodic video clips or “any new content at times to interact with the users.” Social media components were seen by four, mainly older male participants as a potential way to connect with other teens. This was perceived useful to help users communicate with other teens who have asthma—either app users or simply other teens—to share how they are feeling. Three participants thought it would be very helpful to communicate with others who experience similar conditions, while others did not feel strongly about it.
Finally, participants thought that the app should include fun/entertaining elements. These elements would attract them to use it more frequently and be more engaged with the app. Suggestions included games, avatars, design elements, and incentives on app use. For instance, one suggested game would have the user’s avatar navigate through town and make choices linked to different scenarios in asthma management. Furthermore, participants suggested adding visual or sound effects when reaching goals or using the app. Some (n = 3) mentioned adding a variety of rewards and more engaging tasks that would enhance app use. Avatar accessories, points, stickers, badges, or more app design elements were some rewards suggested for keeping users coming back to the app.
App access
Access and login
Internet access and login information were identified as external barriers to app use. The app, in its current version, is a web-based agnostic platform compatible with all types of smartphone systems (Android, iOS, etc.); this format requires either a data plan or Wi-Fi connection for the user to submit information. Limited data and inconsistent Wi-Fi connection presented barriers to use for three of the participants; others had competing priorities for utilizing their data plan and preferred not spending their “budget” on the app. As a solution, these adolescents suggested designing the app to perform offline with occasional data uploads to avoid dependence on an Internet connection.
In compliance with the Health Insurance Portability and Accountability Act (HIPAA) regulations, app log-in required a user password. This appeared to be a common problem, as users frequently forgot their password or did not properly access their unique URL created for the study. Participants also recounted times when their peak-flow entry would not be saved, which investigations revealed happened if participants revisited a pre-opened URL after their password timed out. A suggested solution was to add a function that allows users to save the access information and direct app download to avoid URL mistakes.
External barriers
Furthermore, participants listed external barriers to app use that are not related to app functionality. These encompassed (1) non-continuous access to a phone for reasons such as battery life, broken device, and loss of phone privileges; (2) school policy that prohibits the use of their phones while in school; and (3) limited free time and overwhelming schedule, especially before school.
Finally, to enter data into the app, one would need a peak-flow meter to measure lung capacity. Unlike their phones, the peak-flow meter is not always accessible to the adolescent. The need to carry another large device limited the opportunities for participant use of the app.
Asthma management
Increased awareness
Adoption of asthma self-management skills was the underlying goal of this app. The overwhelming majority of the participants (n = 18) reported that their ability to manage their asthma improved after using the app. Specifically, the participants displayed increased knowledge of peak-flow scores and how these relate to their asthma status. They noted that the app helped them recognize if their asthma was better and to be aware when they experienced more severe asthma symptoms. They also expressed that the app helped their understanding of asthma triggers such as heavy exercise or certain weather conditions and the connections between the symptoms and those triggers. Overall, the participants felt more independent in regard to managing their asthma. Through the daily reminders, peak-flow scores, and follow-up guidance, they felt aware of their asthma on a day-to-day basis.
Medication adherence
Although the current version of the app does not provide a specific reminder to take asthma medication, most participants (n = 17) noted that the app prompted them to take their maintenance medication regularly and on time, resulting in more consistent adherence to their treatment regimen. Some (n = 8) appreciated the benefit of getting specific instructions for emergency medication when asthma is in the yellow or red zone. App use also reminded two users to take their inhaler with them to school or other out-of-home activities. Several participants thought the improved medication adherence resulted in an overall better asthma control and fewer exacerbations.
Improved asthma status
Overall, participants felt that their asthma symptoms or the way that they self-manage their asthma improved since they began using the app. Participants noted many times that the reminders helped them improve their overall asthma management by knowing when it was time to take their medication or use their peak-flow meter. Also, physiological asthma symptoms for some participants were said to have improved over the course of the study as well; one participant mentioned he would be hospitalized more often if he were not using the app.
Discussion and conclusion
Discussion
The convenience, accessibility, and immediacy of smartphones position a variety of populations within easy reach and generate an opportunity for targeted information exchange. Researchers around the globe invest efforts in exploring the role of mHealth in facilitating disease education, self-management skills, and patient–provider communication. 17 While some mHealth interventions show user acceptance of the tools offered and preliminary positive adoption of asthma management practices, the field lacks detailed qualitative research that explores users’ perspective of these technologies.17,18 Furthermore, gaps exist in mHealth apps that target adolescent populations or that are carefully tailored to the preferences of certain consumer groups. More so, studies assessing the acceptability, feasibility, and impact of mHealth as a form of asthma disease care among adolescents are sparse. 19 In addressing these gaps, this study—from its preliminary phases through the trial—has added a breadth of qualitative knowledge capturing adolescents’ experiences and perceptions. Overall, participants in the study shared positive feedback on the tested app. App features offer a feasible supplement to the traditional disease care that is compliant with the recommended patient-centered care elements (i.e. supported self-management, patient–provider non-face-to-face communication, and a care management plan). Further improvements are imperative to enhance systems functionality and app use by the intended users. Specifically, participants recommended more engaging elements, interactive training material, and opportunities to communicate with their healthcare providers, tech support, and each other through the app. The involvement of the targeted groups in the development and pretesting phases is essential to designing a relevant and effective tool.20,21 Moreover, whereas messaging was found to enhance patient–provider communication, apps to date lack messaging that is responsive to the patient’s present disease status. 17 We believe the tested app is a step forward in filling this gap by sending the user clear action steps that link their asthma status (i.e. symptoms and peak-flow values) to their individual AAP. The app further provides a link to phone number of provider on call where users can contact live support/help when asthma exacerbation or emergency occurs. In the next phase of this app development, we plan to link the patients’ real-time asthma status to healthcare personnel.
While numerous pilot studies have shown plausible and positive results in asthma outcomes,3,22,23 future research should incorporate larger sample size and implementation over a longer period to evaluate effectiveness and sustainability of mHealth interventions. Studies should also determine the optimal frequency of messaging and interaction with the users to facilitate compliance while avoiding user fatigue. To better understand the usability and effectiveness of the app on both ends of the system, insights of other stakeholders (e.g. healthcare providers) are valuable in refining the app to meet standards of disease care and user needs. 7 Furthermore, to establish evidence-based practices in mHealth, a randomized controlled trial is recommended for future research design. This allows the evaluation of the mHealth intervention’s impact on self-management practices and asthma outcomes with a larger sample size and in comparison to the traditional, in-person care.
Limitations
While the selection of a purposive sample may pose a bias, the requirement of a verified physician diagnosis of persistent asthma limited our potential patient population, as we could not rely on participants’ self-report. Working with a specific age group and in a specific geographical area likely presents barriers to generalizability of findings, yet such specifics are important as the literature indicates effective disease management tools should be tailored to the users’ needs and preferences.4–7 We, therefore, think that the strength of focusing on a specific group in the development of a user-centered app exceeds its limitation. In addition, despite the small sample size, our data collection reached saturation; noted by information redundancy and lack of new ideas that arose by the participants beyond the 10th interviewee. Finally, the trial period of 3 months limited our ability to evaluate the sustainability of app use and long-term user preferences and perceived benefits. We hope to overcome this gap in future inquiries.
Conclusion and implications
Mobile devices can improve access to asthma education and asthma care through an easy reach of specific targeted groups. The study findings demonstrate that the tested asthma app is a viable means to assist adolescents to manage their asthma. Participants’ recommendations can inform future development to improve adolescent compliance with asthma self-management guidelines. Further research efforts should assess the impact of app use on asthma outcomes over a longer term of follow-up period and in comparison with traditional care. The feasibility of utilizing such technologies within the clinic setting should be tested as well.
Footnotes
Author’s note
Laura Baum is now affiliated with RTI International.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of South Florida College of Public Health Interdisciplinary Team Award to Dr Amy Alman.