
Abstract
Mobile applications or ‘apps’ have significant potential for use in mental health interventions with adolescents. However, there is a lack of research exploring end users’ needs from such technologies. The aim of this study was to explore adolescents’ needs and concerns in relation to mental health mobile apps. Five focus groups were conducted with young people aged 15–16 years (N = 34, 60% male). Participants were asked about their views in relation to the use of mental health mobile technologies and were asked to give their responses to a mental health app prototype. Participants identified (1) safety, (2) engagement, (3) functionality, (4) social interaction, (5) awareness, (6) accessibility, (7) gender and (8) young people in control as important factors. Understanding end users’ needs and concerns in relation to this topic will inform the future development of youth-oriented mental health apps that are acceptable to young people.
Introduction
Mental health disorders affect approximately 20 per cent of adolescents in the developed world,1,2 and early intervention is essential in order to improve outcomes for young people. 3 A key challenge faced is how to develop effective interventions that are acceptable to adolescents and an innovative means of doing this is through mobile technology. Recent technological advances have resulted in the availability of more sophisticated and affordable mobile devices. The almost ubiquitous nature of these technologies makes them ideal sources for delivering cost-effective mental health interventions. Mobile technologies can provide almost constant support to users and allow interventions to be administered in users’ natural environments, thus ensuring a high level of ecological validity. 4 Such technologies may be particularly salient for adolescents, approximately 81 per cent of whom now own smartphones. 5 Adolescents use their phones on a daily basis and are likely to find them appealing as a familiar intervention medium. 6 Furthermore, as mobile interventions can be used at any time, in any place, they may be particularly valuable for adolescents in remote communities who face long waiting lists and limited choice of mental health services. 7
Currently, there is little research on the use of mobile technologies in mental health, particularly with adolescents. A small number of studies have explored the use of mobile technologies as supplements to therapeutic programmes with adults, and findings suggest these can be effective in reducing negative cognitions and improving behaviours.8,9 Studies suggest adolescents may also find this type of intervention useful, 10 and that mobile interventions based on self-monitoring principles may be effective in reducing depressive symptoms among adolescents with mental health problems. 11
Over the coming years, it is predicted that the use of mobile technologies in mental health will continue to rapidly increase. 12 Indeed, there are already a plethora of automated mental health programmes available to the general public as mobile applications or ‘apps’. In 2012, MobiHealthNews reported over 700 mental health apps were available to download in the Apple App Store alone. 12 However, the problem with almost all these health-based apps is that they are not research-based or subject to regulatory assessments or evaluations, thus their effectiveness cannot be verified. 13 There is a growing demand for the design, development and evaluation of evidence-based mental health apps that can be used effectively to improve mental health outcomes. 12
Human–computer interaction research emphasises that understanding end user needs is the first step in designing these types of technology-based interventions.6,14 However, there is currently a lack of research exploring users’ needs from mental health mobile apps. One study with adults identified privacy, feedback, ease and speed of use, personalisation and control over the amount of information received as important features in mental health mobile technologies. 15 However, adolescents’ experiences of mental health difficulties are different from adults and consequently they may have different treatment needs. 16
Whittaker et al. 10 reported cost, confidentiality, realism, credibility, positivity and simple, clear messages as issues highlighted by adolescents during the development process of their therapeutic mobile intervention. However, they did not elaborate on these issues or report details of adolescents’ perspectives on them. Researchers must develop a thorough understanding of adolescents’ needs to ensure that they can be appropriately met through mental health mobile apps. Consequently, young people will be more likely to use these apps, which will increase their overall reach and impact. 17 Furthermore, involving young people in the design process assures them that their voices are being heard and that their opinions are of value. However, to the authors’ knowledge, there is no existing study that has taken an in-depth approach to exploring adolescents’ needs from mental health apps.
The aim of this study was to address this gap and inform the development of mental health mobile apps by exploring (1) adolescents’ needs from mental health mobile apps and (2) adolescents’ perspectives on a mental health mobile app prototype. Given the exploratory nature of the research question and its concern with the subjective opinions of adolescents, a qualitative approach was considered suitable to obtain in-depth information from adolescents’ perspective.
Method
Sample
Participants were 34 adolescents (60% male) aged 15–16 years recruited from fourth-year classes (equivalent of UK Year 11) in two single-sex secondary schools in Dublin, Ireland. Single-sex schools are common in Ireland with 62 per cent of male and 73 per cent of female secondary school students attending single-sex schools. 18 Both schools were non-fee paying and neither school was categorised as socially or economically disadvantaged under national guidelines established by the Department of Education and Skills. 19 To ensure informed consent was obtained, students were provided with parental information sheets and consent forms prior to participation. Those who returned signed parental consent forms were eligible to participate.
Procedure
Ethical approval for this research was granted by the Human Research Ethics Committee in the authors’ university. Data were collected in March and April 2013 using five focus groups. Each group comprised between six and eight participants and lasted 30–40 min. It is recommended to conduct single-sex focus groups with adolescents as they may have significant interest in the opposite sex, which can adversely impact group productivity 20 and they may not feel comfortable discussing potentially sensitive or personal issues, such as mental health, in mixed-gender groups. 17 Therefore, three groups of male students and two groups of female students were recruited.
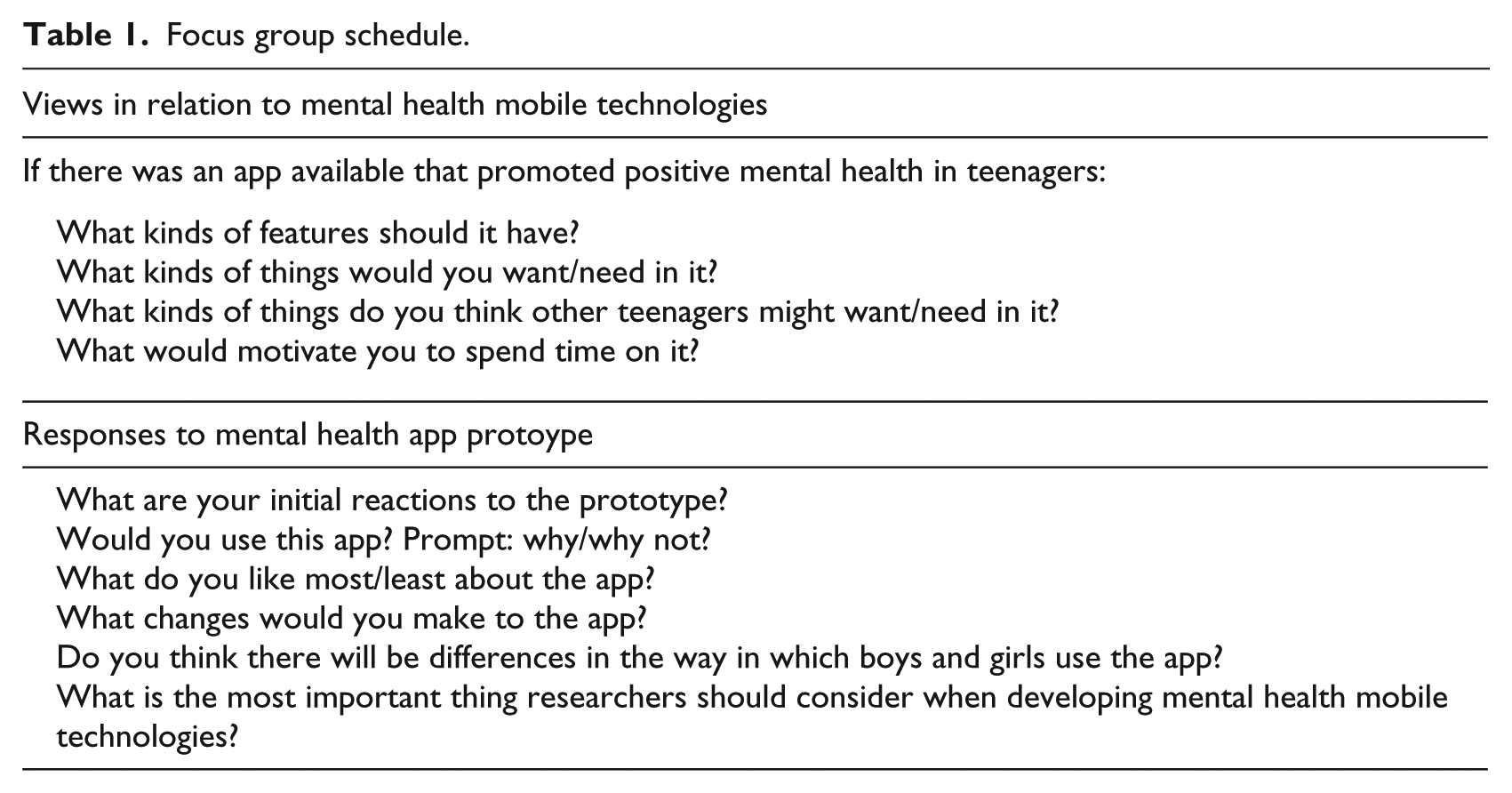
The moderator began the focus groups by providing students with a definition of positive mental health in order to ensure a consistent understanding of the term across participants. The definition of Positive mental health is as follows: ‘Positive mental health is not just the absence of mental health problems. Positive mental health is characterised by a person’s ability to fully engage in functions and activities such as learning, feeling and expressing positive and negative emotions, forming and maintaining good relationships with others, and coping with change and uncertainty’ (adapted from the Mental Health Foundation website http://www.mentalhealth.org.uk/help-information/an-introduction-to-mental-health/what-is-good-mental-health/). Students were then asked about their views in relation to the use of mobile apps to promote positive mental health and about their responses to screenshot images of a mental health mobile app prototype (see Figure 1). The moderator followed a focus group schedule and included prompts to focus the discussion and elicit further information from participants where necessary (see Table 1). Focus groups were audio recorded and transcribed verbatim.
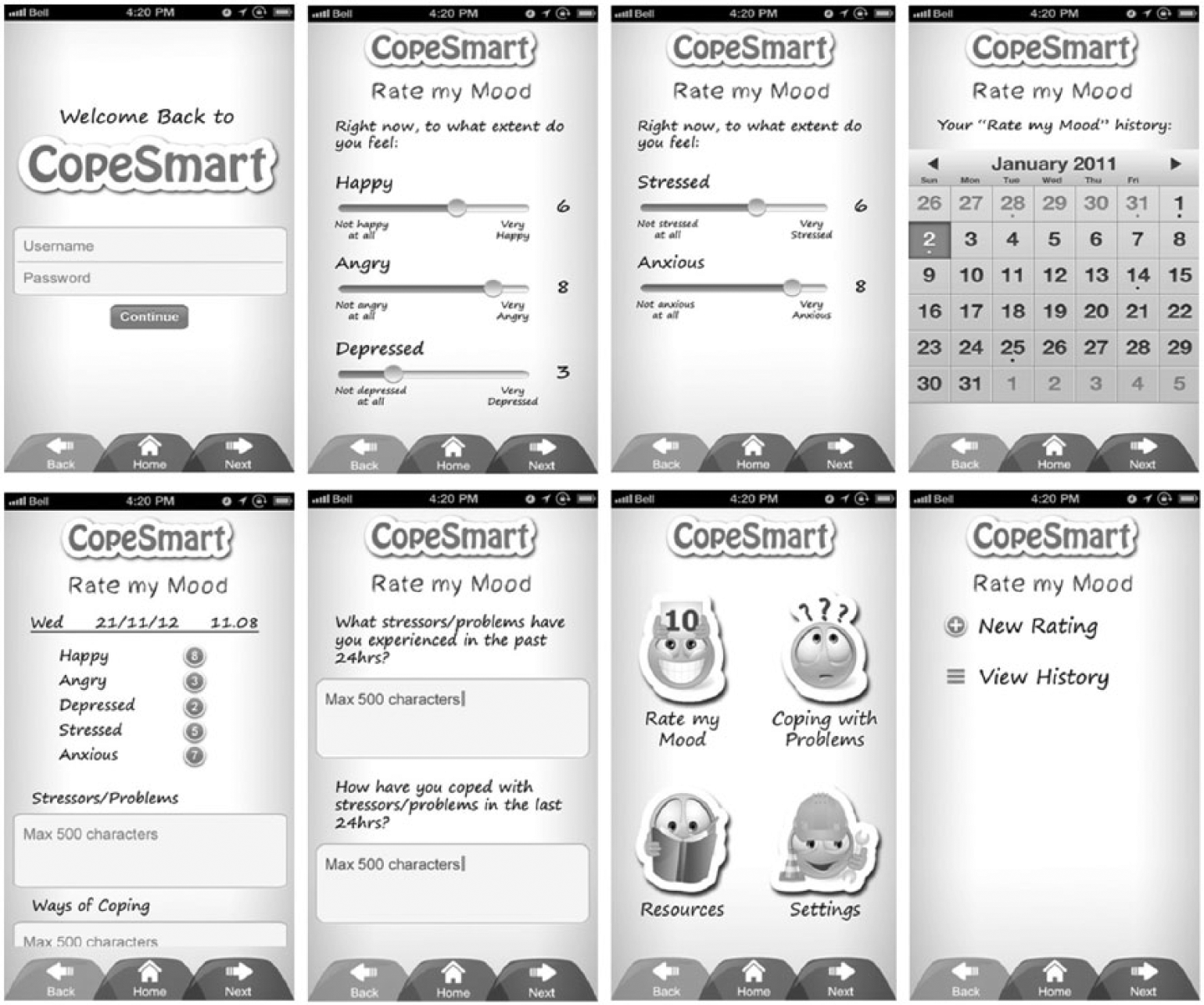
Prototype screenshots.
Focus group schedule.
Prototype design
Eight static images of prototype screens were created in consultation with a Dublin-based mobile development executive (see Figure 1). Prototype content was designed to be representative of a generic self-monitoring tool, similar to those used in previous research,6,11 on which an individual can monitor their mood, stressors and coping strategies on a day-to-day basis. Graphics and colour were included to enhance the prototype’s visual appeal and the prototype was given the name ‘CopeSmart’.
Analysis
Data were analysed using thematic analysis. This is a flexible method of qualitative analysis that allows for the identification of patterns of responding within the data. 21 This analysis was considered appropriate as it provides a richly detailed description of a data set and generates insights into participants’ perspectives on a specific topic. 21 Transcripts were initially analysed separately by two independent coders who subsequently compared and integrated their analyses, and through discussion developed a master-coding frame of themes identified within the data (see Table 2). Braun and Clarke 21 identify a theme as any subject relevant to the research question that is represented by some level of patterned response within the data set. Thus, in this study, a theme was considered to be any subject that was discussed by participants on more than one independent occasion during the focus groups. A third researcher independently applied the master-coding frame to approximately 60 per cent of the data, resulting in an inter-rater agreement of 73 per cent, which is considered an adequate level of reliability. 22
Coding frame detailing frequency of themes and subthemes within the data.
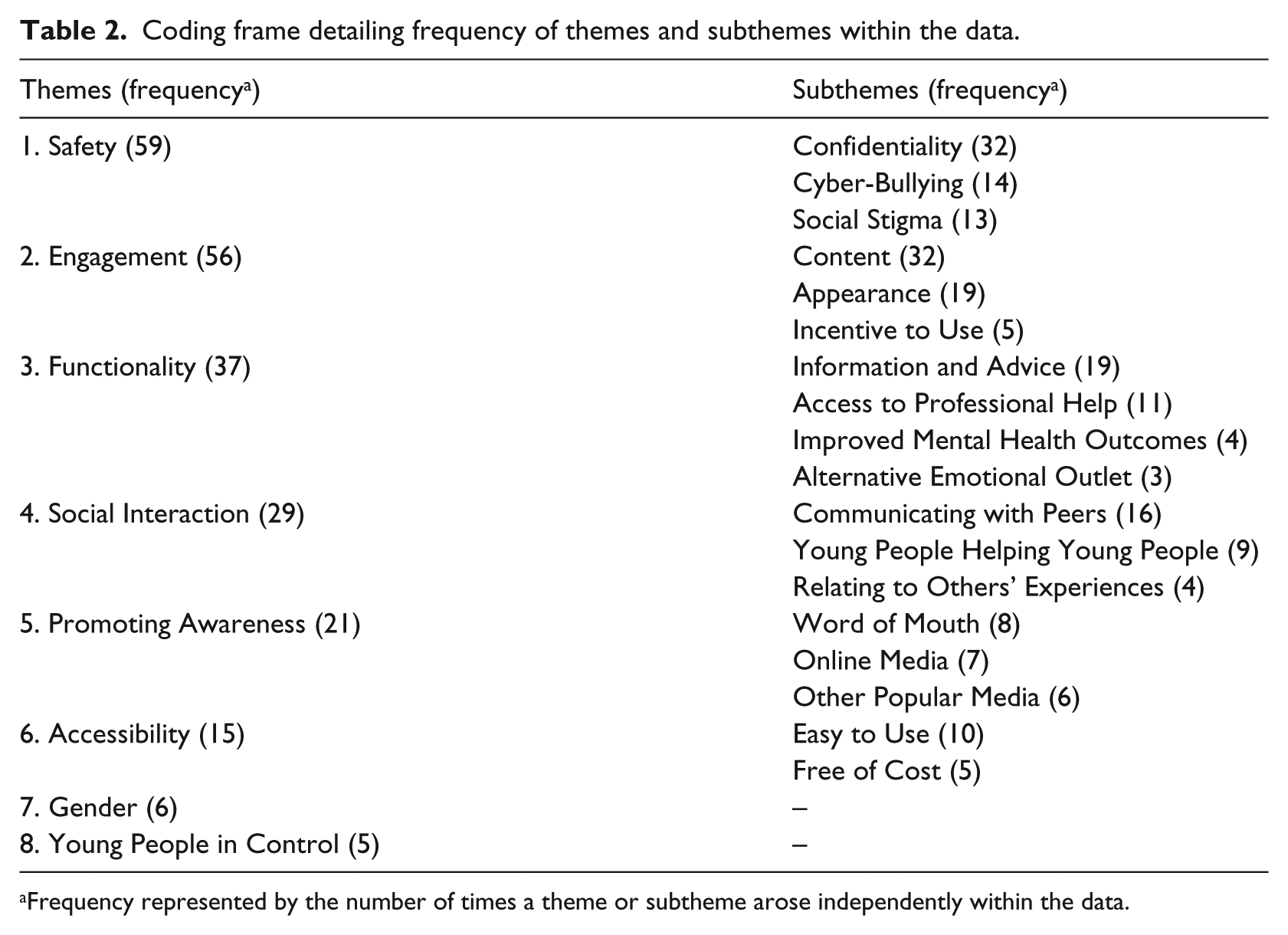
Frequency represented by the number of times a theme or subtheme arose independently within the data.
Results
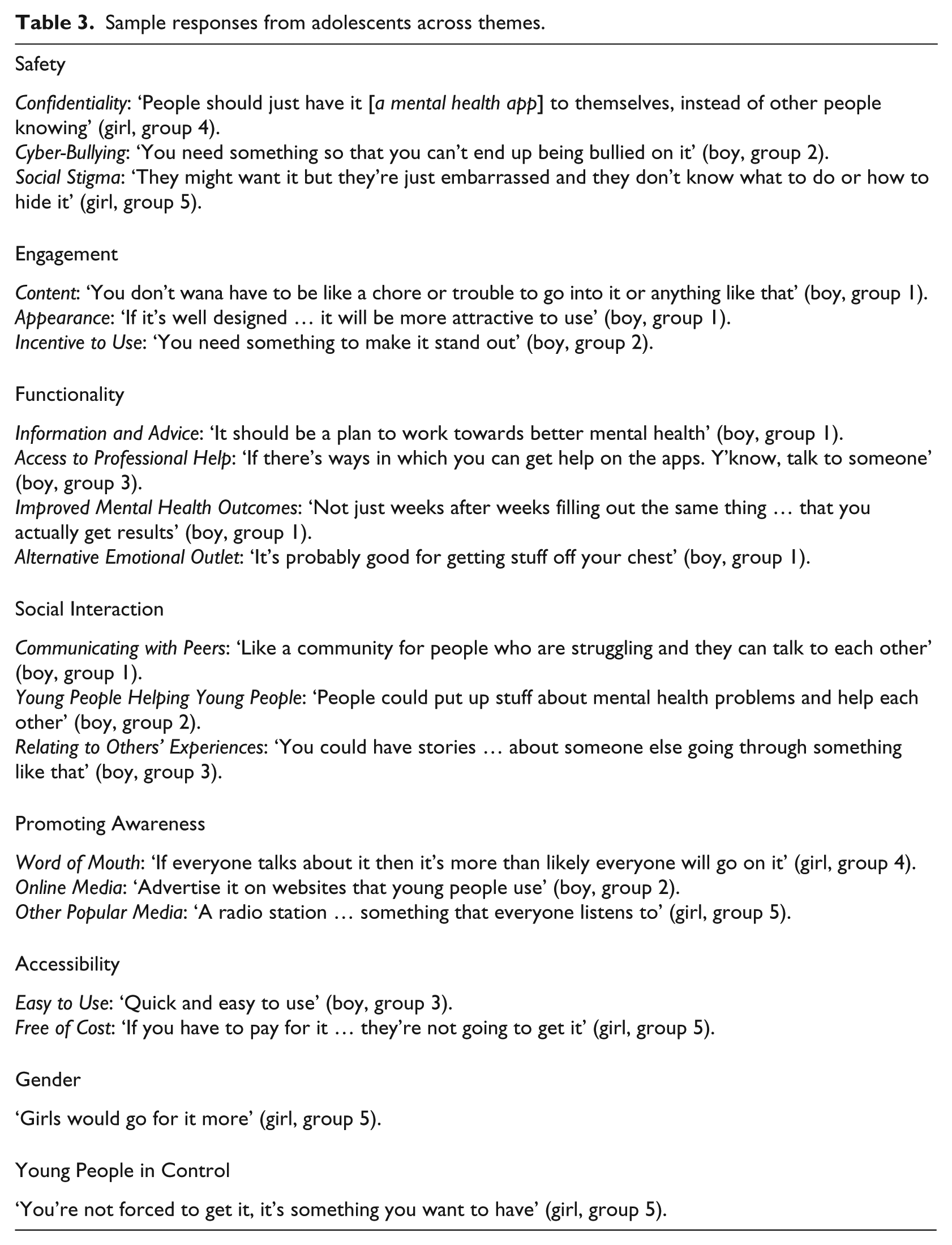
Eight core themes were identified in the data: safety, engagement, functionality, social interaction, promoting awareness, accessibility, gender and young people in control. A visual representation of themes is presented in Figure 2, and sample responses from participants across themes are detailed in Table 3.
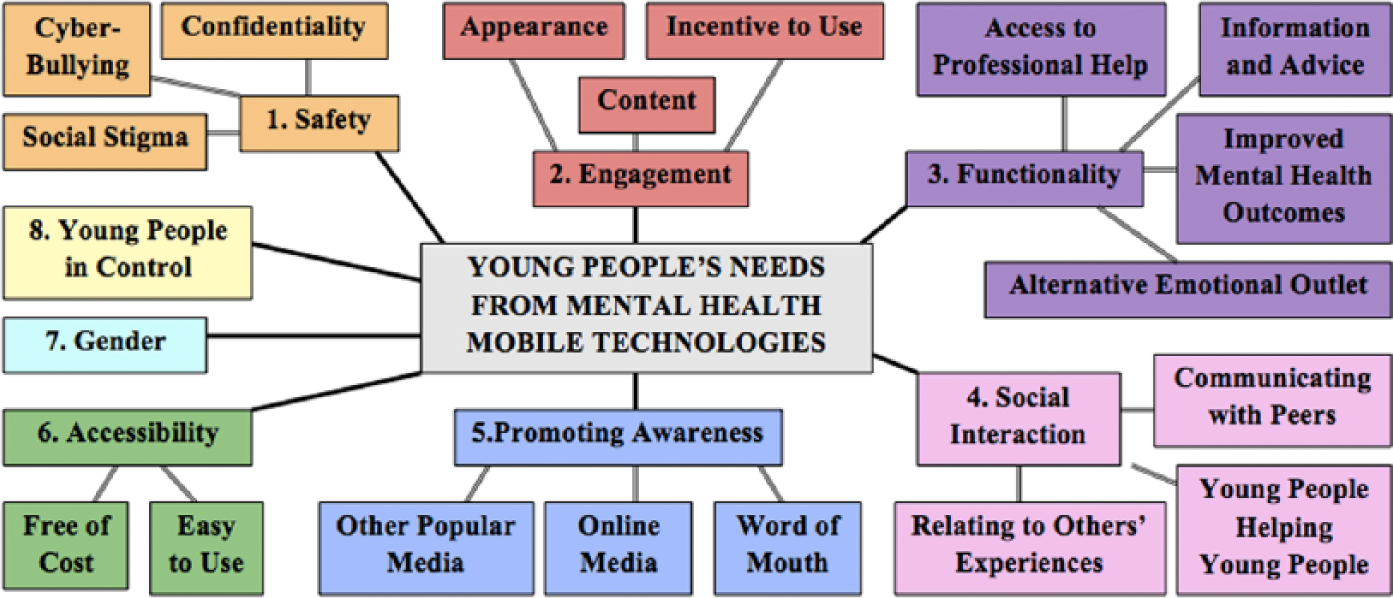
Visual representation of themes.
Sample responses from adolescents across themes.
Safety
Young people highlighted that mental health apps must be safe to use in terms of confidentiality, cyber-bullying and stigma. They reported that apps should be password protected and user control over privacy should be incorporated so users can choose whether they want to share their personal information or keep it private or anonymous. Cyber-bullying was a concern and participants reported that the anonymity afforded by some technologies encourages cyber-bullies to be abusive towards other users. Features such as the ability to ‘block’ bullies and report abuse to a moderator were identified as ways of dealing with this, although participants pointed out that this does not always solve the problem. Stigma was also an issue; participants felt that some people might not want others to know that they were using a mental health app. Ways of addressing this were discussed, such as ensuring apps are discrete and easy to conceal on a phone.
Engagement
Participants emphasised that mental health apps must be engaging and that information presented via apps should be concise and to the point. They reported that content should be made fun and interactive through the use of pictures, music, videos and games. The importance of an attractive interface that uses colour and graphics was emphasised and the ability to personalise the interface was appealing to participants, for example, by adding personal pictures and creating one’s own personal profile. Participants highlighted that apps must have something new or different to make them stand out so that teenagers will download and use them. Participants also said they would like the ability to set reminders so that they remember to use the app at different times of day.
Functionality
Participants ascertained that mental health apps must serve a useful and relevant function. The provision of information and advice pertaining to mental health was mentioned as important by participants, who emphasised that this information should be positive and uplifting. Participants also suggested that apps should provide access to professional help, for example, through a feature where users could send questions to mental health professionals and receive a response, or simply through the provision of contact details for mental health services. Participants also emphasised that they should notice tangible improvements in their mental health as a result of using these apps.
Social interaction
Adolescents reported a desire to use mental health apps to interact socially with peers in order to share problems, give each other advice and to relate to other adolescents’ experiences. It was suggested that anonymous forums could be incorporated where young people could chat and ask each other questions. The prospect of users being ‘matched’ to chat to each other based on their interests or problems they are experiencing was also suggested.
Promoting awareness
Adolescents emphasised the importance of creating awareness of these apps by promoting them through word of mouth. Participants reported that hearing their peers talk about using these apps would increase their social acceptability and incentivise other adolescents to use them. Promotion through online media such as Facebook, Twitter and mental health websites was suggested and some participants also discussed the potential of magazines, newspapers, television and radio as promotion tools. There was an emphasis on the importance of media being youth-focused, for example, teenage magazines and radio stations listened to by young people.
Accessibility
Participants outlined that mental health apps should be easily accessible, well designed and easy to use. One participant in particular highlighted the importance of using appropriate language to ensure any information provided is accessible to young people. Emphasis was placed on the importance of apps being free of cost and participants highlighted that if there is a charge for these apps, young people will not use them.
Gender
Some participants felt that boys would be less likely to use mental health apps than girls, which was expressed as being linked to the idea that boys are less willing to express emotion than girls. However, other participants felt that boys’ unwillingness to overtly express emotion might be a motivating factor for them to use such apps as alternative emotional outlets. Others felt that differences in usage would not be gender-related but would depend on the type of person the user is; for example, lazier or more forgetful people would use these apps less. In terms of reaction to the prototype, girls reported that they would use it if it were available; however, responses from boys were mixed. Some boys reported they would use it if they were feeling depressed, whereas others reported that it needed to be more fun or include games or they would not use it.
Young people in control
In one of the focus groups, the importance of young people being in control of how they use mental health apps was emphasised a number of times. Participants stressed that young people do not like being told what to do and that it should be their choice as to whether they use such apps; they should not be ‘forced’ to use them.
Discussion
Overall, participants responded positively to the mental health app prototype, suggesting that this type of tool is acceptable to adolescents. In relation to the use of mental health apps, safety, engagement and functionality were the most frequently occurring concerns for adolescents. Other themes such as social interaction, promoting awareness, accessibility, gender and young people in control were also identified but were mentioned less frequently. These themes provide a useful reference framework for the development of mental health mobile apps for young people.
Confidentiality was a key concern, which is in line with adolescents’ needs from mental health services in general. 23 Thus, controls over privacy settings and password protection are vital features that must be incorporated into mental health apps. Participants were also concerned about the stigma associated with using mental health apps, thus apps should be designed to be discrete and not attract attention to the user. 6
While participants reported a desire for social interaction via mental health apps, cyber-bullying was a prominent concern. Cyber-bullying is linked to increased mental health difficulties in adolescents, 24 thus a key challenge faced is incorporating social interaction into mental health apps while protecting users. This is important as social interaction via such technologies can give adolescents a sense of belonging and connection, which is important for well-being and emotional stability. 24 Previous studies have suggested technical solutions such as changing one’s username or ‘blocking’ bullies from interacting with the user are effective mechanisms for dealing with cyber-bullying; 25 however, participants in this study expressed concerns that this did not always solve the problem. Strategies such as cyber-safety education programmes or school-based cyber-bullying prevention programmes may be a means of addressing this in the future. 25
Engagement and functionality were identified as important themes, indicating that mental health apps must serve a useful, relevant purpose while simultaneously engaging adolescents’ interest. Features promoting user engagement may be particularly pertinent for boys, as findings suggest they may be less inclined to use such technologies. This is consistent with research on gender differences in engagement with online mental health interventions. 26 In line with recommendations for medical mobile apps, 27 adolescents in this study indicated that large chunks of text should be avoided and that multimedia features such as music and videos should be included to maximise user engagement. Incorporating reward systems such as unlocking games may also be a useful means of engaging adolescents with these apps. 6
Adolescents highlighted the importance of accessibility, thus mental health apps must be easy to use and affordable, if not free of cost. 24 Creating awareness was also a theme, thus developers should strive to ensure apps are well-promoted and openly discussed by young people, in order to increase their social acceptability and consequently adolescents’ engagement with them. The present findings also highlight the importance of ensuring that adolescents feel in control of how they access support for their mental health. To achieve this, young people should be involved at all stages of the app development process including, planning, design, delivery and evaluation in line with the International Declaration on Youth Mental Health recommendations. 28
Strengths and limitations
A key strength of this study was the use of focus groups, a particularly advantageous method of collecting data from adolescents. In one-to-one interview situations, young people may feel nervous and reluctant to voice personal opinions or may feel pressured to respond the way they think the researcher wants. 17 Focus groups remove much of this pressure by offering a more natural and relaxed environment, allowing for interaction and stimulation of ideas between adolescents in a peer group context.17,20 Another strength of this study was the use of two independent coders to analyse the data and a third independent researcher to conduct inter-rater reliability. This helped control for researcher bias, thus enhancing the reliability and validity of the themes identified. 29
However, some limitations should be acknowledged. First, participants were recruited from two non-fee paying, single-sex schools in the same postal code area of Dublin, neither of which was considered to be disadvantaged. Thus, generalisability of the results may be limited across location and socio-economic status. Furthermore, the opt-in method of obtaining consent may have resulted in the recruitment of adolescents who are more motivated to engage with activities and interventions related to mental health. Future studies in this area should explore a range of diverse samples so that mental health apps can be tailored for different adolescent populations according to their specific needs.
Conclusion
This research is the first phase of a larger study that aims to develop and evaluate the effectiveness of a mental health mobile app for adolescents. Findings generated insight into adolescents’ perspectives on the use of mobile apps in mental health and identified safety, engagement and functionality as key concerns. A key challenge faced by future developers of mental health mobile technologies will be negotiating the potential tension between the preferences of adolescents, and feasibility, design and development constraints. The findings of this study will provide a valuable reference point for these developers and will help ensure that such technologies are developed to be acceptable and engaging for adolescents, in order to maximise their overall reach and impact.
Footnotes
Acknowledgements
We would like to thank Mr Conall Tunney and Ms Alanna Donnelly for their assistance with data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of a PhD thesis funded by the Irish Research Council.