
Abstract
The main aim of this article is to present a research agenda and systematic framework of what the field of health information systems is about, namely its central topics and connecting areas. In doing so, we try to provide a cohesive ‘big picture’ for academics and professionals that are interested in conducting research in this broad area. By using a large number of disparate data sources, we identified 3 major research fields and 18 sub-fields. As this discipline is quite new and heterogeneous in terms of themes and the educational backgrounds of its researchers, we see our conceptualisation as a first step in obtaining a collective understanding of this field, as well as being a common starting point for discussing future directions.
Keywords
Introduction
In the past decade the effects of globalisation, diversification and specialisation of markets, and technological advances revolutionised, first and foremost, highly competitive sectors such as the manufacturing and engineering sectors. Health systems across all industrialised countries have contrarily registered unsatisfactory performance developments in both cost and quality over many years. 1 Health systems in Europe, in particular, are facing considerable pressures, as life expectancy is increasing and birth rates are constantly falling. As a result, the number of Europeans aged over 65 years will rise by nearly 40% in the next 20 years. 2 Some effects of this demographic change are already noticeable, for example higher expectations and demands in relation to health service delivery, a lack of highly qualified health professionals to provide these demanded health services efficiently and continuously increasing public-sector or private-spending (in the case of a mainly privately-funded health system) to maintain the efficiency and quality of the entire sector.
Since the emergence of ‘e-health’ in the early 2000s, many expectations have raised the notion that the adoption of information and communication technology (ICT) in healthcare will potentially solve or reduce some of the problems. For instance, as stated by the World Health Organization, 3 cost-savings are expected by reducing redundancy and duplication of examinations, and enabling economies of scale. Owing to the fact that the term and concept of e-health is quite new, there is a significant variability in its scope and focus.
In terms of its functional scope, most definitions conceptualise e-health as a broad range of medical informatics applications for facilitating the management and delivery of healthcare. Purported applications include dissemination of health-related information, storage and exchange of clinical data, inter-professional communication, computer-based support, patient-provider interaction and service delivery, education, health service management, health communities, and telemedicine, among others.
4
However, we see e-health and the related technologies as only one component (indeed, an important one) of the whole spectrum of potential solutions in the field of health information systems (HIS) to address all aspects of the problem.
The aim of this article, therefore, is to provide a common research agenda and systematic framework for academics and professionals who are interested in exploring ‘technology-induced’ or ‘technology-enabled’ change in healthcare. Despite great activity in this research area, producing a wide range of theories, models, methods and software applications, we think that an underlying framework which provides a ‘big picture’ for the subject and field is still missing. Notwithstanding singular content or topic maps for distinct specialisations or sub-fields,4, 5 we think that it is important to have a holistic view, such as debated in the field of (management) information systems 6 or health services research. 7
As the field of HIS is relatively new and still in the ‘phase of formation’, we want to help to improve knowledge-building and communication between the distinct research groups (clinicians, computer scientists, economists, social scientists). Frameworks (explicit/formalised or implicit/tacit) are seen as being helpful in this endeavour. 8 Nevertheless, many have argued the value of such frameworks. For instance, a criticism is that a specific discipline or field cannot be ‘managed’ by any imposed structure and that it often discourages or restricts researchers from being creative and ingenious. In contrast, the main argument for a common research agenda is that scientists and professionals can build their research portfolio on a consistent set of ‘assignments’, thereby reducing the time for finding their way in, and ultimately improving acceptability of, the respective field. As research itself remains ‘a moving target’, 9 we are also aware of the temporal validity and reliability of our proposition. We therefore conceive this article as being rather a discussion that researchers can draw upon when creating their own ‘framework for understanding’.
Method
The nature of the research undertaken in developing this article is largely qualitative and inductive. We used the principles of grounded theory 10 as the foundation for defining our framework. Hence, as opposed to positivist or deductive research, we did not start from a priori theory or formulised hypotheses, but categorised common concepts into diverse categories. By constantly comparing the main characteristics of the data, the categories were reduced to a minimal set in order to get a plausible representation of the main fields in HIS.
Data necessary in developing this categorisation was obtained by searching ACM Digital Library, AISeL, EBSCO, IEEE Xplore, PUBMED and SCOPUS for articles containing ‘health information systems’, ‘health technology’ and ‘electronic health’ (and its various spellings) as keywords. This provided the first output from where three main themes were identified. As we could not analyse all the gathered articles in great detail, only abstracts of the most cited papers were read in the first stage. In turn, this helped to further refine the main themes into 18 sub-themes.
We are aware that with such an approach we cannot guarantee completeness of all topics covered in HIS. Moreover, we also noticed some changes in ‘denomination’ of similar topics over time (hence, our results are also dependent on specific temporal trends). As it is not our objective to be as detailed as possible or to define a permanent research agenda for the field, but rather to provide a basis for discussion, we think that the applied method yielded rigorous and interesting results.
In order to obtain an outside perspective to our categorisation, we also presented the framework at various informal meetings with other academic and professional institutions, and thereby obtained valuable feedback for further revising its structure and presentation.
Framework for the field of HIS
As result of the extensive literature review and discussion with colleagues, we decided to expatiate ‘our’ framework of understanding in the form of a graphical illustration (Figure 1).
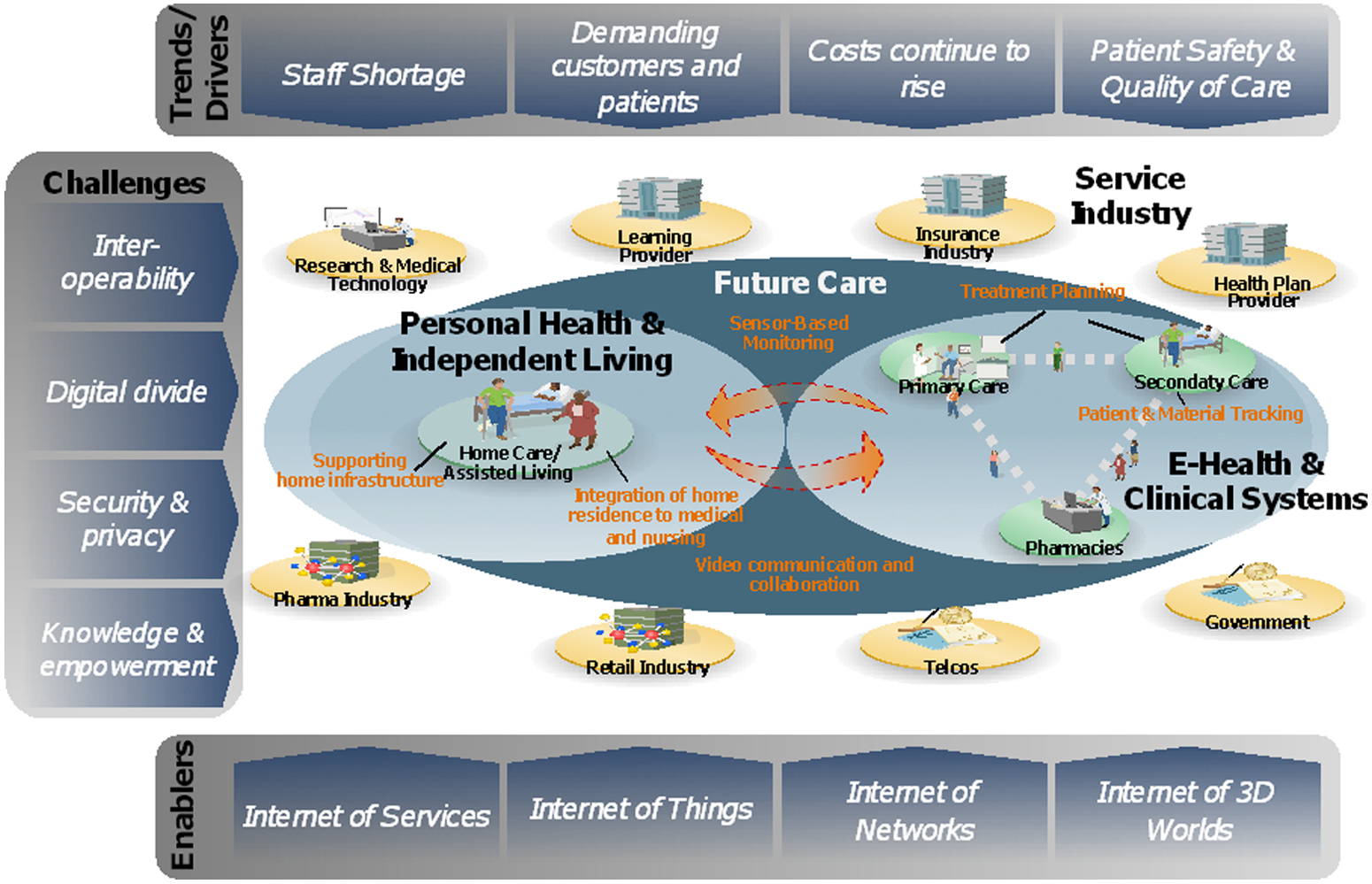
Framework for continued research in health information systems
Main areas of research in HIS
We identified three main areas of research in HIS. The most predominant area (and maybe the most mature of the three) is e-health and clinical systems. This is driven mainly by clinicians and technologists that have a deep understanding of medical processes and treatments, and thus has considerable overlap with the field of medical informatics. However, unlike medical informatics, which is often focused on a specific sub-specialisation of medicine (e.g. medical imaging or surgery), the defined field of e-health and clinical systems rather emphasises inter-organisational and inter-disciplinary research in the intersection between medical institutions (e.g. primary care, secondary care, pharmacies) and/or the service industry (e.g. the insurance industry, government, learning provider).
The second main area for researching HIS is personal health and independent living. As opposed to the first area, this approaches the adoption of information and communication technologies in the peripherals outside a healthcare organisation (e.g. in the home of the patient) and thus has a much stronger focus on non-medical professionals and patients. Also, medical outcomes may represent but one factor to be optimised by research (e.g. patient-centricity, accessibility and applicability may be equally important).
Finally, there is also the need for cross-sectional topics to be explored within the field of HIS. This may include issues related to educational, societal, economic and behavioural aspects of HIS, but also studies that explicitly address the intersection between e-health and clinical systems and personal health and independent living.
Trends and drivers for change
As already stated in the Introduction, healthcare is experiencing different causes for change. Among others, the most important drivers that we found in literature were:
insider perspective (e.g. hospital managers, clinicians, physicians)—drastic need for health professionals and general shortage of well-educated staff;
outsider perspective (e.g. patients, relatives, tax-payers)—higher demands from the side of patients and more ‘value for money’, as well as internationalisation;
authority perspective (e.g. local and national government agencies)—continuously increasing public-spending in times of forced saving;
ethical perspective (all the stakeholders): patient safety and quality of care must be improved and be adapted and conform to the modern way of living.
Challenges
We also identified some key challenges in order to effectively implement and disseminate HIS research results. Major challenges were:
technology view—inter-operability of systems and a wide range of ‘standards’ making it too complex to address a problem quickly without having extensive knowledge or infrastructure; 11
economy view—the effects of the ‘digital divide’ 12 between industrialised countries and emerging economies makes it difficult to convey research results as they often presuppose a well-equipped infrastructure that works reliably;
legal view—national laws stipulate different rules related to security and privacy of patients’ and healthcare professionals’ information, and are frequently behind the actual technological possibilities; 13
research view—knowledge about HIS is scarce (e.g. few universities providing courses) and confidence in seeing HIS as discipline is low (e.g. not having it’s own scholarly association).
Enabling technologies
With regard to the information technology (IT)-enablers for change, we identified four major Internet technologies that may improve not only the effectiveness, efficiency and quality of health services delivery, but also the transparency of economic activities and the availability of information in real time:
Internet of services—development of new health-related services that are easily accessible and consumable with current web-technologies, thus not requiring an extensive infrastructure by both services provider and services consumer (e.g. web-based clinical trials system 14 );
Internet of things—integration of physical ‘smart objects’ by means of sensors, scanners to provide novel completely new possibilities of electronic health services (e.g. sensor-enabled smart home for elderly 15 );
Internet of networks—expansion of traditional hardwired networks and transition to wireless transmission channels (e.g. wireless health monitoring 16 );
Internet of three-dimensional worlds—creation of new virtual ‘reality-like’ environments for provisioning of new health services (e.g. Avatar therapy 17 ).
Formulating a research agenda
In our opinion, research should be directed toward exploring the three main areas identified, i.e. e-health and clinical systems, personal health and independent living, and cross-sectional research, in more detail. The following section provides an overview of the sub-fields we identified during our literature review and gives a first impression of potential topics to be addressed in a common research agenda.
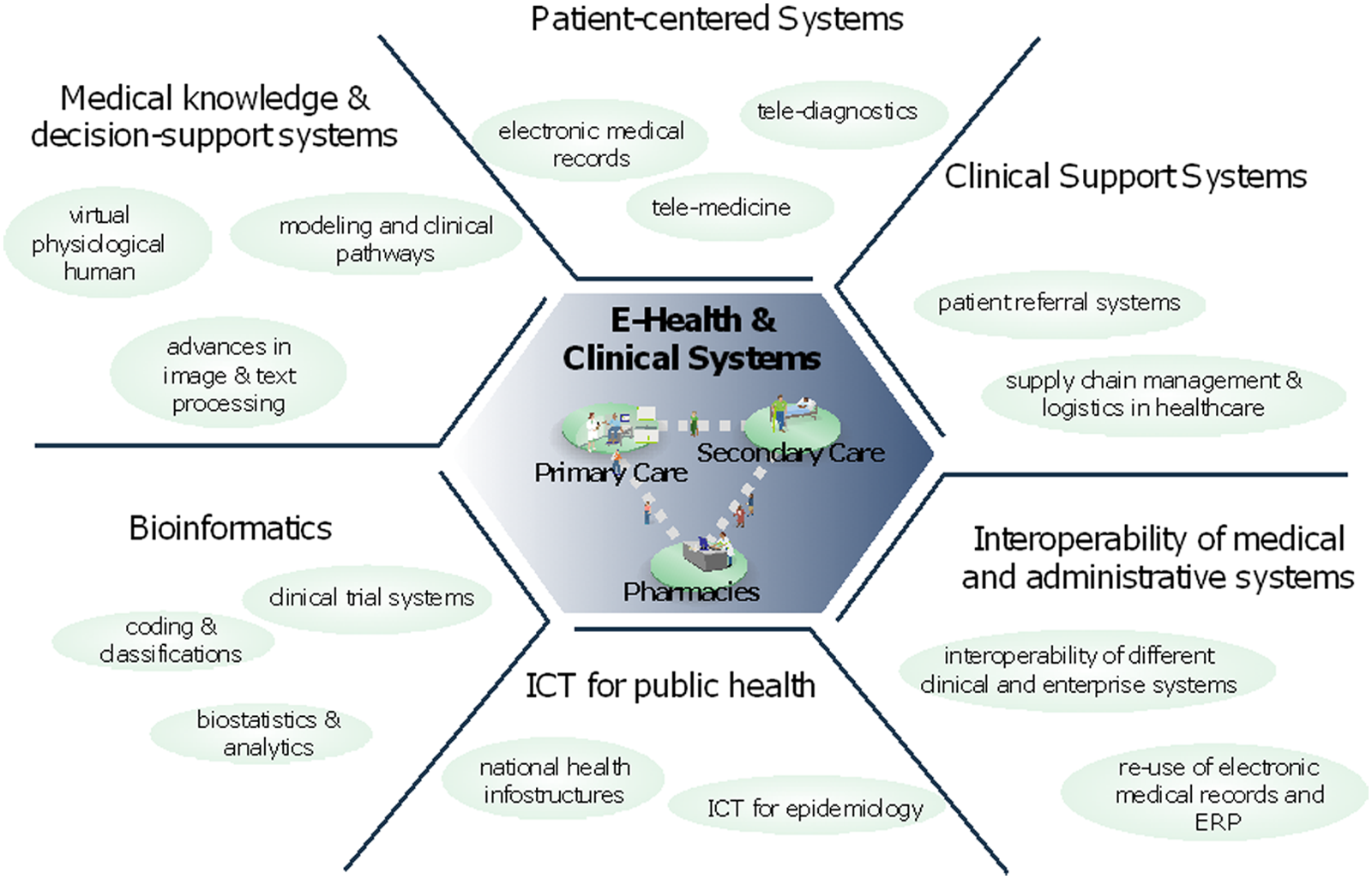
Topics in e-Health and clinical systems
Within the research area of e-health and clinical systems we identified six potential sub-fields and related topics for further exploration (see Figure 2).
Patient-centred systems: a systematic (re-)use of information about, and collaborative interaction with, patients is key for a well-functioning doctor–patient relationship. Therefore, this sub-field of HIS has a strong overlap with ‘classical’ medical informatics, although it is more interested in the inter-organisational exchange and collaboration (e.g. by means of one of the discussed Internet technologies).
Clinical support systems: good health services delivery not only depends on highly qualified doctors, but also on timely and efficient logistical services (informational and physical). Research in this sub-field therefore aims at improving logistics, for example between primary and secondary care institutions, or between a healthcare organisation and a service provider (e.g. pharmaceutical wholesales).
Inter-operability of medical and administrative systems: as already stated, inter-operability of data and processes is seen as being one of the big challenges of the coming years. Research in this area may help to improve administrative workflows within and across organisations in the healthcare sector and improve reuse of existing information.
ICT for public health: seeing healthcare not only from an organisational, but also from a national or international ‘network’, point of view, further research is needed to better connect regional/local/organisational efforts and information with a commonly used ‘overall infostructure’.
Bioinformatics: the core of clinical systems is often based on research results from bioinformatics. Hence, this sub-field will still be an important part of HIS research; however, like patient-centred systems, it will be more directed toward using Internet technologies.
Medical knowledge and decision support systems: finally, there is also a need for continued research in the sub-field of medical knowledge and decision-support system.
Topics in e-health and clinical systems
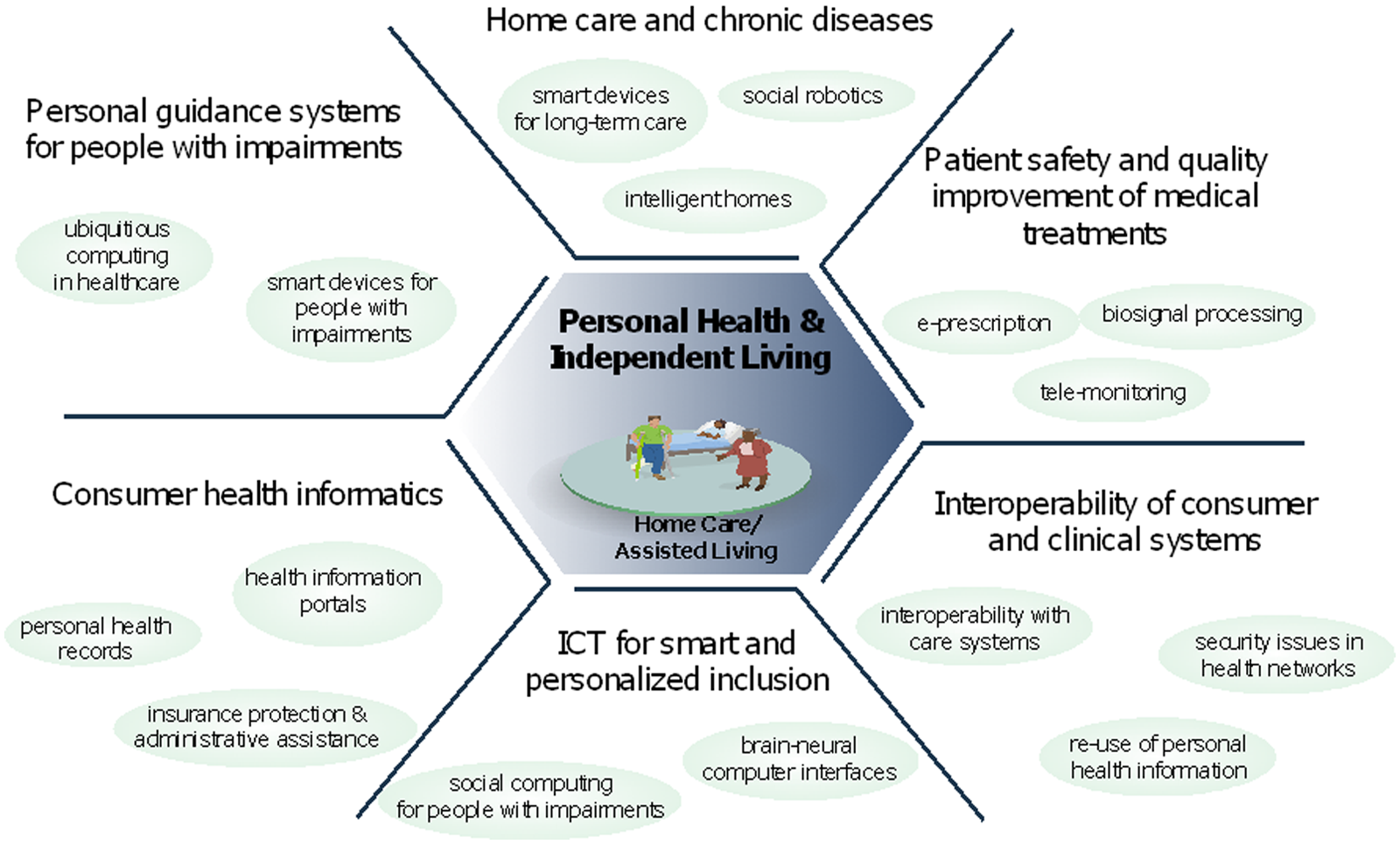
Topics in personal health and independent living
With respect to personal health and independent living we found the sub-fields listed below.
Home care and chronic diseases: research is needed that assists ‘healthy ageing’ and supporting older and chronically ill people to live as long as possible in their homes. In this context, much work related to social robotics and intelligent homes, as well as smart devices for long-term care, is found.
Patient safety and quality improvement of medical treatments: evidence exists that poor data quality can cause severe complications or even the death of patients. In particular, when patients receive an ambulant treatment it is necessary to ensure the same safety and quality standards as when being treated at a healthcare organisation (e.g. by means of biosignal processing, tele-monitoring or e-prescribing).
Inter-operability of consumer and clinical systems: many systems in this area of HIS are developed independently from existing clinical systems and standards. However, in order to connect both the ‘clinical world’ and the ‘consumer world’ more research is required that emphasises inter-operability between these two worlds.
ICT for smart and personalised inclusion: a ‘digital divide’ not only exists between rich and poor countries, but also between the healthy and the impaired. Thus, we strongly recommend paying attention to topics such as social computing for people with impairments or interfaces that help disabled people to be included.
Consumer health informatics: making medical knowledge ‘usable’ for everyone is a fundamental change in health services delivery. Although supported by some clinicians, it also is strongly criticised. Hence, research is needed that assures quality of health information use on portals, as well as that which assists healthy and ill people to keeping track of their health (and insurance) status.
Personal guidance systems for people with impairments: there is also a demand for personal guidance systems, especially for people with impairments. This can be implemented in the form of smart devices and other possibilities that are offered by ubiquitous computing.
Topics in personal health and independent living
Cross-sectional topics in HIS
Finally, we observed some cross-sectional themes that are studied with regards to HIS.
Human–computer interaction: acceptance of a new HIS considerably depends on how well it is able to fulfil the requirements of the users. In healthcare, this is normally not an easy task as a wide range of different user groups with various educational backgrounds, habits and needs exist. 18 Hence, new methods and models are needed that help researchers to systematically build and evaluate HIS.
Social implications: HIS is not only about machines, but mostly about people. As with any invention not only new evidence is required of how individuals accept and use novel systems (see the pervious sub-field), but also studies that explore the effects of ethical, cultural or demographic conditions.
Standardisation and conformity: as the world is becoming more globalised, research is needed that addresses not only the ‘technical’ inter-operability of HIS but helps in internationalising and standardising research methods and outcomes.
Education, training and dissemination: what is the value of breakthrough scientific findings and inventions when nobody understands or benefits from them? Improving education, training and dissemination of new knowledge, and continuously refining existing knowledge, is thus crucial for any field.
Security issues in health networks: with the digitisation and improved accessibility of large amounts of information, there is also a need for enhanced security and privacy mechanisms. A holistic research agenda for HIS has therefore also to account for security-related topics.
Value of IT in healthcare: as stated in the Introduction, public-spending on healthcare is continuously increasing; however, countries may no longer be able to afford this in the long-run. Hence, with every invention and adoption of a new technology there will always be space for studying its effects on the economy and welfare. Potential topics in this sub-field are, therefore, for instance, value assessment methods, business models, entrepreneurship and other economic aspects of IT-enabled healthcare.
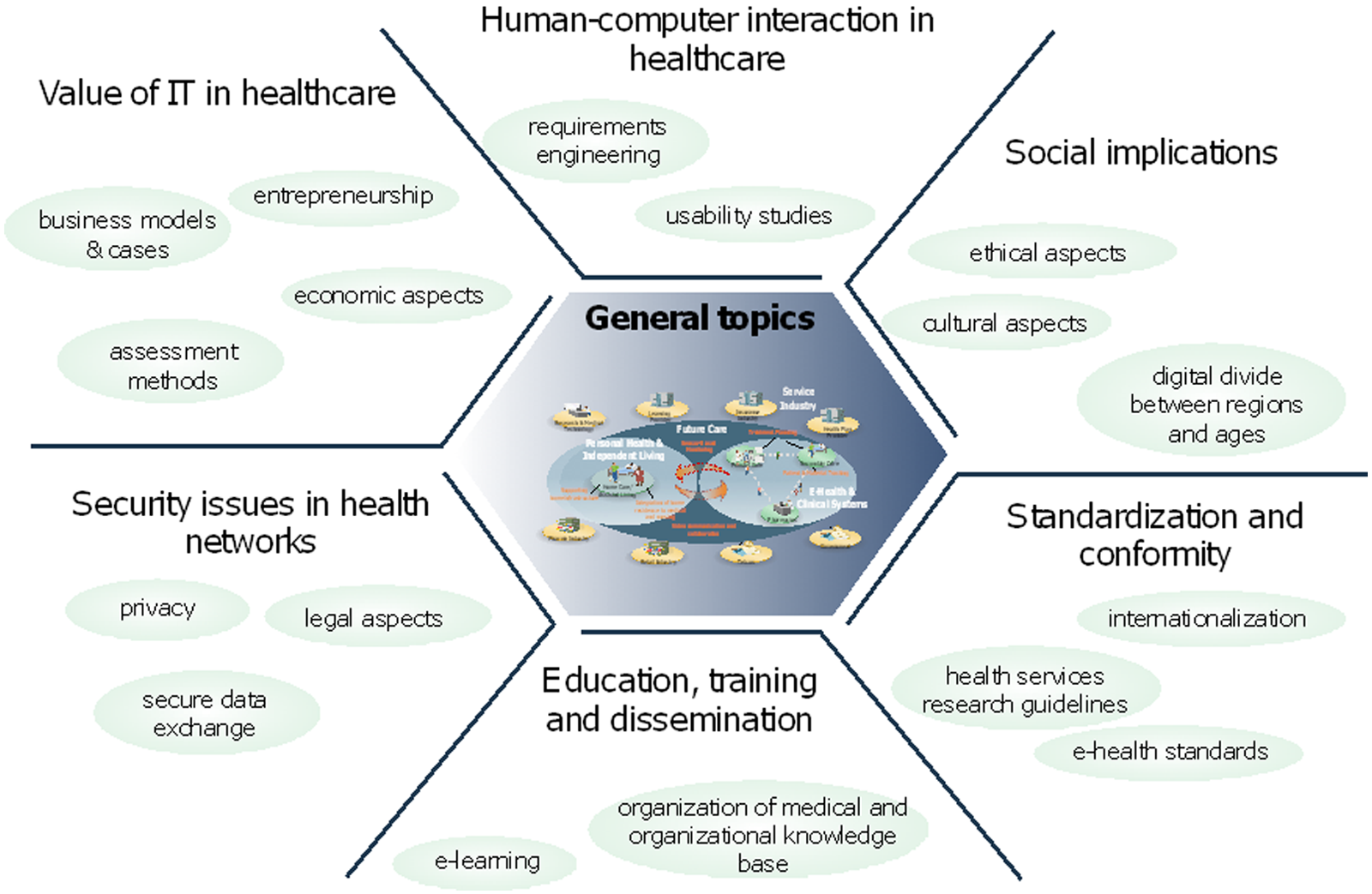
General topics in health information systems
Conclusions
In this article we have discussed a systematic framework and research agenda for the new field of HIS. Based on the grounded theory approach, we identified 3 main areas and 18 sub-fields for continued research in the field. We think that in making use of the presented framework, it may become easier to represent the significance of a particular research interest and where it ties into other areas of the field. By creating an overall ‘big picture’, it may also help to better identify specific research topics to be pursued, as well as encourage the linkage of other fields, such as medical informatics and health services research.
Footnotes
Acknowledgements
We thank all the participants of the discussions who kindly offered their time and helped us to improve our work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.