
Abstract
In an age where mandatory computer usage within clinical care settings is a non-negotiable term of employment, the amount of applications a provider must access to document care is rapidly increasing. Each application contains an associated username and password. The increasing frequency with which clinicians have to log in and out of different applications is a source of frustration for many healthcare professionals. Healthcare executives see lost productivity. Single sign-on with added computer application roaming capabilities on shared workstations is a viable solution for both the clinician and the organization. The aim of this study is to assess the effect of implementation of single sign-on technology with application roaming on shared workstations. This study focuses on the perception of satisfaction with the implementation of single sign-on technologies within a midsized integrated delivery health network’s five emergency departments. We contribute to theory with the following: (1) the development of a construct called facilitated technology interruptions, (2) validation of the construct facilitated technology interruptions, and (3) application of a quantitative method to test the relationship between facilitated technology interruptions and user satisfaction. We surveyed five emergency departments and proposed five hypotheses. We found the positive relationship between facilitated technology interruptions and user satisfaction; the positive relationships between effort expectancy and satisfaction, and effort expectancy and willingness to recommend; and the positive relationship between satisfaction and willingness to recommend. We did not confirm the positive relationship between facilitated technology interruptions and willingness to recommend. We conclude that single sign-on technology increases user satisfaction. Other organizations may use the findings from this study and perform pre–single sign-on versus post–single sign-on evaluations. In practice, single sign-on improved productivity and ensured compliance with the Health Insurance Portability and Accountability Act, minimization of errors, and disruption for critical work.
Keywords
Introduction
There has been a proliferation of healthcare-related applications and computer devices installed within healthcare settings, 1 such as emergency departments over the past few years. This increase in computer devices and the system applications accessed from the in-patient care settings is related to the expansion of the electronic health record (EHR), along with new regulatory requirements for electronic structured data reporting. Activities traditionally on paper are now frequently performed on computer devices, for example, documenting patient care assessments, treatments, and entering orders. 2 Other important tasks that require the use of computers in a clinical setting include accessing laboratory results, reviewing radiology diagnostic study images, looking up past records in the archived medical record, interacting with clinical decision support assistance tools and calculators and procedure and document libraries, along with a host of other tasks using niche applications specific to the hospital setting. 1 With every application implemented, there is TYPICALLY an associated username and password, OFTEN with a predetermined session inactivity timeout. 2
With every timeout or reactivation from a privacy mode screen saver, the end user is required to enter their associated application username and password. Care providers have become overwhelmed with the need to remember several user names and associated application passwords in order to perform patient care activities when interacting with the computer. 2 Research has identified that healthcare workers providing patient care have on average 12 different, unique login user names and passwords to ensure that the integrity of electronic healthcare data accessed remains intact. 3 Other healthcare information technology (IT) literature estimates this number to be closer to 20 login credentials per user. 3
A time study performed at a midsized integrated delivery health network (IDN) in Kentucky comprising five health systems found that the time and the dollars spent in 2009 within one of their five emergency departments utilizing traditional login methods and application timeouts to access an electronic tracking board required 14.26 h of lost productivity during the course of an 8-h shift, equating to US$588,600 over the course of a year. 4 The corporate IDN IT leadership forecasted a cost to their system in excess of 1 million dollars in lost productivity time within one emergency department when an electronic information system with Computerized Physician Order Entry (CPOE) was implemented. 5 Armed with these data and in advance of a system-wide emergency department documentation and CPOE implementation, the organization focused upon implementing a single sign-on (SSO) with roaming capabilities solution on all the shared computer workstations within their five emergency departments.
In this article, we built on prior literature and developed a construct called facilitated technology interruptions (SSO) and used a self-reporting instrument to validate the relationship between facilitated technology interruptions and user satisfaction. Using the results of the self-reporting instrument, we performed a series of analyses of variance (ANOVAs) to test the differences in effort expectancy, facilitated technology interruptions, satisfaction, and willingness to recommend on different roles and did not find a statistical difference between roles. We contribute to the literature with the following: (1) development of a construct called facilitated technology interruptions, (2) validation of the construct facilitated technology interruptions, and (3) application of a quantitative method to test the relationship between facilitated technology interruptions and user satisfaction.
SSO and computer roaming in healthcare
Single sign-on, or SSO as it is commonly referred to, is the ability to centralize the authentication process thereby allowing a user to access multiple independent applications without further login process requirements. Computer roaming is a complimentary capability that allows the user’s session to remain active, or “Hot,” while they move between shared workstations within a predetermined zone of networked devices.6,7 The ability to augment the SSO process with a second form of authentication, in this case an employee identification badge, can enhance the security of a reduced application authentication process thereby incorporating a tap of a badge in conjunction with entry of a password at the start of the shift followed by tapping in, over, and out of applications for the remainder of the work shift. 6
The goal of SSO authentication is to alleviate the burden and cumbersome process of utilizing different user names and passwords for independent applications, relieving the password fatigue, and reducing the time spent in the application authentication process. 3 SSO maximizes user convenience, promotes interoperability among applications, and recoups lost productivity time associated with the login process, while ensuring compliance with regulatory requirements such as Health Insurance Portability and Accountability (HIPAA) 8 —a long-standing mandate within the United States developed to assure electronic patient health information is protected and secure at rest and when in transition.
This is not unique to the United States. Similar rigorous legislation policy mandating patient protections requiring security and management of electronic patient data can be found outside the United States. In Canada, there is the Personal Information Protection and Electronic Documentation Act (PIPEDA) and in Australia the Health Records (Privacy and Access) Act of 1997. In Europe, the right to data privacy was heavily regulated and actively enforced as early as 1981 within the Council of Europe. In general, the European Union (EU) protection of privacy, including personally identifiable medical information, is more comprehensive than that of US privacy laws. Hiller et al. 9 made direct comparisons of US and EU medical privacy laws on the five Fair Information Practices Principles (FIPs) adopted by the Federal Trade Commission and other international bodies. They concluded that although US laws are increasing protections of personal health information, they are still limited in comparison to the EU.
Increasing numbers of hospitals and healthcare centers are adopting EHR systems with the goal of improving healthcare quality while potentially decreasing costs. These systems are presently undergoing greater scrutiny as models throughout the United States can be systematically evaluated.
The 2011 Leadership Survey Health Information Management System Society (HIMSS) ranks technologies involved with desktop virtualization and SSO within their Top Ten list of IT priorities for healthcare organizations as identified by IT leadership members. 10 Recent research indicates that approximately 36 percent of healthcare organizations in the United States utilize some form of SSO. 4 SSO solutions are now used in conjunction with National Health Service (NHS) Connecting for Health smart cards in the United Kingdom and the French la Carte de Professionnel de Santé (CPS) smart card. Additionally, this identity and access management technology can be found integrated within systems in Belgium, The Netherlands, and the Middle East. In 2011, Microsoft, partnering with GE Healthcare, created Caradigm, an international company formed with the core goal of enhancing data usage across the healthcare continuum to foster insight, collaboration, and best practice using clinical applications for population management. The core technology at the heart of the Caradigm business model is SSO technology used for identification and access management to make it easier for care providers to rapidly access secured patient data stored across multiple application platforms. This Microsoft–GE Healthcare partnership demonstrates the recognition of the need and commitment to streamline clinical workflow and the potential of the technology to expand beyond borders and become a ubiquitous presence with new-era clinical data access management.
Facilitated technology interruptions and satisfaction/willingness to recommend
It is well recognized that technologies deliver many benefits for people but at the same time can create interruptions at work.11–15 Interruptions as defined by Basoglu et al. 16 result in a disruption of work, which is interpreted as an interference to current activities outside of the control of the user, forcing the user to change gears and multitask, potentially impacting good decision-making. Unanticipated interruptions are viewed by people as nonproductive and anxiety provoking and can cause the user to have difficulty resuming a task. 17
Technology interruptions in the clinical setting can be the result of many factors that include connectivity issues, system downtime, unintended user misuse, and login issues.12,13 The aim of facilitated technology interruption technologies, such as SSO and computer roaming, is to improve negative disruptive impacts associated with traditional login processes into legacy and new applications 13 and to reduce the need for care providers to circumvent the system with workarounds while improving the user perception of increased productivity.12,13
This technology allows users to move from one workstation to another by tapping their identification badge without logging completely out of one station and restarting the login process at another. 6 HIPAA session timeouts and privacy screen protocols requiring reauthentication processes are also viewed by care providers as disruptive. The 18, intent of the HIPAA security policy is to ensure electronic patient data are secured and protected. 8 Facilitated technology interruption technologies meet mandated HIPAA requirements 12 by introducing two-form authentication mechanisms, and security privacy screen functionality without creating the perception care activities is interrupted by the login and logout process. 6
Many users complain of frustration due to the time spent daily logging in and out of applications.13,19 An observational study of user behavior when interacting with EHRs in emergency departments identified many complexities care providers potentially encounter when solutions are layered upon legacy applications, resulting in interoperability issues for care providers who then have a tendency to utilize self-developed workarounds and suboptimal ways to access these applications in order to provide care. 20
A recent study by Marie D’Costa-Alphonso and Lane 3 associated increased user satisfaction with the use of facilitated technology interruption technologies such as SSO. Constant logging in and out of system applications is viewed as an interruption 13 that causes frustration for the users, thus generating dissatisfaction. The implementation of SSO with computer roaming capabilities simplifies the login process and allows for extended uninterrupted workflow. 3 This extended uninterrupted workflow increases users’ satisfaction and increases the likelihood of users endorsing the facilitated technologies to others. We therefore propose the following hypotheses:
H1: Facilitated technology interruptions positively influence user satisfaction.
H2: Facilitated technology interruptions positively influence user’s willingness to recommend.
Effort expectancy and satisfaction/willingness to recommend
The use of these technologies and the agreement by an organization to commit time, money, and resources to the development and implementation of these technologies indicate a commitment by the organization to address and alleviate password fatigue and reduce the amount of time required to login during a work shift. Although computer usage is mandated, key underlying reason for the introduction of these new technologies is to improve ease of use and user satisfaction. 3 In addition to time and productivity savings anticipated with the implementation of computer roaming and SSO capabilities, of equal importance is the impact of this new technology in regard to ease of use, self-efficacy, and staff reactions and perceptions regarding these technologies.1,3 Ease of use was originally developed by Davis, 21 but in 2003, Venkatesh et al. 22 revised the ease of use construct as effort expectancy in their Unified Theory of Acceptance and Use of Technology (UTAUT) model. Joo et al. 23 concluded that the ease of use is a significant predictor for satisfaction. Users value the ease of use of the technologies and would speak highly for the ease of use feature of technologies. In this study, we used the synonym for ease of use—effort expectancy—to propose the following hypotheses:
H3: Effort expectancy positively influences user satisfaction.
H4: Effort expectancy positively influences user’s willingness to recommend.
Satisfaction and willingness to recommend have been of interest to management in many industries; satisfied customers are loyal customers. 11 In healthcare, satisfaction is one of the most widely assessed measures of hospital care quality. 24 The word-of-mouth literature provides prolific findings on the positive relationship between satisfaction and willingness to recommend. O’Holleran et al. 24 studied patient satisfaction after rotator cuff surgery and reported a significant relationship between satisfaction and a willingness to recommend the surgery to another. Lin and Hsieh 25 found that flexible, self-servicing technologies controlling space and time improve user satisfaction and increase the likelihood a user will recommend the technology to others. The technological characteristic of an environment, for example, technology availability facilitating and improving upon collaboration, influences the intent to use and recommend these capabilities to others. 26 Our hypothesis therefore is as follows:
H5: User satisfaction positively influences user’s willingness to recommend.
The present study
The aim of this study was to better understand the impact of SSO capabilities in conjunction with the ability for users to roam between multiple devices on ease of use and user satisfaction. This study analyzes factors affecting user satisfaction and willingness of users to recommend an SSO authentication approach on shared computer workstations. We tested the five hypotheses proposed above. The environment studied contains shared workstations set up with roaming capabilities and a small attached device designed for the users to tap their employee identification badge to gain access, take over another user’s sessions, or to end a work session on the shared device. This study entails a self-reporting instrument distributed to end users within the integrated delivery network’s emergency departments post-implementation of HealthCast technologies. 6 HealthCast technologies provide staff and providers the ability to move freely throughout the care environment while maintaining active application sessions, utilizing an SSO authentication process in order to reduce negative perceptions associated with login overload.
Key variables measured within the study instrument included effort expectancy, satisfaction, facilitated technology interruptions, and willingness to recommend these technologies to other healthcare providers working within emergency departments. Figure 1 shows our research framework. The theoretical foundations of our work are drawn from the technology acceptance model and consumer satisfaction theory in marketing.
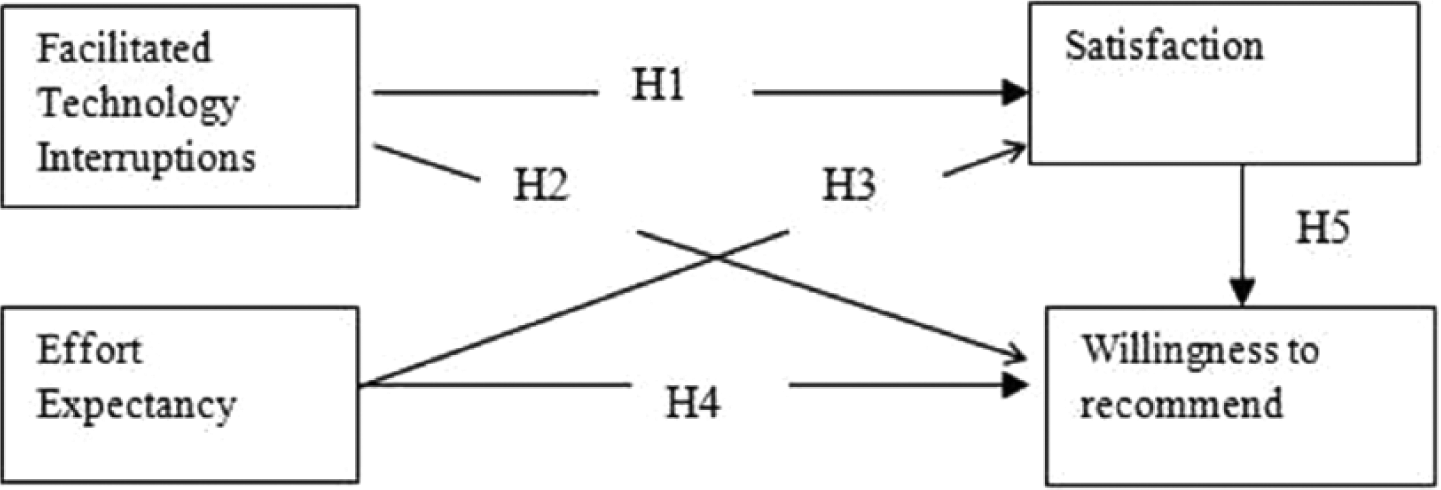
Research model.
Methodology
Sampling
A survey method was used in this study. The target population of this study is the end users who interact with the SSO software on computer roaming workstations within five emergency departments. The new reduced-login, desktop application roaming capabilities were introduced into the five emergency department environments in conjunction with the implementation of T-SystemEV, an electronic documentation and CPOE information system platform.
The study population includes physicians, allied health professionals, staff nurses, technicians, clerks, and department management. A total of 250 surveys were distributed to five emergency departments; a total of 177 completed surveys were returned, representing a response rate of 70.8 percent.
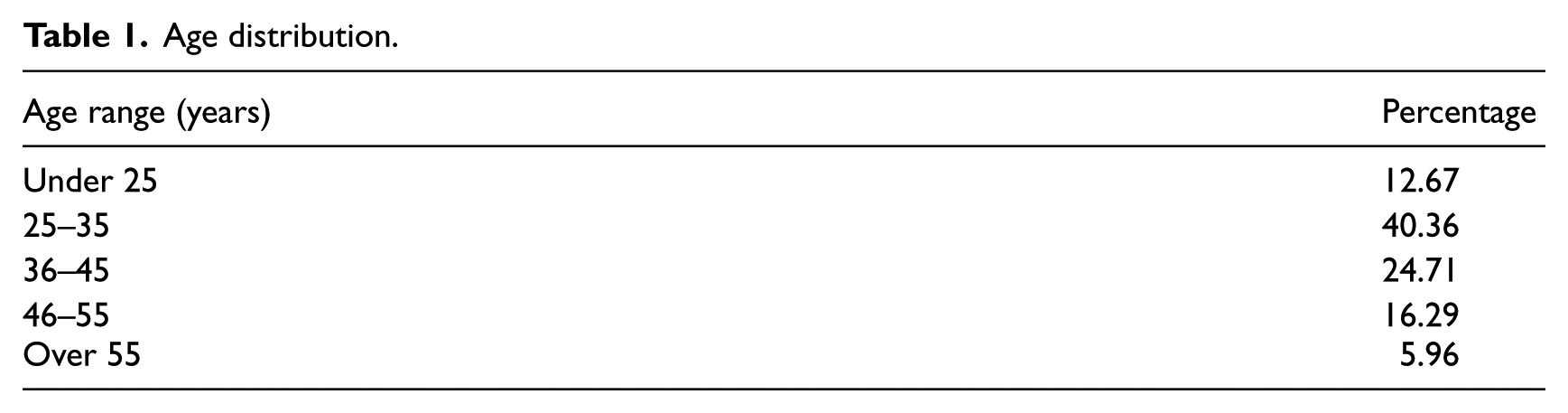
The self-reporting instrument was predominately completed by females working full time in the nursing role. The response rate for female was 69.5 percent and for male was 25.5 percent. Seventy-five percent of the respondents work full time, 25 percent are part-timers, and 7 percent are pro re nata (PRN) employees. Table 1 shows the age distribution of the respondents and Table 2 shows the role distribution.
Age distribution.
Role distribution.
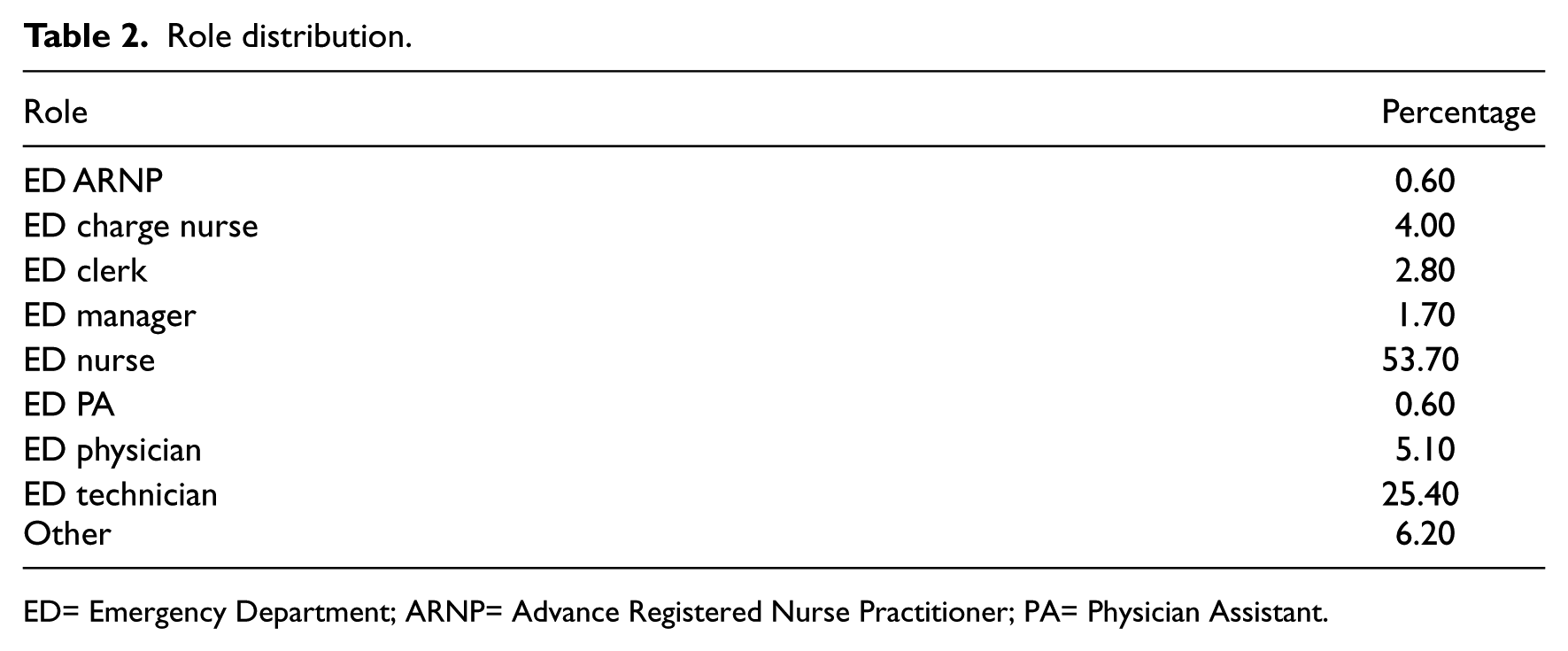
ED= Emergency Department; ARNP= Advance Registered Nurse Practitioner; PA= Physician Assistant.
Measures
We developed a self-reporting instrument consisting of 12 questions specific to determining staff opinions of facilitated technology interruptions, effort expectancy regarding satisfaction with SSO, and computer roaming technologies. We adopted and adapted measures from prior literature whenever possible. Among all the constructs used in this study, only facilitated technology interruption was self-developed. Based on the practical experiences, we deem three items are relevant and useful in evaluating the SSO impact. We asked members of the Corporate Clinical Informatics department to review and critique the appearance, sentence structure, and content of the self-reporting instrument and sought their feedback regarding the soundness and appropriateness of the instrument questions and assessment of the demographic section, and we worked with them to assure that the presentation of the questionnaire met the standards required by the healthcare organization. Table 3 shows the study constructs and the items associated with each construct. Each question was rated using the Likert scale with answer options ranging from Strongly Agree to Strongly Disagree on a rating scale of 1–7. A not applicable (NA) option was also listed. Demographic information gathered included age range, gender, job title, and work schedule.
Measures.
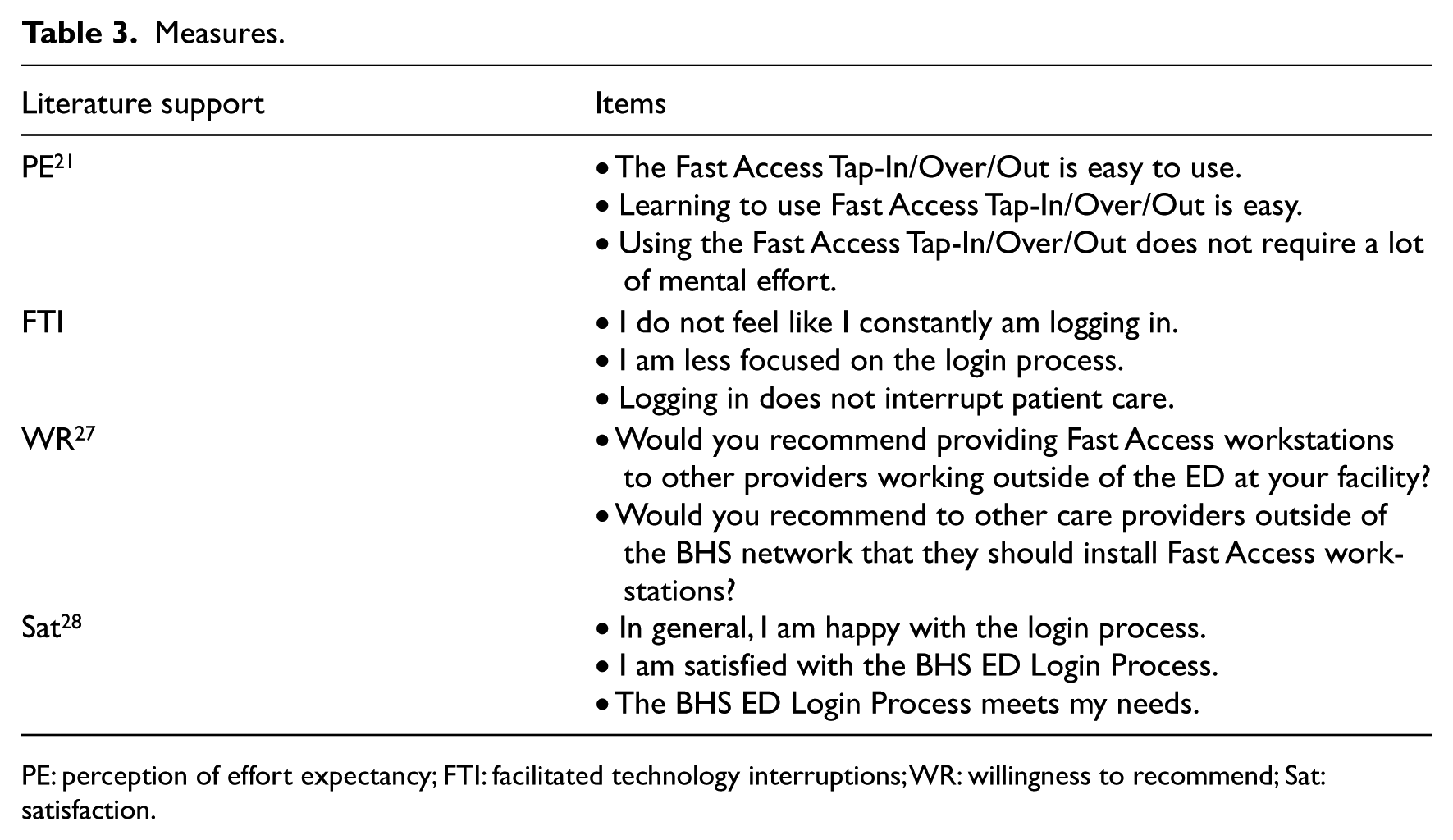
PE: perception of effort expectancy; FTI: facilitated technology interruptions; WR: willingness to recommend; Sat: satisfaction.
Procedure
The use, content, and distribution of the study survey instrument were approved by the organization prior to distribution. To facilitate emergency department participation, the emergency department directors from each of the five departments within the healthcare delivery network were recruited to assist with survey distribution, collection of surveys, and returning surveys. Each director received a study kit that included a box of chocolates for their assistance with the survey distribution process; preprinted surveys on yellow paper; bags of chocolates for distribution to each staff member completing the survey; and a prepaid, pre-labeled FedEx Overnight shipping envelope. The emergency department directors were advised to collect and securely store all completed surveys and to return them to the researcher on a predetermined date via the provided FedEx shipping envelope. The survey does not contain any user-identifiable information and survey responses are anonymous. All returned FedEx envelopes were delivered to the researcher on the same day.
Additionally, input from the emergency department directors included statements recommending the researchers to perform more research involving the use of IT within their departments. A theme emerged indicating that they value research and support future research endeavors.
Returned surveys were securely stored, and a data compilation tool was created using Microsoft Excel. A corporate executive assistant was enlisted to enter the survey results, saving the results in a predefined, secured, network drive accessible to only the researcher and the executive assistant to prevent any security breaches. Using the results of the self-reporting instrument, we performed ANOVA to test the differences on effort expectancy, facilitated technology interruptions, satisfaction, and willingness to recommend on different roles. ANOVA results show that the significance levels for effort expectancy, facilitated technology interruptions, satisfaction, and willingness to recommend are 0.12, 0.32, 0.12, and 0.06, respectively. We therefore conclude that there is no statistical difference between roles.
Results
Reliability and validity of constructs
In order to establish construct validity, reliability, convergent validity, and discriminant validity must be assessed. We used a second-generation multivariate statistical technique—partial least squares (PLS)—to confirm the reliability and validity of the measurement model analysis and to test the hypothesized relationships in the structural model. PLS Graph 3.0 is a software package that supports statistical multivariate technique PLS, which is a mean-based structural equation modeling (SEM). PLS was used to conduct an assessment of the validity and reliability of the measurement model and to test hypothesized paths in the structural model. We used PLS as our statistical analysis tool for several reasons. First, the objective of PLS is to maximize the variances explained. 29 PLS trades parameter estimation efficiency for prediction accuracy and simplicity and has fewer assumptions than many other statistical methodologies. Second, Falk and Miller 30 state that it is also appropriate when cross-sectional survey data are used. Third, one construct (willingness to recommend) contains two items. However, covariance-based SEM (CBSEM) such as linear structural relations (LISREL) requires a minimum of three items. 31
The composite reliability scores are 0.81, 0.86, 0.97, and 0.98 for effort expectancy, facilitated technology interruptions, satisfaction, and willingness to recommend, respectively, and all these values are greater than the suggested value of 0.7. 32 The average variance extracted (AVE) is in the range of 0.75 and 0.98 greater than the suggested value of 0.5. 32 The loadings for all the constructs are greater than 0.7. The composite reliability scores, AVEs, and loadings all suggest that convergent validity is established. Evaluating discriminant validity is to examine item to construct relationships to ensure items correlate higher to the construct they intend to measure than to other constructs. 33 Our correlation analysis shows that all items correlate highly with their respective construct. Therefore, we conclude that discriminant validity is achieved. Table 4 shows means, standard deviation, loadings of all the items, AVEs, and the composite reliability score of the constructs.
Descriptive statistics, loadings, AVE, and reliability.
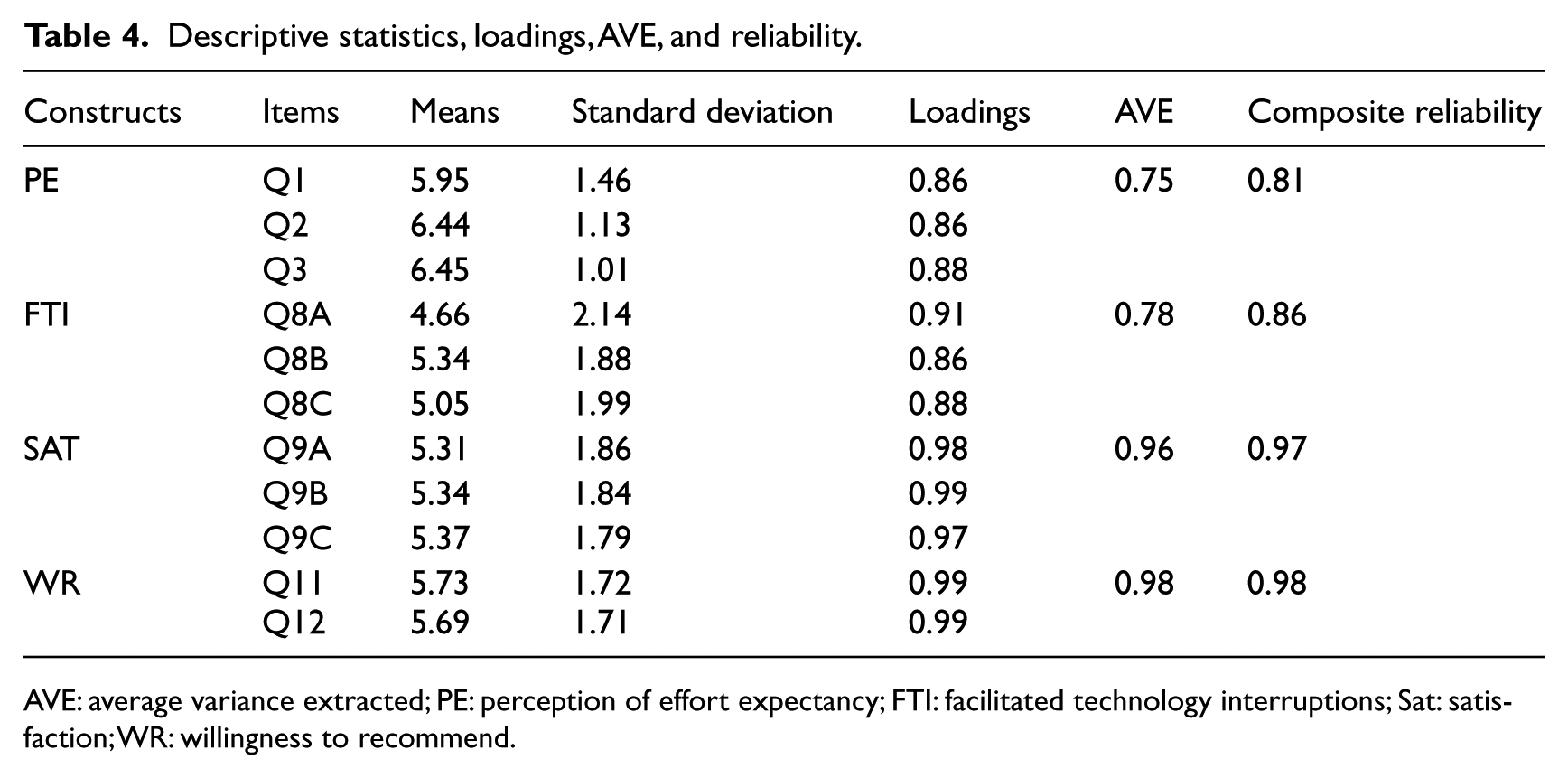
AVE: average variance extracted; PE: perception of effort expectancy; FTI: facilitated technology interruptions; Sat: satisfaction; WR: willingness to recommend.
Test of hypotheses
We use PLS Graph 3.0 to test the five hypotheses. Figure 2 shows the results of PLS analysis. The paths from facilitated technology interruptions to satisfaction and from satisfaction to willingness to recommend are significant at 1 percent level; the path from effort expectancy to satisfaction is significant at 5 percent level; the path from facilitated technology interruptions to willingness to recommend is not significant at 5 percent level. The r2 for satisfaction is 72 percent when facilitated technology interruptions and effort expectancy are used to predict satisfaction, and the r2 is 74 percent when facilitated technology interruptions, effort expectancy, and satisfaction are used to predict willingness to recommend. In summary, our data analysis confirmed four of the five study hypotheses, the exception being the path from facilitated technology interruptions to willingness to recommend.
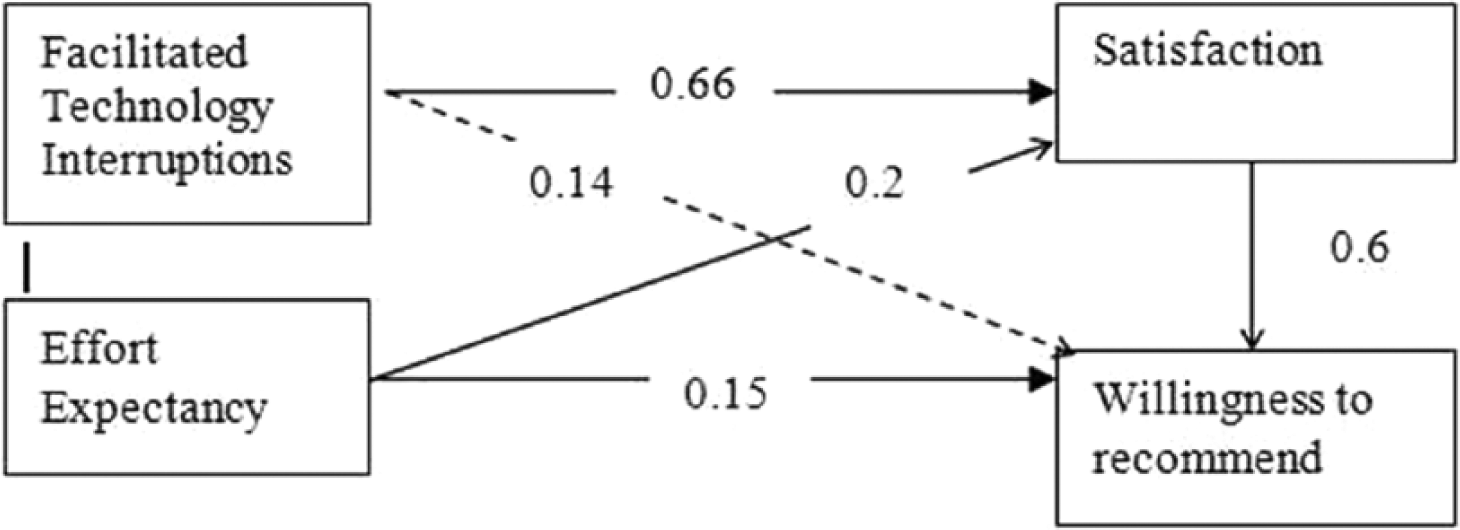
PLS results.
Discussion
This study investigates the impact of SSO technology and shared computer roaming workstations. We proposed a new construct—facility technology interruption—and relate it to the satisfaction and willingness to recommend. Although there is a well-documented relationship between satisfaction and willingness to recommend in the marketing literature,22,24 empirical data are not as widespread as anticipated on SSO and are lacking in terms of computer roaming satisfaction and willingness to recommend.1,13 This study tested the relationship between satisfaction and willingness to recommend in the SSO technology and we confirm this positive relationship. Lin and Hsieh 25 examined the relationship between satisfaction and behavioral intention with the use of self-servicing technologies such as kiosks and automated teller machines (ATMs), finding a statistically significant correlation between satisfaction and the likelihood that users would recommend self-servicing technologies to others. Self-servicing technologies are defined as mechanisms that allow the user to interface with technology in a manner that reduces bottlenecks, improves efficiency, and increases productivity. 25 SSO fits the self-servicing technology model in that it enhances the user experience by reducing the burden of constant login attempts whenever a user changes devices, by allowing user sessions to remain active over longer periods than traditional prescribed time allotments, and by improving upon login accuracy by autocompleting credential fields during a login process for applications tied to the technology. In the mandatory computer usage setting, satisfaction is a more appropriate dependent variable than behavioral intentions. 34 Our data confirm that users are satisfied with SSO and computer roaming and that there is the significant probability users will recommend usage to others.
Past research finds that the ease of use increases user satisfaction.20,21 Ease of use is the root construct of effort expectancy. Our analysis confirms the relationship between effort expectancy and satisfaction in the SSO context. The confirmation of this relationship is helpful in the promotion of SSO. We expect more user acceptance of the SSO technology. When implementing new technology with the intent to improve user satisfaction, reduce effort, and decrease nonproductive technology interruptions, it is essential to validate the achievement of these goals. Without post-implementation follow-up, it would be difficult to determine whether the facilitated technology interruption solution achieved the intended purpose. Additionally, it is important to recognize that users of the system provide solicited and unsolicited feedback and recommendations within the healthcare community. Therefore, we recommend that the facility engage the end user in the evaluation process post-implementation of facilitated technology interruption solutions.
Hypothesis 2 (facilitated technology interruptions → willingness to recommend) is not confirmed. This suggests that even though users are satisfied with SSO, they may not necessarily recommend this technology to others. Our findings provide practical guidance for other organizations when implementing SSO. Facilitated technology interruptions and effort expectancy are the two significant predictors for user satisfaction. When users are happy and satisfied, they work more productively. 35 Other organizations may use the findings from this study and perform pre-SSO versus post-SSO evaluations. Healthcare professionals are burdened by the constant login/logout. With SSO, the elimination of numerous login/logout will result in better job performance for healthcare professionals, and therefore produce other benefits such as more time spent providing patient care. We intend to follow up with end users to determine whether the technology has positively affected their ability to provide care while recouping lost productivity related to the removal of traditional authentication processes.
Limitations
This study investigates SSO implementation in a midsized hospital. Large hospitals may have different organization cultures and operation processes. In addition, the data were collected from a single organization. To that extent, generalization may be applied with caution. Another limitation is that this study focuses on the implementation of innovative technology within five hospitals all using the same suite of software applications. Hospitals using different software within the clinical setting could experience different response characteristics with these innovative technologies.
Conclusion
In this study, we conducted an empirical study on the impact of SSO technologies with added computer roaming capabilities in the integrated healthcare delivery network emergency departments. Our contribution to the theory includes the development of a construct (facilitated technology interruptions) associated with SSO technology and the testing of the relationships between facilitated technology interruptions, user satisfaction, and willingness to recommend. We proposed five hypotheses and our data analysis confirmed four hypotheses. The positive ratings on all study measures indicate that users are satisfied with this technology, as was anticipated by the organization. The study findings support user satisfaction and a willingness to recommend the introduction of SSO and computer roaming capabilities within emergency departments. This confirms and supports the investment of time and resources required to implement and support facilitated technology interruption technologies within fast-paced healthcare environments where care providers are expected to use computer applications on shared devices while effectively performing patient care activities. Our contribution to practice identifies enhanced care provider productivity when utilizing SSO capabilities with computer application roaming technologies. The authors recommend the implementation of these technologies within other organizations for the purpose of decreasing workflow interruptions and loss of valuable time associated with repetitive application authentication requirements. In addition, these contributions enhance the security mechanisms used to protect patient health record information. Enabling these technologies within healthcare settings, particularly fast-paced settings where shared workstations are utilized such as emergency departments, facilitates point of care documentation on devices within patient rooms, nursing stations, and physician workstations, thus saving care providers’ time and decreasing frustrations associated with username and password input errors while streamlining workflow within the acute care setting. Furthermore, making the login process more efficient without compromising security is desirable and valuable as a facilitating factor for greater user acceptance and adoption of an organization’s EHR.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.