
Abstract
The growing need to gain efficiencies within a home care setting has prompted home care practitioners to focus on health informatics to address the needs of an aging clientele. The remote and heterogeneous nature of the home care environment necessitates the use of non-intrusive client monitoring and a portable, point-of-care graphical user interface. Using a grounded theory approach, this article examines the simulated use of a graphical user interface by practitioners in a home care setting to explore the salient features of monitoring the activity of home care clients. The results demonstrate the need for simple, interactive displays that can provide large amounts of geographical and temporal data relating to patient activity. Additional emerging themes from interviews indicate that home care professionals would use a graphical user interface of this type for patient education and goal setting as well as to assist in the decision-making process of home care practitioners.
Keywords
Introduction
Two of the most salient issues in contemporary health-care planning are the impacts of shifting demographics and the increased utilization of informatics in health care. There is growing attention within the health-care community toward providing support for older adults who live independently in their homes as they grow older. A significant portion of these health-care clients are both elderly and live alone. 1 Home care for these clients is more challenging than care in a clinical setting due to the heterogeneity of the environment and short duration of health-care provider home visits.2,3 Coordination and communication of information related to care is also a unique challenge, due in large part to the relative isolation and autonomy of the work environment of home care practitioners. 1 In addition, next to medication, the cost of home care is the most rapidly increasing area within the publicly funded health-care system in Canada. 4
The purpose of this study is to investigate the efficacy of a user interface that integrates the bio-physiological information of home care clients into a decision support system that provides home care clinicians with better scheduling capabilities, assessment of client activity in and out of home, and timely access to information into a user-friendly decision support system. The project focuses on the integration of existing technologies that were adapted to the home care context; specifically: (1) non-intrusive monitoring approaches, using binary and analog sensors for measuring night-time sleep patterns developed by Dr Goubran and his team at Carleton University;5 –7 (2) a cell phone–based Global Positioning System (GPS)-supported monitoring system to track patients’ daytime life events and health conditions developed by Dr Doherty and his team at Wilfrid Laurier University;8,9 and (3) a prototype web-based software application developed by Dr Doran and her team at the University of Toronto10 –12 that equips clinicians with handheld units to assist in the collection and utilization of bedside patient data and provide real-time feedback, including suggested best-practice guidelines, tailored to an individual patient’s needs. That software was adapted specifically for the home care clinicians’ environment.
Two prototype displays were developed that map information flow for a number of patient-specific conditions/scenarios. Data on these displays were gathered from focus groups comprising home care nurses. A simulation laboratory was then used to conduct one-on-one interviews with home care professionals to determine the usability of the various aspects of these interfaces. The data were used to explore the most effective means of visually displaying information gathered from a non-intrusive client monitoring system. In addition, the data from the interviews were analyzed to determine how home care nurses would use the information from these interfaces in a real-world setting. This article examines the results of these simulations in order to explore how home health-care professionals can use decision support technologies that integrate bio-physiological information obtained through non-intrusive monitoring to support safer patient care practices for seniors.
Literature review
The increasing demand for home care by an aging population makes patient safety a growing concern for home care professionals. Health researchers and practitioners have documented both the significance of adverse events in a home care environment as well as the measures being taken to reduce their occurrence.2,3,13,14 The heterogeneity of the home care environment in addition to the increased demands on home care professionals make the reduction of adverse events more challenging, including urinary tract infection, fall or accident at home, wound deterioration, unexpected nursing home admission, increase in the number of pressure ulcers, improper medication administration or side effects, hypo/hyperglycemia, and unexpected death. 7 Exacerbating these concerns are increased demands on home care professionals as well as the global shortage of health-care workers. 8
A recent review by Paré et al. 14 highlights the growing importance and efficacy of informatics in home care. Their review of home telemonitoring literature found that eHealth interventions have aided practitioners in monitoring and controlling blood sugar levels, asthma attacks, hypertension, and heart failure. The use of this technology has the potential to address a number of these concerns through improved patient monitoring in home care settings and improved communications among providers within the health system.
Home health-care teams use structured or narrative notes to record most of the client data. 5 This information is garnered from monitors (e.g. blood pressure, pulse oximetry) and laboratory instruments (e.g. glucometer). However, most telehealth applications gather data from only a single device, such as blood glucose monitoring. The fear of overburdening the patient and home with multiple devices and applications inhibits the gathering of additional patient data. Therefore, the future home care environment must incorporate eHealth technologies that integrate multiple points of data, including remote monitoring and remote patient data entry, in a non-intrusive, user-friendly format. 15
Non-intrusive monitoring of home care client activity and mobility
To prevent chronic diseases such as cardiovascular disease and diabetes, home care practitioners encourage regular physical activity. 16 Also, research has demonstrated that monitoring of physical activity can facilitate patient self-management of their ailments, along with providing detailed feedback for medication adjustments and tailoring care regimes.17,18 In particular, Alpay et al. 19 found that eHealth monitoring technology can be an effective tool for patient education and health literacy and lead to more effective patient self-management. Tools that can automatically monitor and log patients’ daily activities with specifics on physical activity, mobility, travel, and sedentary activity could enhance opportunities for diagnosis, education, and promotion of self-management. Thus, cell phones equipped with GPS technology in conjunction with current Geomatic technologies allow for the development of an automated monitoring system that is able to wirelessly transmit a home care client’s location to a central server in order to provide a very accurate depiction of personal or vehicular movements over long durations.20,21 Using a cell phone to monitor patient activity can provide useful information about patient habits that can be used to refine care regimens.
Intuitive integrated health monitoring systems
The isolated and heterogeneous environments of home care require monitoring devices that are suited for the issues that emerge most often in these settings. 15 Although the technology exists to collect patient data from non-intrusive monitors, creating a computerized clinical decision support system (CDSS) in a home care situation has proven challenging. According to Garg and Tonelli, in a hospital setting, a CDSS can improve clinical decision-making by delivering several modes of decision support, such as “alerts of critical values, reminders of overdue preventive health tasks, advice for drug prescribing, and suggestions for various care issues.” 22 In addition, Garg and Tonelli determined that a computer-based CDSS is most effective when it is integrated into a health-care practitioner’s workflow and provides relevant and contemporaneous recommendations in the place where it is needed.
To support a CDSS, current hardware and software technology can collect, analyze, and organize large amounts of data almost instantaneously. This process, called data mining, has proven useful for processing large amounts of information from health-care databases for the purposes of improving the quality of patient care. 17 By using data-mining techniques, information can be garnered from monitors to accurately estimate important home care client information such as vital signs and respiration rate, movements, sleeping patterns, and sounds and be displayed on a CDSS.4,6,23
The use of a computer-based CDSS to improve the efficiency in health-care delivery is currently being introduced into hospitals; however, these technologies have not yet been applied to a home care environment. 24 JeongGil et al. 24 note that in order to facilitate more effective and efficient home care delivery, this intuitive technology should be able to sense its environment, monitor multiple environments, and make assessments based on the context of these environments; user needs; and institutional policies, procedures, and permissions. In addition, these tools should process this information and adapt, block, or generate information flows based on the actions decided upon.
In a home care setting, the intuitive, integrated monitoring technology like a computer-based CDSS can be used to provide home care professionals with the most relevant information on patient preferences, save search time by understanding the relative proximity of the clinician and patient, as well as realize significant efficiencies by identifying clients that require a visit based on need rather than scheduling visits to all clients.
Methods
Data for this article were collected as part of a larger study focusing on the development of an integrated telehealth application system for use in a home care scenario. Prior phases of this study included the initial technical development of graphical user interfaces (GUIs) that present multiple sources of patient data, collected from non-intrusive monitoring devices, on a low-fidelity, handheld device such as a personal data assistant, cell phone, or tablet. Another earlier phase of the study consisted of a series of focus groups conducted to further develop and refine the initial GUI. These phases were designed to implement a user-based approach to the construction of this technology with the goal of producing an instrument that home care professionals and their clients would find intuitive and easy to incorporate into their care regimen.
The data used in this article draw primarily from the third phase of the study which utilized individual interviews to garner feedback to facilitate the further refinement of the GUI as well as explore emergent themes related to how this integrated technology may be used in the heterogeneous environment of a home care setting. This phase of the study consisted of eight semi-structured interviews conducted in a simulation laboratory setting which focused on end-user exploration of the most important GUI features. To this end, two possible versions of data monitoring GUIs were developed and compared by the interviewee. The target end users, home care nurses, physiotherapists, occupational therapists, and case managers were recruited from a home care service agency. In all, eight study participants were selected from these user groups with the exception of physiotherapists who were not available to be interviewed during the time of the study.
To facilitate the collection of qualitative data, a usability test was developed whereby the participants used cursor movements on a laptop computer screen to simulate their interaction with the GUI on a future mobile phone or tablet device. The simulation of a low-fidelity device was necessary to prepare for the next phase of the study in which home care professionals will use the device in a real-world setting to conduct real-time tests of the non-intrusive client monitoring and decision support interface. The use of the laptop at this stage was a pragmatic choice, as it provided a better platform on which to view and record nurses’ interaction with the technology, and provided a more familiar interface for nurses at the time. Additionally, the innovation in this study was the integration of different existing technologies, rather than the hardware platform utilized.
To encourage collection of a rich qualitative data set, each participant was presented with a simulated case of a 79-year-old male patient who had recently broken his ankle. The case was developed to be representative of the type of clinical issues that arise in community nursing. It was developed with the input of clinical experts associated with the research team and with the input of the professional practice director from the home care provider agency that participated in the study. The participants were asked by a facilitator a series of open-ended questions designed to elicit information regarding the GUIs’ ease of use, types of functions and features participants found helpful, and areas of improvement. In addition, interviewees were asked to “think aloud” as they interacted with the prototype interfaces. Each test lasted approximately an hour and was documented using audio recordings of the participant’s verbal responses and video recordings of the computer screen to obtain a visual account of the participants’ interactions with the GUIs.
Interviews were transcribed verbatim and the qualitative data analysis software NVivo was used to analyze the results. The data from the interviews were examined using a qualitative analysis framework to determine relevant themes that emerge from the interviews. An iterative process for coding and analyzing the data collected from the interviews was utilized. The analysis of the data was based on grounded theory techniques described by Miles and Huberman 25 and Strauss and Corbin. 26 These techniques included open coding, code notes, memos, and theoretical notes. Memos were made throughout the analysis process. The memos were used primarily in the initial analysis of the transcribed data. Key concepts from the memos were then used to reexamine the data and further refine emergent themes and concepts in the interviews. Through iterative passes of the transcribed interviews, themes emerged and were refined.
Results
The primary purpose of this usability analysis was to uncover various parameters to GUI refinement. As a result, many of the initial findings from the interviews with home care professionals related to fine tuning various aspects of the display such as font size and style, colors, graph axis locations, navigation issues, and how the information was grouped. These specific findings are being incorporated into a refined version of this technology. On more thorough qualitative analysis of the usability findings, four significant themes emerged that have broader applications to the field of health informatics client monitoring and decision support system development. These relate more to the application of this technology in a home health-care setting and how home care professionals could gain efficiencies in their administration of care in a heterogeneous and remote environment. These are the main focus of the results to follow.
Polar displays and interactive graphics
While testing the GUI prototypes, participants identified a user experience which was both efficient and comprehendible by the use of “polar” displays. Polar displays are a type of configural graphic that are “created by orienting the axes of several variables so they originate from the same point.” 27 These displays were created by normalizing the data and setting the normal to the same distance on each axis to produce the polar stars. Participants found this means of display superior to the GUI that used horizontal bar graphs to display patients’ goal attainment. For instance, commenting on the usability of the polar display GUI (Figure 1) over the sparkline GUI (Figure 2), one participant said, “Um, yeah the layout, this is fine. This is fine. It’s easily readable …” (P002). Another participant noted this format’s ability to display whether home care clients are attaining their personal goals, “… it does give us a comparison with the goal and the actual” (P007).
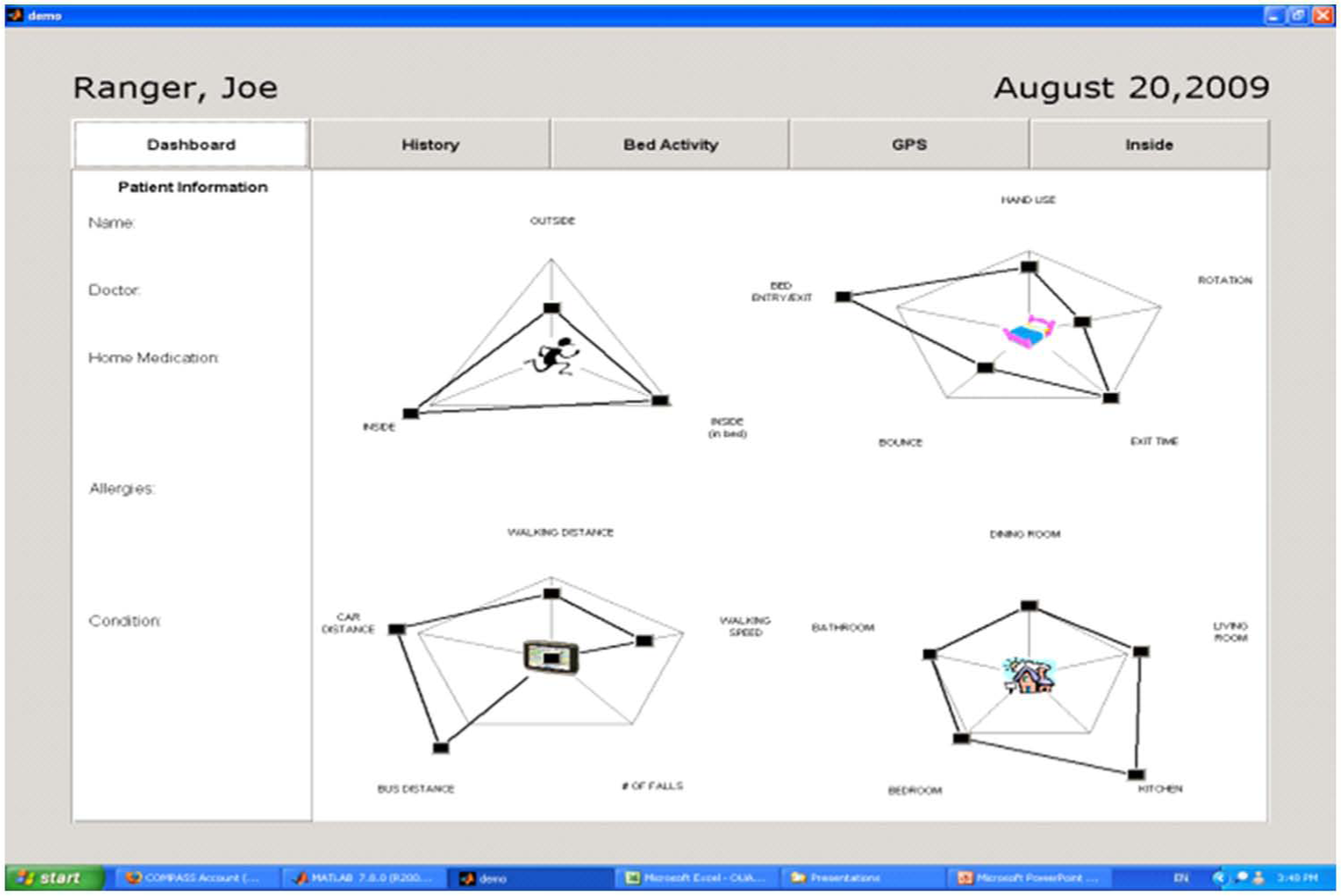
Polar display homepage.
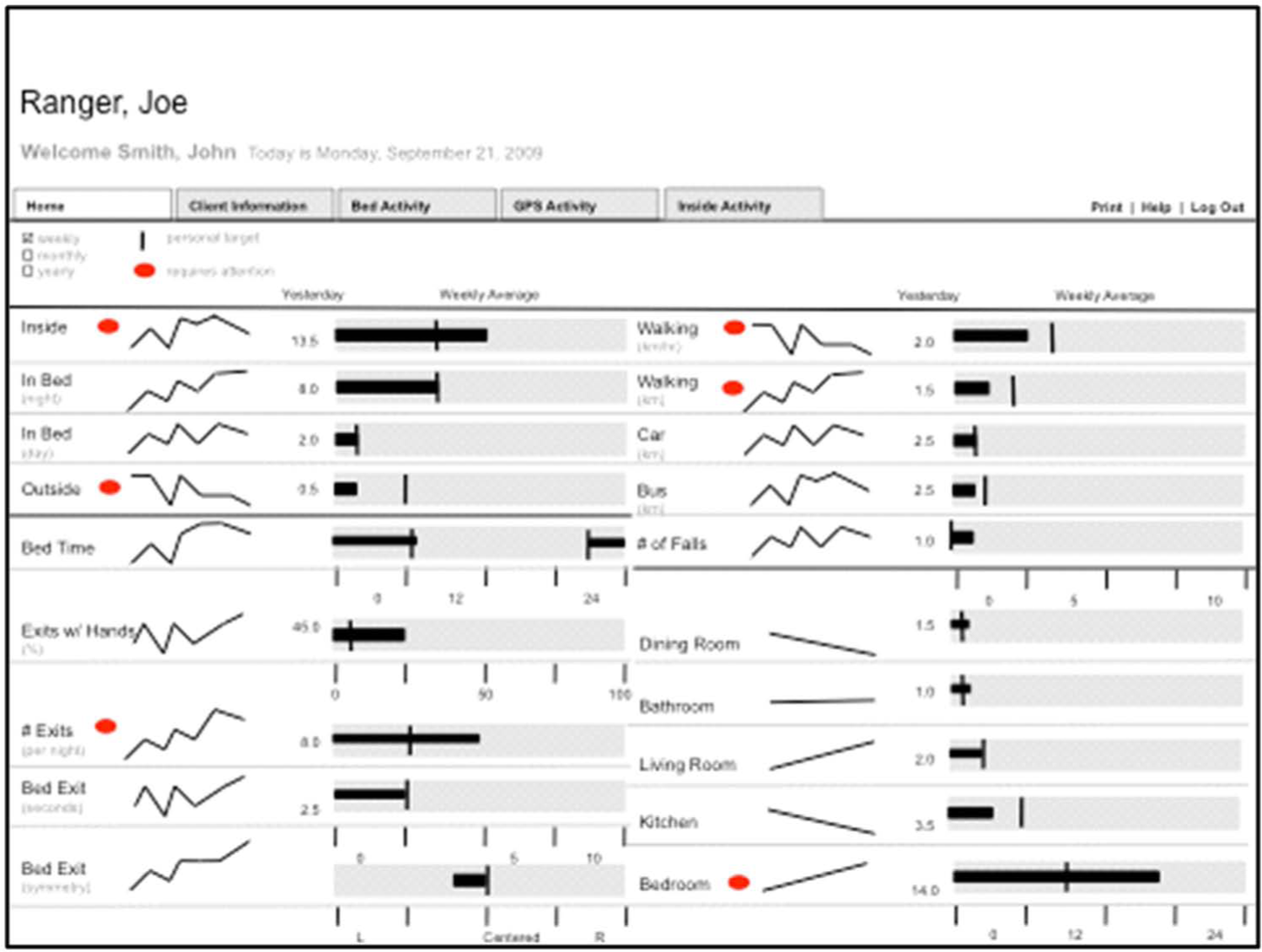
Sparkline homepage.
Another finding that emerged from the data which is pertinent to health informatics was that many of the participants wanted an interactive GUI that allowed them to access additional information in a manner similar to web 2.0 applications. For example, some of the participants indicated that the ability to scroll over unfamiliar terms and have them defined, similar to the interactive help button on computer software programs, would enhance the usability of the GUI: Now … inside. What I’m curious about if they have any definition, let’s say if I put my curser on the word “inside.” When I put it, it’s just the same graph as when I, you know I put in on the weekly average. It’s the same graph. (P001)
In addition, several participants indicated that they would appreciate the ability to rescale patient data to look at results from longer or shorter periods of patient monitoring. As one study participant noted, Again it would really be nice to have the option just to click there. Oh, look at that. I can. That’s awesome. See I like that ‘cause then I can just um, could I make this bigger so I could cover it with the whole screen? (P004)
The majority of study participants appreciated the simplicity of a display that presented a limited amount of data but was, at the click of a button, able present more detailed client information.
Patient history
Participants noted that knowing a patient’s history, apart from the general information such as primary contact(s), health card number and medications used, and so on, would allow for better collaborative servicing of the client. For instance, one participant noted that, “… I think the more information we [all health care personnel] have in common about the person the better, so we’re all hearing and talking about the same thing …” (P004). Another participant added, “In the ideal world … I wanna know everything … I need to know their surgical history, if they just came out of the hospital or their medical history, all of it, social history …” (P003).
In the same vein, others commented on how useful the system’s patient history tab would be if it informed them of the family care regime, in particular the dynamic of the family, for instance, whether the children were involved in their parents’ care giving efforts and/or the children and parents’ relationship status. One participant stated the need to view specific instances of repetitive patient behavior, “I guess under conditions you’d probably have a history of falls” (P004). Alternatively, one participant stated that information displayed should be tailored to the home care professionals’ needs, “I’m a nurse … I want to see nursing graphs” (P007).
Patient targets and goal setting
While evaluating the monitoring system, consisting of data on patient’s activity patterns and mobility risks in and outside the home, most home care providers pointed out that understanding a patient’s personal health targets were useful for them in providing care to the client. For instance, one participant stated, “I like personal [targets] because everybody is different … people have lots of different problems so I don’t like to group people together and say: ok everybody has to be at this target” (P007). A couple of participants felt strongly about possessing the knowledge of the larger population target as a means for client education, but at the same time being able to determine an individual one, … if you want to educate the client, you know, and you don’t have that information readily available … up to date stats that would indicate … for knee surgery it takes about six to eight weeks for this stuff to heal. (P001)
There were different opinions among participants as to who would determine the patient’s personal targets. When asked who would actually set the target, one participant remarked, “I would assume whoever has the permission … the physio or OT because they’re the most qualified to discuss what targets these people should be making” (P003). Others agreed and preferred that the target be a personal target set by them for each individual client, “That would be helpful because each individual is different” (P001). Conversely, one participant stated, “I would set it with the client … that’s how we do our goal setting because the more we get them involved in this process the better the outcome is going to be” (P004). One participant agreed that health targets should be patient driven but was curious to know who would set the patient standards, “Well we know everybody does what the book says. But everyone has their within normal range … so I think it should be really what is within norm of that individual.” Another participant agreed that the client should set the targets but that it was not always practical to do so, “… it has to be the client’s target with consultation of course … cause they won’t agree if they’re not on board.”
Visual showcasing
When discussing with a patient their condition, the ability to easily visually showcase these health data to clients was found to be extremely important among most participants as the display function would act as a teaching tool during client visits. The following participant’s thoughts demonstrate this finding, “… if you have something visual to show them this is the before and this is the after again it objectifies what we’re doing and they actually get to see some of the progress or progression” (P004). Similarly, others indicated that it would be easier to plan a care regime if a patient’s monthly medical condition was logged and available for display, as they could more readily recognize patterns and make correlations regarding their health, especially in chronically ill patients (P001).
More specifically, a couple of participants mentioned that the ability to visually showcase data to patients in a weekly, monthly, and yearly comparison would be an asset to patient education and make their treatment plans more meaningful. One participant stated, “that would be great for the patients to see on a weekly basis and on a monthly basis where they come and…I think that would be great” (P006). Data of this nature would also be used for patient management in the following way, … if the patient says: “Well I want to know where I’m at?” Then this would be a good indicator. We can say this is what normally what everybody is and this is where you are at this point. (P001)
Another participant echoed this same sentiment, … if you show them a goal and where they’re at it kind of gives them a little bit of an initiative to work harder and also it kind of gives them a little bit of an idea of what’s normal, of where they should be at.
Other participants stated the importance of visual information as a means to justifying to patients the need for assistive devices and home modifications. “… if we had data like this we could say you know this is the reason why we’re recommending this sort of stuff” (P004). Finally, a couple of participants mentioned the ability to magnify the data for persons with visual impairments as a means to better communicate with the patient.
Summary and conclusion
Using decision support technologies that integrate bio-physiological information obtained through multiple non-intrusive monitoring for home care has important implications for improving the productivity of home care professionals and promoting safe client education. This article demonstrates the importance of a user-friendly GUI design in the application of a multi-sensor monitoring tool. While assessing the technical performance of the GUI, home care providers overwhelmingly stated the importance of a user-friendly client monitoring and decision support system, which enables them to anticipate safety risks, monitor progress toward rehabilitation goals, and support virtual health-care management. Specifically, most agreed that an optimal system would not only provide a detailed patient history and visualization of their client’s activities but also support the collaborative creation of a patient’s personal health targets, in turn furthering patient self-management and education. Also, they saw it as a means of contextualizing and standardizing clients’ perception (such as how far of a walk a client went on when they gave vague answers such as long or short), and in providing a GUI that could be shared with their clients, as a means of illustrating where they are meeting or falling short of their goals. Thus, the home care practitioners viewed the GUI not only as a decision support tool but also as a means of more effectively interacting with their clients.
With this function in mind, most of the interviewees indicated that their preference was for a GUI that was easy to understand but capable of representing pertinent data. To this end, the home care practitioners in this study felt that a simple homepage with the ability to interact with the displays was the best means of displaying temporal and geographic data at different scales. Documenting the outcomes of this simulation study has demonstrated that there are directions for improving the feasibility and effectiveness of integrating bio-physiological information with decision support technologies.
Footnotes
Acknowledgements
The authors would like to acknowledge Vilas Joshi, Ha Nguyen, Eric Sadowski, and Anneliis Tosine for their work in the data collection phase of this process and Lindsay Woodside in the writing phase of this article.
Funding
This work was supported by the Canadian Institutes of Health Research (CIHR) and Natural Sciences and Engineering Research Council of Canada (NSERC) Collaborative Health Research (Project grant number CHRPJ351154 – 08).