
Abstract
Diabetes and its sequelae cause a growing burden of morbidity and mortality. For many patients living with diabetes, the Internet is an important source of health information and support. In the course of the development of an Interactive Health Communication Application, combining evidence-based information with behavior change and decision support, we assessed the characteristics, information, and decision support needs of patients with type 2 diabetes.
The needs assessment was performed in two steps. First, we conducted semi-structured interviews with 10 patients and seven physicians. In the second step, we developed a self-assessment questionnaire based on the results of the interviews and administered it to a new and larger sample of diabetes patients (N = 178). The questionnaire comprised four main sections: (1) Internet use and Internet experience, (2) diabetes knowledge, (3) relevant decisions and decision preferences, and (4) online health information needs. Descriptive data analyses were performed.
In the questionnaire study, the patient sample was heterogeneous in terms of age, time since diagnosis, and glycemic control. (1) Most participants (61.7%) have searched the web for health information at least once. The majority (62%) of those who have used the web use it at least once per month. (2) Diabetes knowledge was scarce: Only a small percentage (1.9%) of the respondents answered all items of the knowledge questionnaire correctly. (3) The most relevant treatment decisions concerned glycemic control, oral medication, and acute complications. The most difficult treatment decision was whether to start insulin treatment. Of the respondents, 69.4 percent thought that medical decisions should be made by them and their doctor together. (4) The most important information needs concerned sequelae of diabetes, blood glucose control, and basic diabetes information.
The Internet seems to be a feasible way to reach people with type 2 diabetes. The heterogeneity of the sample, especially with respect to diabetes knowledge, makes it clear that the projected Interactive Health Communication Application should tailor the content to the individual user, taking account of individual characteristics and preferences. A wide range of topics should be covered. Special attention should be paid to the advantages and disadvantages of insulin treatment and the fears and hopes associated with it. These results were taken into account when developing the Interactive Health Communication Application that is currently being evaluated in a randomized controlled trial (International Clinical Trials Registry DRKS00003322).
Background
Diabetes is a chronic condition with a large and growing impact on the quality of life of many people and health care costs all over the world.
1
Projections expect the prevalence to rise from 2.8 percent of the world’s population in the year 2000 to 4.4 percent in 2030.
2
Type 2 diabetes accounts for 90–95 percent of diabetes cases
3
and presents a major challenge for the health care system. Patient empowerment is a key for both the individual patient and for the health care system to cope with these challenges. It is defined as
helping patients discover and develop the inherent capacity to be responsible for one’s own life. People are empowered when they have sufficient knowledge to make rational decisions, sufficient control and resources to implement their decisions, and sufficient experience to evaluate the effectiveness of their decisions. (p. 38)
4
This makes it clear that health information is one necessary part of empowerment. 5 Patients need to be informed about their disease, its potential course, and the treatment options at hand, including their advantages and disadvantages. 6 Consequently, diabetes education has long been recognized as a cornerstone of diabetes management and implemented in the Standards of Medical Care. 7 However, due to limited resources in health care, large numbers of patients still do not have access to feasible diabetes education.8,9 The Internet can be an important complementary source for health information and support for people living with diabetes. Wagner et al. 10 found that 52 percent of diabetes patients search the Internet for health information. The information they find influence treatment decisions, coping, health behavior, and decisions on whether a health professional is consulted or not. 11 Trials of systematically developed online health interventions for chronic diseases show small but consistent effects on clinical outcomes12–15 even in older populations who are generally thought to be less inclined to use the web. 16 However, the correctness, usefulness, and readability of online health information vary greatly.17–19 Systematic website development might lead to improved quality. 20
In an ongoing project, 21 we are developing an Interactive Health Communication Application (IHCA) for patients with type 2 diabetes. IHCAs are “computer-based, usually web-based, information packages for patients that combine health information with at least one of social support, decision support, or behaviour change support” (p. 1). 22 They were found to have positive effects on knowledge, social support, clinical, and behavioral outcomes. 22 Needs assessments are a crucial step in the participatory planning of such health interventions20,23 and a systematic method for identifying and prioritizing the needs of a defined target population. 24 In this study, information and decision support needs of patients with type 2 diabetes in Germany are assessed in order to inform the development of an IHCA offering information and decision support. To our knowledge, this is the first German study researching this target group with a focus on the Internet as a source for diabetes information. Existing studies on Internet use by patients with type 2 diabetes mostly describe US populations; the most comprehensive and recent surveys have been provided by the Pew Research Center.11,25 Pew reports that people living with a chronic condition in the United States have Internet access significantly less frequently than people with no chronic condition (72% vs 89%). If they do, however, the information they find online has major impact on the treatment decisions they make, whether they see a doctor or not, whether they ask their doctor new questions or get a second opinion, and the way they cope with and manage their condition. 26 Looking at diabetes specifically, there were significant differences between people living with and without diabetes (but potentially another chronic condition) with respect to the topics they looked up online: People with diabetes looked more often for information on a drug they had seen advertised or on medical test results, while they looked less for information on pregnancy and childbirth. 25
Methods
The process was led by published guidelines to needs assessments in health care.23,24 The needs assessment was performed in two steps: First, we conducted semi-structured interviews with physicians and patients in order to explore the perspectives and preferences of both groups. In the second step, we developed a self-assessment questionnaire based on the main results of the interviews and administered it to a new and larger patient sample. This two-step procedure was chosen for two reasons: First, qualitative interviews are a good method to explore a field, leaving the interviewees the freedom to bring up topics of their own. Data quality is enhanced if different sources (patients and physicians) are included. 27 Second, by developing the questionnaire from qualitative data obtained from the interviews, we aimed to develop an instrument covering all relevant topics and assessing quantitative data that can serve as a basis for the projected IHCA. The study was approved by the Ethics Committee of the Medical Council of Hamburg (Process number: PV3412).
Preliminary qualitative interviews and questionnaire development
The aim of the interviews was to gain insight into the views of patients with type 2 diabetes and their physicians on information needs, sources used for diabetes information, medical decisions in the management of type 2 diabetes, and the role of the Internet in the search for health information and support. The interviews were semi-structured one-hour face-to-face interviews conducted by two doctoral medical students. In order to leave room for all topics relevant to the interviewees, open-ended questions were used and interviewees were invited to introduce issues that were not originally covered by the interviews. Table 1 displays the questions posed by the interviewers. The interviews were recorded and transcribed.
Interview with physicians and patients.
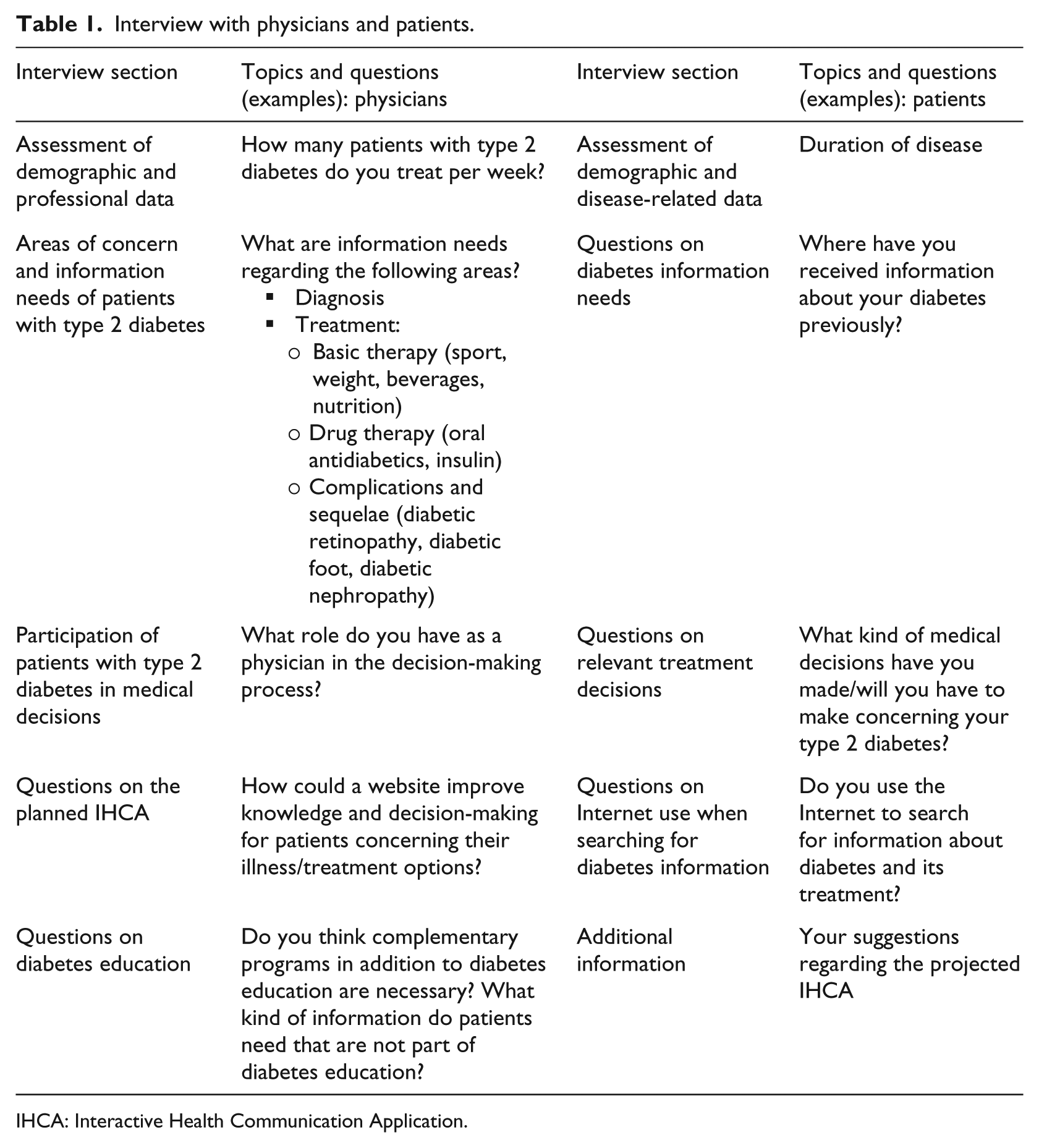
IHCA: Interactive Health Communication Application.
Interviewees were a convenience sample recruited from the diabetes polyclinic of the University Hospital Hamburg-Eppendorf and pre-existing cooperation with practices. For the analysis, we used conventional content analysis 28 or inductive category development. 29 In a first step, we read the transcripts of the interviews. We developed response categories for each question. In a next step, we counted the number of responses that fell into each category. Each category that was mentioned by more than one interviewee was transformed into an item or response option in the questionnaire study.
Patient interview results
In total, 10 patients were interviewed. They were mostly male (9 out of 10 patients), had a mean age of 62 years (range: 48–83 years), and covered the whole educational range from 9 years of schooling to a university degree (3 patients, respectively). On the average, they had been diagnosed with diabetes 8.6 years ago (range: 3–22 years). The treatment the respondents received following diagnosis ranged from insulin treatment (2 respondents) to the recommendation to change their diet (2 respondents). Only one interviewee reported having received a structured diabetes education and extensive counseling on diabetes right after the diagnosis. At the time of the interview, six respondents received insulin treatment, and nine were on oral medication. One respondent received no medication at all. The participants’ current A1C was 6.9 at mean, ranging from 5.5 to 8.3.
For most patients, their physician is the most important source of information and support. All interviewed patients use complementary sources of information (press, pharmacist, Internet, friends with diabetes, television (TV)) if they do not understand, agree with, or are not satisfied with the information provided by their physician. Patients reported that the most difficult decision in diabetes treatment is whether to start insulin treatment or not. Reasons why this decision was regarded as especially difficult were fear (of weight gain, of reduced life expectancy, of stigmatization, of not being “normal” any more, of depending on insulin shots for the rest of one’s life), the subjective feeling of not being ill, and not understanding the information provided. Seven patients felt that their physicians made this treatment decision for them. Two said their physicians had provided them with information and advice so they could make the decision. One said the decision had been shared between him and his physician. Accordingly, seven patients reported not having been informed about treatment alternatives when deciding on insulin treatment. Three said oral antidiabetics, different kinds of insulin, or combining insulin and oral antidiabetics had been presented to them as an alternative. All patients said they would generally like to share decisions with their physicians, and to be able to do this, they needed more recent and understandable information on diabetes, on treatment options, and their risks and benefits. Patients desire the projected IHCA to provide sophisticated and correct, understandable, and individual education.
Physician interview results
Of the seven physicians interviewed, three were female. They were 60 years old at mean. All were internists; two of them had specialized in diabetology. One worked as a general practitioner. Five had their own practice, and two worked in a diabetes polyclinic in the University Hospital Hamburg-Eppendorf.
The physicians agreed with the patients that the most difficult decision in diabetes treatment is whether to start insulin treatment or not. Perceived reasons for the difficulty were that patients were overstrained by the amount of information given to them on insulin therapy, that they were not sufficiently motivated for the lifestyle changes that should accompany insulin treatment, and that patients got wrong information from the pharmaceutical industry. As remedies they suggested independent, profound, understandable patient information; individual patient education; and making it clear to patients that they are responsible for a good part of their diabetes management.
The physicians also agreed with the patients that they mostly made the treatment decisions for them. Physicians said this was necessary due to lacking and misleading information on the patients’ side. Consequently, they suggested informing patients about insulin treatment, especially the aspects that frighten patients, and generally fostering health literacy (HL) as steps toward more patient-centered decision-making. While patients feel uncomfortable with the amount of responsibility given to them by their physicians for their disease and its treatment, the physicians would like their patients to take more responsibility. Like the patients, the physicians too desire the projected IHCA to provide sophisticated and correct, understandable, and individually tailored education and so disburden the consultation.
Questionnaire study
Data collection
The questionnaire study aimed at quantifying the patients’ perspective and identifying relevant content for the projected IHCA. Items on diabetes knowledge were added in order to become acquainted with the target group. The resulting questionnaire comprised four main sections: (1) Internet use and Internet experience, (2) diabetes knowledge, (3) relevant decisions and decision preferences, and (4) online health information needs.
In contrast to the interviews, closed-ended questions offering between 2 and 10 response options were used. Where feasible, multiple responses were possible. Internet use was assessed using the following questions: Have you ever searched for diabetes information on the Internet (yes/no format)? When was the last time (<3 months, 3–12 months, >12 months)? How often have you searched the Internet for diabetes information during the last 3 months (5 response options ranging from “(almost) daily” to “never”)? Why did you decide to use the Internet (4 options including the option for a free answer)? Which kind of diabetes information have you looked for (10 options including the option for a free answer)? Participants were then asked to evaluate the usefulness of their online searches using 13 items (e.g. “The diabetes information on the Internet was credible.”) on a 5-point Likert scale. Diabetes knowledge was measured with six true/false items assessing knowledge on fasting blood sugar, A1C, insulin treatment, diet, sequelae, and hypoglycemia. With respect to decision-making and information needs, a scale adapted from Man-Son-Hing et al. 30 assessed the extent to which a participant wishes to participate in medical decision-making. Relevant decisions were identified asking in which of seven decision areas (e.g. oral antidiabetics) a treatment decision had to be made during the last 2 years (yes/no response format). Finally, participants were asked to rate the importance of 14 topics on a diabetes website using a 4-point scale ranging from 1 (very important) to 4 (very unimportant).
In addition, participant characteristics such as demographics and HL were assessed. HL as defined by Ishikawa et al. 31 is “the capacity of individuals to access, understand, and use health information to make informed and appropriate health-related decisions” (p. 874). The authors developed an instrument (HL Scales) measuring the three subscales functional HL, communicative HL, and critical HL in patients with type 2 diabetes. A total HL score can be formed. The subdomains are defined as follows: 32 Functional or basic HL means having “sufficient basic skills in reading and writing to be able to function effectively in everyday situations” (p. 263). Communicative or interactive HL comprises “more advanced cognitive and literacy skills which, together with social skills, can be used to actively participate in everyday activities, to extract information and derive meaning from different forms of communication, and to apply new information to changing circumstances” (pp. 263f.). Critical HL is defined as “more advanced cognitive skills which, together with social skills, can be applied to critically analyze information, and to use this information to exert greater control over life events and situations” (p. 264). There is no suggested hierarchy or structure among the three subscales. The instrument contains five items for functional and communicative HL, respectively, and four items for critical HL. Each item is rated on a 4-point scale. Construct validity and internal consistency of the three scales (functional HL: α = 0.84, communicative HL: α = 0.77, critical HL: α = 0.65) are satisfactory. 31 The questionnaire was available in a paper-and-pencil format and an online format using QuestBack Survey Software. 33 Patients could choose which format they preferred to answer.
Participants
The patient sample for the questionnaire study was again recruited via the pathways described above. In addition, we searched the Internet for diabetes self-help groups. To those groups that had an email address on the website, we mailed a request for cooperation, a link to the online questionnaire, and the offer to provide paper-and-pencil questionnaires. We asked relevant German diabetes self-help associations, for example, Deutscher Diabetiker Bund (DDB) and diabeteDE, whether they were willing to place a short invitation and the link to our online questionnaire on their websites.
Data analysis
Descriptive data analysis (M, standard deviation (SD), min/max, %) and Pearson’s correlations were performed using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA).
Results
Sample characteristics
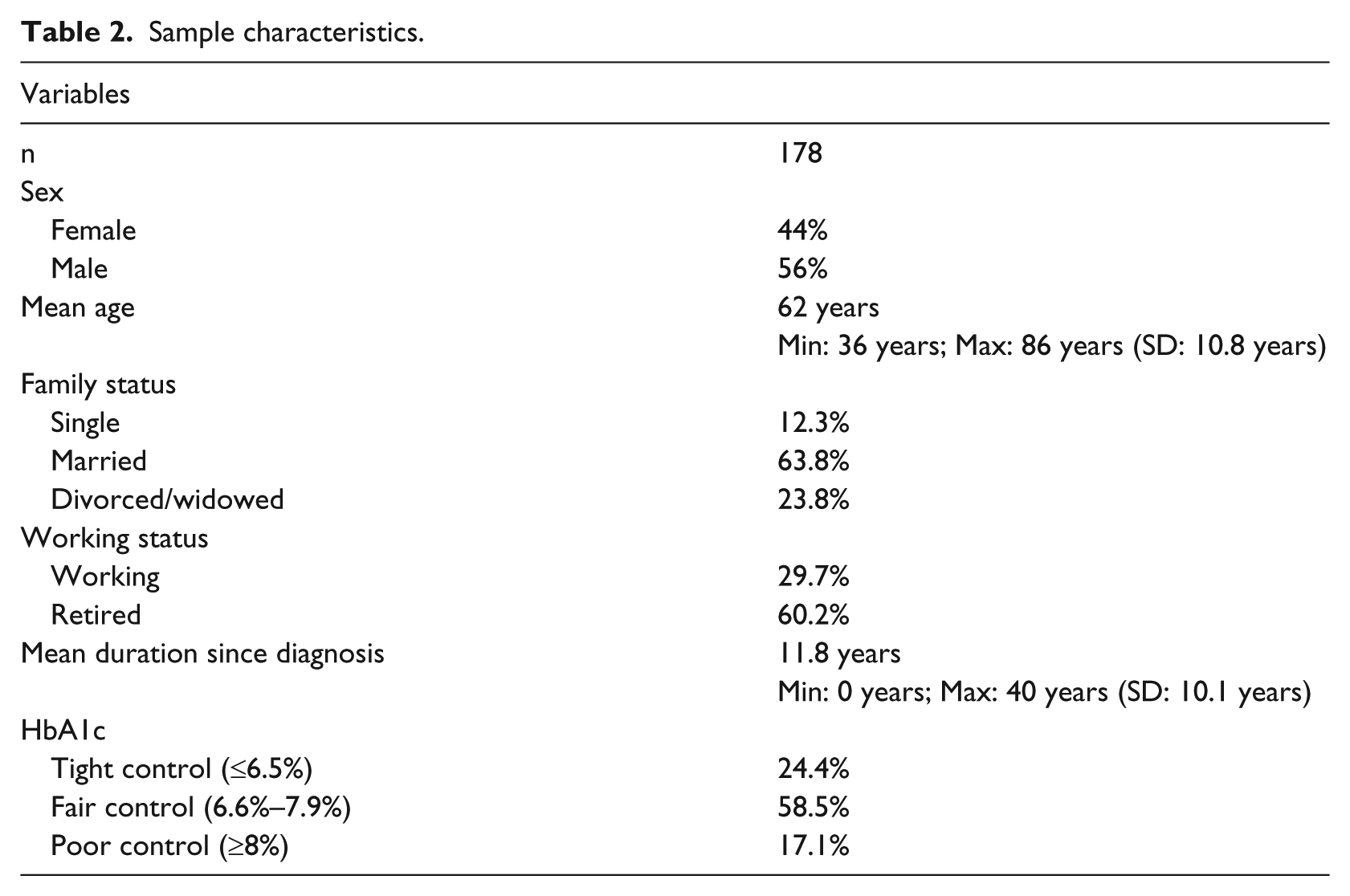
In total, 178 patients with type 2 diabetes completed the questionnaire. The sample characteristics are displayed in Table 2. Of the participants, 41 percent were treated with insulin, 52.7 percent were on oral medication, 18.2 percent combined both, and 5.5 percent reported taking neither insulin nor oral medication. The overall HL was fairly good (M = 2.8, SD = 0.4), and the sample was quite heterogeneous with HL scores ranging from 1.6 to the maximum score of 4. The scores on all three subscales ranged from 1.0 to 4.0, covering the whole range of possible scores. Communicative HL had was highest (M = 3.2, SD = 0.6), followed by critical (M = 2.9, SD = 0.7) and functional HL (M = 2.4, SD = 0.7).
Sample characteristics.
Internet use
Of the participants, 61.7 percent reported having looked for health information online. Of the respondents who reported never having looked for health information online, 35.1 percent said they did not have Internet access, 31.5 percent said they preferred asking their doctor for information on health and diseases, 15.8 percent said they were not used to using the Internet, and 8.8 percent reported having no trust in the Internet as a source for this kind of information. Of the respondents who reported having looked for health information online, 68.5 percent had performed their last search less than 3 months ago. The majority of respondents (62%) said they searched the web for diabetes information at least once a month. A significant proportion of respondents reported some difficulties with online search: 48.5 percent judged the information they found to be of low quality, 32.4 percent found it not credible, 25.8 percent said the information was too extensive, and 47.9 percent reported difficulties of comprehension (see Figure 1). When asked for the reasons why they used the web for diabetes information, 28.2 percent said the information they received from their physicians was not sufficient and 11.7 percent said that the information they received from their physicians was too hard to understand or that they did not agree with them. The most frequently searched topics were general information on diabetes, diet and exercise (42.7%, respectively), treatment options (39.8%), sequelae (34%), self-help groups and patient forums (32%), risks and side effects of specific treatment options (30.1%), and acute complications (24.3%).
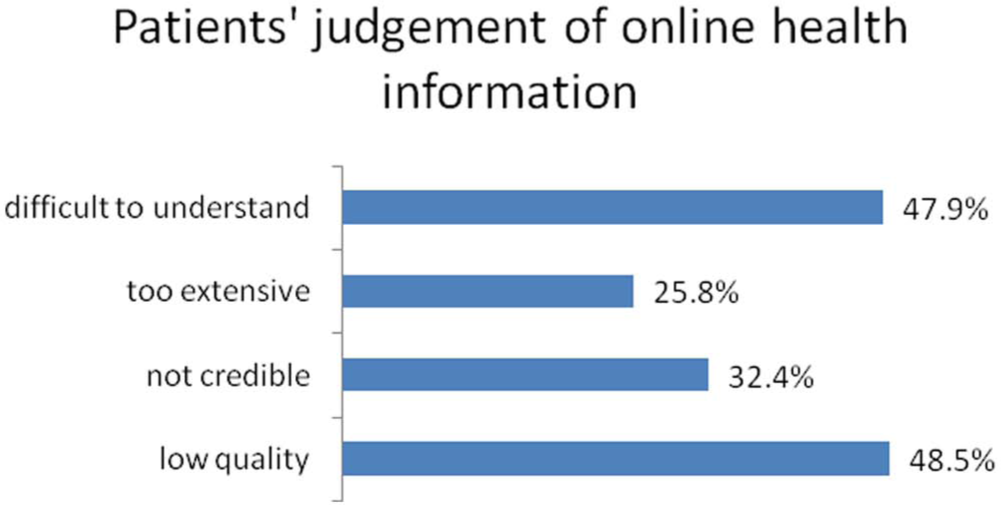
How do you evaluate the health information you found online?
Diabetes knowledge
Only two (1.9%) of the respondents answered all six items assessing diabetes knowledge correctly. One respondent (1%) had only one correct answer. Especially difficult was the item asking for the optimal fasting blood glucose (answered correctly by 9.2%), while “A healthy diabetes diet is …” was the easiest item (answered correctly by 95.8%).
Decision-making needs
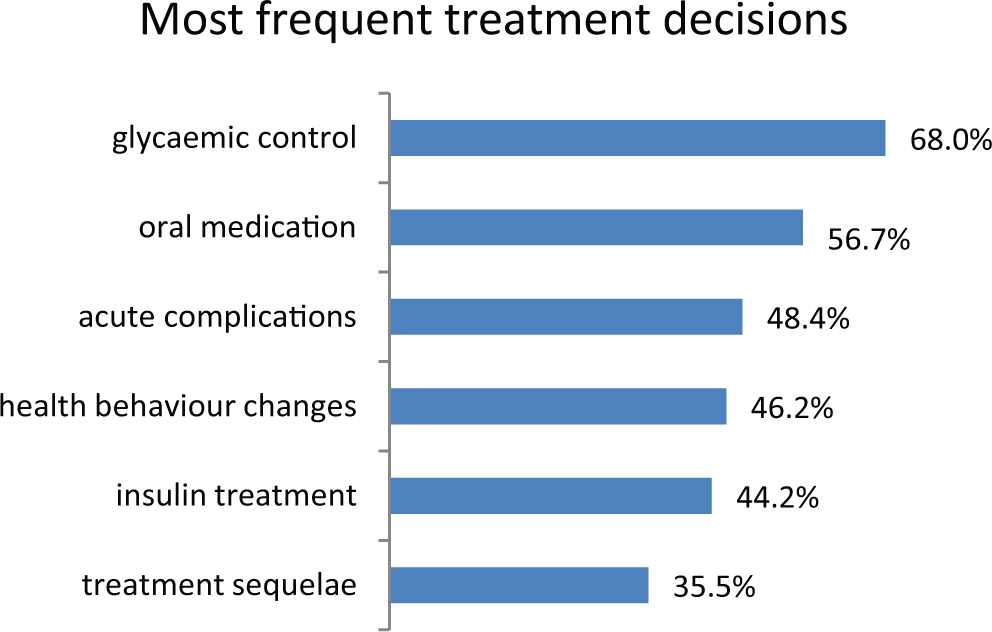
Most respondents thought that medical decisions should be made by them and their doctor together (69.4%, see Figure 2). Among the most frequent treatment decisions respondents and their doctors made during the last 2 years were decisions concerning glycemic control (68%), oral medication (56.7%), acute complications (48.4%), health behavior changes (46.2%), insulin treatment (44.2%), and treatment of sequelae (35.5%, see Figure 3).
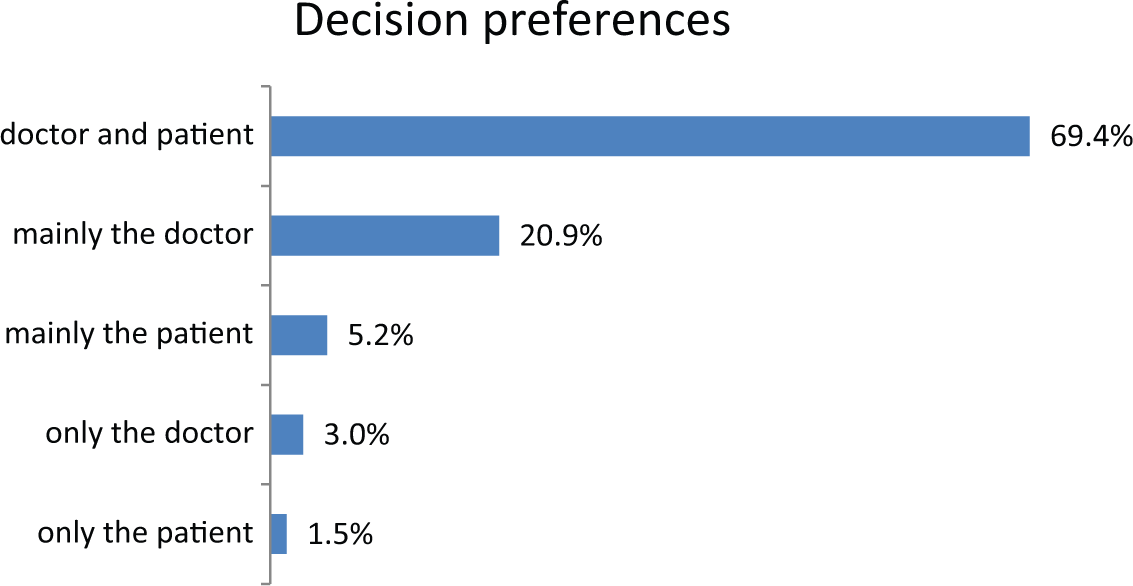
Who should generally make medical decisions regarding your condition?
Did you or your doctor have to make a decision on the following options?
Health information needs
Almost every topic that was offered in the questionnaire was rated “very important” by more than half of the interviewees. The topic that was considered very important by the biggest proportion of participants was sequelae of diabetes, followed by blood glucose control, basic information on diabetes, effectiveness of treatment options, and risks and side effects of treatment options. The topic that was considered least important was combination therapy (see Figure 4).
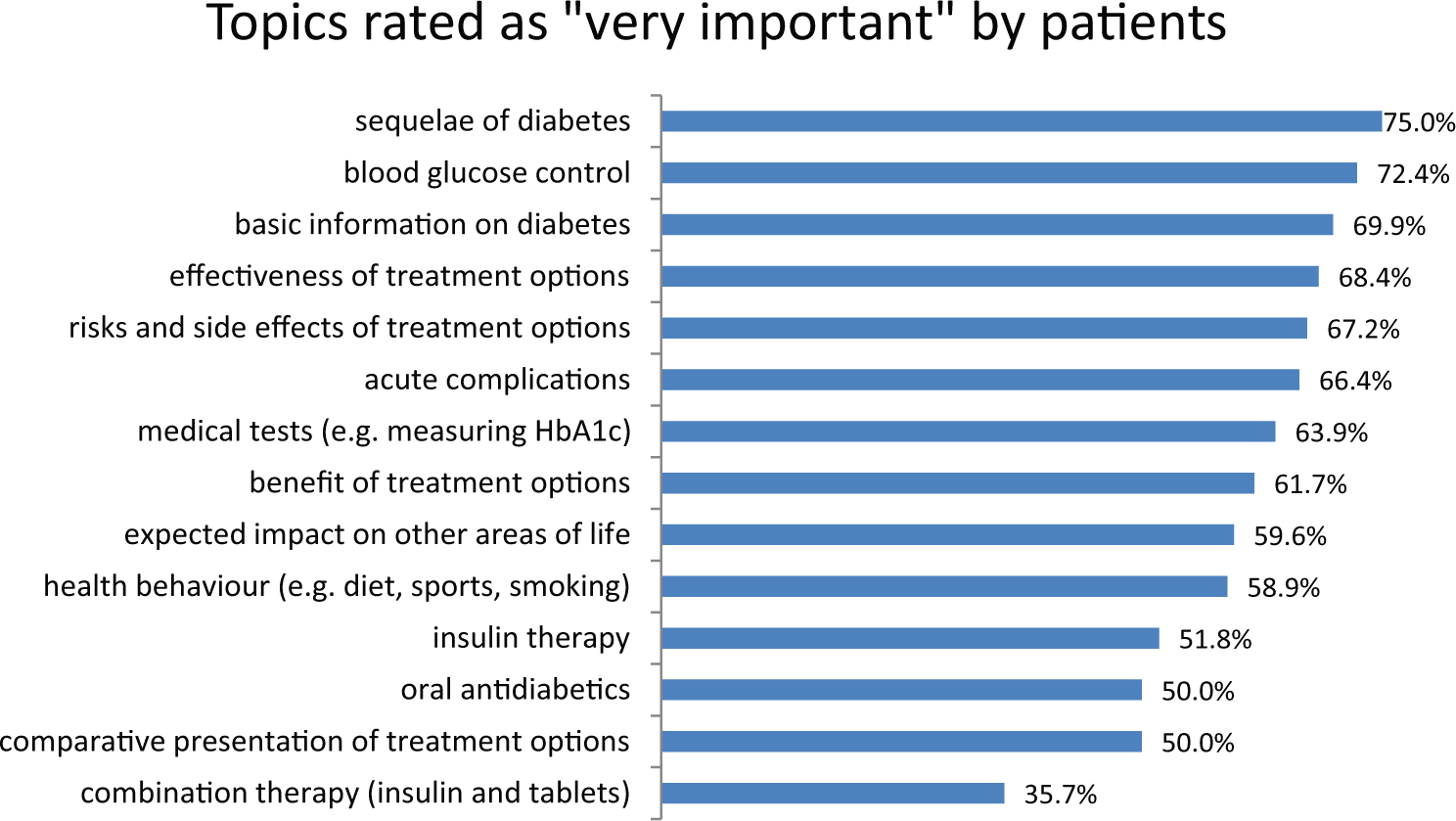
How important are the following topics for you on a diabetes website?
Subgroup analysis
Since the prevalence of type 2 diabetes increases with age, while international and German studies found that Internet use declines with age,34–36 we examined whether Internet use and satisfaction with Internet use are correlated with age in this sample. Another relevant moderator could be HL. It has been reported that reading levels of online patient materials are often too high for the average user, 37 which might lead to lower Internet use in people with lower HL. 38
Age, Internet use, and satisfaction with Internet use
For further descriptive analysis, we split the sample into three age groups (<55 years, 55–69 years, ≥70 years). In total, 54 participants (30.3%) were younger than 55 years, 27 (15.2%) were aged between 55 and 69 years, and 31 (17.4%) were aged 70 years or older. And 66 participants (37.1%) did not report their age. Looking at frequency of Internet use in these three groups, we found that 55.1 percent of the youngest group had ever searched for diabetes information online, 57.7 percent of the group between 55 and 69 years, and 40.9 percent of the oldest group. The fact that these numbers are all lower than the overall Internet adoption in our sample (61.7%) suggests that there are systematic missings.
There was no significant correlation (r = −1.4, p = 0.16) between age and Internet adoption (“Have you ever looked for diabetes information online?”). Pearson’s correlation between age and satisfaction with Internet use (“How was the overall usefulness of your online search for diabetes information?”) was also not significant (r = −0.06, p = 0.64).
HL, Internet use, and satisfaction with Internet use
For further descriptive analysis, we split the sample into two groups (median split: HL ≤ 2.8, HL > 2.8). In all, 68 participants (38.2%) had an overall HL of 2.8 or lower and 72 participants (40.4%) had a HL higher than 2.8. The HL score was missing for 38 participants (21.3%). Looking at frequency of Internet use in these two groups, we found that 55.7% of the lower HL group and 57.8% of the higher HL group had ever searched for diabetes information online. Again, the fact that these numbers are all lower than the overall Internet adoption in our sample (61.7%) suggests that there are systematic missings.
There was no significant correlation (r = −0.01, p = 0.25) between overall HL and Internet use. HL and satisfaction with Internet use were negatively and significantly correlated (r = −0.24, p = 0.03).
Discussion
This study is the first needs assessment among patients with type 2 diabetes in Germany, focusing on the Internet as a source for diabetes information. In order to develop an IHCA that meets the specific needs of patients with type 2 diabetes, we undertook a cross-sectional assessment in two steps, conducting interviews with patients and physicians and deepening our understanding of the patients’ view in a questionnaire study.
The majority of participants have used the web when searching for health information. Of these, the majority performs diabetes-related searches at least once a month on a wide variety of topics. Still, the Internet adoption rate of 61.7 percent found in our sample is relatively small compared to the German general population: A 2013 representative survey of Internet adoption found that 77.2 percent of the population aged 18 years and older used the web. 36 This difference might be due to the fact that we did not ask for Internet adoption itself but for searching the Internet for health information. It is possible that some participants do use the web but not for health purposes. As an orientation, the Pew Internet & American Life Project found that 86 percent of the chronically ill who do use the web at all also use it for health purposes. The authors also report that less people living with a chronic condition go online (51%) than do those without a chronic condition (74%) in the United States and that this is due to higher age and lower educational status in the chronically ill subgroup, as well as to being chronically ill itself. 26 These factors might also contribute to the low Internet adoption rate in our sample compared to the general population.
Looking at the older age groups, we found higher adoption rates in our sample than in the general population. Even though the increase in Internet adoption over the last years is mostly due to the age group over 50 years, older Germans still are not avid Internet users: while 82.7 percent of those between 50 and 59 years of age reported being online, only 42.9 percent of those aged 60 years or older and 30.4 percent of those over 70 years of age have ever used the web. 36 In our sample, 40.9 percent of those over 70 years of age have searched the web for diabetes information. This gap might be due to a bias in our sample: It is possible that those who are willing and interested in taking part in a scientific study are also more interested in new technologies. This might also explain why we, in contrast to prior national and international studies,34–36 did not find a significant correlation between age and Internet use or age and satisfaction with Internet use.
Neither did we find a correlation between HL and Internet adoption, even though the literature suggests that reading levels of online health information are often too high for users with lower HL.39–41 As Schulz and Nakamoto 42 suggest in their recent article, lower HL might not lead to less Internet use but to more misunderstandings and dangers related to wrong or biased information found online. This concern was also uttered by the physicians in our interviews. Schulz and Nakamoto claim that patients, especially those with lower HL, need guidance from their health professionals when using the Internet for health purposes. Our finding that HL is negatively correlated with satisfaction with Internet use might thus reflect the capability of more health-literate patients to critically reflect on the information they find. Further research should explore Internet adoption as well as use and understanding of health information found online in patients with different levels of HL.
In summary, the Internet can be regarded as a feasible supplementary medium to provide patients with type 2 diabetes in Germany with information and support, but its low adoption rate emphasizes the need to maintain traditional sources of information. In our sample, both patients and physicians would welcome the development of evidence-based, readable online diabetes information. The wide range of diabetes knowledge found in the sample should be addressed by the IHCA. Both patients and physicians said that not understanding the information provided or a lack of knowledge is among the most important reasons why medical decisions are difficult to make. Knowledge gaps result in anxiety (in some cases, even unnecessary fears like being afraid of a loss-of-life expectancy if starting insulin treatment) and helplessness on the patients’ side. The most important topics when it comes to information needs and treatment decisions are basic diabetes information, lifestyle topics, treatment options, sequelae, and self-help. These content areas should be covered by the IHCA. While the questionnaire study shows that starting insulin treatment is not among the most frequent decisions that patients with type 2 diabetes have to make, it was pointed out as the hardest decision by patients and physicians in the interviews. The decision on insulin treatment should, therefore, receive special attention.
The vast majority of respondents wish to share the decision with their physicians. Both patients and physicians state that this is not yet reality: usually the physicians make decisions. This finding corresponds to the literature.43,44 In our study, knowledge gaps and communication problems (too little time, information not understandable) between patient and physician are named as the main reasons why decisions are not shared. This, too, corresponds to findings reported in the literature. Time pressure and communication problems like the absence of a shared understanding of the disease are named as key impediments to shared decision-making on the physicians’ side, while low HL, fear, and denial are barriers on the patients’ side.45–48 Throughout the IHCA, patients should be encouraged to share the information and support they received from the IHCA with their physician and use the IHCA as a preparation for consultations and shared decision-making.
There are some limitations to the work presented. Since we worked with convenience samples, we cannot know whether the results of our needs assessment are representative for the population of people with type 2 diabetes in Germany. When compared to data from other studies,49–51 we found similar results with respect to age, gender, treatment, and glycemic control. To our knowledge, there are no data available on HL, health locus of control, or diabetes knowledge of people with type 2 diabetes in Germany. Additionally, it might have broadened our perspective if we had interviewed not only patients and physicians but also caregivers of diabetes patients and diabetes educators. With regard to the target group of the IHCA, we also could have included caregivers who are even more actively searching the web for health information than the patients themselves.11,52 Moreover, the measurements we used were only partly standardized and partly developed or adapted for our purposes. Strengths of the study are the inclusion of qualitative and quantitative data from two sources (patients and physicians) as well as the broad range of data assessed.
Sample characteristics as well as the concerns expressed by the patients and physicians in this study are consistent with findings in the international literature. This confirms that the data obtained are a valid base for the development of an IHCA. Needs regarding content and structure could clearly be identified. Within a randomized controlled trial, we are currently evaluating the IHCA we developed based on the needs assessment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Ministry of Education and Research (grant number 01GX0710).