
Abstract
The aim of this study was to investigate the use of electronic patient records in daily practice. In four wards of a large hospital district in Finland, N = 43 patients’ care and activities were observed and analysed in terms of the Grounded Theory method. The findings revealed that using electronic patient records created a particular process of writing and reading. Wireless technology enabled simultaneous patient involvement and point-of-care documentation, additionally supporting real-time reading. Remote and retrospective documentation was distant in terms of both space and time. The remoteness caused double documentation, reduced accuracy and less-efficient use of time. ‘Non-reading’ practices were witnessed in retrospective reading, causing delays in patient care and increase in workload. Similarly, if documentation was insufficient or non-existent, the consequences were found to be detrimental to the patients. The use of an electronic patient record system has a significant impact on patient care. Therefore, it is crucial to develop wireless technology and interdisciplinary collaboration in order to improve and support high-quality patient care.
Introduction
Research into the use of electronic patient records (EPRs) has revealed multidimensional complexity. EPRs have been valued for, among other things, their legibility, that is, the absence of unclear handwriting.1–6 Typed documentation is also a patient safety benefit because of increased readability. 7
A further advantage is the easy accessibility of EPRs for health-care professionals. As a communication tool among these professionals, written notes can be read remotely, which may help interdisciplinary collaboration in patient care, and thus make the care faster, more flexible and more beneficial to the patient care process. 8 The organisation of patient charts has been mentioned as an advantage in two ways: first, in how the charts are organised and thus how the needed information can be found, and second, by saving a lot of time, in not having to find lost paper records. In this sense, chart organisation means easier access to the information needed. 8
In implementing information technology (IT), attention to structured documentation has simultaneously brought an increase in accuracy and quality,9–12 also facilitating the decision-making process in patient care. 13 Studies which report on educational interventions of standardised documentation have shown improvement in accuracy by means of high-quality computerised documentation in various areas.9–12
Despite the successful outcomes of structured documentation, it has also been found to be occasionally inaccurate and inadequate.9,10,12 Nurses have complained that standardisation prevents them from individualising patient care. It also makes it difficult to document particular incidents, since finding the right terminology to describe a situation can be challenging. 14 Moreover, using structured documentation can be time-consuming, both in writing and reading, if the amount of written information increases but is not necessarily useful for its purpose. 15 This, however, is not the fault of the structured documentation per se but of the sheer amount of written text. A lack of structure can result in important information being missed, and focus lost, because of reporting unnecessary data.8,15 Paans et al. 5 suggest that in order to improve the accuracy of EPRs, the structures need to have flexibility and supplementary resources for more efficient e-documentation (e-Doc).
Documentation needs to fulfil legal requirements and to be transparent.16,17 The Finnish Act on patients’ rights 16 requires a patient-centred approach, since self-determination is a crucial part of patients’ care and documentation. At the same time, there are pressures on current health care, such as the reduced length of patients’ stay in hospitals 18 and frequent transfers from one care facility to another.19,20 In addition, the time for using computers in health care is limited. 17 A response to meet these challenges can be found in wireless technology, which supports point-of-care (POC) documentation, providing an effective tool for real-time information transmission, 21 whereby any problems can be promptly identified and addressed. POC applications can be utilised in clinical decision-making right at the bedside 22 and, for example, increase efficiency in the administration of medication. 23 However, computers at the bedside have been found to be inconvenient because of environmental and system barriers.2,24,25 Documentation at the bedside in a crowded room can be inconvenient, and disruptions in patient care have been reported. 2
In addition, nurses raise concerns that complicated computer systems distance patients and nurses from each other, and thus allow less time for direct nursing care.25,26 Computers’ physical location in the ward office not only distances nurses from the patients but also leads to more oral communication, resulting in loss of information. 9 In addition, computers are not necessarily provided for every nurse who takes care of the patients.2,25 This means that nurses need to wait their turn to be able to do their documentation,2,6,25 or must compete with other professionals in order to use the computers. 14 Consequently, nurses sometimes end up with a habit of first writing their notes on a scrap of paper and later transferring the information to the computer.9,26–28 The scraps of paper may contain information which might be important for the patient’s care but which does not always end up in the documentation.3,27 Moreover, this kind of double documentation also increases documentation time.3,9,26,27 Finally, complex computer systems can cause increased workload and thereby negatively affect the attitudes of health-care professionals towards those systems.6,29
IT in patient care has clearly changed the daily practices of nursing. But the success of an IT system in and of itself is not enough; one also needs to assess who benefits from that success. 30 Ever since the time of paper records, 31 there have been expectations that EPRs would make nursing documentation more patient-focused and beneficial for patients. According to Vikkelsoe, 32 the assumptions are that information exchange in EPRs improves communication between professionals, and thus improves both the quality of patient care and the coordination across organisational boundaries. However, the psychosocial aspects of documentation and involvement of patients in their care are weakened. 32 One can only hope that this is simply a matter of time. When the IT improves and nurses get more accustomed to using it, the distance between the patients and nurses decreases, and nurses have more time for patient care. 25
Because of the complexity of daily practice, there needs to be more focus on the relationship between e-Doc and patient-focused care. To provide continuity of care, an understanding of patterns of information exchange between and within organisations is crucial. 20 The importance of exploring working practices has been emphasised.11,30 Because of the issues mentioned here, this study takes the matter directly into the field of nursing by using participant observation in acute care settings, with the aim of discovering what impact the use of EPRs has and what kind of daily patterns in the exchange of information can be unveiled. Participant observation was chosen specifically because it can uncover the daily reality on the ward, allowing us to see the reality behind what participants say and do not say, or, indeed, are not even able to articulate. 33
Methodology
Patient care events, different daily practices and related use of EPRs were observed in four acute care wards. The primary researcher made all the observations. The style of observation varied from the researcher’s participation in events to simply watching the events from the side. Social interaction was an integral part of being in the field, and communication with the participants involved discussions and informal interviews, which are a natural and central part of observations.34,35 They focus on asking straight or open-ended questions, gathering explanations and clarifying situations. 34
Logging data in the field, the researcher usually jotted notes or occasionally wrote the text directly on a computer. 35 The notes were transcribed to the computer as soon as possible, never later than the same night after the event or the following day. This was an opportunity to reflect on the daily events and identify any need to return to the field and gain more information about the subject.33,36
The data were analysed according to the Grounded Theory method as formulated by Strauss and Corbin,33,36 which includes open, axial and selective coding. Data collection and analysis occurred simultaneously, and a constant comparative technique was used. In open coding, the written data were broken into details forming substantive codes. In this study, such microanalysis was employed to gain enhanced insight into the observations. Using microanalysis, pieces of data were broken down to uncover details of events observed. The data were interrogated for answers to questions such as ‘what is going on?’, ‘who are the actors?’ and ‘what is an actor doing?’.33,36 As data collection and analysis proceeded, the codes were grouped into categories with particular properties and dimensions. Finally, the categories were given more meaningful names.33,36
In the axial coding, the data were reorganised. The created categories were constantly compared and structured according to how they related to each other. The observations were also compared to the data from written patient records in order to increase the understanding of how a single observed event was part of the whole care process.33,36 At the beginning, the data collection and analysis followed the inductive approach. As the process went further, an exchange of induction and deduction took place when the comparisons were investigated. To connect the structure and process, the paradigm model33,36 was used. Additionally, the conditional relationship matrix by Strauss and Corbin 36 and Corbin and Strauss 33 as well as Wilson Scott and Howel 37 was adapted for the analysis. The exchange of information was then described under the categories ‘writing’ and ‘reading’, with their subcategories – which are presented up to axial coding as findings of this study.33,36
Sample and setting
The interest of the study was in acute care settings in order to gain an insight into somatic wards where the patients’ stay was short; the patients’ average hospital stay varied from 1 to 3 days, with some exceptions (up to 4 weeks). Thus, purposive sampling was used when choosing the study sites and informants. Table 1 illustrates the nature of the wards.
Description of the wards.
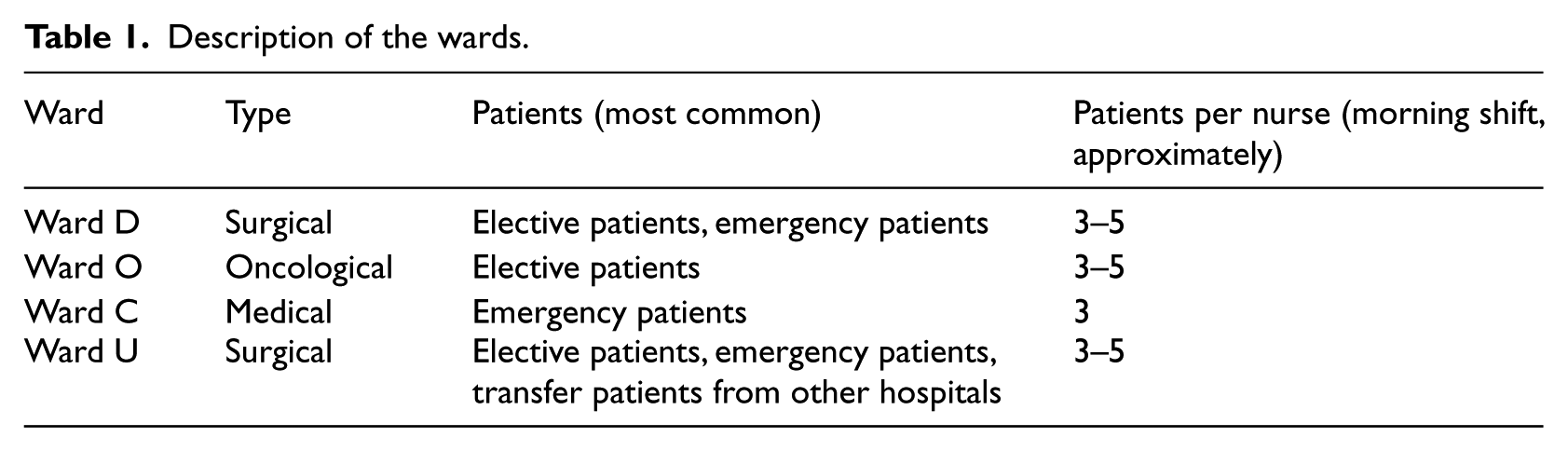
All the wards were responsible for acute care patients, and they had both similarities and differences regarding their delivery of patient care. One significant common feature was the speed of the care processes. At the time of initial data collection, the EPR system had been in use for almost 2 years in every ward studied, but it was still in constant development. The continuous patient history was available both in electronic format and on paper, but some information, such as charts and graphs, existed only in a paper version.
Every ward used the system in its own adapted way. The software menu was planned to be a multidisciplinary tool, following the process of patient care. There were both fixed and mobile computers for staff use. The fixed computers (desktop) were located in different rooms such as nursing or doctors’ offices and in consultation or examining rooms. The mobile computers were laptops placed on wheeled carts. They were of a suitable size for moving through the ward corridors, offices and patient rooms. Their use everywhere was dependent on a wireless signal for which coverage was limited. Sometimes the network system caused frustration because of slowness or ‘downtime’, especially concerning the mobile units. Constant efforts were made to improve the system.
In all four wards, desktop computers were available in the offices. In Ward D, nurses and doctors were provided mobile computers for their daily use. In Wards O, C and U, some mobile computers were available and were used mainly on doctors’ rounds.
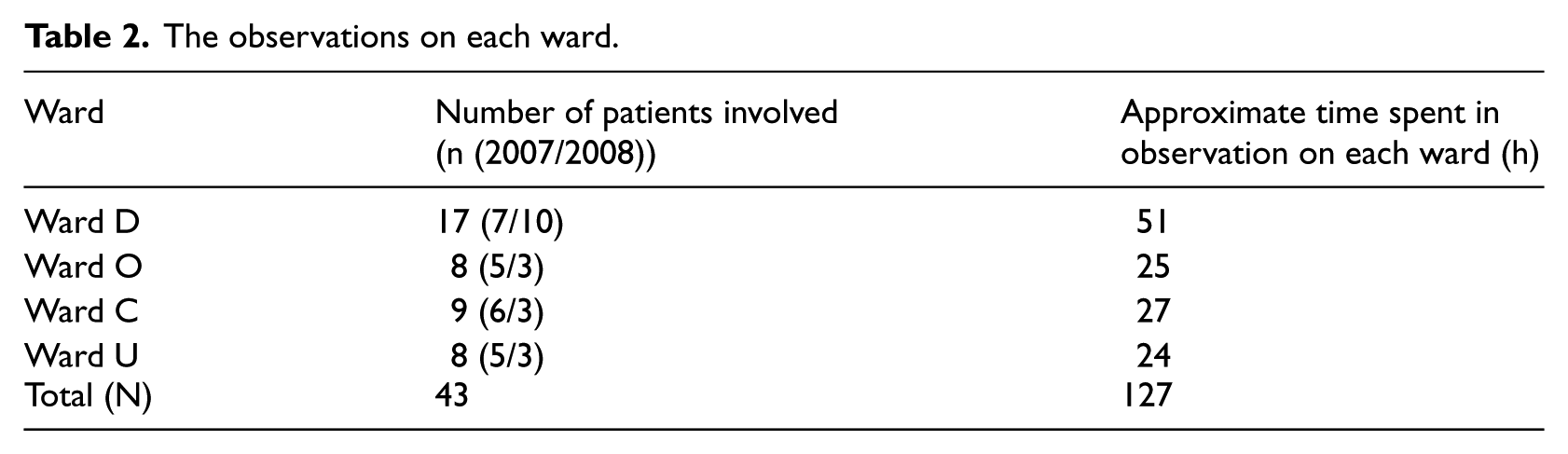
Due to differences in the use of EPRs and in the daily practices of the wards, the data were collected purposefully. The amount of data differed among the wards. In the second year of data collection, one of the wards (D) changed its nursing practices; thus, more data were collected on this particular ward in order to reach an adequate data saturation.33,36 A total of 43 (N = 43) adult patients were involved in this study. The patients were admitted to the hospital for medical procedures, for example, operations, tests and treatments. Table 2 summarises the observations on each ward.
The observations on each ward.
Findings
Use of EPRs in the acute care wards formed a complex process. Two categories, writing and reading, were observed along with associated subcategories. Writing and reading both occurred simultaneously. However, there were temporal and spatial dimensions which affected the consequences of patient care. Therefore, the categories are presented individually. Examples of field notes and EPRs are presented in the text in italics.
All four wards had similarities and differences in using EPRs in daily practice. Computers were provided to nurses; however, only in Ward D were a sufficient amount of mobile units provided for nurses’ use. Although Wards C and U did have a few mobile computers for use by nurses, the nurses normally did not use them. Rather, they used the fixed computers in the nursing office. Doctors used their own mobile computers on their rounds, mainly writing the daily orders on them. This gave the nurses an opportunity to use the updated information and carry out the orders.
The exception was Ward O, which in the first year of observation, was located in the old hospital building. Due to the weak signal coverage in the corridors, only fixed computers were provided for the professionals’ use. By the second year of observation, Ward O had moved to a new building. However, all of the computers observed there were fixed and located in the nursing offices. In none of the wards were the processes described in these categories applied systematically; rather, these are patterns that were uncovered in this study setting. Table 3 shows the general similarities and differences.
Similarities and differences of using EPRs between the wards.
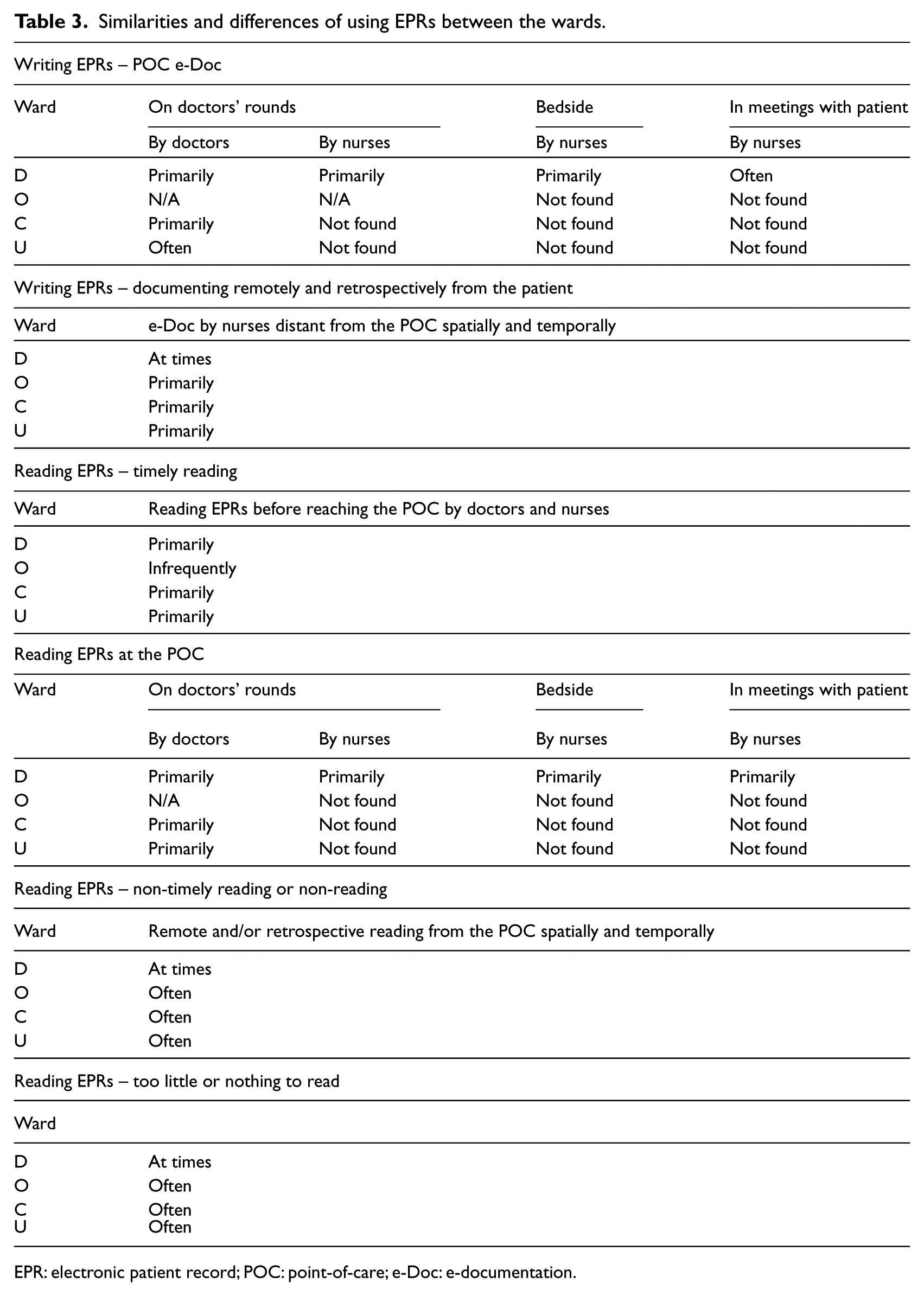
EPR: electronic patient record; POC: point-of-care; e-Doc: e-documentation.
Writing EPRs
POC e-Doc
POC in this study refers to the location where various patient-focused events occurred. POC e-Doc was done in different situations, such as at the bedside or in offices in simultaneous conversations between the patient and the professional. Incidences of POC e-Doc included admissions, doctors’ or nurses’ rounds or care procedures. Since the interest was in the patient-focused nursing care and documentation, the POC and related events were observed specifically in relation to the patient care.
The doctors took the mobile computer to the bedside and wrote their orders and annotations for future care directly on the computer while interacting with the patients. Patients participated by expressing their own perspectives, emotions and wishes, as well as by asking questions or explaining their health history. POC e-Doc ensured that the documented text was ready to reuse and especially that the care plan was ready to proceed. The next field diary description illustrates an event from the doctors’ round:
Example: The roles and actions at the POC e-Doc.
The nurse and doctor entered the patient’s room, both having their mobile computers along. The doctor stood next to the patient’s bed, while the patient was lying there. The patient’s husband stood on the other side of the bed. The nurse with her mobile computer stood nearby, on the side. Patient and doctor had a dialogue, in which the patient’s spouse also participated.
The patient and the doctor updated the patient’s situation, tracing back the operation, its causes and consequences. The patient and her spouse posed intensive questions such as ‘why?’, ‘what if?’, and ‘is it possible?’ The doctor answered, giving detailed information, asking additional questions and browsing at the same time through the information, such as lab results, on the computer. The patient and doctor made an agreement about future actions, including plans for the patient’s discharge. The doctor wrote new orders and recorded their decisions on the computer while discussing them with the patient and her spouse. The mobile computer was thus like an open book.
Afterwards I talked with the patient and her spouse. She spontaneously evaluated the previous event, expressing her satisfaction. Both the patient and her spouse emphasized that with mutual understanding it was easy to proceed. Two mobile computers in the room simultaneously did not attract any attention.
During the doctors’ rounds in this ward, the nurses documented simultaneously, on the second computer, how the patients’ care had proceeded, including the interpretation of lab tests and so on. The nurses did not repeat the doctors’ orders or their words; their purpose was to observe and write down in the EPRs what the patients were told, what they knew about their situation and how they received the information. This was a way to assure the continuity of care and thus to give to on-coming nurses a point of departure for how they should proceed in this particular patient’s care:
I discussed with the head nurse of the ward the purpose of the nurses’ e-documenting simultaneously. She explained that in this way the nurses were aware, for example, of what the patient already knew about his/her situation and what kind of information the oncoming nurses should explain or teach to the patient later on.
POC e-Doc also took place at the bedside, where nurses took the mobile computer to review the patients’ status with him or her while simultaneously writing notes on the EPR. This was a reciprocal way to ask and answer questions in order to increase information in the EPR about the patients’ situation.
One mode of POC e-Doc was done in preoperative meetings between patient and nurse. The purpose of the event was to exchange information regarding the patient’s upcoming surgical procedure. In the private office room where the preoperative meetings were held, the seats of both the patient and the nurse were located in such a way that the computer screen was easily visible to both parties.
In one of the wards, patients arrived from the emergency room with the need to get a clear diagnosis, so as to find the right treatment for them. The patients generally had a complex history of co-morbidities. In their rounds, the doctors talked to the patients, asking multiple questions in order to get as thorough a picture of the situation as possible. The previous history (such as co-morbidities) provided background information, which pointed to ways to get more information, such as lab-tests or other procedures. The detailed probing discussion using simultaneous background information and documentation in the EPRs was an effective method for updating, and acquiring more, written information:
The doctor’s questions were numerous, detailed, diverse, accurate and holistic. She did some clinical examinations, such as palpation and auscultation of the lungs, while at the same time explaining the purpose of her questions, and bringing into the discussion the lab test results and various alternatives, using understandable language. The patient’s own views were considered important and he was actively involved in the discussion. Simultaneously, the doctor’s findings and orders were documented on the computer. The discussions were intense, almost like interrogations, but always with the goal of the patient’s well-being.
Documenting remotely and retrospectively from the patient
Another mode of e-Doc that was found occurred away from the patients. Remote e-Doc was distant from the POC in two ways: space and time. Nurses usually gathered to work on the computer – whether mobile or fixed – in the nursing office. The offices were busy places with constant disruptions. As a consequence, the nurses’ concentration was distracted away from the patients’ affairs to other matters. The nurses worked on the computers many times during their shift. They also updated necessary information on the paper flow-sheets or other paper forms. They commuted between the patients’ rooms and the office in order to ask additional questions and thus complete the necessary information.
At POC, the nurses wrote short handwritten notes on a piece of paper, from which they later transferred information to the EPRs. This was a pattern in various events, such as on doctors’ rounds, when interviewing a new patient at the bedside asking some information from the patients or on end-of-shift handovers. Memo-notes were also used by nurses as checklists of things to do, taking information for themselves from the computer, usually at the beginning of the shift or in connection with urgent occasions. Many nurses wrote paper notes even though the computer had been available in the room where the event took place. These notes had an effect on everyday patterns, regarding how the information was held and maintained. They were unofficial yet important tools for nurses in everyday practice, which, at the end of the shift, ended up in the trash basket:
When I asked why the nurse did not write straight on the computer, she mentioned the slowness of the documentation system on the computer and that there were ‘too many clicks’.
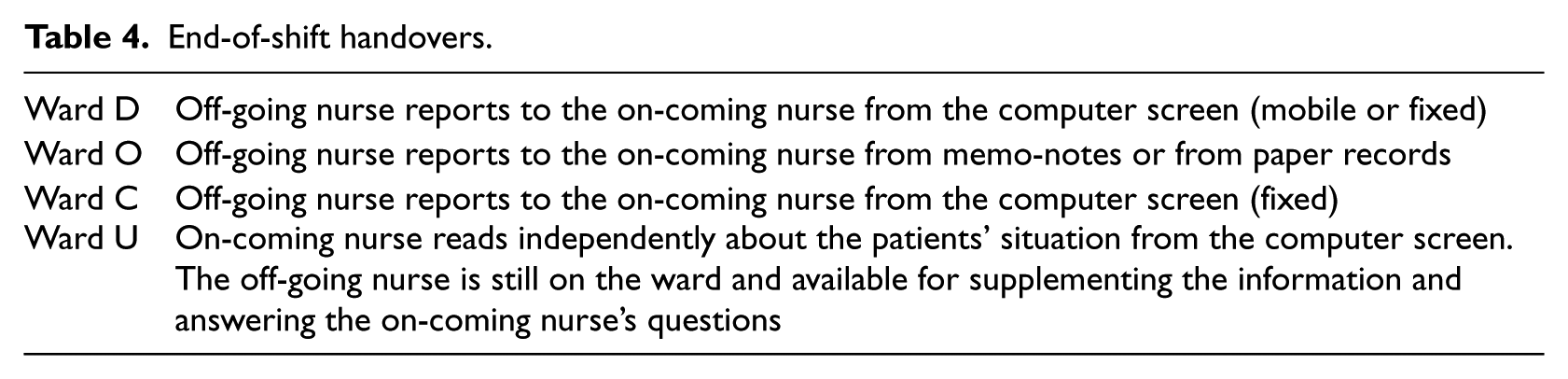
Nurses were responsible for approximately three to five patients in one shift, some of whom were admitted, some discharged and some taken to or returning from procedures outside the ward. With regard to observations of these different events, the time of the documentation varied. Other than those which were documented at the POC, the time lapse ranged from approximately a quarter of an hour to 6 or 7 h, which was at the end of the nurse’s shift. The peak time for documentation was in the afternoon. Some of the nurses mentioned that the time for documentation was ‘when all the other work had been done’. The information from memo-notes written earlier was only at this time, retrospectively, transcribed to the computers. This meant that the documentation was sometimes performed after the handover to the next shift. Observed from the morning shift, each ward had its own practice of end-of-shift handover. The observations in this study revealed the following end-of-shift handover modes, which are presented in Table 4:
After a busy morning the nurse did not have time to put her documentation on the computer until after the shift change. First she gave an oral report to the on-coming nurses from her notes and also from the paper-charts describing the patients’ medical history.
End-of-shift handovers.
Reading EPRs
Timely reading
In this study, timely reading was found to occur before reaching the POC and at the POC. By means of timely reading of EPRs, nurses and doctors oriented themselves to meet the patients in order to learn the patients’ health situation and needs for care. Those situations were revealed before meeting the patients, such as on doctors’ rounds, planned nursing care, pre-planned interviewing of patients (e.g. in admissions) or ongoing nursing shifts.
The medical and nursing viewpoints on patient documentation were different. In the best case scenario, all professionals benefited from relevant and real-time documentation and reading because it made the care paths smoother. Characteristic incidents were, for example, where the nurse had explained the patient’s symptoms in the EPR. Later, the doctor used the nurse’s previously documented EPR text as background information while reading the EPR at the patient’s bedside.
Timely reading at the POC was observed, for example, when nurses were discussing the care plan with the patients. Those events were usually in admissions or in preoperative meetings, which occurred a few days or weeks before the surgical operation. The patients’ previous history in EPRs complemented the interviews and was important in bringing out potential safety issues:
At the patient’s pre-operative meeting, the patient and a nursing student had an extended conversation before the operation. In the background, the nurse was simultaneously reading the patient’s history of previous operations. She found out that the patient still had a metal plate in her leg. This information was important regarding the coming operation, and thus improved the patient’s safety.
Timely reading also occurred as the on-coming nurses received the end-of-shift report. Nurses spent time reading the EPRs of the patients who were assigned to them. In the end, the off-going nurse was still on the ward and available to complete the information. In another observed ward, both on-coming and off-going nurse reviewed the EPRs together. Although this kind of timely reading was meant to be helpful for gaining information, it happened remotely from the patients, usually in the busy nursing office with other distractions.
Non-timely reading or non-reading
Remote and/or retrospective reading was distant from the POC spatially and temporally and took place at times when there were no other routinely programmed plans or acute events. This was also a way to become familiar with the patient and his or her care. In addition to remote writing, non-timely remote reading also led to incidents where the delayed reading meant that the patient’s care was also delayed or even omitted:
In the middle of the shift, a nurse noticed in the EPR that the patient should have been prepared for a scheduled radiological procedure. However, the time had passed and the patient missed the procedure. The nurse protested that, at the handover, ‘nobody mentioned about the patient’s procedure’.
Non-timely reading occasionally caused unnecessary hustle and bustle, resulting in many extra steps, questions to patients and other professionals, phone calls and confusion. As a consequence, this meant extra work for the staff, causing a number of hurried situations and taking time away from more important issues:
The patient was ready to go home, but some discharge information from the doctor was missing. Nurses tried to contact the doctor they thought should discharge the patient; they asked around and made phone calls. After a couple of hours, the nurse eventually read the patient’s EPR. She found all the discharge papers already written from the previous day, because the doctor was not scheduled to be at the hospital on that day. Meanwhile, the patient was waiting and was eager to go home; he waited in vain only because the EPR-text had not been read. Everybody’s time was wasted.
Similarly, e-Doc was sometimes not read at all by the health-care professionals even when it was available (i.e. non-reading). This consequently led to situations where patients were repeatedly asked the same questions by various professionals, even about things which had already been decided or resolved. For example, one patient was asked how her wound should be treated, although that procedure was described in the notes. Professionals, both nurses and doctors, were frustrated when they had written careful documentation and later noticed that this careful documentation had not been read by their colleagues.
Too little or nothing to read
Situations arose when the professionals were seeking specific information but nothing – or only a little – was documented. In this situation, both nurses and doctors questioned each other because missing documentation affected complicated aspects of patient care. Missing documentation entailed many repeated questions and extra work – the same kind of situations as noted in the previous category. It also resulted in a deviation from the direct path of the patients’ care, since missing or insufficient information interrupted that care or misdirected it. There was also a lack of information about patients’ sensory dysfunctions, such as hearing, which caused communication problems in important interactions. Such information would help daily life interventions in both nursing and medical care. The following two examples from nursing documentation illustrate this difficulty: The sentence ‘Patient teaching has been given’ tells that the nurse has taught the patient, but an assessment of the teaching situation is missing. Missing information about the specific details of a patient’s transfer to another ward: ‘To be transferred to another ward’ was the only written sentence about the issue.
In the Ward U, which regularly received transfer patients from other hospitals, missing information regarding EPRs emerged. Due to the different computer systems between two hospitals, EPRs were not available for reading. Paper prints and also handwritten reports followed transferred patients, with varying levels of information. However, nurses expressed their worries regarding insufficient information. The findings are summarised in Table 5.
Summary of the findings (adapted from Wilson Scott and Howel 37 and modified for observational data).
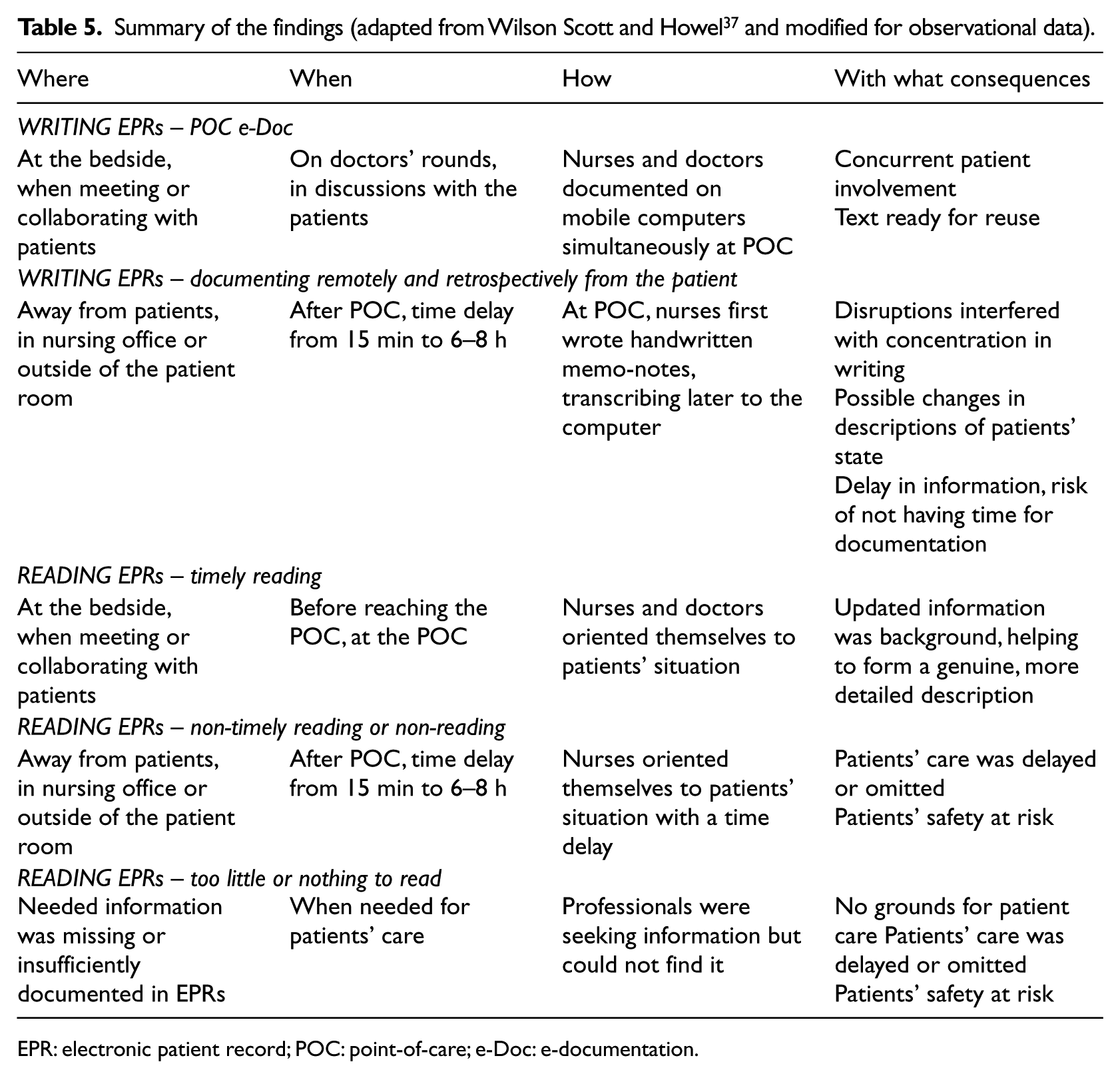
EPR: electronic patient record; POC: point-of-care; e-Doc: e-documentation.
Discussion
Credibility
The principal researcher had experience in the field of clinical nursing. Thus, she had an insider’s advantage to ‘intuitively recognise situations that are sensitive’ (p. 312). 38 In the field, she chose to write notes out of sight of the participants. This was based on the thought that the hectic environment was full of stimuli, and making notes in private seemed to be the least disruptive way of data logging. 38 Throughout the study, the researcher simultaneously collected, analysed and interpreted the data. Writing constantly in the field diary helped to increase the understanding of the data. The co-researchers were involved in reviewing and reflecting on the collected data and analysis. In addition, microanalysis as part of the data analysis was utilised in order to gain as detailed an insight as possible. This contributed to increasing the credibility of the study as a whole.33,36
Ethical considerations
The study was conducted in accordance with the research policy of the hospital district. 38 The ethics committee of the hospital approved the study; all the participating patients and staff on the wards were informed about the study both verbally and in writing. Participating patients signed an informed consent to confirm their agreement. 38 Only patients whose physical and mental status was stable were involved in the study. Thus, all the participant patients were capable of making their own decisions regarding their participation in the study. They also knew that they could withdraw from the study at any time. Confidentiality was assured for all the participants.33,36,39 Therefore, based on the promises of confidentiality to the local ethics committee and the wards, no names or symbols of the wards are mentioned in the examples. 35
Findings
In the processes of writing and reading EPR documentation, all of the observed wards had similarities and differences. Common characteristics were, for example, the fast pace and daily patterns of the care processes. Doctors’ e-Doc also had similar patterns in three of the four wards. Comparing the nursing e-Doc on all four wards, only in Ward D was POC e-Doc significant. In this ward, mobile computers were provided for nurses, thus making timely writing and reading – along with timely patient care – possible. When the information was written without delay, it was direct, that is, without interpretation and with less susceptibility of erroneous recollection. Developing and/or supporting wireless devices at the POC have provided good, precise results in patient care and thereby improved the safety and quality of nursing care.21,22 Additionally, just as previous studies have emphasised the importance of patient involvement in their own care,19,31,40 the findings in this study suggest that wireless documentation at the POC allows an opportunity for patients to be involved: from their perspective on their history, through assessment of their current status and on to decision-making regarding future plans. In her study of care plans in paper records, Mason 40 reached similar findings in one of her research wards. As witnessed in this study, an important benefit of electronic documentation is the availability it affords for immediate and continuous use of the written text. Furthermore, writing information at the POC avoided the need for retrospective documentation or recalling. 40 This is an important concern for developing the care processes when everywhere in health care the staff are struggling with time and speed.
Consistent with the findings in this study, issues regarding remote or retrospective documentation have been apparent in previous studies of computerised documentation.2,9,23,24 Instead of documenting directly on the computers, nurses resorted to scratch-paper notes. The information these notes contain often is wasted by being thrown away, or at least it is not fully utilised for the benefit of patient care. 26 The remote mode of doing the documentation occurred when the computers were located in nursing offices or distant from the patients. 9 In previous studies, nurses have indicated their concern about constant disruptions, distance from the patients and less time for patient care. Nurses share their time with several patients during one shift and are also responsible for many other indirect tasks.2,6,23,24 Those consequences were also seen in this study. All these factors can contribute to a situation where oral transmission of information leads to loss of information. 9 Congruently, this study suggests that disruptions and distance mean a discontinuity of care, which can lead to inconsistency in patient treatment.
Even in Ward D, where mobile computers were provided for nurses, at times they gathered together in the nursing office to update the EPRs. Understandably, in order to make a picture of patient care and how to proceed in it, some remote reading was necessary, for example, in handovers or admitting incoming patients. However, this study discovered occasions when patient care would have been more up to date and more consistent if the reading had occurred in real time at the POC. In any case, it was evident in this study as well as in others that using EPRs, whether writing or reading, in an environment with constant disruptions and distractions distanced the nurses from patient care.2,24–26
With timely reading at the POC, the professionals were effectively able to review and get up to date with the patients’ situations. Some of the observations in this study indicated that timely reading and concurrent interaction with the patients gave a valuable opportunity for collaborative decision-making between the patients and professionals and consequently improved patients’ involvement in their care.19,31,40
Investigating the use of EPRs revealed that the ‘non-reading’ practices of some professionals caused a lack of communication among members of the multidisciplinary team, resulting in frustration for all who were involved in the care. 23 Non-reading habits meant that precious time was squandered. Even the non-read text was finally read; however, the fact of initial non-reading meant that when the reading was eventually done, it may have been too late for its purpose. In those circumstances, when the reading was delayed, the process of patient care was delayed.4,15
A similar situation was observed in the category of ‘too little or nothing to read’; essential information was not written at all or it was documented insufficiently. When the time of documentation was left for the end of the shift, or nurses’ work was in other ways disrupted, there was a risk that accurate documentation was not done at all.2,9,41 As merely oral communication has been found ineffective, 9 the focus for more timely and accurate documentation is a serious need for health care. Insufficient or completely lacking documentation creates difficulties for the interdisciplinary team; consequently, the patients in their care are those who suffer the most.
Based on the findings, more research on the e-Doc is needed in acute care from the patients’ point of view. One suggestion is to investigate how structured documentation can support patient-focused and POC documentation. It is also suggested for further research how the patients’ perspective could assume priority in EPR documentation.
Limitations
This study has several limitations. Participant observation requires time in order to gain an understanding of the subject of interest. Therefore, the limited amount of patient care observed may be one of the limitations of the study. In addition, having two participant observers, instead of only one, could have given deeper insight into the process. In addition to the revealed pattern, focused interviews with professionals could have given more profound findings.
Conclusion
This study found that using EPRs in a timely manner at the POC has a pronounced impact on writing and reading, thereby improving the quality, safety and continuity of care. It facilitates patients’ own involvement in their care and increases accuracy. Nurses and the other professionals at the POC have an opportunity to collect, process and transfer information for timely care. Thus, wireless EPR systems support patient-focused care; therefore, it is crucial to make use of the EPRs as flexible as possible, in terms of both time and place.
It is obvious that electronic documentation is an interdisciplinary tool. The results of many previous studies and the observations of this study regarding the use of EPRs to greater or lesser effect lead to the conclusion that timely collaboration is important for effective health care. Interdisciplinary professionals need to agree on the ‘who, what, when, where, why and how’ of documentation in order to support the safety, quality and continuity of patient care. Different professions have their own domains of knowledge, and sharing information collaboratively in the best interest of the patient is crucial. If everyone has a common understanding of the use of EPRs and proceeds accordingly, benefits will accrue to both the writers and the readers of electronic documentation in fragmented modern health-care systems, where time is precious. In order to develop the use of EPRs, therefore, there needs to be a simultaneous emphasis on developing all the processes of health care in a patient-focused direction. In the daily pattern, this needs to be facilitated and is an administrative responsibility.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was financially supported by the competitive research funding of the Tampere University Hospital (Grant 9H151 and Grant 9J053), Department of Musculoskeletal Diseases of Tampere University Hospital, Pirkanmaa Hospital District and the Finnish Nurses Association.