
Abstract
Our interest here is with the ‘marriage’ of e-patient information systems with care pathways in order to deliver integrated care. We report on the development and implementation of four such pathways within two National Health Service primary care trusts in England: (a) frail elderly care, (b) stroke care, (c) diabetic retinopathy screening and (d) intermediate care. The pathways were selected because each represents a different type of information and data ‘couplings’, in terms of task interdependency with some pathways/systems reflecting more complex coordinating patterns than others. Our aim here is identify and explain how health professionals and information specialists in two organisational National Health Service primary care trusts organisationally construct and use such systems and, in particular, the implications this has for issues of professional and managerial control and autonomy. The article is informed by an institutionalist analysis.
Introduction
This article examines the challenges of e-patient information systems’ support for care pathways drawing on research carried out within two English local health-care communities, or networks. Specifically, we report on how health professionals and information specialists within two National Health Service (NHS) primary care trusts (PCTs) implemented and utilised information technology (IT)–supported care pathways (e-care pathways). There is an intriguing aspect to care pathways: that is, they represent two contesting control systems. On the one hand, they reflect occupational control being a professionally (nurse)-led system to improve quality of care and to reinforce nursing jurisdiction. 1 On the other hand, however, they also embody managerial control in the form of a strategy to re-engineer the organisation and deliver good quality care more efficiently. The context for the growth of IT-supported care pathways within the English NHS is that of providing health-care services at a time of austerity, 2 exacerbating the already challenging secular trends: (a) ageing populations, (b) rising costs of health technologies and (c) rising patient and public expectations. 3 The Organisation for Economic Co-operation and Development (OECD) projects that public health-care spending could increase by 3.5–6 per cent of gross domestic product (GDP) by 2050 across OECD countries. 4
The NHS has changed from a ‘command and control’ organisation 5 to more like a tax-funded Health Maintenance Organisation (HMO) with elements of market competition.6,7 This context is important as care pathways are the product of an HMO rationale. 6 Our focus here is on the day-to-day realities of implementing and working with e-care pathways.
The article is in four sections. We start with an account of care pathways, their development, the role of IT and the implications for managerial and interprofessional interdependencies. This is in order to provide the context to the two case studies: Walsall and Northant’s local health networks, preceded by details of our research methods. We then examine the four e-care pathways, focusing on the following: (a) the crossing organisational boundaries, (b) nurse hybrids and (c) ‘progress chasing’; these we identified from the field research as crucial elements to the effective implementation of various e-care pathways. We close with the discussion and conclusion.
Care pathways + IT = integrated care?
Care pathways were first developed in the New England Medical Centre, Boston, 8 and were introduced in the United States to support managed care organisations control escalating costs 9 and as a response to the pressure from health-care insurers. 10 Care pathways fit well with the rationale embedded in the White Paper The New NHS, Modern and Dependable 11 that asserts the ‘new’ NHS would be organised according to the principles of ‘integrated care, based on partnership and driven by performance’. It is hardly surprising, therefore, that care pathways are becoming the dominant mode of NHS organisation, dictating the relations between hospitals, general practice and community care.
Care pathways go under a number of different names
12
(p. 80), but the most commonly used and which describes best the intent of the technology is ‘Integrated Care Pathways’ (ICPs).
12
They are ‘multidisciplinary care management tools, which map out chronologically key activities in a healthcare process’
9
(p. 354). But they are much more than that, for they also have roots in the rationale of audit society:
13
They are simultaneously a work flow system and a record of care. Unlike [clinical] guidelines, pathways specify the activities to be accomplished and require documentation to indicate compliance or non-compliance with the planned trajectory of care.
9
(p. 354)
ICPs originated as tools for managing nursing care, 14 and as a consequence, nurses have gained jurisdiction over their development. ICPs, however, are clever and complex instruments; 15 they bring together health professionals, management and – in principle – the patients, in the coordination of care. This is done in ways that permit the auditing of the professionals’ effectiveness and efficiency. At the same time, ICPs are premised on evidence-based medicine and practice, incorporating clinical guidelines within the overall trajectory of care, 16 which makes it difficult for health professionals to disregard them.
This is not to assume that ICPs have been without their critics. Goodwin et al., 17 for example, have pointed out that ICP development has been ‘problematic and effectiveness unproven’, and other researchers have observed that ICPs take time to become embedded being very context-specific.18–20 This evidence, one should note, is drawn solely from the hospital sector, and not from primary and community care as reported on here. Another point that requires noting is that ICPs as workflow systems do not necessarily need e-health systems, but they are recognised as a particularly useful approach to the design and implementation of e-care pathways (eICPs).
Theories and methods
We undertook a longitudinal, socio-technical, qualitative evaluation of a range of e-patient information systems within two PCTs and the local health networks of which they are part (e.g. acute hospitals, social care, private care homes). This process included mapping pathways, interviewing IT and health professionals (20 interviews in Northants and 24 in Walsall), observing eICP development meetings over several months and undertaking documentary analysis. We will first explain the selection of the two PCTs and then that of the eICPs.
The case studies
Walsall and Northants local health networks are situated in the English midlands, with Walsall being about 60 miles west of Northants. They were selected because of their contrasting demographic and urban/rural mix: Walsall is a ‘Black Country’ town shaped by its industrial past in mining and steel, ethnic diversity and recent economic deprivation; its unemployment figures are nearly 6 per cent higher than in Northants. 21 Northants was less obviously urban or multi-ethnic and historically had a much more rural economy. Another reason for the choice of PCTs was the combination of (a) cultures within the two PCTs, (b) the different strategies of their informatics services (IT departments) and (c) their relations with users.
Northants and Walsall local health networks reflected different institutional logics: ‘belief systems and related practices that predominate in an organizational field’
22
(p. 139). Logics, as Reay and Hinings
23
(p. 629) point out, ‘help to explain connections that create a sense of common purpose and unity within an organizational field’ and help explain the difference between them. Where one draws the boundaries around such a ‘field’ will depend on the level of analysis. Here we are comparing two local health networks that comprised of a network of organisations and agencies, which were primarily but not solely coordinated from within the two PCTs. This approach corresponds with that of Scott
24
(pp. 207–208; cited in Reay and Hinings
23
(p. 353)): The notion of field connotes the existence of a community of organizations that partakes of a common meaning system and whose participants interact more frequently and fatefully with one another than with actors outside of the field.
The ‘logics’ of the two local health networks produced different scripts 25 for the adaption and implementation of eICPs – one, as we will show, was more management led, the other more occupationally controlled 26 (p. 40). Institutional logics do not come into being fully formed, but evolve and adapt 22 (p. 353) for reasons that are related to their history, best explained in terms of path dependency. 27
Organisational path dependencies
Schreyögg and Sydow 27 have recently argued for the application of path dependency theory to organisations, although it is better known for its application to the analysis of health systems 28 and policy analysis.29,30 It is a theory that emphasises inertia and resistance to change, but it also focuses attention on those critical junctures that force organisations to change. These processes are institutionalised 31 through self-reinforcing mechanisms that read like a positive gloss on ICPs (and eICPs): (a) improved coordination, (b) synergies (‘complementarity effects’), (c) learning leading to efficiency and (d) preference (‘adaptive expectation’). 27
eICPs and interdependencies
Institutional logics shape organisational fields in ways that reflect their path dependency, but these are insufficient for analysing the dynamics of eICPs. Here, we adopted Thompson’s 32 task interdependency model. This classic contingency approach continues to be influential within systems thinking (see Van Fenema et al. 33 ) and works well when applied to care pathways (Figure 1).
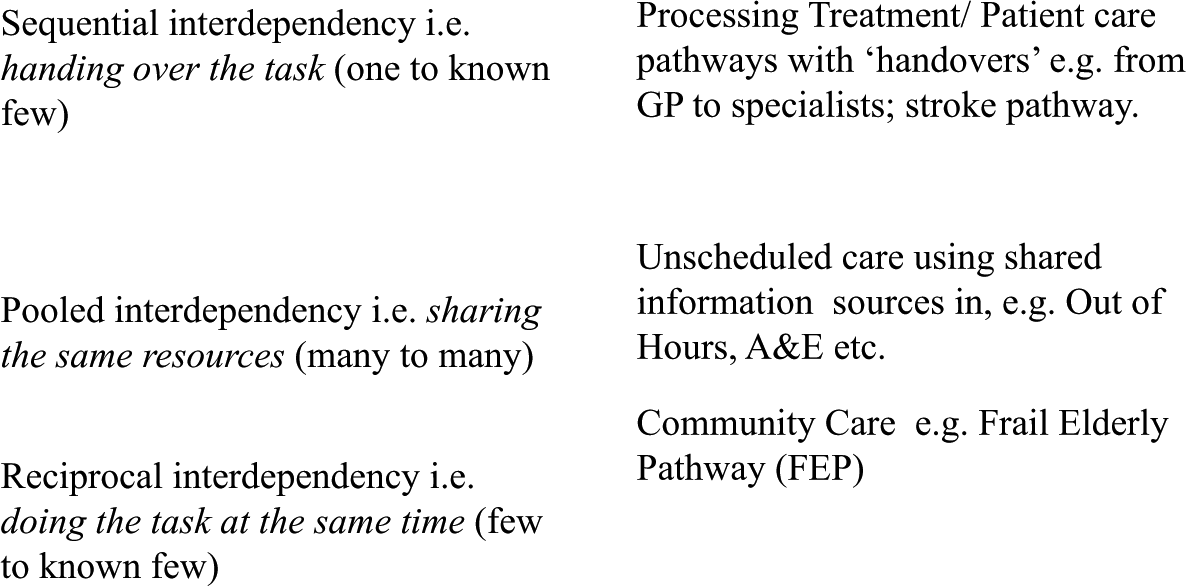
Task interdependency and care pathways.
The approach has some limitations in that it only deals with single functional correspondences, whereas care pathways usually exhibit a mix of ‘task interdependencies’. Even so, one ‘interdependency’ will normally be dominant. The typology is a useful way of identifying crucial characteristics of different systems and effectively differentiating between the relatively simple to the more complex processes. Moreover, it sits well within our broader institutionalist framework (Thompson’s contingency theory directly influenced the construction of new institutionalism 34 ).
The research reported here is based on six care pathways selected according to the following criteria:
characterised by each of the three types of task interdependencies;
crossed a range of organisational boundaries internal and external to the PCT;
originated within both Walsall and Northants PCTs;
in the process of being implemented at the time of the fieldwork.
Based on these criteria, and in discussion with local informatics staff, we selected six e-care pathways, although we will only report on four here: frail elderly care (Walsall), stroke care (Walsall), diabetic retinopathy screening (Northants) and intermediate care (Northants).
We have omitted ‘Unscheduled Care’ for both Northants and Walsall for reasons of space, and we can achieve our aims without its inclusion (see Eason et al. 35 ).
Experience of eICPs
We will focus on three key themes, which are crucial to the success or failure of eICPs and are themselves inter-related. These deal with the social, or organisational, aspects of the socio-technical e-care system rather than the technical aspects. The first, and most critical, are organisational boundaries, widely recognised as major challenge to delivering integrated care with e-health systems. 36 It was also the central focus of the research project upon which this article is based. The second theme we will explore deals with the challenge posed by information not crossing boundaries easily and reliably. One response has been the creation of hybrid roles, typically filled by nurses (or ex-nurses) with systems experience. Their work is important in reducing the limitations of the eICPs at the boundaries. Then, in order to ensure the smooth running of some eICPs, a further level of boundary spanning activity is required, one more focused on keeping track on patients should they be separated from their e-care records. This is a role carried out by ‘progress chasers’ whose job it is to unblock any blockages in the system. All three themes are at play when trying to get eICPs to work effectively within the community as we show.
Organisational boundaries
The stroke and frail elderly pathways (FEP) in Walsall were confronted with one big organisational boundary problem: that of getting the NHS and Social Services systems to ‘talk to one another’ as the two organisations used different computer and coding systems,
The NHS staff used portal system known as Fusion (see also Eason and Waterson
37
), while the Social Services employed a system that was called ‘Paris’. There were attempts made to link the two systems up sufficiently so that the health and social care could be better integrated. As an informatics manager (2010) explained, We would give them access to Fusion through the secure link, and that was the plan … and the only problem with that is that all of health information is based on a unique identifier of both NHS numbers and hospital numbers.
Paris is not based on NHS numbers or coding and hence the problem. There have been attempts more recently to integrate the two systems electronically, but for day-to-day purposes the staff found their own ways to work around the lack of integration between the two systems. As one care coordinator (2011) explained, We don’t have access to Paris, which is the social care system. But how we get around that is we ask social workers to fax the information or email the information to us.
Elsewhere, in the nearby social work building, one finds systems integration achieved even more directly: Social workers, nurses, OT’s and physio’s [are] all based within one room so the information is passed from one to another … [across the boundary via notes for manual re-entry on the other system. PCs] are on every desktop in there, so they can ‘pull them’ [i.e. directly pass the information] from one to the other. (Advanced Nurse Practitioner (ANP) 2011)
There are also many boundaries within the NHS which challenge e-care pathways, for example, between hospital and the community. In the case of stroke care at Walsall, the eICP was unable to electronically cross between the two organisations (see also Eason and Waterson
37
). To achieve the boundary crossing, we were to learn from a conversation with one of the community stroke nurses, while at a Stroke Pathway Scoping day (fieldnotes, June 2011), the nurses relied on oral, face-to-face communication: an interdisciplinary ‘handover’ meeting between community and hospital staff, with the patient, in the hospital. This was, in part, because such direct contact is seen as important to good quality care, but it was also necessary because of the lack of cross-boundary patient information, for there are issues around the level of information that the patient comes out of hospital [with] and the quality of that information. (Stroke Coordinator 2010)
Within the community, the stroke rehabilitation team recorded the patient data and information within a paper-based single assessment process (SAP) document. This was kept at the patient’s home, data which were later entered onto both the community care patient information system and stroke pathway (to provide data for the key performance indicators (KPIs)), but this was long after it had any relevance for the work of the nurses (see also Eason and Waterson 37 ).
In Northants, the challenge of boundary crossing was intended to be overcome with SystmOne, a clinical database system supported by the National Programme for Information Technology (NPfIT) that has been widely deployed in primary care 35 (paras 3 and 4.3.2). NPfIT was the overarching IT strategy within the NHS between 1998 and 2011, 35 and on the face of it, provided a good rationale for the PCT to follow. When patients entered a pathway, a SystmOne record was created to be shared by all involved; for example, the Intermediate Care team – with permission of the patient and the team – would share the record with other community staff and with the general practitioners (GPs) using SystmOne. This would have been fine if all parties involved used the same system, but they did not. Only a minority of the GPs did so (most preferred Egton Medical Information Systems (EMIS), a system specifically developed for general practice and not initially included within the NPfIT); Social Services used another system (as in Walsall), as did the private providers of intermediate care beds.
Hybrids
The development and implementation of e-care pathways was the responsibility of the informatics services. They recruited hybrid ‘change facilitators’ for the task. Hybrids have been around in the NHS since the 1990s 38 (pp. 72–74); however, the ones we are discussing here have been introduced specifically to facilitate the implementation of both electronic information systems and the care pathways they supported. This new generation of hybrids function to re-organise health service provision along the more standardised lines of care pathways.
The ‘hybrids’ were predominantly nurses, employed by informatics services to help design and implement e-care pathways. This involved working closely with the health professionals to adapt and modify the systems as far as possible to meet local circumstances.
At Northants these hybrids were nurses seconded as clinical change facilitators working in small teams on specific projects, while at Walsall they were employed on longer term contracts. A further difference between the two was their approach to pathway design and IT support. In Northants, as we have seen, they encouraged the universal adoption of the SystmOne solution and the emphasis was on training the users. In Walsall, in contrast, the commitment to the portal Fusion system avoided the single-system solution. This, in turn, meant that informatics services could be more responsive to requests for modifications from the users.
Progress chasing
Care pathways are generic instruments, designed to manage a patient with a particular disease or condition (e.g. stroke). Patients, however, often present with multiple conditions; this can complicate matters and may mean that the pathway cannot be easily applied without the risk of a patient being overlooked. To overcome this kind of problem, another role – ‘patient tracking’ – has been developed, primarily for nurses, which we are calling for the moment ‘progress chaser’. The most common type is ‘case management’.39,40 Here we discuss two variants: one in relation to the FEP pathway and the other relates to the diabetic retinopathy pathway. The FEP was a complex pathway because of its reciprocal interdependencies (see Figure 1). Diabetic retinopathy had linear, sequential interdependencies and therefore appeared relatively simple. Yet it too had complexity in relation to patient tracking.
In the FEP pathway, the ‘frail elderly’ are persons over 75 years, who are ‘at risk’ because of their poor health. They may, for example, be suffering from dementia or recovering from a stroke. One major risk is from falling and then being admitted to hospital. The pathway was designed to minimise this possibility as the elderly person usually preferred to stay in his or her own home. This was the option the PCT preferred, it being less expensive than inpatient care. The hospitals benefitted too as it freed up hospital beds
40
(p. 15). Information on patients ‘at risk’ could be provided by Fusion, but the health professionals preferred to use their own judgement, as one experienced nurse explained: Our remit, … is keeping people out of hospital. [To identify those] at … high risk, we used to use electronic forms …, we have used everything from the Fusion tools, to PARIS … absolutely everything, but we have gone back to ‘hunch’ and I know that sounds really daft, but the GPs and the staff out there know the[ir] patients … (ANP 2011)
If the elderly person did need to be admitted to hospital, then the next important juncture on the pathway was his or her discharge. If an elderly person was admitted to hospital, however, then it had to be ensured he or she did not stay there longer than was necessary: These patients are already on the Matron’s caseload. We have what we call a Fusion alert, which is an email message that goes to all of the Matrons every time one of our patients goes into hospital. (ANP 2011)
A community matron, or similarly senior nurse, would visit the hospital regularly to check on FEP patients and ensure they were discharged as early as possible. As ANP, quoted earlier, explained, I am spending two days a week in hospital, trawling the wards [for Community] Matron patients so anybody that’s … actually admitted, my job is to go and get them back out … [What] I am doing with a lot of patients is establishing the ‘pathways’ [in the community so] that they can quickly link into [these] and get them [the patient] back out …
The process is rather more complex and patient focused than the quote may sound: So we are looking at things like, if they are medically unstable, I will push things through … with physio. … I will ‘bleep’ the teams, I will ‘bleep’ consultants and say ‘can you tell me what we are doing with this person on this ward?’ … Rather than them [the patient] waiting for another day to be seen by so and so, [I get them discharged] … [possibly onto] the intermediate [care pathway. If it] isn’t intermediate care, if it is a case that they might be a little bit mentally unstable, but enough that we can take that risk and feel happy to take that risk, then I may bring them out on frail elderly pathway and send the Matrons into support. (ANP March 2011)
This was case management, in practice, based on the Evercare model.
As part of the strategy of keeping the frail elderly in their homes, in Walsall, an e-health ‘virtual ward’ was being introduced (IT provides the clinical data in the same way as in the hospital). An elderly person who, for example, has had a fall will undergo a ‘rapid assessment’ to identify whether he or she can be treated adequately on the ‘virtual ward’: We [could] support them at home. Yes they might need twenty four hour care for the first couple of days and [a] step down the line they might need nursing care going in … We’d be checking on observations, that could be monitored [via tele-health] by one nurse looking after twenty patients in their own home rather than twenty patients in a ward …
Then when the patient had recovered sufficiently, they would be ‘virtually’ discharged, while never leaving their homes.
In Northants, another, different, form of ‘progress chasing’ was carried out by the failsafe officers on the diabetic retinopathy pathway. 41 Patients would be referred by their GPs, and once on the pathway, they were invited for annual retinopathy screening. If abnormalities were identified, the patient would be referred to an Ophthalmology Department, urgent cases being seen within 2 weeks, while non-urgent cases could wait up to 13 weeks.
In practice, there was a problem, some patients got lost in the system: In the database we had patients who had moved out of area or were now deceased that the surgeries hadn’t told us about and close on 2,000 patients that the surgeries had never told us about. Quite often GP surgeries were not telling us when they had a patient that was diagnosed with diabetes, and some were not telling us when a patient had died or a patient had moved out of area. (Member of the Restart Team)
This was not an issue specific to Northants, but ‘teething problems’ necessitated a relaunch in 2010 and the appointment of three failsafe officers charged with keeping a track on patients on the pathway. They soon developed a good working relationship with GPs largely because they needed to make many more manual entries than was originally intended as the system could not cope: adding, deleting or moving patients between the ‘urgent’ and ‘non-urgent’ categories: Everything is manually entered onto [the] Digital Healthcare [system] … and nothing entered automatically … Yes …, it is massive, … it’s never ending. (Failsafe Officer 2010)
The failsafe officers’ work was largely a manual process because the information they needed was mostly held outside the reach of the system. One key reason for this was that hospital ophthalmologists had only limited access, so they, instead, completed a written form and sent that to the failsafe officers for them to enter onto the system.
Another aspect of their work was ‘tracking patients’; if a patient did not attend his or her appointment, known as a DNA (or the images taken were of a poor quality), he or she would be contacted for a new appointment. But this did not happen automatically: The ophthalmologist should know, but if we find that they have got no ‘follow on’ appointment we would then alert the ophthalmologist again and say ‘we have noticed this patient’s DNA’d, there is no appointment been made, and you know we need another one made, but that is why [this] is such a fiddly job.
Not all patients responded when invited to a new appointment and some refused to be screened. Previously, rather than chasing them the officers would delete these patients from the system, to protect the service’s KPI performance returns. One failsafe officer explained the process as follows: it is following the pathway through … if [a] patient says ‘no I really don’t want it’ … they go … ‘refuse screening’, so they get called automatically again next year. What ‘refuse screening’ does it just holds them for a year, and then next year they will automatically get called back in again because circumstances may have changed. (Failsafe Officer)
The FEP and Diabetic Retinopathy pathways both required ‘progress chasers’ to ensure patients were not overlooked. In one case (retinopathy) it was largely because of the technical limitations of the system; in the other (FEP), the IT system could not have sole responsibility for taking clinical decisions, as patients could get lost. In both cases the specific need for patient surveillance came about because when an eICP crossed organisational boundaries, electronic communications could no longer be relied upon.
Discussion and conclusion
The principal conclusion one can draw from these case studies is that eICPs, if they are to be implemented effectively, need to reflect sufficiently the ‘belief systems and related practices’ 22 that one might say ‘cultures’ and practices within the local health networks, but being networks of different organisations and agencies it would be misleading to refer to these as organisational cultures. Instead these are ‘institutional’ logics because they relate to a network of different organisations and agencies which collectively and in complex ways shape the ways in which the e-health systems will be developed, implemented and used. The institutional logic of a health-care network will reflect a particular history, or histories, ‘ways of doing things’ that can be difficult to change, unless there are events that force change in ways it has not previously considered. While the pressures to implement eICPs were considerable within both health-care networks, they were never so great that their institutional logics were fundamentally undermined. Therefore, when the informatics departments were tasked with designing and implementing the eICPs, they adopted strategies in keeping with their understanding of how things worked in their ‘patch’ and in line with their previous practices, as far as they could. In Northants, the approach within the informatics services could be reasonably described as corporate, while Walsall was rather different, more of an autonomously adaptive preference. The corporate label is easily enough explained, for the PCT had a strongly corporate management approach which was translated within the informatics services as a preference for following the official guidance for the NPfIT. The autonomously adaptive preference at Walsall, on the other hand, characterised a greater willingness to engage in innovative developments, reflecting within the informatics services a ‘loosely coupled’ 42 relationship to NPfIT policy and guidance.
The corporate logic within the Northants case meant that the local implementation of care pathways was led by the informatics services and premised on the assumption that nearly everyone would be using SystmOne. This was a fiction and was, for example, one of the reasons for some of the ‘work arounds’ that evolved to circumvent the irrational implications of this assumption. Walsall avoided the necessity of system standardisation with its portal strategy, which supported a logic (or ‘preference’) we have called autonomously adaptive because the informatics services saw their role more as adapting the eICPs to the requirements of the health and social care professional users more so than the other way about. The effectiveness of the eICPs in the two health networks was not solely or primarily dependent on the underlying system rationality as reflected in the task interdependencies, although they were important, because they set the challenges that the informatics services and health professionals had to resolve, for example, in the cases of reciprocal interdependencies in the frail elderly or intermediate care pathways touched upon within this article, but set out in detail in Eason et al. 35 (available online).
The relationship between the group of concepts and eICPs is set out in Figure 2. The arrows connecting the group indicate the lines of influence shaping the eICPs, demonstrating the relative importance of each. The diagram enables one to visualise how it is possible for arrangements to emerge within each local health network dependent on their path dependency (history) and institutional logic. This helps demonstrate why there will be systematically different ways of designing and implementing eICPs even with those with the same task independencies. Northants, for example, tended to assume that eventually everyone will be using SystmOne and maybe everyone could ‘muddle through’ until then, while Walsall informatics services would attempt to find ways of getting the different computer systems to ‘talk’ to one another in order to support the care pathway.
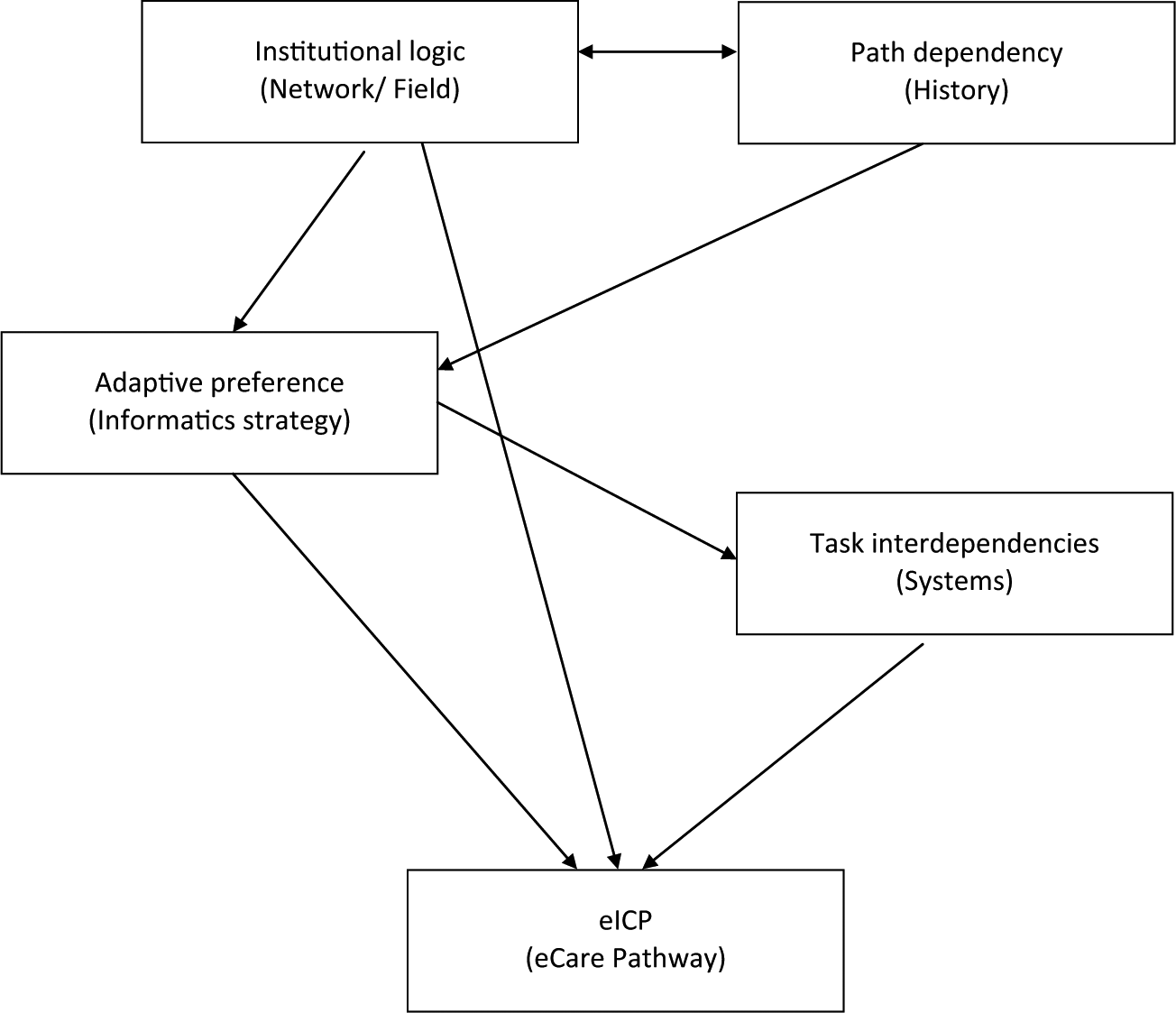
Conceptual map of institutional logics, adaptive preferences and task interdependencies.
Whatever the adaptive preference that might be apparent, reflecting whatever institutional logic, the lesson from this study is that informatics services as well as users have to be adaptable for implementing eICPs, which is a complex process requiring or implying the following:
considerable involvement of change facilitators (‘hybrids’) to support and implement pathways locally,
health professionals working with patients having to recognise they cannot rely wholly on eICPs. It is necessary for case managers, community matrons or otherwise designated ‘progress chasers’ to prevent patients getting ‘lost within the system’.
pragmatically, local ‘work arounds’ (‘loose coupling’) develop to ensure eICPs are able effectively to cross organisational boundaries. Such local adaptations are not random; they have their own rationale, which correlate with the institutional logics 23 within the local health network.
Moreover, eICPs are characterised by an apparent contradiction: they are professionally led systems designed to improve the quality of care, while re-engineering the delivery of care that enhances management control. In the case of the eICPs discussed here we found that in one (Northants), the managerial rationality tended to dominate more than in the other (Walsall). This can be explained in terms of their path dependency, which tells us that implementing technical and organisational change is challenging and where we need to look in order to bring about change successfully.
Footnotes
Acknowledgements
We wish to acknowledge our debt here to Ken Eason and Patrick Waterson, who first pointed out the relevance of Thompson’s work for this research. Earlier versions of this article were presented at the 27th European Group for Organizational Studies (EGOS) Colloquium in Gothenburg, Sweden, 2011, and Dilemmas for Human Services Conference, Friends Meeting House, London, 2011.
Declaration of conflicting interests
The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Service Delivery and Organisation (SDO) programme, National Institute for Health Research (NIHR), National Health Service (NHS) or the Department of Health.
Funding
This project was funded by the National Institute for Health Research Service Delivery and Organisation (NIHR SDO) programme (project number 08/1803/226). Visit the SDO programme website for more information.