
Abstract
New Zealand is moving towards an integrated health-care model with information accessible electronically regardless of location, linking existing health provider systems, regional clinical results repositories and a shared care record. However, such information sharing has been a major concern for patients attending sexual health services. In this study, we investigated patient attitudes towards a change in practice to support an integrated care model. Outcomes showed that confidentiality remains a significant concern, and routine sharing of patient information may create barriers to attendance for some, leading to a potential increase in untreated infections. We conclude that sexual health services may be able to change their information management practices to an opt-out consent system and routinely share health information with other health providers, but further public discussion to ensure informed consent is needed before this can happen. Regardless of national policy, it is still necessary to keep clinic visit details confidential for some patients attending sexual health services.
Introduction
New Zealand is moving towards an integrated health-care model with information accessible electronically regardless of location, linking existing health provider systems, regional clinical results repositories and a shared care record. 1 A unique patient identifier (UPI) for the medical records of patients, uniquely identifying the patient throughout the health system, is considered essential to enable safe information sharing by several Western countries, including New Zealand and the United Kingdom. 2 Provided it is non-disclosing (contains no personal demographic information), 3 it can enhance confidentiality, 4 preserve anonymity 3 and provide protection from inadvertent information access or disclosure. 3 The New Zealand health system has used such non-disclosing UPIs since 1993, the National Health Index (NHI), given to each individual automatically at birth or on later contact with the public health system, for example, immigrants. 5 The research presented in this article explored the implications of using the NHI to increase sharing of health information by sexual health services (SHS) with other health providers in New Zealand. The implications of a change in practice to an opt-off system of sharing information rather than an opt-in system will be considered.
Sexually transmitted infections (STIs), such as chlamydia, gonorrhoea, genital warts and genital herpes, are among the main preventable causes of ill health among young people in New Zealand. 6 As many as one in five adults may have genital herpes (type 2), but most will have asymptomatic or unrecognised disease. 7 Genital chlamydia infection was the most commonly reported STI in New Zealand, highest among women aged 15–19 years (7098 per 100,000 population), and national rates are considerably higher than the United Kingdom, Australia and the United States. 7 The incidence of STIs such as syphilis and HIV, although relatively low in New Zealand, is likewise increasing. 7 In New Zealand, sexual health care is mainly provided by free sexual health clinics and family planning and youth clinics and general practitioners (GPs) with varying levels of fee subsidy. 7 However, information sharing with other health providers has been a major concern for patients attending SHS,8–10 where the sensitive nature of relevant information is potentially stigmatising – contracting an STI is often perceived as due to ‘amoral’ or ‘deviant’ behaviours – that people with STIs are somehow socially and morally unacceptable, and thus, people with STIs can be subjected to embarrassment, discrimination, criminalisation and abuse.11–13 Thus, patients may limit disclosure of information that is essential for correct treatment or be deterred from attending for care.8 –15 Most SHS currently use their own sexual health code numbers, a similar practice to that of sexual health and genitourinary medicine (GUM) clinics in the United Kingdom, 8 to keep patients’ records and test results separate from hospital and regional databases, thus maintaining a confidential service for SHS patients. 16
Adoption of NHI numbers with laboratory tests by SHS has already occurred in large, high–population density centres in New Zealand, such as Auckland, but has raised concerns regarding patient privacy. 17 Laboratory results indicate the nature of the tests performed and potentially the health concerns leading to testing. In cities/towns with lower population density, the likelihood of familial or friendship connections to laboratory or health-care staff is high, increasing the potential for perceived loss of privacy and confidentiality. This research project, based in a regional hospital-based SHS in provincial New Zealand, aimed first to investigate patient awareness of NHI numbers and reason for clinic attendance at the SHS; second to ascertain patient attitudes to the adoption of NHI numbers on laboratory request forms and discharge letters, containing details of clinic attendance, being routinely sent to GPs, and finally, to determine potential adverse consequences of a change in information sharing practices by the SHS.
Methods
The study was performed at a New Zealand provincial hospital-based part-time SHS with rural outreach clinics, serving a large geographical region with a population around 160,000. 18 The SHS operates both as a specialist secondary health provider and as a primary health provider for self-referred patients, many of whom have no GP or will not attend their GP for sexual health issues.
A self-administered questionnaire was offered to consecutive SHS attendees in the period 10 August to 11 September 2009. Patients were eligible if they were aged 16 years or over and had no cognitive or language barrier to completing the questionnaire. The questionnaire was developed from a previous survey, 19 extensively pretested with a pilot study undertaken with SHS patients. Questionnaires were distributed by the receptionist to avoid any perceived pressure to participate or association with provision of care, and the researchers and SHS staff were unaware of participants. Participants could complete the questionnaire in the waiting room or take the questionnaire away and return it by post in a prepaid envelope. Consent was implied by choosing to participate. The questionnaire included an information brochure explaining the NHI number. 20
Data gathered included patient age, gender, ethnicity, sexual orientation, motivation for clinic attendance, clinic referral pathway, patient preferences about using the NHI number on laboratory requests, the routine sending of discharge letters to GPs and hospital doctors/nurses access to computerised laboratory results.
Ethical approval was granted by the Central Regional Ethics Committee (Reference CEN/09/06/042). Final data analysis involving descriptive statistics and chi-squared i tests was performed using PASW Statistics v18 software, and the results have a maximum margin of error ii of ±6.9 per cent.
Results
A total of 249 patients attended the SHS (at both the regional hospital and the outreach clinics) during the study period; 216 (87%) completed the questionnaire. There were no ineligible patients. Seven questionnaires were discounted due to incomplete data; thus, 209 respondents, 80 (38%) men and 129 (62%) women, were included in the study (84% usable response rate). Of these, 126 (60%) had previously attended the service.
In all, 29 per cent (16) of respondents were aged 16–19 years with 55 per cent (114) aged under 25 years; 31 per cent (65) identified as Māori iii and 61 per cent (128) as New Zealand European with responses from other ethnic groups being too small to use for analysis; 91 per cent (191) identified as heterosexual.
NHI awareness and reason for clinic attendance
A total of 70 per cent (146) of respondents stated that they knew nothing about the NHI before participating in this study, 20 per cent (41) knew a little and 10 per cent (20) knew a lot. The level of knowledge about the NHI is significantly greater for females than males (p = 0.001) and for >19-year-olds than for 16–19-year-olds (p = 0.011). There was no relationship between prior level of knowledge about the NHI and attitudes to the use of the NHI; thus, the lack of prior awareness of the NHI is unlikely to have significantly confounded the results. Fifty-four (26%) respondents were referred by another health provider. Of the 151 who self-referred, confidentiality (47%) and cost (40%) concerns were the main reasons for attendance.
Attitudes towards information sharing
Respondents were asked about their attitudes towards using a UPI (the NHI) on laboratory tests and routine discharge letters to health professionals, including their GP. As the SHS is located in a regional hospital setting but keeps its test results separate to the hospital laboratory repository, respondents were also asked whether other hospital doctors/nurses should be able to access SHS laboratory test results (see Figure 1). Of note is the large group in the ‘maybe’ category across all three information sharing activities (39%, 37% and 33%). The ‘maybe’ category consisted of respondents who wanted more information before they could answer (NHI use and discharge letter) or were ‘neutral’ (other medical staff). There were no identifying/distinguishing demographic features about this ‘maybe’ group.
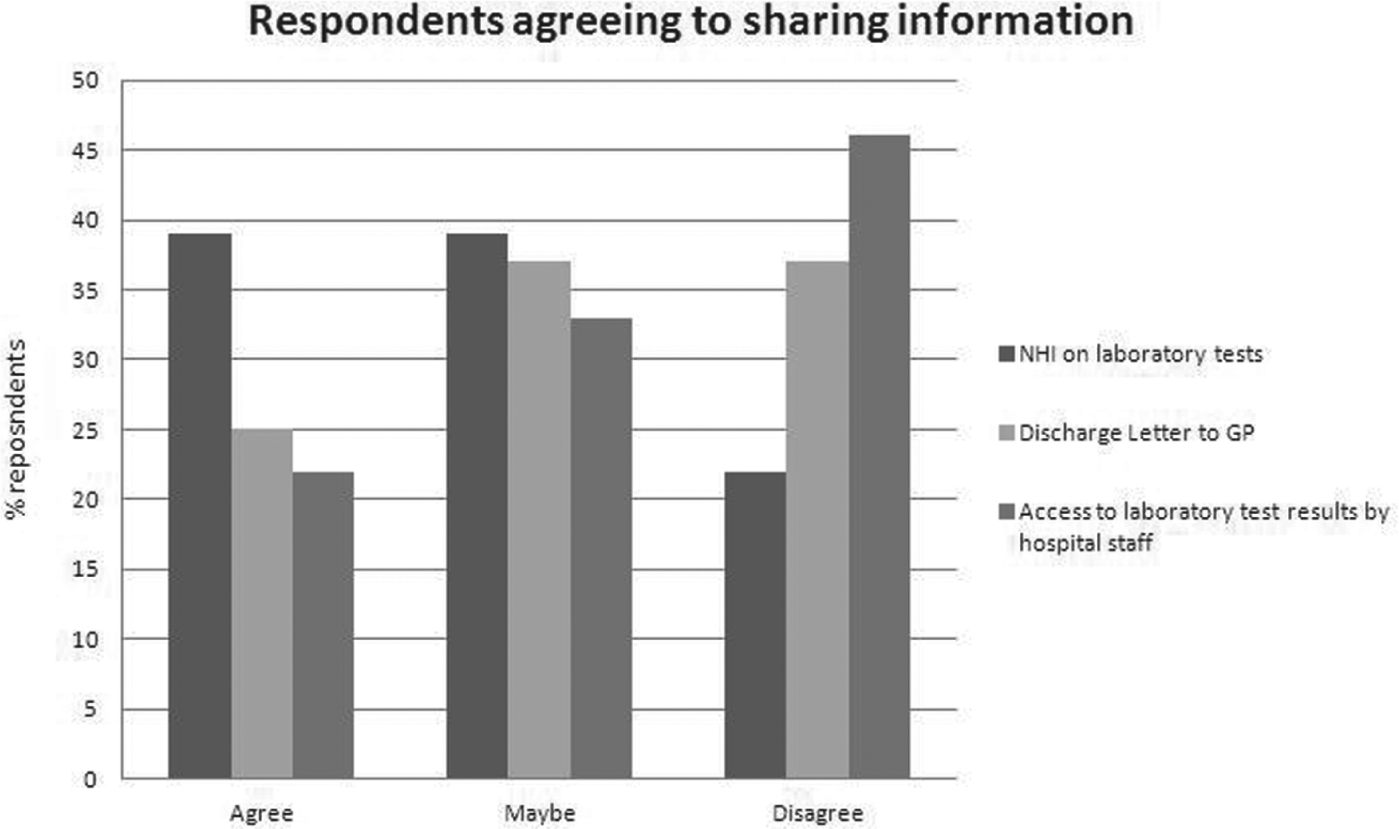
Attitudes to information sharing activities.
Respondents were able to give additional free text comments about increased information sharing by the SHS, and this was done by 20 respondents. The need for prior discussion and informed consent was highlighted by several, for example: ‘I don’t see the point to this change, if the information is needed the patient deserves the right to choose who it goes to and why’, ‘it would be nice to discuss the GP letter on an individual basis’ and ‘I think confidentiality is important and the client should be able to decide what and how much information is divulged and to whom’. These comments demonstrate that patients want to be engaged in a discussion around sharing their information.
A series of chi-square tests were used to examine whether the respondents’ attitudes towards sharing information were related to any of the demographic variables. The only statistically significant result was for respondents aged 16–19 years, who were less likely to agree for all three information sharing activities (p < 0.05). Of particular note is that there was no association between those who attended for a stated reason of confidentiality and their likelihood to agree or disagree to any of the three information sharing activities. There were highly statistical significant relationships between allowing other hospital medical staff to access SHS results and agreement to the use of NHI on laboratory forms and agreement to sending a GP discharge letter, respectively, and also between agreement to the use of NHI on laboratory forms and agreement to sending a GP discharge letter, all at p = 0.000.
Table 1 provides details about attitudes regarding the use of NHI numbers on laboratory forms and what information could be shared. As respondents could choose several options in this question, the numbers exceed the number of respondents. Thirty-six per cent (72) stated that they did not know enough about the NHI, despite having being given written information regarding the NHI. Of the subset of respondents who were referred to the SHS, only 35 per cent (19) would agree to a discharge letter to their GP and 28 per cent (15) wanted to talk about it first. Thirty-seven per cent (20) of those referred outright disagreed with a discharge letter to their GP. A series of chi-square tests demonstrated no relationship between the types of information shared and any of the demographic variables. However, the relationship between sharing no information at all with disagreeing with the use of the NHI on laboratory forms, discharge letters to GP and other hospital staff accessing SHS test results was highly significant, all at p = 0.000.
Attitudes towards information sharing (N = total number of respondents for that question, n = number of respondents who ticked that they agreed with the statement).
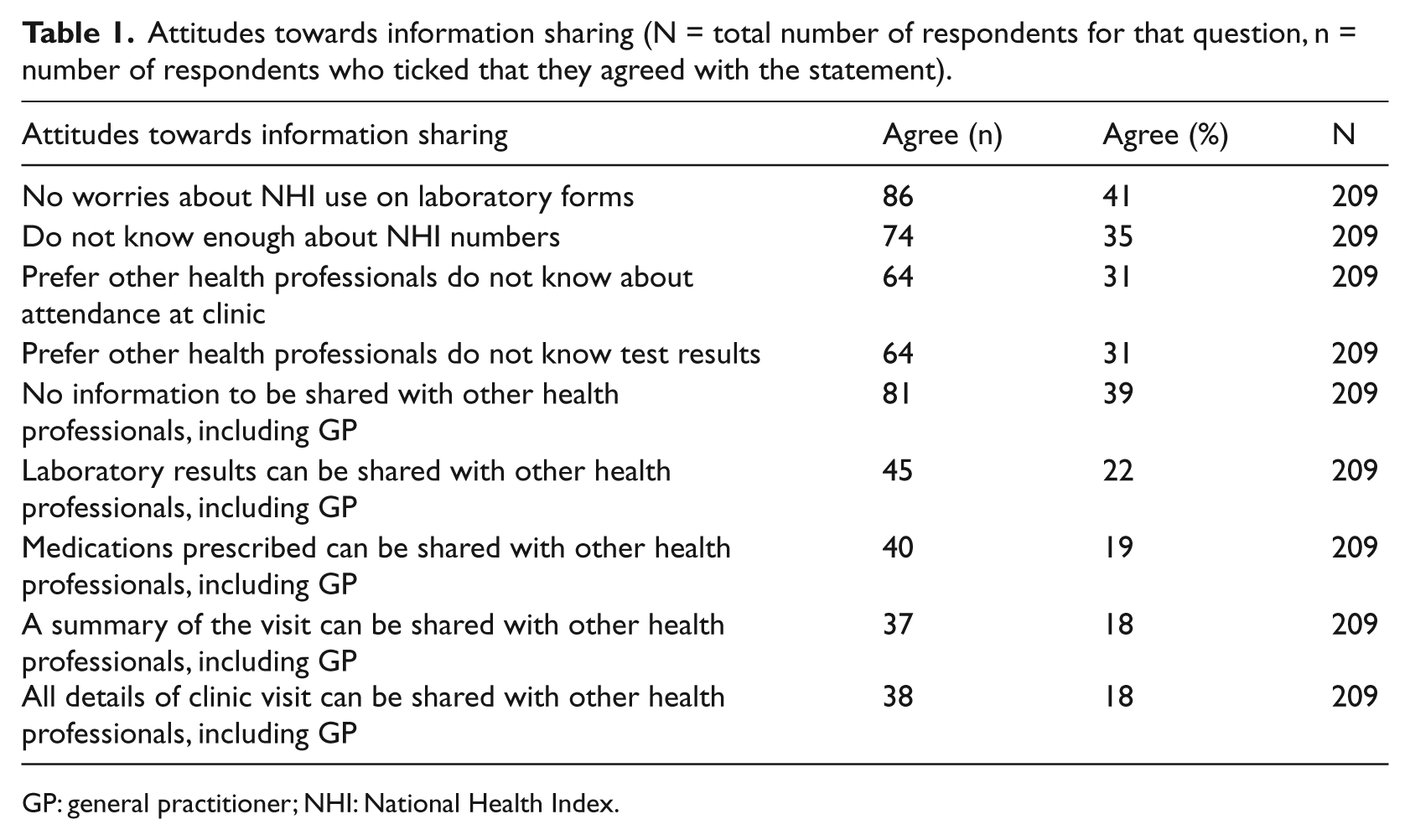
GP: general practitioner; NHI: National Health Index.
Again, several free text comments supported the need to maintain confidentiality and privacy, for example, ‘don’t really agree with the idea of information in regards to sexual health matters being shared with other medical staff’ and ‘I think that no one should know about teenagers coming to SHS. It should be held in confidentiality’.
Confidentiality and the need for informed consent were not the only reasons for disagreeing with increased information sharing demonstrated by the free text comments: the lack of a perceived need for sharing the information at all was also identified: ‘not in the GPs job description to know what tests are done at the clinic’, ‘haven’t been to the doctor in years so no need for him to know unless it is something fatal’ and ‘I don’t see any reason for a d/c letter to be sent to my GP’. One final reason given was a fear of negative perceptions: ‘I have received inadequate services from a GP in town. ID through NHI numbers may help him pass on his negative opinions’. There was only one positive comment from participants: ‘Obviously this is to benefit the patient extending lines of communication between GP and others is only in our best interests in the end and I would support the idea’.
Consequences of increased information sharing
In order to determine what impact a change to current information sharing practices might have on clinic attendance, respondents were asked to indicate how the use of NHI on laboratory forms and sending discharge letters to their GP might affect them (see Table 2). While it is reassuring that a significant majority would be happy to attend the clinic again and would encourage others to attend the clinic, 30 per cent (62) of respondents stated that they would not encourage others to attend if the SHS used NHI numbers on laboratory forms and 36 per cent (73) if the SHS sent discharge letters to GPs. Table 1 shows respondents’ attitudes to increased sharing of information, while Table 2 shows what actions, if any, respondents might take if information sharing was increased by the SHS. Comparing results across both tables found that the results from Tables 1 and 2 support each other. Respondents who would not encourage others to attend, would also use an alias or would stop attending the SHS were statistically associated with those who needed more information or disagreed with the information sharing activity (p < 0.001); for example, of the 61 respondents (31%) who would stop attending the SHS if a discharge letter was sent to their GP, 75 per cent disagreed with sending a discharge letter. These results support the existence of a group of patients attending the SHS for whom sharing of information by the SHS would be a problem and who may respond to a change in current practice by reduced attendance for diagnosis and treatment of any STIs.
Consequences of increased information sharing (N = total number of respondents for that question, n = number of respondents who ticked that they agreed with the statement).
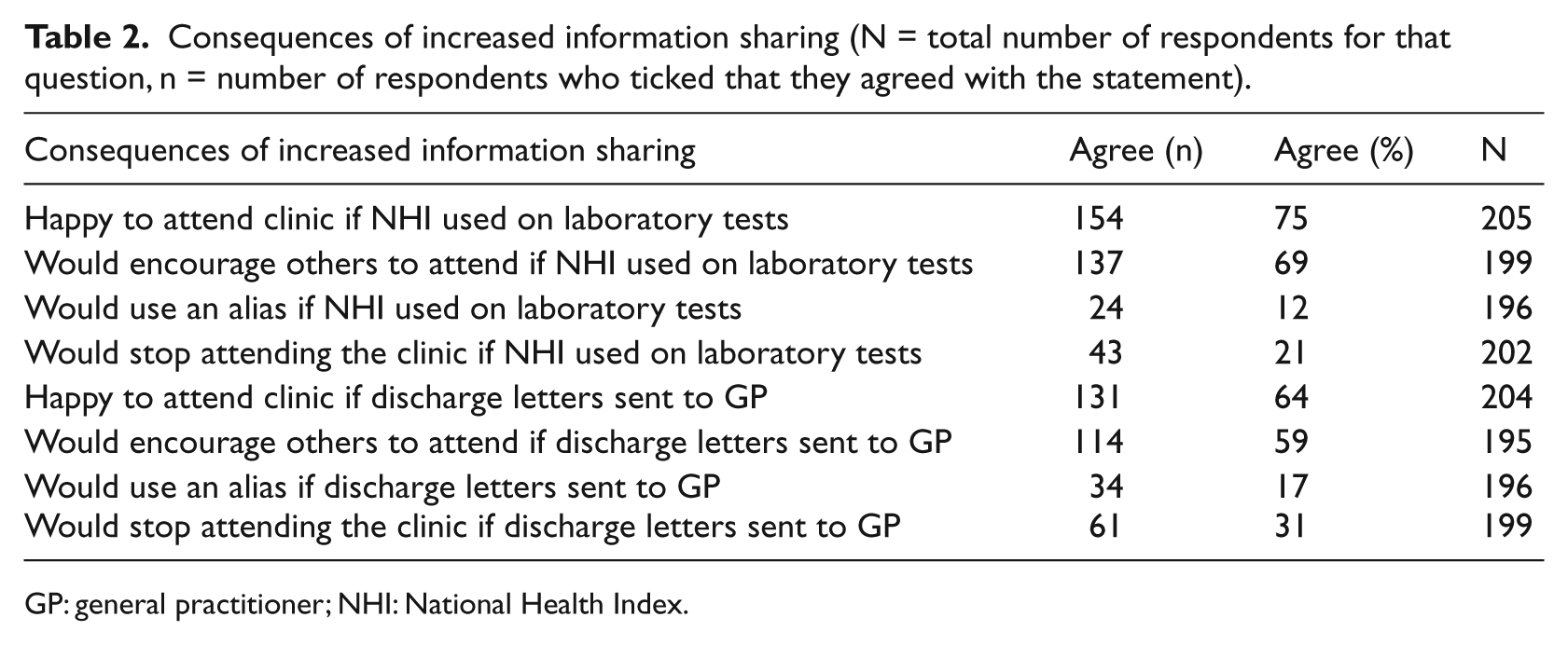
GP: general practitioner; NHI: National Health Index.
Discussion
Despite our previous research showing that members of the New Zealand public generally agree with sharing personal information with other health professionals, especially general practice/hospital doctors/nurses,19,21,22 39 per cent of SHS preferred that no information at all about their visit to the clinic be shared with other health professionals and 18 per cent agreed that all details of clinic visit can be shared with other health professionals, including their GP. Clearly information sharing from SHS is an area of concern for some patients. However, it was not possible to predict from routinely collected patient registration demographic data who may attend for reasons of confidentiality or cost (or indeed any reason for attendance). In particular, there was no association between those who stated that they had attended for reasons of confidentiality and their likelihood to agree or disagree to share information for any of the three information sharing activities; therefore, one cannot conclude that just because a patient said they attended because of confidentiality that they would disagree with sharing information about their visit to the SHS. This makes it difficult to predict in advance who may agree to increasing sharing of information from SHS and who may not.
Similar to a previous study with UK GUM clinic patients, 8 46 per cent of respondents in this study disagreed with other hospital medical staff accessing their sexual health test results and 49 per cent agreed that the SHS could replace the current separate SHS code on laboratory forms with NHI numbers. This indicates that the inclusion of all SHS laboratory results in regional repositories may cause a barrier to attending the SHS, given the 21 per cent of respondents who said that they would stop attending the SHS if NHI numbers were used. However, we acknowledge that proposed behaviour does not always predict actual behaviour, so the impact may be less.
Respondents aged 16–19 years were less likely to agree to any of the three information sharing activities. These findings are supported by the Office of the Children’s Commissioner (2006), which showed that it was very unusual for young people to agree to full information sharing and that selective information sharing generally required informed consent. This report found that young people would not talk to adults unless they trusted them, and confidentiality for their personal information was a core part of that trust. This was especially true for information regarding their access to mental and SHS. 10 Given the high numbers of this age group who attend the SHS, this finding is important and goes against the public perception, driven by social media use, that young people are happy to share their personal information – it may be that as long as the young person does the sharing it is okay but not for the health sector to do this.
Referred patients, however, were more likely to agree to a discharge letter to their GP (35% compared with 25%), although at a slightly lower level than previous studies,8,23 indicating that the concerns of patients attending sexual health clinics may not be limited to a provincial SHS in New Zealand. The SHS receives referrals (both formal written and informal verbal) from many different health professionals, so a respondent may have been referred to the SHS by a non-GP referrer, which may account for our slightly lower figure but warrants further investigation. These lower rates are in contrast with an almost universal acceptance of letters from outpatient clinics to GPs, indicating that the concerns of patients attending sexual health clinics are to some extent different from those of patients attending general outpatient clinics.
Acceptance rates were not increased by a selective sharing of information since medications, laboratory test results, a summary or all details were all equally unpopular (only 18%−22% agreed). It seems that anything relevant is acceptable, nothing is acceptable or there is a need for prior discussion. Indeed, 39 per cent of respondents in this study wanted more information and prior discussion regarding the discharge letters indicating that informed consent may increase acceptance rates. This finding aligns with a previous study at GUM clinics in the United Kingdom that found that 80 per cent of self-referred patients delivered a discharge letter to their GP following a detailed discussion of letter contents with the right to change content. 24
The need to address this high level of reluctance by SHS patients to share information is highlighted by the consequences of increased information sharing without any intervention. With separate coding systems from mainstream health services, SHS traditionally deliver care with a high level of confidentiality. This provides clients who feel unable to discuss sensitive issues with their GPs,15,16,25 or who have no GP, with an accessible alternative to primary care. This study demonstrates that there is a group of patients who would not attend the SHS and/or not recommend the SHS to others if information was shared. While proposed behaviour may not always predict actual behaviour, any increase in non-attendance at the service could have a significant impact on diagnosis and treatment of the rising incidence of STIs.7,16 This is of particular concern for specific populations at increased risk from STIs such as youth and indigenous populations 7 who make up significant percentages (30%−50%) of the sexual service patients and are identified as at risk of health inequalities in New Zealand. 26
Respondents who considered that they did not know enough about NHI numbers (35%) were statistically associated with having none/little prior level of NHI knowledge, supporting previous calls for patient education regarding the use of the NHI.5,27 Respondents had been provided with publically available written information from the Ministry of Health about the NHI 20 indicating that these documents were not read or not understood by the participants or are insufficient to answer patients’ questions regarding the use of the NHI.
The perceived need for confidentiality for SHS attendance may, at least in part, be due to a lack of knowledge about the benefits and risks (perceived or proven) of information sharing and the enhanced privacy protection offered by the use of UPIs. The best way to provide such patient education needs further investigation given the disappointing experiences from the introduction of Summary Care Record in the United Kingdom 28 and the Emergency Care Summary Record in Scotland. 29 One benefit of a population-based education campaign followed by a switch to an opt-out strategy may be that the use of UPIs and discharge letters by SHS would become normalised, a strategy that in addition may help to normalise attendance for sexual health care in general. Opt-out methods of consent have been successfully used in national screening programmes, such as the national cervical screening programme, 30 and in sensitive areas such as increasing the uptake of HIV testing. 31 However, an opt-out method of consent may be not be appropriate for implementing centrally stored summary care records, 29 as ensuring patients take full responsibility for their decision to opt-out (or opt-in) may not be possible 28 and current mass media education campaigns have not been successful in obtaining informed consent. 28
Limitations
The low level of awareness regarding NHI numbers shown by the respondents is a limitation of this study. A greater understanding of NHI numbers and how they work might have influenced responses. Maori and young people were over-represented in the respondents compared with national statistics 32 but are aligned with the demographics of the SHS attendees. The results of this study can therefore be generalised only to SHS with similar demographics. There may be greater privacy concerns in areas with a smaller population base or fewer concerns in those areas with a higher population density.
Conclusion
Confidentiality remains a significant concern for attendance at provincial sexual health clinics and is not mitigated by the use of UPIs. There are significant patient concerns toward increasing information sharing of clinic visits. Appropriately developed and implemented public education initiatives regarding the use of UPIs and the benefits for patients from sharing their personal health information with other health professionals are urgently needed to enable patients to make informed choices about their health information prior to the introduction of either opt-in or opt-out systems for routine information sharing from SHS. This study shows that regardless of national policy supporting increased information sharing between health-care providers, it is still necessary to keep clinic visit details confidential for some patients attending SHS.
Footnotes
Acknowledgements
We thank the patients who participated in this study, the Sexual Health Service that allowed us to recruit patients in their waiting room and Dr Barry MacDonald, Massey University, who advised on sample sizes.
Declaration of conflicting interest
The authors declare that they have no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Authors’ contributions
Contributors: I.H. conceived and designed the project, undertook the final analysis, co-wrote the industry report and drafted the article. G.H.E. conducted the initial literature review, assisted with questionnaire design, collected and entered data, undertook initial analysis and co-wrote the industry report. R.W. advised on project and questionnaire design. All authors revised drafts of the article. Clinical staff and line management of the Sexual Health Service advised on questionnaire design. All authors had full access to all the data in the study and can take responsibility for the integrity of that data and the accuracy of the data analysis.
Study approval: The study was approved by the Central Regional Ethics Committee, of the New Zealand Health and Disability Ethics Committees (Reference CEN/09/06/042).
Data sharing: No additional data available.
Provenance and peer review: Not commissioned; externally peer reviewed.