
Abstract
With the increasing nationwide emphasis on eHealth, there has been a rapid growth in the use of the Internet to deliver health promotion interventions. Although there has been a great deal of research in this field, little information is available regarding the methodologies to develop and implement effective online interventions. This article describes two social cognitive theory–based online health behavior interventions used in a large-scale dissemination study (N = 866), their implementation processes, and the lessons learned during the implementation processes. The two interventions were a short-term (8-week) intensive online Bone Power program and a longer term (12-month) Bone Power Plus program, including the Bone Power program followed by a 10-month online booster intervention (biweekly eHealth newsletters). This study used a small-group approach (32 intervention groups), and to effectively manage those groups, an eLearning management program was used as an upper layer of the Web intervention. Both interventions were implemented successfully with high retention rates (80.7% at 18 months). The theory-based approaches and the online infrastructure used in this study showed a promising potential as an effective platform for online behavior studies. Further replication studies with different samples and settings are needed to validate the utility of this intervention structure.
Introduction
In recent years, the Internet has become an integral part of people’s lives. In 2014, 87 percent of American adults were Internet users, 1 and more than 90 percent of them accessed the Internet to find information and to communicate with others. 2 With this trend, there has been national and global emphasis on expanding the use of eHealth (i.e. use of information and communication technologies for health).3,4 Currently, an unprecedented amount of health information is publicly available in the Internet (e.g. the National Institutes of Health and the National Osteoporosis Foundation).5,6 Many laypersons, however, are either unaware of specific websites that can help improve their health or overwhelmed by the amount of information available. 7 Thus, there is great opportunity to improve dissemination strategies to effectively package and deliver the available online health resources to the public.
In addition to serving as a repository for health information, the Internet is now being used by consumers to complete health-related transactions (e.g. medication refills) and by clinicians to deliver specific health interventions, such as health promotion,8,9 caregiver support, 10 or other therapeutic interventions. 11 Compared with face-to-face interventions, online interventions have unique additional benefits, such as the ability to reach out to large numbers of individuals and to distribute uniform interventions to multiple sites.12,13 Participants can use the interventions at their convenience. The effectiveness of eHealth interventions on health behaviors (e.g. diet, exercise, weight) has been demonstrated previously.14,15
Many health-related online intervention trials have also been conducted to assess effectiveness of different interventions.16–18 Various software programs are currently available to develop and to implement online interventions, and investigators use different approaches to deliver online interventions and maintain communication with their participants. Systematic reviews of eHealth studies have addressed inconsistencies in the interventions and design of those studies.19–21 Despite the large body of literature, in the eHealth area,22–24 there is a paucity of research that investigates effective approaches to the development and the implementation of online health interventions.
In a recent online dissemination study (N = 866), our investigative team assessed the impact of two online theory-based bone health programs on selected health outcomes of older adults including osteoporosis knowledge, self-efficacy and outcome expectations for calcium intake and exercise, and the behaviors of calcium intake and exercise. The two interventions were an intensive short-term 8-week online Bone Power program and the same Bone Power program followed by a 10-month booster intervention (biweekly eHealth newsletters with follow-up of each participant’s bone health behaviors) (Figure 1). In this trial, we are particularly interested in extending a short-term intensive online behavioral intervention, which has shown some effectiveness,10,25 to a longer term intervention by adding a booster intervention. As compared to face-to-face health behavior interventions, online interventions tend to be shorter than 6 months. 19 There has been a lack of studies that address the effects of booster interventions in online behavioral studies. The purpose of this article is to describe the development and implementation of the two theory-based online behavioral interventions used in our study and the lessons learned during those phases.

Sample screens of Bone Power website and the eHealth newsletter.
Theoretical framework
The development and implementation of the interventions were guided by social cognitive theory (SCT).26–28 The effectiveness of SCT on individuals’ health behavior changes has been demonstrated in both face-to-face and online behavioral studies.29–32 SCT addresses several pertinent factors that can influence individuals’ behaviors, including motivation, self-efficacy, outcome expectations, and goal setting. For example, individuals’ goals are important in motivational mechanisms and guide their health behaviors.26,27 A person’s belief in his or her ability to carry out a behavior (self-efficacy26–28) and the benefit of the behavior (outcome expectations26–28) promotes a person’s health behaviors. Efficacy beliefs can be enhanced through the following mechanisms: 31 (1) enactive mastery experience (i.e. through one’s prior successful accomplishments of planned behaviors), (2) vicarious experiences (i.e. through modeling others’ successful performances), (3) verbal persuasion (i.e. through verbal encouragement given), and (4) physiological and emotional states (i.e. through enhancing physical status (e.g. pain relief), reducing stress, and negative mood). Table 1 describes the application of the theory to the development and implementation of online interventions.
Application of SCT in the intervention development and implementation.
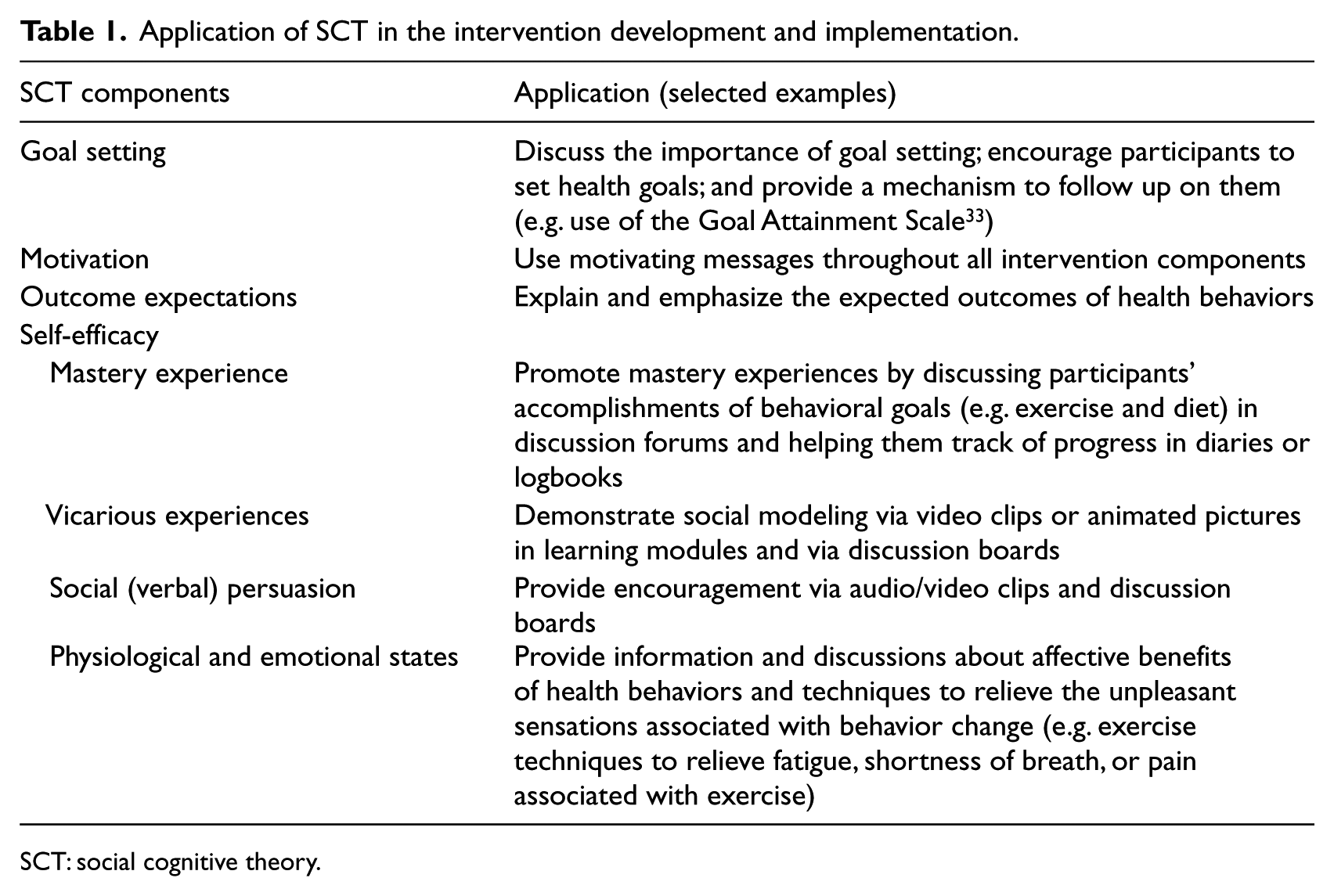
SCT: social cognitive theory.
Discussion boards can be particularly helpful in applying SCT to trials, as they can provide settings where participants can interact with others and voice their thoughts.10,18 To facilitate participants’ interaction, this study used a small-group approach in which approximately 20 participants began the trial concurrently (each intervention group had its own Web intervention site). Throughout this trial, we randomized participants to a total of 48 groups, in three cohorts (two interventions and no-intervention control). To manage the group structure, we used an eLearning management program as an upper layer of the study’s Web infrastructure.
The study and sample
This study was a three-armed randomized controlled trial (RCT) with five waves of data collection (baseline, 8 weeks, 6, 12, and 18 months). Individuals were eligible if they were 50 years or older, had access to the Internet/e-mail, could use the Internet/e-mail independently, and could read and write English. Participants were recruited from two large online communities (SeniorNet 34 and MyHealtheVet 35 ), in which a brief description of this study and a hyperlink to the study’s website were posted. The screening and consenting process were completed online. Individuals who met all eligibility criteria and agreed to participate in the study were placed on a waiting list. Once approximately 60 participants were available on the waiting list, they were contacted to complete the online baseline survey. Upon completion of the survey, participants were randomized into three groups, Bone Power, Bone Power Plus, and Control, and the intervention group participants started using the interventions. At the end of the recruitment phase (30 November 2010 to 9 July 2011), a total of 866 participants were randomized into three cohorts (Bone Power, Bone Power Plus, and Control), each consisting of 16 groups. (In this study, a group consisted of those participants who were randomized into a condition at the same time. A cohort is defined as a collective set of participants in each condition at any given time point of the trial.)
Table 2 summarizes the selected demographic characteristics of participants. More than half (63.4%) of participants were male, with a mean age of 62.8 ± 8.5 years. The majority of participants were White (89.6%) and 7.4 percent were Black. More than half (52.7%) were married. The majority (87.2%) had some college or higher level of education. More than half of participants (56.5%) reported having high blood pressure, 24.7 percent reported having diabetes, and 23.3 percent reported having osteoporosis. The majority (83.6%) reported their level of computer knowledge as competent or higher, and 17 percent reported having some difficulty using a computer due to arthritis in the hands. The average number of years of Web experience was 14.5 ± 6.6, and the mean amount of time spent using the Web was 15 ± 13.8 h per week. The average level of eHealth literacy assessed by the eHealth literacy scale developed by Norman and Skinner
36
was 30.9 ± 6.0 (range: 8
Characteristics of participants.

SD: standard deviation; PC: personal computer; BP: blood pressure.
Bone Power program
The 8-week Bone Power program includes the following: (1) Web learning modules, (2) moderated discussion boards, (3) an Ask-the-Experts section, (4) virtual libraries, and (5) a health toolkit (see Figure 1 for selected screen shots). The Bone Power program had a total of 11 learning modules that can be grouped into three categories (Table 3): bone health core modules (Modules 1–5), condition-specific bone health modules (Modules 6–8), and general health promotion modules (Modules 9–11). Some parts of the learning modules (e.g. exercise, fracture prevention, calcium-rich diet) had been developed and tested during our previous grant projects.9,10,37 The modules were developed by an expert panel that included a geriatrician who had expertise in osteoporosis, a geriatric nurse practitioner, physical therapists, and gerontology researchers. The experts used SCT as a guiding framework in the development of the content. Each module comprises specific learning objectives, structured learning content (for fundamentally important content) with external Web links to other relevant health sites (for further information), and self-assessment quizzes.
Learning modules and topics.
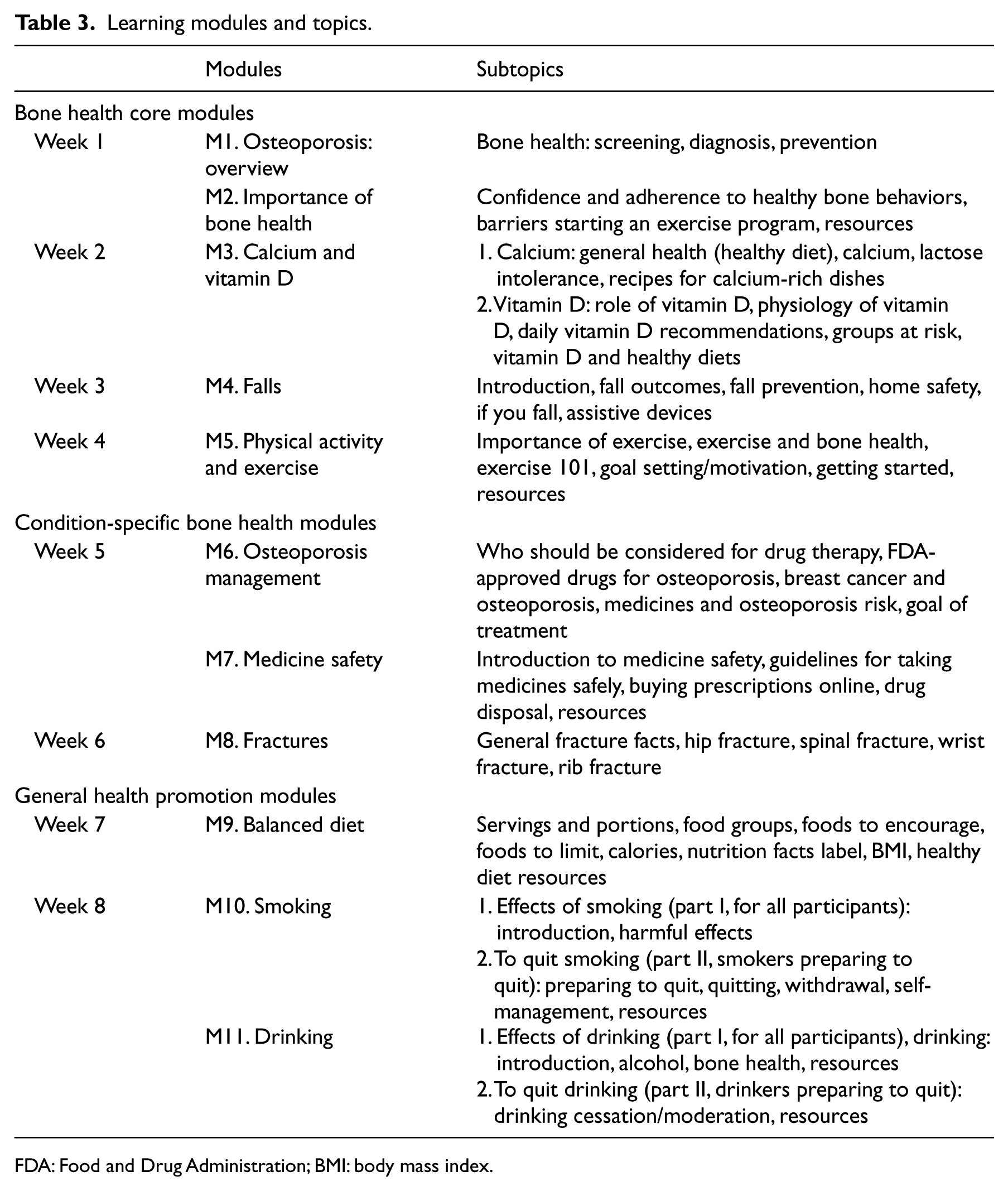
FDA: Food and Drug Administration; BMI: body mass index.
In an effort to disseminate evidence-based health information, the content of the online program included established health and practice guidelines,38–40 hyperlinks to credible health websites, and various health tools (e.g. bone mineral density (BMD) calculator, Fracture Risk Assessment Tool (FRAX®)), 41 and interactive health trackers (e.g. SuperTracker 42 ). Our expert panel members also developed short lecture video clips on selected topics (e.g. fall prevention, FRAX®, 41 BMD demonstration). The content of those lectures was based on our experts’ research findings, which was consistent with the aim of this dissemination study.
Biweekly eHealth newsletters (Bone Power Plus program only)
The eHealth newsletters, which started after the 8-week Bone Power program, were delivered via e-mail for 10 months every other week. These newsletters were developed based on SCT and included content that highlighted major health topics in the learning modules, recent research findings on a selected topic, calcium-rich recipes, and health tools (or short video demonstration clips). They also included other fellow participants’ success stories. An interactive goal attainment form was included in every other newsletter to encourage participants to continue following up on their health goals.
Online intervention platform
The password-protected intervention website was developed by the University of Maryland School of Nursing research Web development team, who developed the Web programs for our prior studies.9,10 To effectively manage multiple groups of participants that started the 18-month trial at different times, we used the Blackboard (BB) eLearning program 43 as an upper layer of the Web architecture. The BB program has been frequently used for higher education43–45 and tends to have busy user screens that include various functions (e.g. various tools). The original BB user screens were significantly modified to simulate regular Web pages (Figure 1). The Web pages for learning modules were developed using Adobe Dreamweaver 46 and Flash, 47 following the Web development guidelines developed by National Institute on Aging (NIA) guidelines.48,49 In consideration of the online study targeting older adults, special efforts were made to provide user-friendly tutorials for the program. In addition to a text-based introduction, we developed a short video tutorial using Camtasia Studio® 50 to demonstrate how to use the online intervention components.
Asynchronous discussion forums were developed using the BB discussion board function. A new discussion forum was deployed weekly for 8 weeks with each new learning module(s). The program also had an Ask-the-Experts function. Participants could submit their questions using interactive Web forms. The project manager (PM), who was a seasoned registered nurse and is familiar with online trials, managed the participants’ enquiries consulting with the expert panel comprising a nurse practitioner, physician, dietician, and activity expert. Participants were referred to their own health care providers for specific questions about their personal health conditions. The virtual libraries included articles and Web links recommended by the expert panel and our investigators’ relevant research findings. The content was grouped by topic and module.
The eHealth newsletters were developed using XHTML and sent via e-mail. Each newsletter was archived in a PDF format on the study website once it was deployed. Help Desk support was available throughout the study from 8 a.m. to 5 p.m. EST, Monday through Friday, via phone and e-mail. All study data were collected online. The surveys were developed using the Remark Web Survey® software, 51 which was used in our prior studies and has proven to be user-friendly, while maintaining appropriate levels of security for research projects.
Implementation of the interventions
Intervention groups
The Bone Power program was used by both intervention groups. During the 8 weeks, a new module and an accompanying discussion forum were deployed to each group’s website weekly, and participants received a weekly e-mail notification about their availability. Once the module and discussion forum were launched, they remained open on the program website. Module 1 (first week) was an overview about bone health, which included information on the national guidelines for exercise and calcium and vitamin D intake.42–44 At the end of the first week, participants in the intervention groups were asked via an online survey to review their baseline health goals and reset their goals as needed. The discussion board was moderated by the PM based on SCT. She monitored the discussion board daily to facilitate discussions and identify any untoward discussion postings. Some information in the virtual libraries was also referred to in the discussion forum. Beginning 2 weeks after completion of the 8-week online Bone Power program, participants in the Bone Power Plus group were sent theory-based newsletters via e-mail for 10 months.
Control group
No specific intervention was provided to the control group participants. To keep in contact with participants, a monthly e-mail was sent to inform them of upcoming follow-up surveys. At the end of the study (upon completion of all five surveys), the control group participants received a CD-ROM that includes all content in the Bone Power program and archived eHealth newsletters. This approach is consistent with our dissemination efforts. We ensured that the content on the CD-ROMs was current when they were sent.
Participants’ use of the program and current study progress
All participants (100%) in the intervention groups logged into the Bone Power program. Participants were encouraged to use the program at least once a week as new content was deployed weekly for 8 weeks. Participants’ weekly use of the program was monitored for each group as the groups were on different schedules. We expected more frequent usage for the core modules (Weeks 1–4) than the condition-specific and general modules (Weeks 5–8) as some modules (e.g. quit smoking) might have not been applicable to many participants. The majority (74.2%) of participants reviewed five or more modules. On average, 63 percent of participants in each group reviewed the new learning content each week for the 4 weeks (many participants logged into modules multiple days during the week).
The data collection was completed in February 2013, and the analysis of data is currently ongoing. Overall, the retention rates remained high. At 18 months, the attrition rate was 19.3 percent, which was better than originally projected (28%). Although much more analyses are still needed, some preliminary findings suggest significantly greater improvement in many outcomes in the intervention group (final outcome findings will be reported in the future).
Lessons learned during the implementation phase
During the trial, our investigative team has learned several important lessons in implementing a large-scale online longitudinal RCT with multiple small groups over an extended time period.
Content management in a multiyear online health behavioral trial
Unlike face-to-face trials, online interventions that focus on dissemination of evidence-based health information often incorporate external links to other credible health websites, such as existing national health guidelines.38–40 Those websites often undergo changes and revisions, and the links must be checked diligently. Although link-checker programs are available in the market, 52 these programs simply check that links are still pointing to active external Web pages. They do not verify the content of the Web pages (e.g. the content of active Web pages could be “This Web page is no longer available”). Thus, regular manual checking is necessary. In our study, we maintain a master database that includes all external links, which are mapped with specific intervention.
Federal health guidelines can also change. During our project, major changes occurred in the diet guidelines, including ChooseMyPlate (2011) 38 and Dietary Guidelines for Americans 2010. 53 Although the majority of the content was similar, many Web pages and graphics (e.g. Food Pyramid vs MyPlate) had to be updated to be consistent with the new guidelines. These changes resulted in a thorough review of the intervention content and revision of many Web pages, as the content was discussed in several areas of the learning modules and virtual libraries. These changes were communicated to the participants via e-mails and eHealth newsletters.
Recently, an increasing number of major health websites send e-mail alerts or periodic summary reports to the subscribers of their listservs or via other mechanisms, such as Really Simple Syndication (RSS) or Facebook. In an effort to maintain the most up-to-date health information, the principal investigator and the PM signed up for the listservs of the health websites included in the Bone Power program and regularly checked the websites.
Intervention development and management
Usability testing is a critical component in the development of online interventions.17,54,55 Upon completion, the program underwent extensive usability testing. The initial testing was conducted by experts who reviewed the program based on existing heuristics. 49 Then, the program underwent alpha testing by selected team members comprising Web developers, network engineers, clinicians, and volunteer community-dwelling older adults at their own locations using their own computers. The program was revised based on the findings. More rigorous usability testing was conducted with 10 participants who met the eligibility criteria for the trial. Each participant completed two separate sessions in their own homes using their own computers. Based on the findings, the program was further refined, and the final product was used for the trial.
In online intervention trials, investigators must consider the program’s technical compatibility with their participants’ computer and the Internet setup. With the advancement of technology, today’s consumers use different types of computers (e.g. Mac, personal computer (PC)), Web browsers (e.g. Google, Mozilla, Firefox), Web security systems (e.g. virus protection programs, pop-up blockers), and Internet service providers (e.g. Comcast, Verizon). In addition, software companies periodically deploy updated versions of Web browsers or plug-ins (e.g. Java™). Our online interventions were developed to be compatible with most of the available computer types and Web browsers. During this study, however, we learned the importance of ongoing testing of the program as new versions of Web browsers and plug-ins became available. For example, we found that some beta versions of Web browsers (few reported cases) could cause issues with a certain component of the BB program (posting discussion responses). The Help Desk was useful for early detection of these issues. Our research team had robust network engineer support and was able to mitigate these issues in a timely manner.
Use of an online learning management program
The online learning management program (BB) can be an efficient tool for online behavioral trials. In our study, the program was especially helpful in the management of multiple groups that started the intervention at different times. When a participant logged into the study website, he or she only saw his or her group intervention. The investigative team, however, could see all groups in the administrative view and easily follow up on each group’s progress in its intervention. The program also reduced staff workload significantly, as we could preload all learning modules and discussion boards and scheduled the weekly release dates for each group. In addition, the program had an efficient announcement function (e.g. all groups vs single group) and helpful reports that showed users’ activities in certain sections. (We used Google Analytics 56 to keep track of usage of individual Web pages.)
Theory-based approach and use of small groups in a large online trial
A small group–based approach in a large online behavioral intervention trial has several benefits. 57 It provides a more effective structure for managing interventions (e.g. periodic release of new learning modules) and follow-up on participants’ specific activities over the intervention period. Based on SCT, it is also important for participants to interact with each other to provide encouragement (e.g. a peer commented, Cutting back is not always easy, when you make the little slips it’s OK, you start again) and serve as role models (e.g. Wow, you are doing great! If I may ask, what tips do you have for fitting this into your schedule and what keeps you motivated?).9,58,59 Based on our prior online trials and extensive experience in teaching online courses,9,60 we placed approximately 20 participants in a group, which we found to be an appropriate number for the selected sample.
In online health promotion studies,10,17,60 it is important to have discussions moderated by qualified personnel (e.g. nurses) to ensure that the information posted by participants is not inaccurate. Furthermore, moderators can apply SCT to the discussions and encourage participants’ healthy behaviors. They can also refer to the content in the modules while facilitating the discussions.
Communication with participants
Availability of a toll-free number for questions and technical support has shown to be important in online trials, especially for older adult participants.9,10,17 Many participants also appreciated our monthly “stay-in-touch” e-mails (after the 8-week intervention), which included a thank-you note and the next activity for the study. In these reminders, we also asked our participants to inform the project team of any changes in their contact information. We found that this type of communication could be more important for the control group participants, as some participants might forget that they signed up for studies that last a long period of time.
Online trials face some challenges when e-mail is the main communication method, as e-mail addresses can change over time and some e-mails can be redirected to a “Trash” folder. In our study, 54 participants changed e-mail addresses during the study period (several changed more than once). Thus, it is important that investigators follow up with participants via phone when they do not receive responses via e-mail.
In addition to monetary incentives given upon completion of the 8-week and 18-month survey, we used small mementos at 6 months (a tote bag) and 12 months (a magnetic memo pad). Although these were very small in monetary value (less than US$2), many participants expressed their appreciation for sending them (e.g. thank-you e-mails from participants).
eHealth newsletters
When eHealth newsletters were sent to the participants via e-mail, it was difficult to determine whether participants reviewed the content. Some e-mail programs, such as MS Outlook, 61 have e-mail tracking functions, but not all e-mail applications or services support read receipts and users can generally disable the function or opt not to send receipts. To assess users’ perceptions of the newsletters, we conducted anonymous volunteer evaluations of the eHealth newsletters when each group received the first three eHealth newsletters. Based on the findings, the majority of participants did not have any problems opening the eHealth newsletters, and the level of knowledge included in the newsletters was appropriate (n = 94, 87% rated the level was “about right”).
Anecdotal reflections
Many eHealth trials employed a relatively shorter term intervention (6 months or less) with varying degrees of attrition rates (0%–83%).62,63 A recent systematic review report identified a lack of and the complexity of capturing usage information in eHealth studies. 63 The findings showed that the number of logins was the most commonly reported measure of adherence, followed by the number of modules completed. Previously, our investigative team had successfully implemented SCT-based interventions in other studies.9,10 These studies had shorter trial periods with shorter and less extensive online interventions (e.g. 11.3% at 3 months). 9 This study has expanded the content and the length of the interventions as well as the overall trial period significantly, and we were able to maintain a high retention rate and participants’ engagement (e.g. participation in the intervention and various qualitative comments).
Conclusion
Healthy People 2020 highlights the importance of using eHealth technologies, 64 which has become a vital component of health care. The Internet has shown to be a powerful tool that can be used to empower the public by disseminating important health information that was unprecedented in the past.65–67 In this article, we described two theory-based online health behavior interventions and their implementation processes. Both interventions were successfully implemented with high adherence and retention rates (80.7% at 18 months). In online studies, the infrastructure of interventions and the implementation methods are as important as the intervention content to achieve planned outcomes. To date, the infrastructure platform used for our study has shown to be effective in delivering theory-based online behavior interventions in a large-scale longitudinal RCT with multiple groups. Further replication studies with different samples and settings are needed to validate the utility of this intervention structure and improve the generalizability of the findings.
Footnotes
Acknowledgements
The authors would like to thank Dr Jay Magaziner for his participation and guidance throughout this project.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was funded by the National Institutes of Health (NIH)/National Institute of Nursing (R01 NR011296).