
Abstract
Web medical forums are relatively unique as knowledge-sharing platforms because physicians participate exclusively as knowledge contributors and not as knowledge recipients. Using the perspective of social exchange theory and considering both extrinsic and intrinsic motivations, this study aims to elicit the factors that significantly influence the willingness of physicians to share professional knowledge on web medical forums and develops a research model to explore the motivations that underlie physicians’ knowledge-sharing attitudes. This model hypothesizes that constructs, including shared vision, reputation, altruism, and self-efficacy, positively influence these attitudes and, by extension, positively impact knowledge-sharing intention. A conventional sampling method and the direct recruitment of physicians at their outpatient clinic gathered valid data from a total of 164 physicians for analysis in the model. The empirical results support the validity of the proposed model and identified shared vision as the most significant factor of influence on knowledge-sharing attitudes, followed in descending order by knowledge-sharing self-efficacy, reputation, and altruism.
Keywords
Introduction
Advances in information and communication technologies have supported the proliferation of various modes of human interaction. One of these is knowledge sharing, which allows knowledge contributors to share their knowledge with others via online platforms. Although knowledge sharing has been well documented in the literature, most studies have focused on the sharing behavior within organizations and within virtual communities of professionals such as civil servants, 1 emergency response personnel, 2 information technology worker,3–5 knowledge-management (KM) practitioners,6–8 legal professionals, 9 managers,10,11 physicians,12,13 public relations work, 14 and software professional,15–18 where the focus of sharing relates primarily to work knowledge and tasks. Few studies have examined nonwork-related virtual communities such as online discussion forums, weblogs, and social media (Facebook).19–21
Various eHealth applications such as health information websites and online social support networks22,23 are now used in the field of health care. Web medical forums (WMF) are one type of health information website. WMF provide an online platform for discussions between patients and physicians and for medical consultations. WMF such as eHealth Forum (http://ehealthforum.com/), KingNet (http://www.kingnet.com.tw/), NetDoctor (http://www.netdoctor.co.uk/), and WebMD (http://my.webmd.com) not only provide forums for health-related discussions but also generate a significant amount of publicly available health information that allows patients to self-check their symptoms. Moreover, most WMF organize health questions by topic and allow site visitors to view physician-provided advice; furthermore, they also allow visitors to post health-related question to relevant forums, with some WMF, including eHealth Forum and KingNet, requiring visitors to register beforehand.
A core function of WMF is to answer the medical questions posted to the forum by site visitors, a form of knowledge-sharing behavior. Because knowledge contributors on ordinary online forums may also be knowledge receivers, reciprocity is an important motivator for participation, with participants anticipating future benefits from their present actions.3,6,7,9,19,24,25 Sharing medical knowledge on WMF differs significantly from the ordinary online forum. Previous studies on the knowledge-sharing behavior of physicians have only considered the knowledge sharing that occurs within the medical team. For example, Lipshitz and Popper 12 reported on knowledge-sharing behavior among medical staff in a case study. Ryu et al. 13 used the theory of reasoned action (TRA) and the theory of planned behavior (TPB) to examine the factors affecting physician knowledge sharing within a hospital department.
Social exchange theory (SET) argues that all human behavior involves benefit maximization and expects relatively long-term relationships from mutual interactions. 24 This theory is one of the most commonly used theoretical bases in studies of knowledge sharing.25,26 Motivations in SET are classified into two categories: extrinsic and intrinsic. Extrinsic motivations treat activities as a means to attain a desired result, while intrinsic motivations treat activities as an end in themselves. 7 The format of extrinsic may be monetary such as profit sharing or stock ownership or nonmonetary such as respect, admiration, or status.6,25,27 Reputation and reciprocity are the most important nonmonetary extrinsic motivations driving knowledge sharing within the SET framework in both work and nonwork contexts.7,9,24 Some knowledge-sharing studies that did not use SET as a base theoretical perspective also treated reciprocity as an important personnel motivator or contextual factor.3,5,9,19,20 A possible reason for this may be that their research setting was limited to ordinary online forums.
SET is also suited as a theoretical framework for exploring knowledge sharing within the WMF. This is because WMF also involves two important issues in knowledge sharing: (1) for physician-participants: WMF must provide benefits (extrinsic motivations) for forum participation. For example, WebMD, eHealth Forum, NetDoctor, and KingNet allow member physicians to post their icon and personnel profile on the forum and post links to personnel blogs as ways to help physicians raise their professional profile and promote their practice. Moreover, WMF should set a clear vision or mission that encourages regular participation from enthusiastic physicians. (2) For the knowledge sharers or contributors: the physician members of WMF should not only have clinical practices knowledge but also have an altruistic interest in sharing this knowledge with forum participants voluntarily and without monetary compensation.
WMF in this context differ significantly from those examined in previous studies because the knowledge contributors are invariably physicians and knowledge recipients are invariably patients or visitors. Reciprocity, one of the key extrinsic motivators identified in previous knowledge-sharing studies, is not applicable in the WMF context. Instead, shared vision (SV) and shared goals with the WMF likely play critical roles in knowledge sharing. WMF represent an increasingly popular form of online health-knowledge sharing and differ significantly from current knowledge-sharing virtual communities (ordinary online forums). WMF help forum participants obtain specialist advice regarding problems/illnesses, direction to the appropriate hospital department for care, facilitate patient care, and reduce the waste of health-care resources. SV should be an extrinsic incentive cultivated by WMF.
In light of the lack of studies investigating this unique knowledge-sharing setting, the objective of this study is to elicit the factors that influence physician willingness to engage in knowledge sharing through WMF. This study uses SET as its theoretical base and substitutes the concept of SV for reciprocity to investigate WMF knowledge-sharing intentions.
The following sections are organized as follows: the TRA is described in the “Theoretical background and hypotheses” section in order to describe the relationship between knowledge-sharing attitudes and knowledge-sharing-attitude intention in WMF. SET is then described as the theoretical framework linking knowledge-sharing attitude to extrinsic incentives such as reputation and SV and to intrinsic incentives such as altruism and knowledge-sharing self-efficacy (KSSE). Furthermore, the measurement instruments, pretest, participants, and data analysis method used in this study are all described in this section. Demographic variables, the measurement model, and the structural model are discussed in the “Results” section. Conclusions and limitations are presented in the final section.
Method
Theoretical background and hypotheses
Knowledge-sharing attitude toward sharing intention
According to the TRA, attitude positively affects behavioral intent. Studies of knowledge sharing have confirmed this positive relationship in the contexts of knowledge sharing and knowledge-management system (KMS) usage.6,10 Chow and Chan combined TRA and social capital theory (SCT) to survey the knowledge-sharing behavior of 190 company managers in Hong Kong. They found a positive association between the attitude of participants toward knowledge sharing and their intention to share knowledge. 10 Bock et al. conducted a field survey of 154 managers in 27 Korean organizations and confirmed this association. He et al.’s 28 application of SCT to explore the effect of social relationships on KMS usage also identified a positive effect of social relationships on attitudes toward knowledge sharing and, consequently, increased use of KMS. In the health-care field, Ryu et al. 13 applied TRA to investigate factors affecting physician knowledge-sharing behavior within a hospital; they further found physician knowledge-sharing attitude to be an important factor of influence on physician intentions. Hence, this study proposes hypothesis 1 as follows:
H1: Attitude toward knowledge sharing positively affects intention toward knowledge sharing within WMF.
Extrinsic incentives
As explained above, SET classifies knowledge-sharing behavior into extrinsic and intrinsic motivation categories. Extrinsic motivation describes those behaviors of an individual that are driven by the perceived values and the benefits of performing a particular action. 29 This motivation category should be cultivated by WMF through such measures as creating a reputation-enhancement effect for those physicians who actively participate and setting a clear mission/value for the WMF.
Reputation or “social reward,” the perception that contributing knowledge will enhance a contributor’s self-image and/or status as a perceived expert, 25 is a mechanism that may motivate an individual to share expert knowledge with others via a social network.1,7,24,29 To attract traffic to WMF, the forum should have adequate breadth and depth in their physician membership to respond appropriately to a broad spectrum of medical problems. To encourage active participation by its physician members, KingNet publishes a regular list of outstanding physician members, holds a regular participant poll to name KingNet’s “physician of the month,” lists physician members by name in each forum department, and indicates which physician members are currently “on duty” in each department. Based on the above, this study proposes hypothesis 2 as follows:
H2: Reputation positively affects physician attitude toward knowledge sharing within WMF.
Reciprocity is another key extrinsic incentive in the SET7,9,24,25,29 as well as an important knowledge-sharing factor of influence in both social cognitive theory and social capital theory.3,5,10,15,17,19,20,30 Social cognitive theory proposes that human behavior is the result of the reciprocal interaction of contextual factors and personnel cognition. Common contextual factors are community norms such as reciprocity, which reflects the belief that current knowledge sharing with others will be reciprocated with future help from others at some point in the future.3,5,15,17 Social capital theory postulates that social capital, embedded in the relationship between individuals and their community, influences interactions between individuals.10,19,20 Reciprocity relates to social capital via the affective nature of the connections between individuals in the community. However, the effect of reciprocity is not consistent. While some studies have found reciprocity to relate positively to intentions or behaviors toward knowledge sharing,3,20 others have not.9,19,24 This difference in findings may be due to the varied nature of communities, with task-oriented or long-term “strong” communities more focused on reciprocal benefits.9,19
WMF are nontask-oriented communities. Therefore, this study did not adopt reciprocity as an extrinsic incentive. Furthermore, because the perceived values of an individual represent an extrinsic incentive, 29 SV or shared goals, that is, the extent to which people in a community share a common perspective or understanding, is one distinct type of cognitive social capital or contextual factor.3,7,10 As the cognitive dimension of social capital, SV significantly affects cohesion among the members of a community and is critical in creating a meaningful sense of community.10,30 SV may be leveraged to enhance intra-community communications and minimize misunderstandings during interaction within communities. 30 The SV of these communities creates social interaction, allowing its members to increase the depth, breadth, and efficiency of their knowledge and idea sharing.3,10 The effect of SV on knowledge sharing was confirmed by Chiu et al. 3 and Chow and Chan. 10 Chiu et al. 3 tested their model with the members of one professional virtual community called BlueShop, a well-known IT-oriented virtual community in Taiwan. Chow and Chan 10 surveyed 190 managers from Hong Kong firms.
WMF own a cyberspace platform that allows physicians to share medical knowledge within the forum; WMF should provide a clear vision statement, such as “enhances the well-being of patients and reduces the waste of healthcare resources,” to earn the recognition and the enthusiastic and voluntary participation of physicians. This study thus proposes that SV increases the understanding of physicians regarding WMF and enhances their positive attitude toward sharing knowledge via the WMF, and proposes hypothesis 3 as follows:
H3: Shared vision positively affects physician attitude toward knowledge sharing within WMF.
Intrinsic incentives
Under the SET framework, intrinsic motivations may influence knowledge sharing in terms of altruism7,24,29 and personal characteristics such as self-evaluation/self-efficacy.9,21,29 Altruism is the degree to which one is willing to increase another’s welfare without expecting to benefit personally. 19 In sharing knowledge with others, the sharer is engaged in an intellectual pursuit or problem solving challenge that is self-fulfilling in terms of being an enjoyable challenge or simply fun. 9 Additionally, altruism plays a key role in nonwork-related virtual communities. Ma and Chan 21 found that altruism had a direct and significant effect on the willingness of users to share knowledge on Facebook.
KSSE is the degree to which an individual believes he or she is able to share knowledge.15,29 This belief may help motivate knowledge sharers to contribute knowledge. 7 In the context of the WMF, physician members should further have adequate clinical experience and medical expertise to respond to forum participant inquiries. According to Wasko and Faraj, 9 Kankanhalli et al., 7 Lin and Huang, 15 and Lin, 29 altruism and KSSE both positively influence knowledge sharing. Moreover, Ghobadi 18 reviewed the literature between 1993 and 2011 on knowledge-sharing behavior within software teams and found the capability of members to be an important driver as well. Based on the above, this study proposes hypotheses 4 and 5 as follows:
H4: Altruism positively affects physician attitude toward knowledge sharing within WMF.
H5: Knowledge-sharing self-efficacy positively affects physician attitude toward knowledge sharing within WMF.
Instruments and pretest
This study adopted multiple scales used previously in similar research. We modified these scales to fit the WMF knowledge-sharing context of this study. We derived four items from two studies for the reputation (Rep) construct.9,20 The scale used to measure SV was adopted from Chiu et al. 3 and Chow and Chan; 10 the scale used to measure altruism (Alt) was adopted from Wasko and Faraj 9 and Kwon and Wen; 31 the scale used to measure KSSE was based on Kankanhalli et al. 7 and Lin et al.; 5 the scale used to measure attitude toward knowledge sharing (ATKS) was adopted from Ryu et al. 13 and Hsu and Lin; 19 and the scale used to measure intention toward knowledge sharing (ITKS) was derived from Chow and Chan 10 and Ryu et al. 13
After the initial items were developed, this study used content validity index (CVI) to test the content validity of the measurement items. Six experts were recruited, including three internal medicine physicians, two surgical physicians, and one rehabilitation physician. These experts were invited to test content relevance by providing ratings ranging from 1 (very inappropriate) to 5 (very appropriate). The CVI was computed as n/N, with n representing the number of experts assigning a score of 4 to 5 and N representing the total number of experts. A CVI larger than 0.8 was considered good. A CVI between 0.6 and 0.8 was considered acceptable but requiring modification based on experts’ suggestions. In this study, the CVI scores for all items were higher than 0.82 with the exception of SV_2, which was 0.67. Table 1 summarizes the construct definitions, construct measurement variables, and construct references for all constructs after the modification of SV_2.
Constructs definition, measurement items, and references.
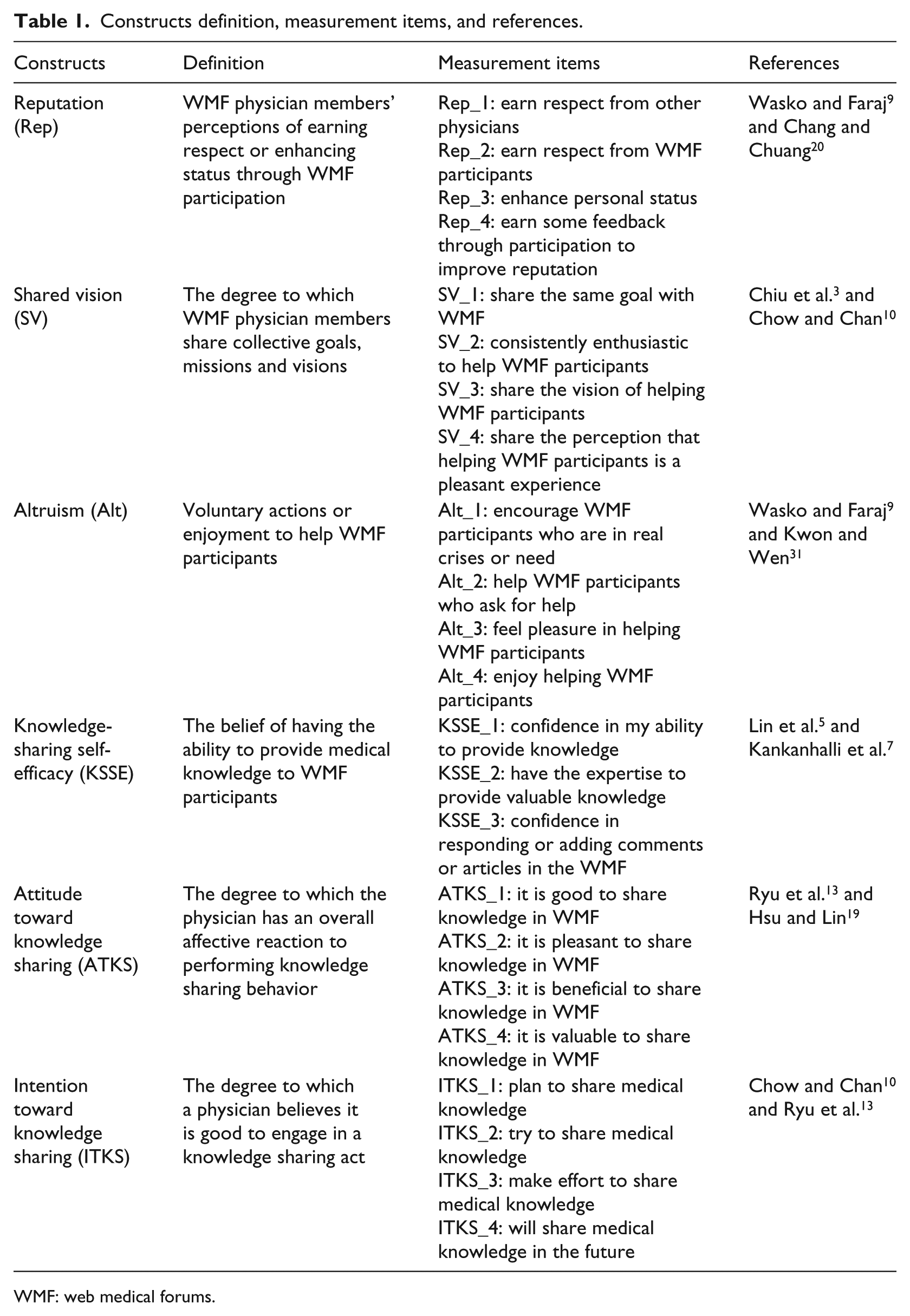
WMF: web medical forums.
The pretest questionnaire had two sections, with 8 questions in the basic information section and 23 questions for the six constructs (Rep, SV, Alt, KSSE, ATKS, and ITKS). A 7-point Likert-type scale was used, with scores ranging from 1 (completely disagree) to 7 (completely agree). A total of 20 physicians were recruited for pretesting to confirm item reliability. Cronbach’s α values for the six constructs in the pretest were 0.804, 0.808, 0.934, 0.865, 0.966, and 0.968, respectively.
Participants
The study used a conventional sampling method that directly approached Taiwan’s physicians in their outpatient clinic to invite them to join our study. We used G*power 3.1, a flexible statistical power analysis program for the social, behavioral, and biomedical sciences to calculate the required sample size. Given an F test (Linear multiple regression: Fixed model) effect size = 0.15 (medium effect size, α = 0.05, and β = 0.8), we obtained the recommended minimum sample size of 153. The study visited physicians in their outpatient clinic to invite them to volunteer for the study and to assure their anonymity. The study delivered the questionnaire and either waited in the outpatient clinic for the physician to provide the completed questionnaire or made an appointment to collect the questionnaire at another appropriate time. An initial 262 questionnaires were sent out and 164 valid questionnaires were collected and used in study research.
Data analysis
This study used IBM SPSS 20.0 and SmartPLS 2.0 (partial least squares (PLS)) for statistical analysis. PLS is a nonparametric, component-based structural equation modeling technique that does not require multivariate data normality and typically allows smaller sample sizes so that 30 observations provide robust results. PLS is the preferred research method in studies designed to predict rather than confirm structural relationships. 32 PLS is also ideally suited to assessing the validity of antecedent variables.15,33 Due to the relatively small (164) sample size and a focus on assessing the predictive validity of the antecedents of physician knowledge-sharing intention, this study focused on paths and used SmartPLS 2.0 to analyze data. 34
Results
Demographics
This study collected 164 valid questionnaires. Table 2 lists participants’ demographics in terms of gender, age, education, position, career, and medical department. Most participants were male (128, 78%); nearly half were in the age group of 31–40 years (76, 46.3%); over half were attending physician (92, 56.1%); one-quarter specialized in internal medicine (39, 23.8%); and three-quarters had over 9 years of work experience (127, 77.4%). In Taiwan, physicians are classified into 23 specialties, of which internal medicine, surgical, obstetrics and gynecology, and pediatrics have the most members, accounting for 21.02 percent, 8.40 percent, 7.50 percent, and 5.31 percent of all physicians, respectively, in 2012. A Chi-square goodness-of-fit test (χ2(4) = 1.622, p = 0.805) demonstrated that the ratio of these specialist categories in this study did not differ significantly from the overall population of physicians in Taiwan.
Respondent demographics.
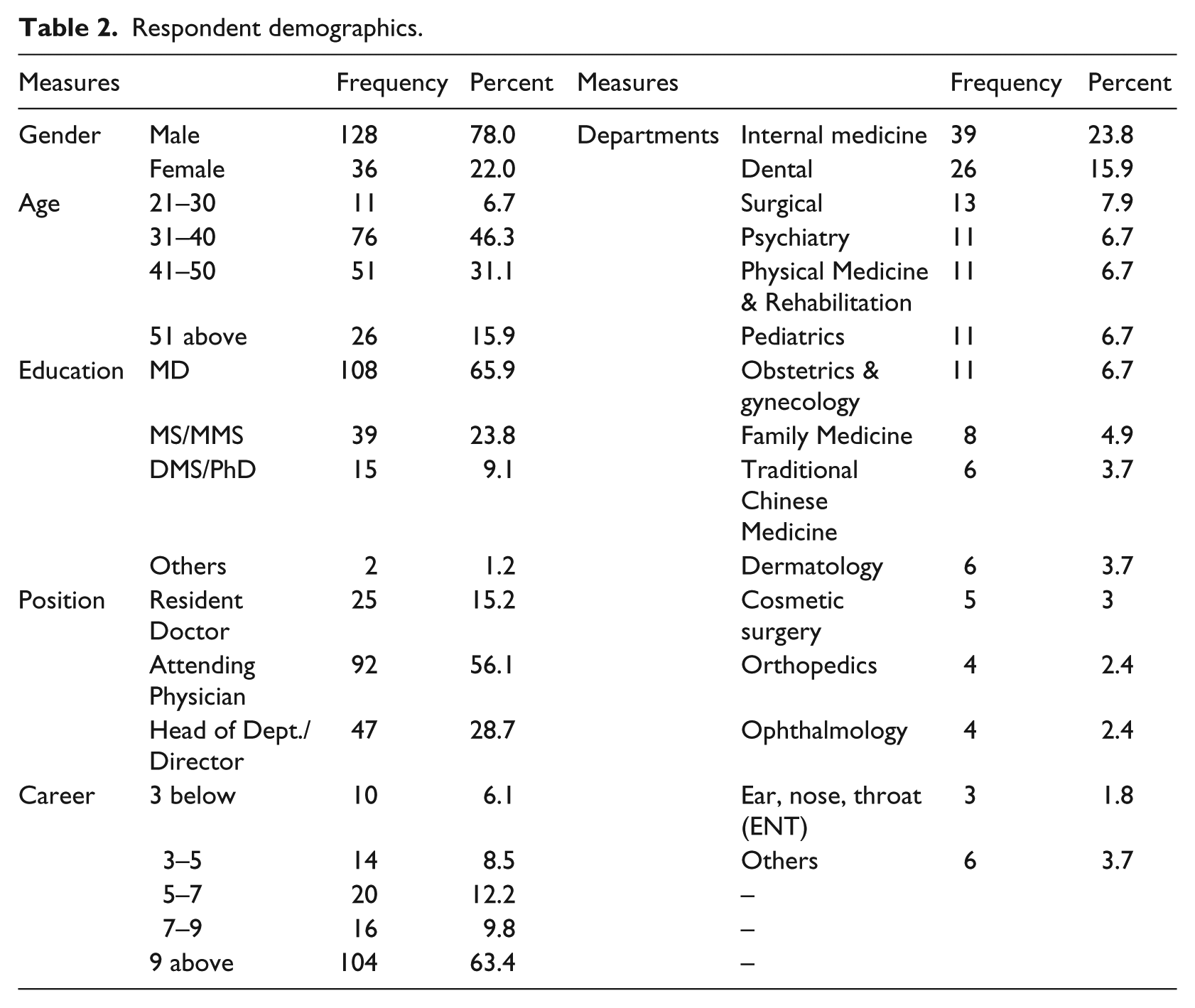
Of the 39 (23.8%) participants who were members of Taiwan-based WMF, 31 were members of KingNet and 8 were members of Taiwan eDoctor. Reasons given by participants for WMF participation (multiple answers acceptable) included the following: reducing the waste of health-care resources (19, 26.8%), helping patients (18, 25.3%), hospital policy (14, 19.7%), enhancing reputation (13, 18.3%), peer influence (4, 5.6%), and others (3, 4.3%). Reasons given by participants for not participating in WMF included the following: fear of confusing the patient relationship (56, 30.3%), fear of medical disputes (51, 27.6%), not asked to join (36, 19.5%), never heard of WMF (23, 12.4%), no practical effects (16, 8.6%), and time requirement (3, 1.6%). Most of the 39 who participated in WMF spent less than 30 min per week (21, 53.8%) followed by 1–2 h per week (9, 23.1%), 30 min–1 h per week (6, 15.4%), 4–5 h per week (2, 5.1%), and 2–3 h per week (1, 2.6%).
A total of 39 of the participants in this study had prior experience participating in WMF. To compare the differences between those with and those without prior WMF participation experience, the study conducted a t-test to compare the mean scores of the constructs that averaged all of the scores of indicators. The results show that WMF participators earned a significantly higher mean score than WMF nonparticipators on the following: SV (4.968 vs 4.614, p = 0.022), altruism (Alt; 5.679 vs 5.354, p = 0.032), KSSE (5.573 vs 4.667, p < 0.000), ATKS (5.404 vs 4.660, p < 0.000), and ITKS (5.468 vs 4.590, p < 0.000). The mean scores for reputation (Rep) were not significantly different between the two subgroups (4.276 vs 4.286, p = 0.451).
Measurement model
PLS analysis should assess the measurement and structural models. The measurement model should evaluate item reliability and construct validity, which comprises convergent and discriminant validities.15,33 Three criteria assess convergent validity for a construct: (1) all construct item loadings should exceed 0.70, (2) construct composite reliability (CR) should exceed 0.80, and (3) construct average variance extracted (AVE) should exceed 0.50. Discriminant validity is assessed using the criterion that the square root of AVE for a construct should exceed its correlations with all other constructs. 33
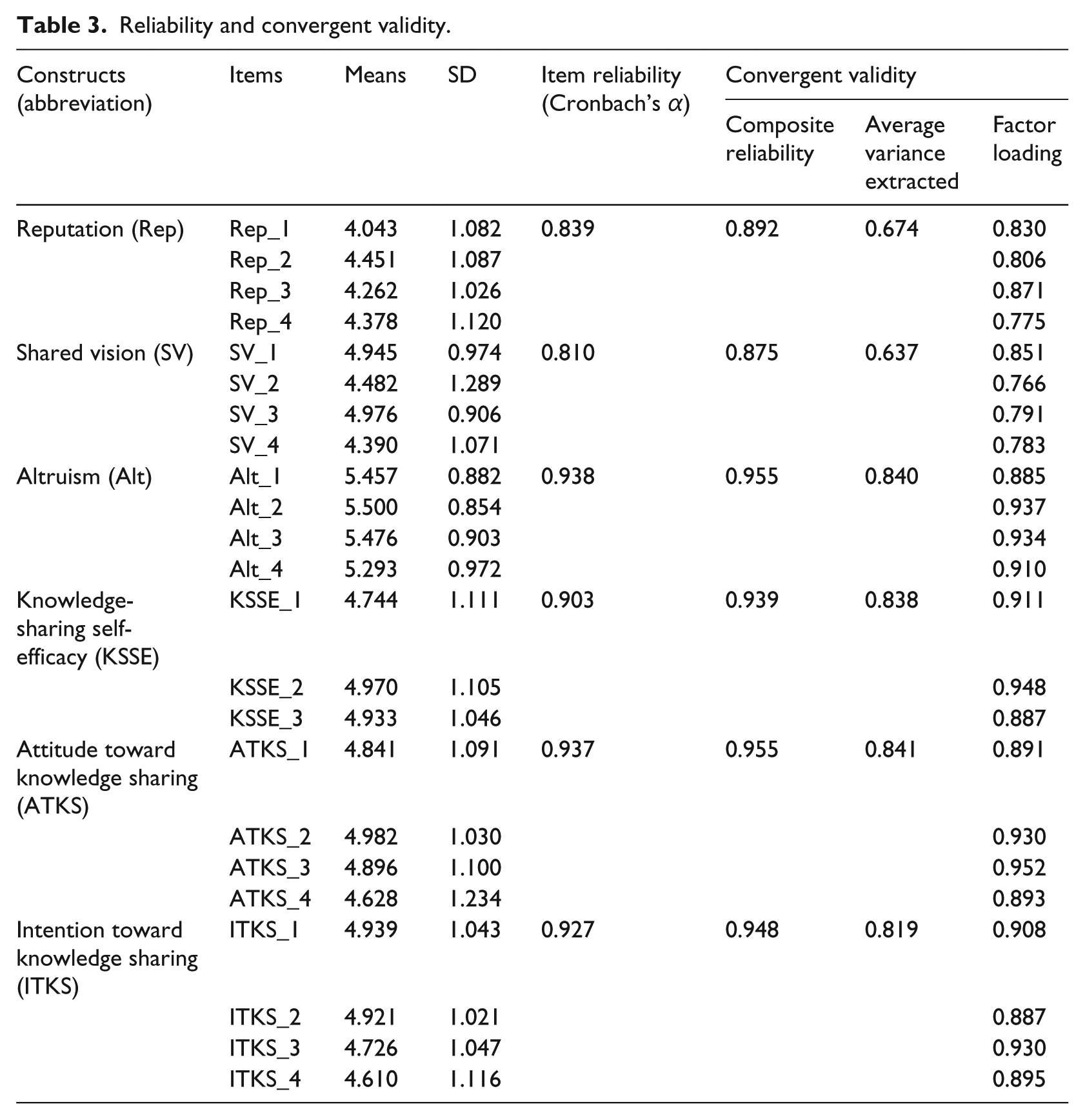
Table 3 shows the indices of reliability and convergent validities for the construct. Cronbach’s α was calculated to assess item reliability for each construct, with SV earning the lowest value (0.810). All items scored well above the minimum criterion of 0.70. Composite reliabilities ranged from 0.875 to 0.955, AVE ranged from 0.637 to 0.841, and item factor loadings ranged from 0.766 to 0.952. Taken as a whole, these indices indicate high convergent validity. Table 4 shows that the square root of AVE for the construct is greater than its correlations with other constructs, further confirming acceptable discriminant validity.
Reliability and convergent validity.
Square root of AVE values and correlations of constructs.
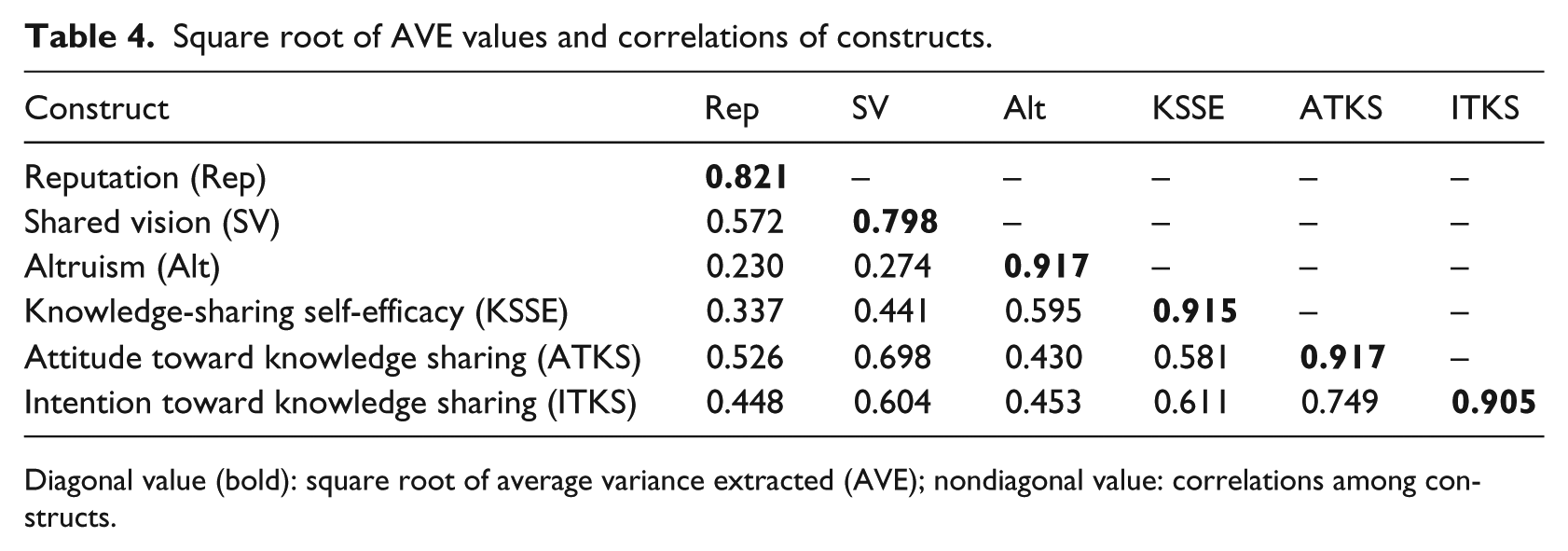
Diagonal value (bold): square root of average variance extracted (AVE); nondiagonal value: correlations among constructs.
Structural model
In PLS, the structural model estimates the standardized path coefficients used to indicate hypothesized associations in the research model as well as the predictive power of the structural model, as assessed using R2. This study used bootstrapping analysis to estimate path coefficients and statistical significance, and followed Wu et al. 33 to do 1000 times re-sampling to obtain a stable analysis result.
The R2 value for ITKS was 0.561, indicating the research model explained half of the variance in ITKS. The standardized path coefficients referring to the significant structural relationship were used to test the hypotheses. Figure 1 shows the results of the structural model.
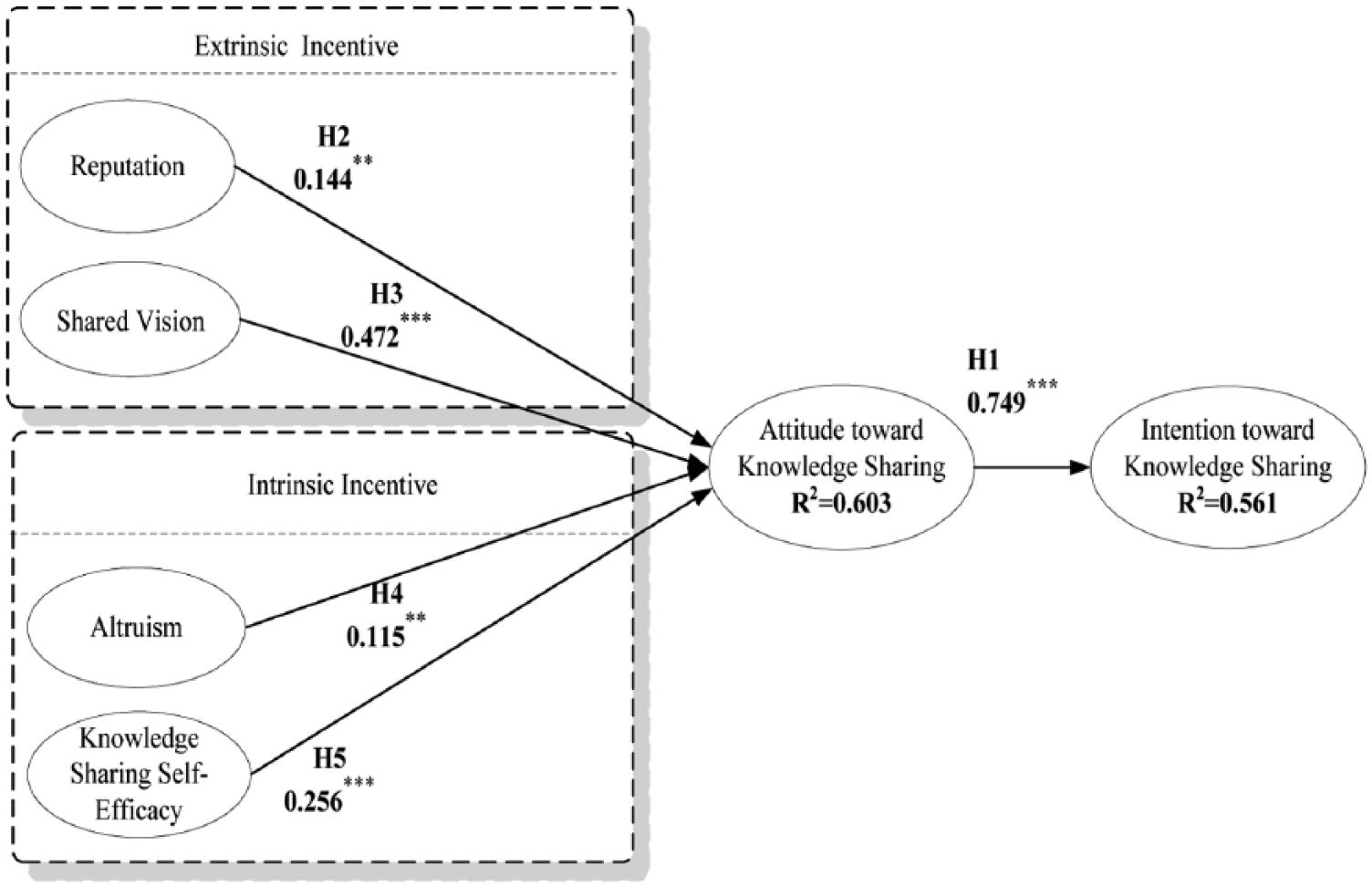
Results of the structural model.
The results indicate that ATKS is an important antecedent of ITKS (H1: β = 0.749, t-value = 17.690, p < 0.001). In terms of extrinsic motivations of WMF, which include reputation and SV, the results indicate that both reputation (H2: β = 0.144, t-value = 2.326, p < 0.01) and SV (H3: β = 0.472, t-value = 6.092, p < 0.001) positively impact attitudes toward knowledge sharing. In terms of intrinsic incentives, which include altruism and KSSE, the results indicate that both altruism (H4: β = 0.115, t-value = 2.083, p < 0.01) and KSSE (H5: β = 0.256, t-value = 3.523, p < 0.001) have significant, positive impacts on ATKS. Our constructs of reputation, SV, altruism, and KSSE together explained 60.3 percent of total variance in ATKS (R2 = 0.603).
Discussion and conclusions
Discussion
Our proposed model has good explanatory power for ITKS, with R2 = 0.561. This was higher than the knowledge-sharing study in the health-care context conducted by Ryu et al. 13 which earned an R2 of 0.461. Other studies of knowledge sharing reported similar levels of predictive power, including Bock et al. 6 with R2 = 0.318, Chow and Chan 10 with R2 = 0.60, Chang and Chuang 20 with R2 = 0.45, Lin and Huang 15 with R2 = 0.497, and Kwon and Wen 31 with R2 = 0.60.
This study found ATKS to positively affect ITKS. This finding is consistent with previous research works. Chow and Chan 10 integrated TRA with SCT and Hsu and Lin 19 combined TRA with Technology Acceptance Model (TAM) and found a positive effect of knowledge-sharing attitude on knowledge-sharing intention. Ryu et al. 13 applied TRA and TPB theories to investigate factors affecting physician’s knowledge-sharing behavior at hospitals in Korea and found attitude to be the second most important factor. Bock et al. 6 and Bock and Kim 1 employed TRA theory to explore knowledge sharing in Korea. Both verified the significant contribution of knowledge-sharing attitude to knowledge-sharing intention.
Four antecedents of ATKS, including reputation, SV, altruism, and KSSE, all had positive effects on ATKS. SV was the most significant factor of influence on ATKS, followed by KSSE, reputation, and altruism. Chiu et al. 3 investigated the effects of the social capital components, including social interaction ties, trust, norm of reciprocity, identification, SV, and shared language, on quantity and quality of knowledge sharing and found that knowledge-sharing quality was significantly affected by SV but not by norm of reciprocity and that knowledge-sharing quantity was significantly affected by norm of reciprocity but not by SV. Chow and Chan 10 compared the effects of three social capital factors (social network, social trust, and shared goals) on knowledge-sharing intention and found that shared goals, which means sharing the same collective goals, missions, and visions with others within an organization, is the most significant factor of influence on attitude toward knowledge. In terms of research setting, Chiu et al. 3 conducted their study on the professional virtual community and Chow and Chan 10 surveyed managers’ knowledge intention within their organization. While both of these research contexts did not distinguish between knowledge contributor and knowledge receiver roles, the research setting for this study defines participants (physicians) as knowledge contributors only. Because of the important role of SV in our research setting as well as those of Chiu et al. and Chow and Chan, SV may be a critical factor in various research setting contexts.
In terms of intrinsic incentive, this study found KSSE to be more important than altruism in the context of health care. The ability of knowledge contributors is a consistently important factor that influences willingness to share knowledge. Ghobadi 18 examined 49 studies related to the knowledge-sharing behavior of software teams and found capability to be one of the seven drivers of knowledge sharing. However, Kankanhalli et al.’s 7 survey of electronic knowledge repositories’ (EKRs) users in Singapore public sector organizations found that altruism had a larger effect than KSSE on knowledge-sharing behavior. Additionally, Ma and Chan’s 21 investigation of the motivators for sharing knowledge on social media (Facebook) reported that altruism contributed significantly more than other motivators to the observed explanatory power. Different research contexts provide a plausible explanation for this discrepancy. The health-care context of this study infers that the theoretical and practical knowledge of physician members should be of vital importance to forum users and that the quality of specialty-based clinical practices should be a critical determinant for forum users accepting a particular physician’s medical services. 13 Hence, KSSE may be expected to be more important to altruism in the health-care context.
In terms of extrinsic incentive, this study found the effect of SV to be higher than that of reputation. This finding was similar to Chang and Chuang, 20 who combined SCT and individual motivation to explore knowledge-sharing behavior in an online community. The authors used multiple regression to analyze their research model and found that reputation had no effect on knowledge sharing when the model included shared language (the cognitive dimension of SCT). Chow and Chan 10 integrated SCT and TRA to investigate the knowledge-sharing behavior of managers in Hong Kong and found that shared goals (cognitive dimension) contributed to knowledge-sharing attitude significantly more than trust (relationship dimension) and social network (structure dimension). This finding was attributed to the enhancement effect of shared goals/vision on mutual understanding, which fostered mutual cohesion and knowledge sharing.
Conclusion
This study based on SET proposes a model that investigates the factors of influence on physicians’ intent to share medical knowledge on WMF using extrinsic and intrinsic motivations. This model demonstrated good explanatory power for physicians’ intent to share knowledge via WMF. Furthermore, the most significant factor of influence on ATKS was SV, followed by KSSE, reputation, and altruism, respectively. In terms of extrinsic motivations, the influence of SV on ATKS was significantly greater than reputation. In terms of intrinsic motivations, the influence of KSSE on ATKS was significantly greater than altruism.
WMF should improve extrinsic motivations to attract more physicians to volunteer and actively participate as WMF members. Relevant measures include developing a clear mission statement and setting goals that reflect an SV with physicians such as enhancing the public welfare and reducing the inefficient use of health-care resources. These measures should be reflected in WMF practices. For example, the stated mission of eHealth Forums is “to preserve and improve human life by bringing health-related information to all people via the Internet” and that of NetDoctor is “collaboration between committed doctors, healthcare professionals, information specialists and patients who believe that medical practice should be based on quality-assessed information and, wherever possible, on the principles of evidence-based medicine.”
Furthermore, WMF should place greater emphasis on the mechanism of social reward such as promoting and enhancing the reputation of their physician members. For example, WebMD, eHealth Forum, NetDoctor, and KingNet all allow physician members to post their icon and personnel profile on forum websites. Moreover, WebMD maintains an online directory of their physicians, eHealth Forum allows physician members to hyperlink to their personal blog, and KingNet publishes a “top-10” physician ranking.
Limitations
Although this study used SET as the basis to investigate the factors influencing physician intent to share medical knowledge on WMF, there were some limitations. First, the participants were recruited using a convenience sampling method and were all from Taiwan. This method may have been affected by selection bias and thus the sampled population may not be the representative of the entire population. Second, this study represents the first use of all of the identified factors in the health-care context. These factors were adopted from previous studies that explored knowledge-sharing behavior in the information technology community. While the identified factors accurately described reasons for study participant willingness to participate in Taiwan-based WMF, other physician-specific factors such as fear of medical disputes and fear of confusing the patient relationship should be added into the model as negative factors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.