
Abstract
This study applied artificial intelligence to help nurses address problems and receive instructions through information technology. Nurses make diagnoses according to professional knowledge, clinical experience, and even instinct. Without comprehensive knowledge and thinking, diagnostic accuracy can be compromised and decisions may be delayed. We used a back-propagation neural network and other tools for data mining and statistical analysis. We further compared the prediction accuracy of the previous methods with an adaptive-network-based fuzzy inference system and the back-propagation neural network, identifying differences in the questions and in nurse satisfaction levels before and after using the nursing information system. This study investigated the use of artificial intelligence to generate nursing diagnoses. The percentage of agreement between diagnoses suggested by the information system and those made by nurses was as much as 87 percent. When patients are hospitalized, we can calculate the probability of various nursing diagnoses based on certain characteristics.
Introduction
The 21st century is an era of information technology (IT). Since 2006, Taiwan’s health authorities have been actively promoting electronic medical records and Internet resource sharing, spurring Taiwan’s medical institutions to rapidly introduce computerized medical systems and nursing information systems in order to help nursing staff members identify problems, determine diagnoses, and analyze decisions when taking care of patients. According to reports released by the National Union of Nurses’ Associations, Taiwan, ROC, and the Taiwan Healthcare Reform Foundation in August 2011, the number of patients who are cared for by healthcare providers in Taiwan today is one to six times as many as the number in other developed countries, 1 a fact that could adversely affect the quality of medical treatment and healthcare and could even cause prolonged hospitalization and a higher occurrence of complications, deaths, and preventable accidents.2,3 When taking care of patients, nursing staff have to collect data, determine nursing diagnoses, make nursing plans, and execute nursing practices based on their own expertise and objective evaluations. The most difficult part of this entire process is making decisions for a nursing diagnosis. 4 Therefore, the development of information systems for the nursing process has to be prioritized. According to previous research, an effective information system could reduce the workload of healthcare providers, increase the time healthcare providers directly spend on patients, improve the quality of healthcare, and ensure patients’ safety in medical treatment. 5
Literature review
Nursing staff and nursing practice
Nurses are on the front line of clinical duties and serve as an important safeguard for patients’ safety. In the current arrangement of nursing staff shifts in Taiwan, one nurse, on average, takes care of 7–12 patients on a day shift and 12–30 patients on a night shift. 2 In Taiwan, only 357.9 nurses are available for every 100,000 people, a number significantly lower than 771 in New Zealand, 724 in the United Kingdom, 492.1 in Singapore, 782 in the United States, and 763.8 in Japan.6,7 As a result, the nurses in Taiwan are overworked, and many quit their jobs, mostly due to stress. According to previous research, junior nursing staff members who quit their jobs accounted for 20–32 percent of the total number of nurses who resigned, much higher than the average 9 percent in other professions. 8 The following are the three major reasons why junior nurses quit: (1) lack of clinical experiences and nursing skills, (2) poor coordination with colleagues, and (3) work overload affecting daily life. 9 Studies indicate that new clinical nurses face multiple forms of stress due to both internal and external factors. They thus tend to make mistakes. However, these mistakes are often caused by flawed systems rather than individual negligence. 10 In an intricate medical system, the mistakes could be linked to all kinds of factors. 11 However, the key factors are often associated with the design of the entire workflow. As a poorly executed process could result in excess pressure on the nursing staff, the development of an efficient nursing information system to support nurses is of vital importance. 12
The first stage in the clinical healthcare process is the nursing assessment—assessing the patient’s vital signs, recording the patient’s major complaints, and conducting a physical examination. The commonly used Gordon’s 11 functional health patterns in clinical nursing care collect subjective and objective data used in the second stage, which includes an analysis of the gathered data and the formulation of a nursing diagnosis. In the third stage, preliminary diagnoses are used to set nursing care targets. The fourth stage involves scheduling and applying treatment methods in accordance with the targets set in the third stage. Finally, in the fifth stage, healthcare providers evaluate whether the targets have been achieved and whether the problems have been resolved. Afterward, they determine the need to continue nursing care or to reevaluate patients to validate the process flow or to detect any new problems. All together, these various stages make up the nursing process. 13
Decision-making in nursing
A nursing decision is defined as the determination of health problems, priorities, and separate nursing practices by a nursing staff member who combines his or her comprehensive physiological, psychological, spiritual, and social views of a nursing case with his or her own knowledge, past experience, and instinct before making a judgment. 12 From several recent studies, we have found that the actual nursing issues faced and nursing practices offered by the nursing staff exceed the items disclosed in most nursing records. In the current medical environment, one in which patients develop quick and unpredictable symptoms, medical techniques and equipment are constantly advancing, and the manpower of nursing staffs is continuously shrinking, it is not easy to make correct nursing decisions and keep accurate records in a limited amount of time.13,14 In clinical practice, a nursing staff is always faced with situations that need prudent decision-making. The nature of the decisions to be made lies in making choices, which could be complicated.14,15 Nurses need to arrive at an effective clinical decision through extensive sources of knowledge and reliable information in a supportive environment. 16 From research studies and first-hand clinical experience, we have found that when a patient is hospitalized, a nursing staff obtains the patient’s preliminary information by using Gordon’s 11 functional health patterns. 17 However, due to the shortage of nurses, poor judgment, and a shortened recording procedure, most nursing staff members experience a lot of stress when making decisions. They find it hard to create accurate and complete nursing diagnoses based on the data they collect and analyze in such a short period of time. 18 Moreover, the recording stage can take substantial time out of a nurse’s busy schedule and is more likely to be interrupted by other duties. Constraints could also affect data gathering and thus result in illegible records and missing information, which could make it difficult for nurses to assess the actual health issues of patients.
A decision support system is a type of information system that helps individuals to make relevant decisions by leveraging databases and the computing capability of artificial intelligence to facilitate decision-making processes.19,20 Nursing staff members usually have to obtain information and make prompt decisions under time constraints, so they often fail to completely understand the health issues of patients and thus limit their capability to make accurate decisions.21,22 According to some academic research reports, decision support systems could provide medical staffs with quick and appropriate suggestions for various clinical symptoms and exceptional testing results. These systems could bring more useful information to healthcare providers so that they can make better decisions.1,3,4,23,24 The main function of decision support systems is to support users and provide relevant information. The results generated by the systems are not necessarily in a particular format but may vary with user inputs. The system database is established initially based on the users’ professional knowledge and experiences. 5
Artificial intelligence technology
Nursing informatics has been developed over recent years as IT has become prevalent in applications to nursing practices. Its purpose is to create a nursing-practice-oriented recording model that is patient-centered. The model is expected to develop empirical nursing information through the support of artificial intelligence technology and to facilitate nursing care in order to establish clinical nursing guidance for various kinds of patients. 20 Thus, if its algorithm can be effectively applied to nursing practices involving patient care and for judging work priorities, it could be of great help to healthcare providers. 21 Artificial intelligence deals with the exploration, study, and design of machines and equipment that simulate human behaviors. These machines and equipment demonstrate human or near-human intelligence and can think, operate, and use their intelligence functions much as people do. As the serial processes of artificial intelligence are similar to the way in which human neurons function by delivering and interpreting messages, machines using artificial intelligence are also called artificial neural networks. 25 At present, the most popular and representative learning model is a back-propagation neural network (BPN), in which training data are input during learning sessions so that the weights in the network can be incessantly adjusted during the learning process. After the learning process is finished, each input of data into the network can bring immediate effective responses.26,27
Previously, BPNs were often used to analyze and determine commercial cases. In recent years, the techniques of artificial neural networks have been widely applied in medical decision-making processes. According to research findings, the application of BPNs could enhance the accuracy and consistency in determining the triage and acuity scale in the emergency department. 20 In forecasting medical caring models of discharge planning services, the use of artificial intelligence techniques could help doctors to appropriately identify the appropriate care facilities for patients after their discharge. 28 A research study developed an online enquiry and diagnosis system that adopted an adaptive-network-based fuzzy inference system (ANFIS) to test the classification of diabetes and metabolic syndromes. It further determined patients’ risk of getting diabetes and its severity according to their biochemical test results and lifestyles. This system proved to be valuable for the medical staff, assisting them in making better clinical decisions as well as in discovering and treating diseases preemptively.7,29
Methodology
Study process and framework
In this study, we constructed a predictive model based on the Cross-Industry Standard Process for Data Mining (CRISP-DM). The model construction involved the following stages: (1) The major data resources used were charts from patient hospitalizations in the same medical specialty over the last year. (2) The data used were then preprocessed. Preprocessing included the screening, deletion, and regularization of information to reduce the effects of noise and incomplete data that might affect the accuracy of the prediction model developed by this study. (3) Factors that might affect nursing diagnoses were investigated based on relevant literature, which was followed by selection of primary discriminating factors from patient files to be integrated as input variables. (4) The K-fold cross-validation technique was applied to group samples into K subset clusters. K-1 groups were used as training groups and the remaining group was used as a testing group to test validity. Then another group was chosen as a testing group with the remaining K-1 groups as training groups. Mean accuracy of the analysis model was averaged after 10 rounds of testing. (5) Prediction models were constructed and the best model from various trial models was selected through comparisons of model accuracy (Figure 1).
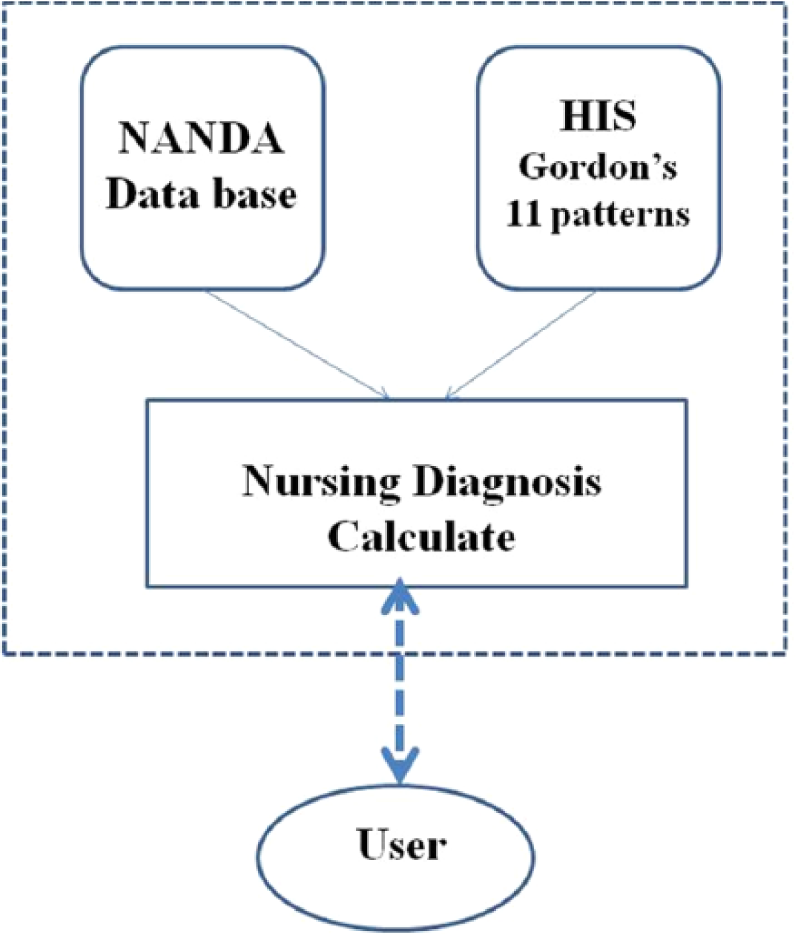
System framework.
Data collection
We first reviewed 216 medical records from 105 patients discharged from the hospital, and we used Gordon’s 11 functional health patterns (Figure 2) to make a comparison with the system according to the established nursing diagnoses prepared by clinical nursing staff members from June 2011 to March 2012. Senior nurses with at least 4 years of clinical experience were qualified to serve in the main assessor roles. With this sample size, analysis results were more reliable and had reference values. Data from each patient were keyed into SPSS software with 26 fields including coding, age, gender, symptoms (a total of 18 fields), and nursing diagnosis (a total of 5 fields). Data from all the fields were keyed into SPSS software for further analysis.
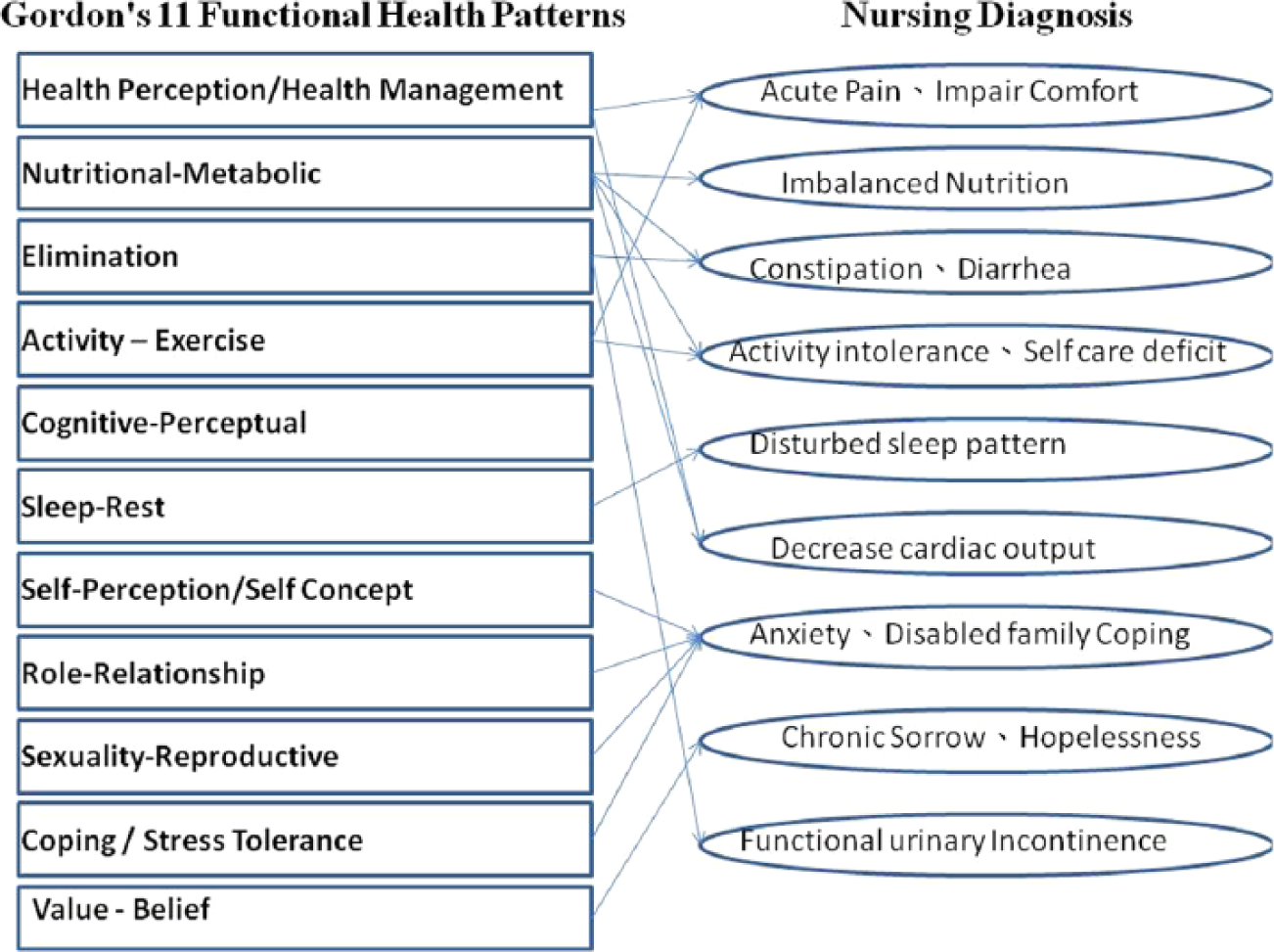
Diagram of Gordon’s 11 functional health patterns with various nursing diagnoses.
Experiment
In this study, we used IBM SPSS, the decision tree in Clementine 12.0, a BPN, and the ANFIS in MATLAB as the analysis tools for data mining and statistical analysis. We first used the decision tree and clustering algorithm to find important factors and association rules that could be used for nursing differential diagnosis. We divided the test samples into two groups. One group served as a training sample and the other as the test sample to test the accuracy of the rules. We further compared the prediction accuracy of the previous methods with the ANFIS and the BPN.
Decision tree
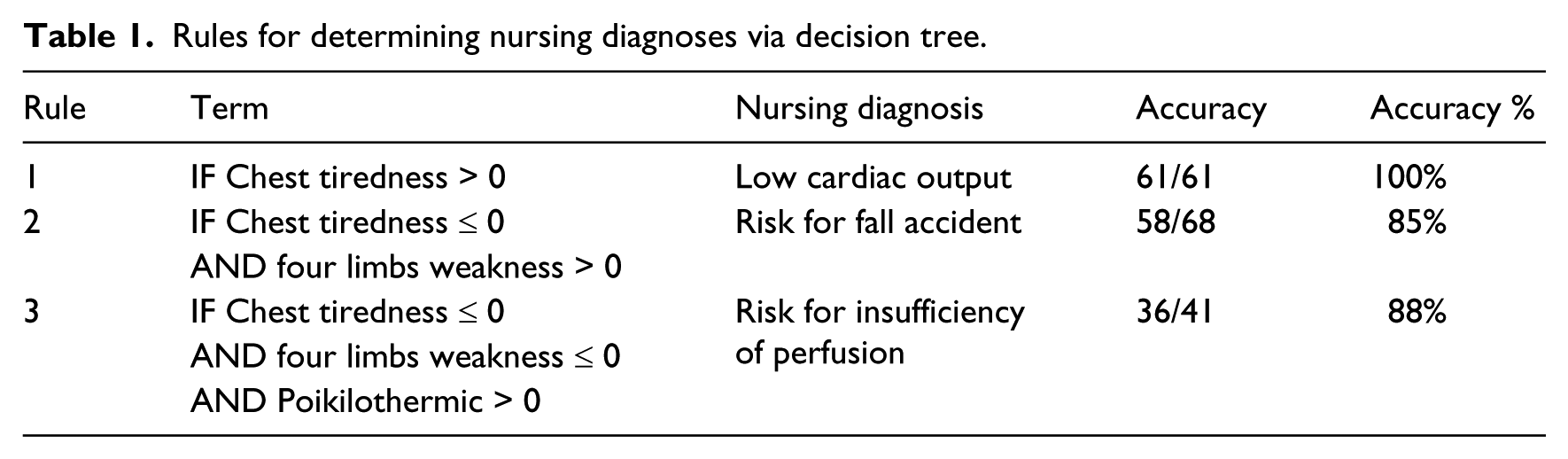
First, SPSS was used to import raw clinical data to Clementine for computing the distribution of each variable of the raw data. For the factor selection, principle component analysis was used to filter out unimportant properties. The decision tree of the data mining techniques was used to construct the classification model. We obtained the error rate from the tree diagram and decision tree by generalizing five common nursing problems and 18 factors (symptoms and signs) related to those problems out of the 216 nursing diagnoses in the training and testing groups and bringing them into the decision tree algorithm. The total error rate for the decision tree algorithm was 12 percent, indicating that the accuracy rate of recognition was as high as 88 percent (Table 1).
Rules for determining nursing diagnoses via decision tree.
BPN
As for the model structure of the BPN, it consisted of a single hidden layer that could provide sufficient accuracy. Therefore, there will only be one hidden layer in the constructed BPN. Because the input layer consisted of quite a number of neurons, we set two neurons in the hidden layer to conduct the testing. The final network output layer consisted of only five neurons: acute pain, discomfort, activity intolerance, self-care deficit, and decreased cardiac output. As for the network parameter setting, we set the learning rate to be 0.2 because we could not get convergent results with a learning rate larger than 0.3. As for the network training guideline, the training termination condition was when the root mean square error (RMSE) was lower or equal to 0.0001 or at most 1000 times training repetitions.
ANFIS
In this study, we used the equation rule in the ANFIS to predict the accuracy of the next nursing diagnosis (Figure 3). MATLAB codes were written to analyze the collected data. ANFIS is an extension of the fuzzy inference system (FIS). ANFIS combines neural network principles and fussy inference principles to construct a network inference model that is a supervised FIS. ANFIS is useful in adjusting optimal parameters to achieve the best predictive effects. As we have already seen, fuzzy systems present particular problems to developers. The if-then rules have to be determined somehow. This is usually done through “knowledge acquisition” from experts, which is a time-consuming process that is fraught with problems (Figure 4; equation (1)). A two-rule Sugeno of ANFIS has rules of the form


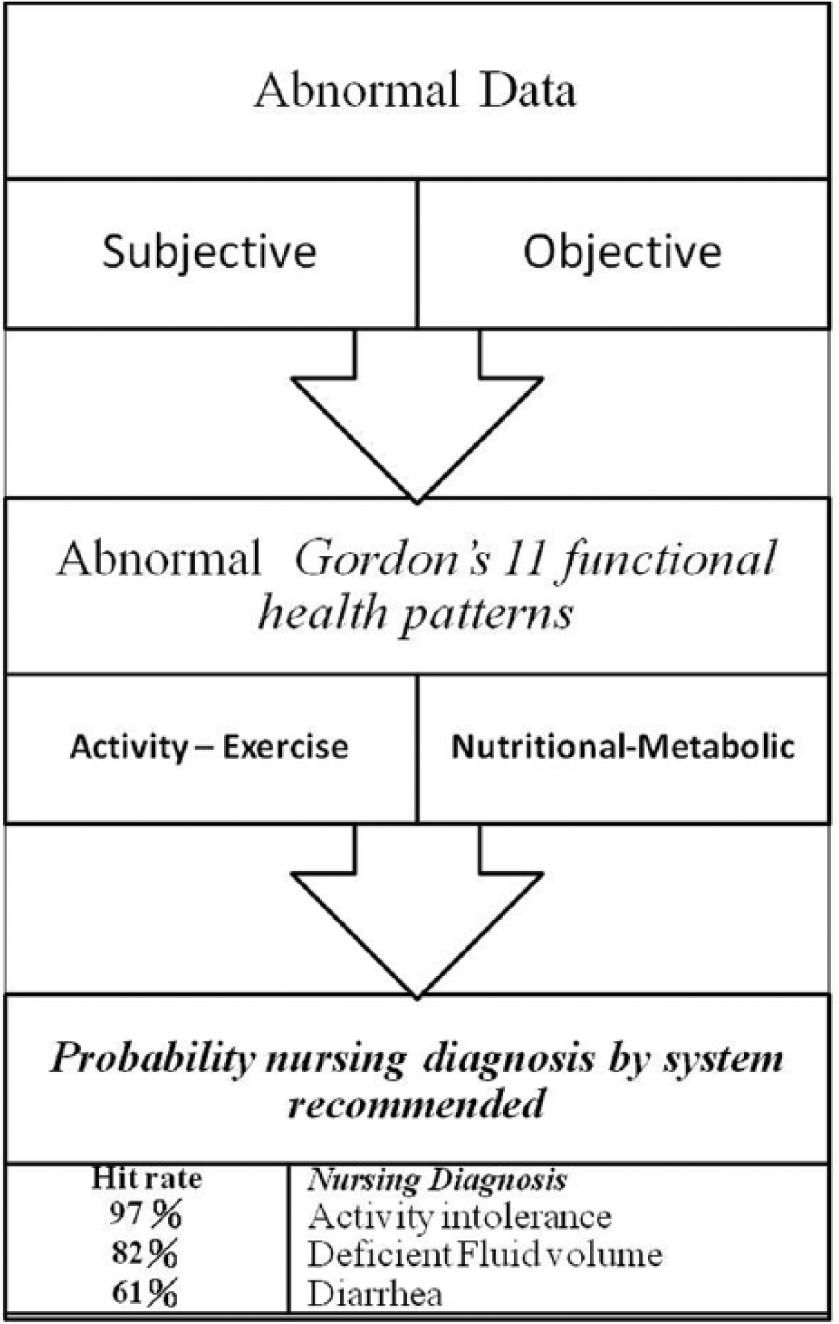
Probability diagram of the nursing diagnosis.
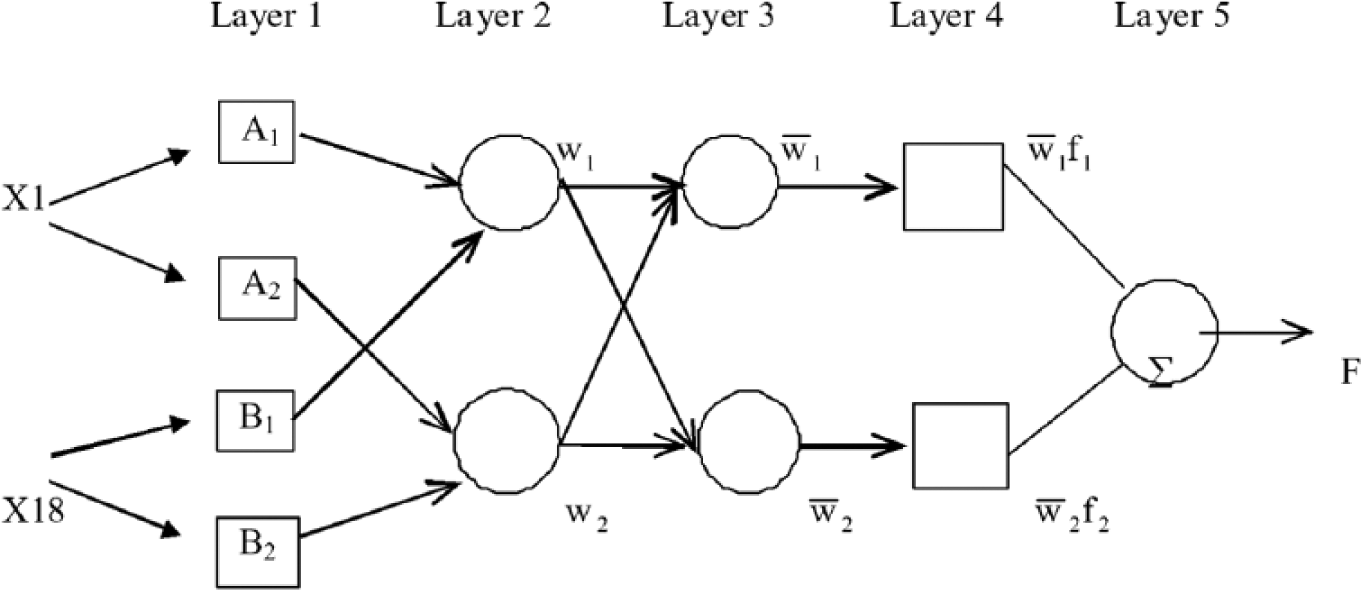
ANFIS architecture for a two-rule Sugeno system.
Clinical trials
This study conducted clinical testing at two healthcare units in one teaching hospital in northern Taipei. The nursing staffs received a 3-month-long training session before the implementation of the system. Then, the preliminary experience was explored and shared 3 months after the implementation.
Using the English version of SPSS 20.0, we analyzed the basic data to identify the differences in the questions and in the nurses’ satisfaction levels before and after using the nursing information system. We also conducted paired t-tests to check whether significant differences exist. A p value less than 0.05 was defined as statistically significant. Moreover, we developed a questionnaire as part of our research method. The questionnaire included two major parts. The first part was concerned with basic information, and the second was about question establishment and satisfaction scoring. The basic information questions included items on age, education, seniority, and basic computer skills (Word, Excel, and PowerPoint). To confirm the questions’ validity, we compared the questions raised by the nursing staffs and the ones suggested by the systems, and then the nurse leaders assessed their accuracy. For satisfaction scoring, the survey adopted a 5-point Likert scale (1 = very unsatisfactory, 2 = unsatisfactory, 3 = near satisfactory, 4 = satisfactory, and 5 = very satisfactory). Among the three units tested using the questionnaire, a total of 36 nurses have used such a system. The statistical result showed a reliability coefficient α of 0.83.
Results
Descriptive analysis
For the 105 cases collected, most of the patients were males with an average age of 51 ± 2.53 years. Among the 11 functional health patterns, health perception, nutrition, activity, and sleep–rest were found to be statistically significant influencing factors. Among nursing diagnoses, acute pain, discomfort, and activity intolerance were most common. The average age of the 36 nursing staff members was 28.92 ± 4.02 years, and the average work experience was 5.95 ± 1.8 years. Half of the nurses were university educated and the other half were college educated. They all have good self-perceptions of their computer operation skills (Table 2).
Basic nursing staff information (N = 36).
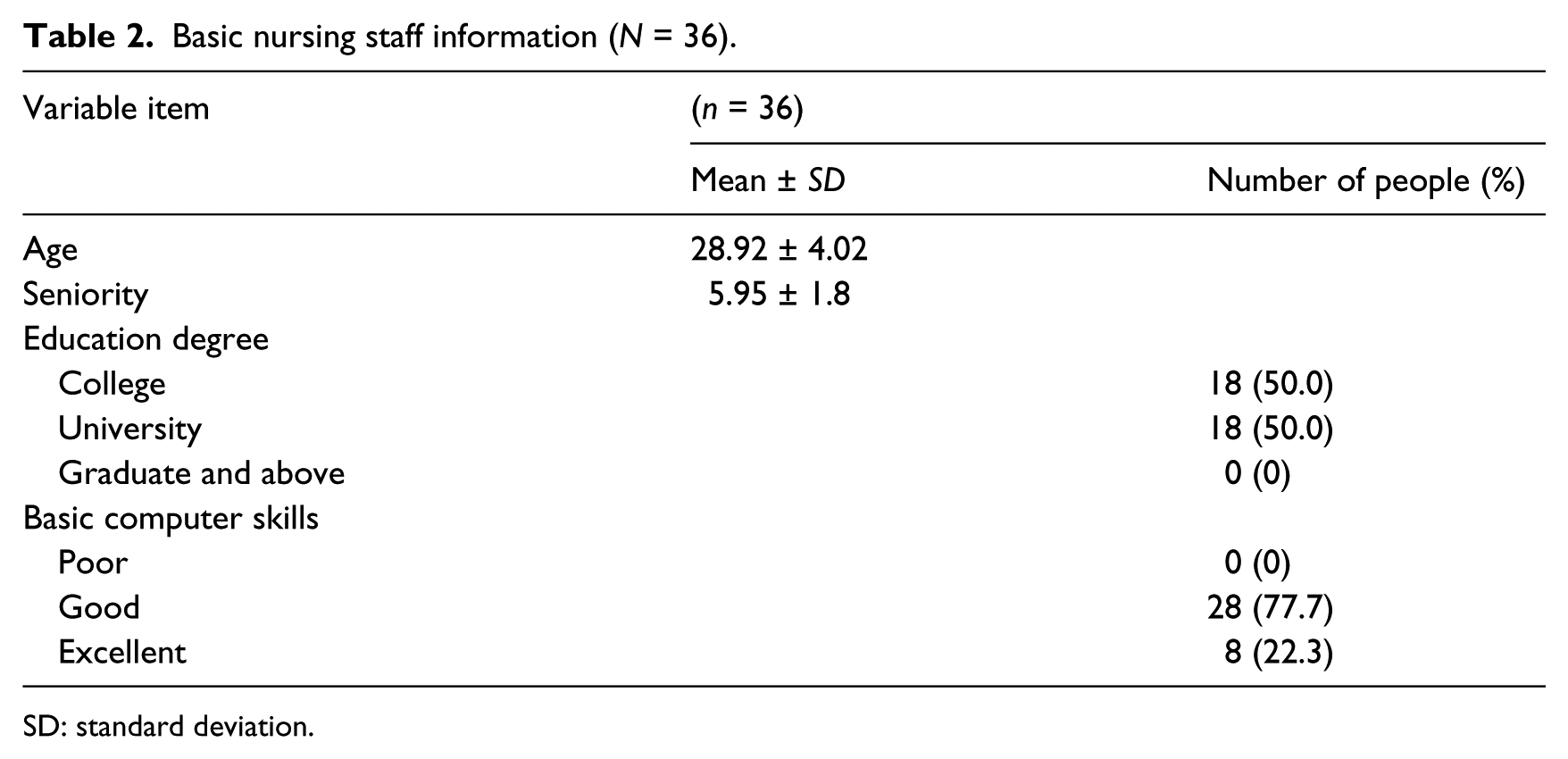
SD: standard deviation.
Comparing different prediction models
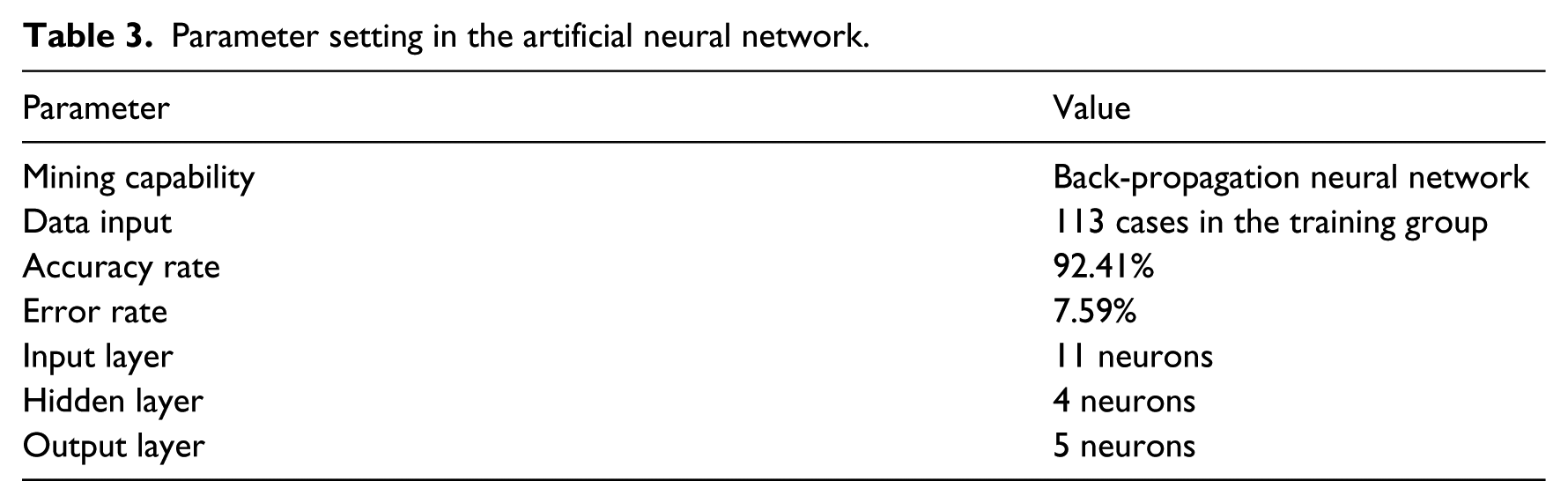
We used the BPN testing by SPSS Clementine 12.0 to determine the hidden number of neurons and the learning ratio α. The BPN included only one hidden layer, and the input layer included 18 neurons. Therefore, the numbers of neurons in the hidden layer were set at three, five, seven, and eight for running the tests. Finally, the output layer of the network included five neurons with a final accuracy rate of 92.41 percent and an error rate of 7.59 percent (Table 3).
Parameter setting in the artificial neural network.
We generalized 18 possible factors related to 5 common nursing diagnoses out of 108 cases and then put the 216 nursing diagnoses into training and testing groups. The ANFIS model in MATLAB was used to verify the accuracy of the clinical diagnoses. The ANFIS adopted in this research yielded a final accuracy rate of 84.82 percent and an error rate of 15.18 percent.
Effectiveness of artificial intelligence technology
We selected only the first three targets generated by the BPN as our first choices in screening the problems of nursing diagnoses. When consolidating the 18 related factors that could affect the nursing diagnoses, we created a forecasting model of the BPN for the 123 sets of training data by using the Clementine software and then used 93 sets of patient data for testing purposes. After using Clementine to determine the accuracy of the aforementioned training data, we achieved an 87.41 percent accuracy rate in predicting patients’ nursing diagnoses.
This nursing information system can enhance the capability of nurses to provide accurate nursing diagnoses. We conducted a clinical test in one teaching hospital in northern Taipei by collecting 54 medical records that were reviewed by senior nurses. The percentage of nursing diagnoses suggested by the information system that coincide with those made by the nursing staff over the total samples is as much as 87 percent. The percentage of the nursing diagnoses made by both the system and the nursing staff that are concurrently in the top three possible results over the 54 samples is 74 percent.
The nursing information system could also improve the job satisfaction of nurses. Results showed that overall patient healthcare was improved, work satisfaction concerning nursing diagnoses was enhanced from 41.1 percent to 75 percent, and the time spent on decision-making was reduced from 35.5 to 19.8 min (Table 4).
Satisfaction and time spent for the forecasting method.
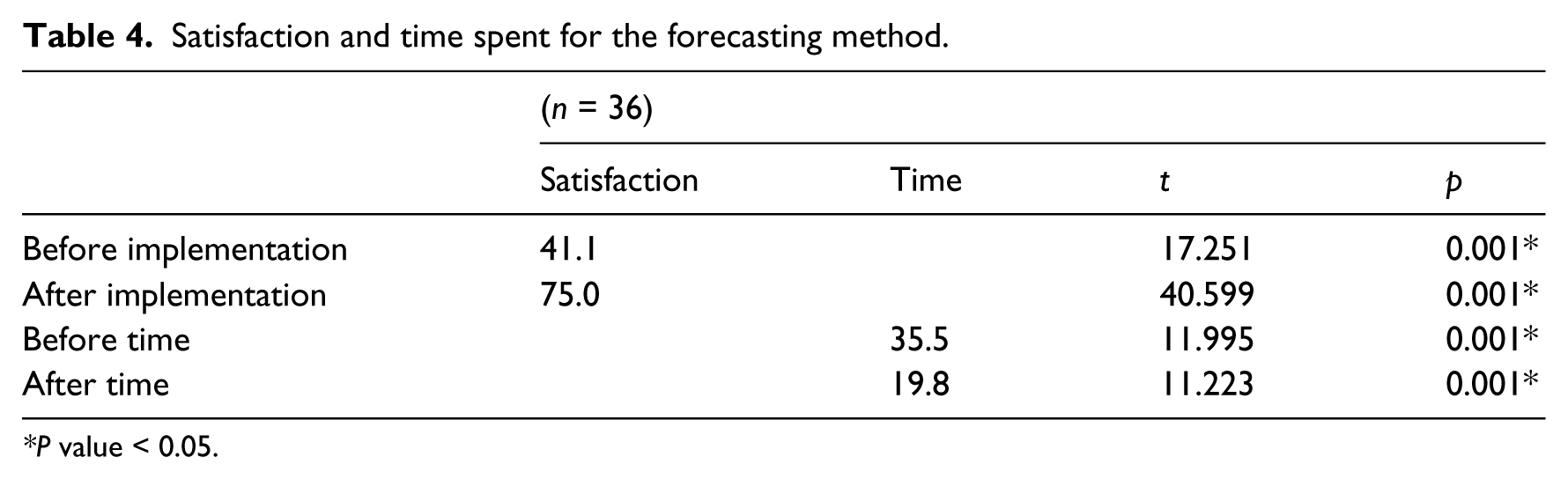
P value < 0.05.
Conclusion
In this study, we used Gordon’s 11 functional health patterns to predict common nursing diagnoses of similar symptoms. Our results showed the best outcome resulted from using a BPN, which was followed in terms of effectiveness by an ANFIS model. This model can effectively derive the differential guidelines for nursing diagnoses of similar symptoms to assist nursing staffs in making nursing diagnoses. Subjective cognitions and judgments on the part of nursing staffs can be reduced to decrease unnecessary working time and to increase the accuracy of nursing diagnoses. The system initially established Gordon’s 11 functional health patterns, and an ancillary system was included for formulating nursing diagnoses. So, the nursing staff on the front line could record information simply by using touch panels. This would reduce the chances of missing major points when completing records, which would not only enhance the accuracy of data disclosure but also improve the quality and timeliness of responses to patients’ health issues.
According to this research, the most common problems that occur when IT people communicate with nursing staffs result from the differences in the languages they speak, the knowledge they have, and the values they hold. If we employ users’ experiences and repeat the software development process, along with creating a common language for both groups to use, the communication barrier in developing the software would be reduced. The results show that IT could enhance the accuracy of collecting and recording data. We suggest that future studies monitor data for a much longer period, say, 6 months to 1 year.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.