
Abstract
In this research in progress, a reference model for the use of electronic patient record (EPR) systems in oncology is described. The model, termed CICERO, comprises technical and functional components, and emphasises usability, clinical safety and user acceptance. One of the functional components of the model—an electronic document and records management (EDRM) system—is monitored in the course of its deployment at a leading oncology centre in the UK. Specifically, the user requirements and design of the EDRM solution are described.The study is interpretative and forms part a wider research programme to define and validate the CICERO model. Preliminary conclusions confirm the importance of a socio-technical perspective in Onco-EPR system design.
Introduction
The requirement for oncology-specific electronic patient record (EPR) systems can be viewed as a special instance of EPR requirements in healthcare. The wider field of EPR has been a subject of intense research in academic and practitioner circles over many years. However, research on EPR in oncology (‘Onco-EPR’) has been relatively muted. Early research includes perspectives on information display in oncology systems
1
and on the specific use of computers in oncology care.
2
More recently, others have presented a longitudinal analysis of an oncological EPR in a European setting.
3
In the USA, the ‘CORE’ project was initiated to establish
However, there is no detailed, consensus-driven reference source of oncology requirements or design model that addresses the delivery of radiation and systemic therapies coupled with the complexity of network-based service delivery arrangements in the UK. This research-in-progress is part of an initiative to redress this by developing a comprehensive model that encompasses all functional, data, process, inter-operability and socio-technical system requirements for successful implementation of EPR systems in cancer treatment services. The conceptual model, ‘CICERO’, is concerned with
This research assesses the extent to which the deployment of an electronic document and records management system (EDRM or EDRMS)—one of the functional modules referred to in the model and the repository for much of the unstructured data involved in Onco-EPR—will meet the requirements of the clinical users with regards to usability and ease of acceptance. It follows development of an EDRM system at the Clatterbridge Centre for Oncology (CCO) between October 2010 and July 2011 (a process that is still underway at the time of writing). The research is being conducted jointly by research staff at CCO, healthcare specialists at the University of Sheffield and by the EDRM product specialists (Kainos Software).
The research comprises a case study approach using questionnaires to gather respondent data. The survey of clinical staff provides a tangible basis for initial assessment of the requirements for the EDRM component of CICERO and socio-technical aspects of the system. The epistemological approach is interpretive and views computer systems embedded in a social context, not just as hardware and software components. This applies particularly to complex systems,such as Onco-EPR, which are highly dependent on the interaction between the clinical user and the computer system. The conclusions from this research will, therefore, have particular relevance for practitioners, whose work practices and perspectives are affected directly by EPR tools. Further research in this programme will examine other technical and functional aspects of the model.
This paper is structured as follows. The first part describes the nature and scope of the research and a brief review of the literature on EPR is provided in the second part. The third part presents an overview of the theoretical framework, research method and case environment. Then, the empirical data and the findings-to-date are presented. Finally, opportunities for further research are identified.
Contextual literature
EPR systems
An EPR is a sub-type of an EHR, and is defined as ‘a repository of patient data in digital form, stored and exchanged securely, and accessible by multiple authorized users. It contains retrospective, concurrent and prospective information, and its primary purpose is to support continuing, efficient and quality integrated health care’. 5
There has been extensive research on the development and implementation of EPR systems in healthcare. A comprehensive summary of the research literature in 2008 considered how EHRs are defined, how the structure of these records are used, who has access to EHRs, which data components are used and studied, what the purpose of research is in this field, what methods of data collection have been used in various studies and what the results were. 6
The literature identifies key design considerations for effective EPR systems. First, the structure of the EPR should be derived from detailed, empirical knowledge of the practice involved rather than on prefixed notions of the organisation and content of medical work. 7 Second, it is crucial to ensure that the systems yield immediate benefits for primary users: the systems should support work, not generate it. Third, designers need to be aware of the socio–political nature of seemingly ‘neutral’ tools such as EPRs. 7
Onco-EPR systems
EPR systems that support cancer services must take into account the specific areas of practice that differentiate oncology from other clinical specialties. Examples include the requirements for accurate tumour staging, flow sheets, the need for multi-disciplinary team documentation, integration of laboratory and imaging reporting, and dealing with chemotherapy ordering and toxicities. 4 Particularly demanding is the ordering, documentation and management of chemotherapy and ancillary medications. 8
Oncology EPRs can offer improved patient safety, clinical efficiency and availability of medical information. However, it is critical to establish principles of safe practice that govern the design of the EPR, its functionality and its integration with the clinical workflow of the treatment centre. In fact, the evaluation and implementation of an EPR provides an opportunity for hospitals to evaluate overall practice principles and to improve patient safety and clinical efficiency. 8
Electronic document management in healthcare in the UK
In the UK, many hospitals are now procuring EPR systems in the expectation that they will simplify and automate inefficient and slow processes. The aim is that patients will be registered electronically, theatre slots will be automatically checked for scheduling clashes and formularies will be verified in real time for the prescription of generic, rather than branded, medicines. The belief is that EPR will help hospitals reduce, and eventually eliminate, reliance on paper.
However, the reality of EPR installation does not live up to the EPR vision. This is largely because, for most hospitals, the bulk of current patient records exist on paper and most business and clinical processes have been built around a paper-based information flow. Thus, even after EPR installation, some processes remain heavily paper-based. 9 In addition, migration to the EPR environment is complex, time-consuming and often unsatisfactory as large sections of paper-based information cannot feasibly be rekeyed or converted to an electronic medium. Furthermore, the challenge of changing existing business processes is greater than many organisations can absorb without a detrimental impact on everyday operations during, and after, EPR installation. In an effort to create a totally paper-free environment, hospitals have had to construct cumbersome electronic solutions.In short, EPR installations have rarely removed the need for hospitals to maintain a sizable and active medical records library service.
As a consequence, there is increased demand for specialist electronic document management (EDM) systems to bridge the gap between paper-intensive environments to fully digital information environments. These systems scan, digitise and store paper records, and can be integrated with other patient information and clinical systems. This allows presentation of a more comprehensive view of the patient record, enabling the clinician to see the electronic information from the point of implementation through the EPR, integrated with other patient data. As for EPR systems, EDM solutions only work effectively when they are aligned with clinical practice and meet patient safety and information governance requirements. 10
Deployment of EDM systems is at an early stage in the NHS in England. It is well established in hospitals in the USA, where examples of EDM being used to support cancer treatment services date back to 1988. 11
Socio-technical perspectives
A socio-technical perspective refers primarily to the view that a technical system inevitably affects, and is affected by, the interdependent social system within which, and upon which, it operates.12, 13 EPR design and implementation projects often fail to appreciate that an EPR computer system is only one part of a complex human activity system, leading to unforeseen complications, delays and increased costs. This applies particularly to complex systems like cancer treatment services, which are highly dependent on the interaction between the clinical user and involve multiple organisations and a range of often disparate computer systems.
This is validated by empirical research, which highlights the point that an inadequate understanding of how people and organisations adopt information technology (IT) has been a major factor leading to the failure of healthcare information systems. 14 This has led to recommendations that a socio-technical approach should be taken when designing clinical IT systems, 15 and to the development of guidelines and mechanisms to support such design principles and approaches. For example, the STAT-HI tool 15 collates evidence-based, good practice recommendations into an annotated checklist under four socio-technical categories: culture; governance and risk; managing change; and technology. Each category contains a list of factors for consideration by health informatics (HI) implementation teams.
In cancer treatment services the socio-technical challenges associated with EPR implementation were investigated by Reidl 16 who found that the political context frames the conditions for an IT project in many ways; organisational fragmentation blurs, or even prevents, awareness of things going wrong; configurational incompatibilities result in lack of ‘fit’; and there can be a profound misunderstanding of user participation.
This implies that the methodologies used in information systems research, particularly in healthcare, must be appropriate. Greenhalgh 17 advocates viewing eHealth evaluation as a ‘social practice’ and argues: ‘…that the assumptions, methods, and study designs of experimental science, whilst useful in many contexts, may be ill-suited to the particular challenges of evaluating eHealth programs, especially in politicised situations where goals and success criteria are contested’.
Research method, theoretical framework and case environment
Research method
This component of the overall research programme comprises a case study approach using a design workshop with clinical stakeholders and questionnaires to gather respondent data.The epistemological approach is interpretive and adopts a perspective that views computer systems embedded in a social context and that it is often the social context that gives rise to the most interesting and problematic aspects of information systems (IS). The reason for using an interpretive case study is because it can potentially distil the experiences of practitioners and thereby develop a theory that is both relevant and grounded.18, 19 Yin notes that the case study benefits from the prior development of theoretical propositions to guide data collection and analysis. 20 Accordingly, this study is inductive rather than hypothetic-deductive. In selecting an interpretive approach at the outset, the researchers do so with the awareness that there are other ways of looking at the model and do not preclude the use of a multi-method approach at a later stage of the research programme.
Theoretical framework
The CICERO model is intended as a preliminary framework for this particular research; in effect, an inductive theoretical phase to be followed by a validation phase. It does not describe a toolset or system solution; rather, it is a conceptual framework designed to support further research in this area from which practical guidelines for practitioners and commercial technology providers will emerge. In this respect, it is intended to follow the path of similar models which started as theoretical constructs that emerged from IS deployment and were subsequently subjected to validation and empirical study.
Functional modules specified for inclusion in CICERO are at various stages of development and implementation and include an integrated patient administration system (PAS); order communications and results reporting for pathology and radiology; electronic scheduling, prescribing and drug administration for complex chemotherapy regimens; radiotherapy action sheets, scheduling and pre-treatment workflow; messaging integration with radiotherapy treatment systems; integration with picture archiving and communication systems; an electronic document and records management system for unstructured data; nursing assessments and care planning forms; a patient journey management module; bed management; and consultant and patient level dashboards, providing work lists and personalised views of the system (Figure 1).
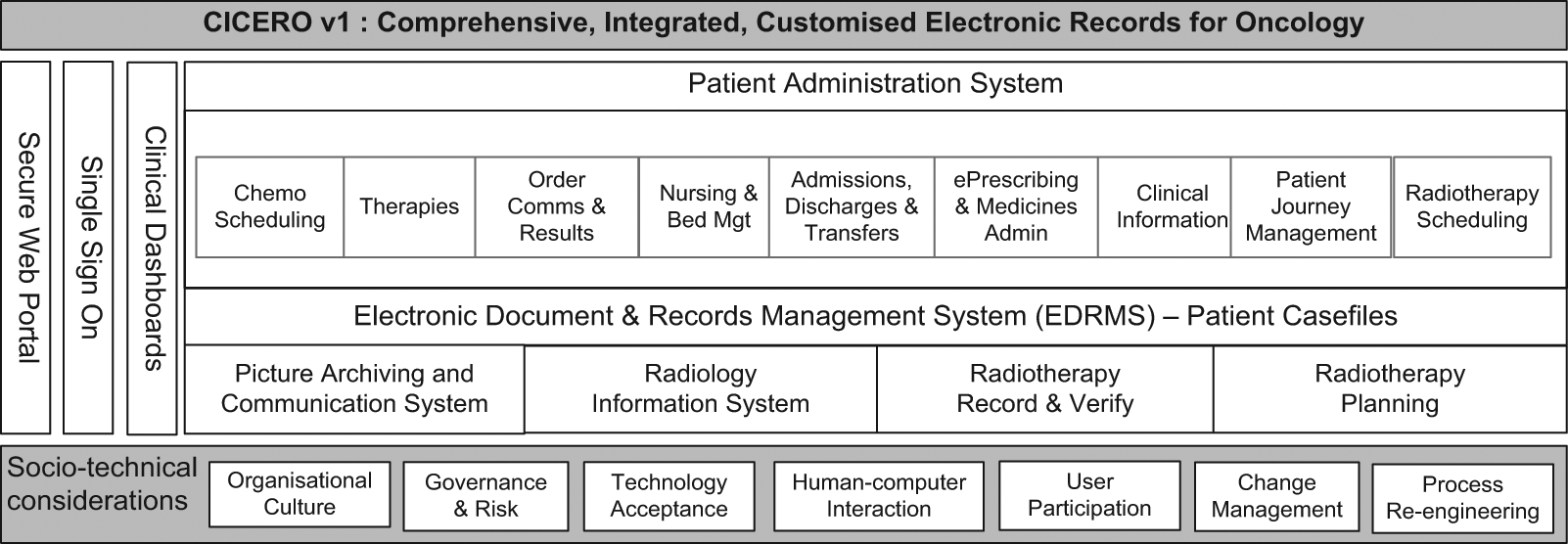
CICERO v.1
This article is concerned with the EDRM component of CICERO. The primary research site developed a business case and a functional requirements specification to procure an EDRM to integrate seamlessly with a new version of hospital’s main EPR system. In September 2010, a project was initiated to implement the Evolve EDRM system (developed by a third party, Kainos Software) as a core component of the Onco-EPR. The integration of the EDRM and EPR systems involves the exchange of messages, or notifications, between them that include:
Health Level 7 (HL7) patient demographic data feeds to the EDRM to support case file creation, metadata updates and case file merges;
launch of a web-based patient-level view of a case file from within the EPR (which effectively calls a search within the EDRM and passes the patient unique reference number as the search parameter);
a HL7 notification from the EDRM to EPR in the event that other types of documents are added directly to the EDRM;
a ‘push’ mechanism to pass portable document file (PDF) documents created and approved in the EPR system to the EDRM for inclusion in the patient case file.
Case study
The data for the overall programme of research, and for this particular phase of the research, is primarily gathered from practitioners and clinicians in a leading oncology centre in the UK.
CCO is one of the largest specialist NHS cancer centres in the UK, with more than 7500 new patients registered each year. Located near the city of Liverpool in the north-west of England, it serves a population of 2.3 million and delivers treatments through radiotherapy and chemotherapy services. CCO uses advanced technology to detect malignant disease and plan treatment, and provides rehabilitation and supportive care to address the palliative aspects of care and needs of family supporters. CCO also delivers chemotherapy treatments at off-site clinics in seven locations.
Patient records are currently stored in both paper and electronic format, with the primary record being the paper-based medical record. A survey conducted in 2010 21 found that for 25.1% of respondents (n = 130) patient records, whether electronic or paper-based, were often unavailable when they needed them. Twenty-three point eight percent of respondents also stated that they were concerned that the information upon which they make decisions is inaccurate, not up-to-date or incomplete.
The hospital’s Information Management and Technology (IM&T) strategy is focused on developing fully electronic patient record systems and the technology used for the EDRM system centres on the Evolve product developed by Kainos Software, a specialist technology organisation. The main purpose of Evolve is to maintain a digital record of patient files, including historic paper records currently stored in offsite archives and remote clinics. These records are scanned into Evolve using document imaging technology, stored as PDF files and integrated with patient data that exists in other systems. Evolve is tightly integrated with the hospital’s primary EPR system, MAXIMS, a proprietary software package. The user interface to the Evolve patient record is provided both natively through the Evolve web-based interface (clinical portal) and via the MAXIMS interface, which is familiar to the clinicians and administrators.
Empirical data and findings-to-date
Workshop and questionnaire data
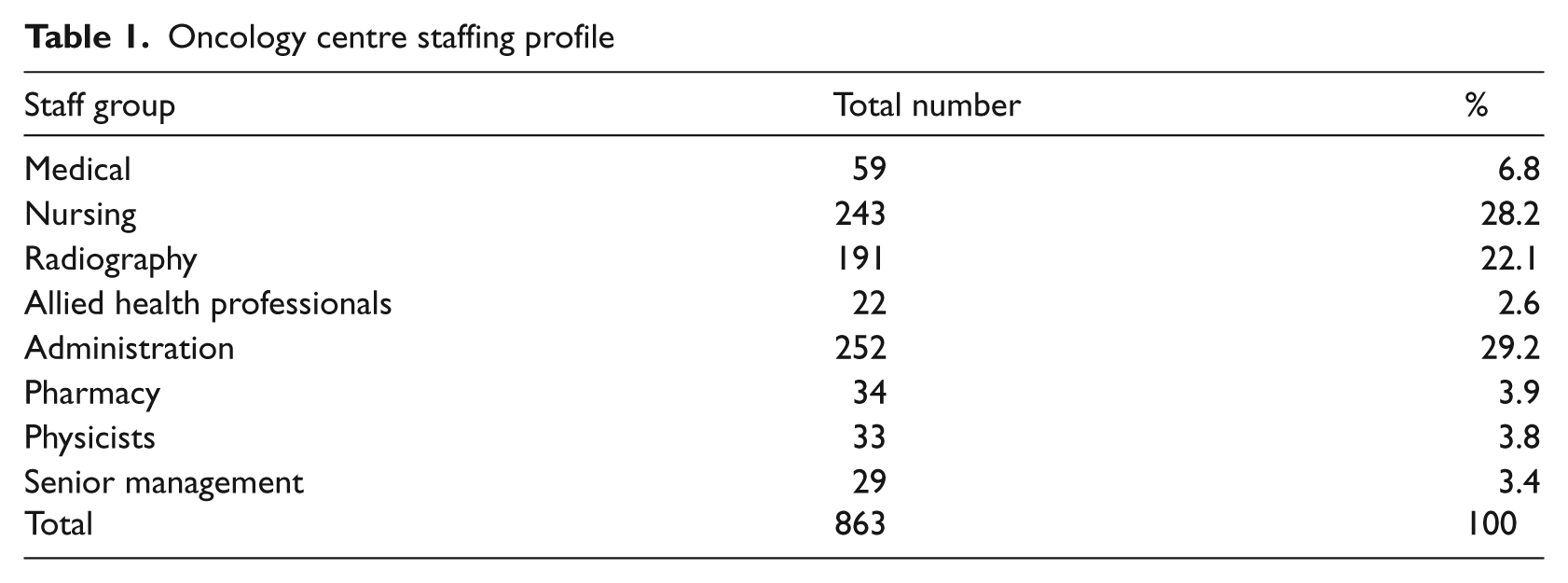
Data collection was facilitated via a design workshop with clinical stakeholders and a questionnaire issued to all staff (n = 863) at the primary research site. Staff at the centre can be broadly categorised into the groups listed in Table 1.
Oncology centre staffing profile
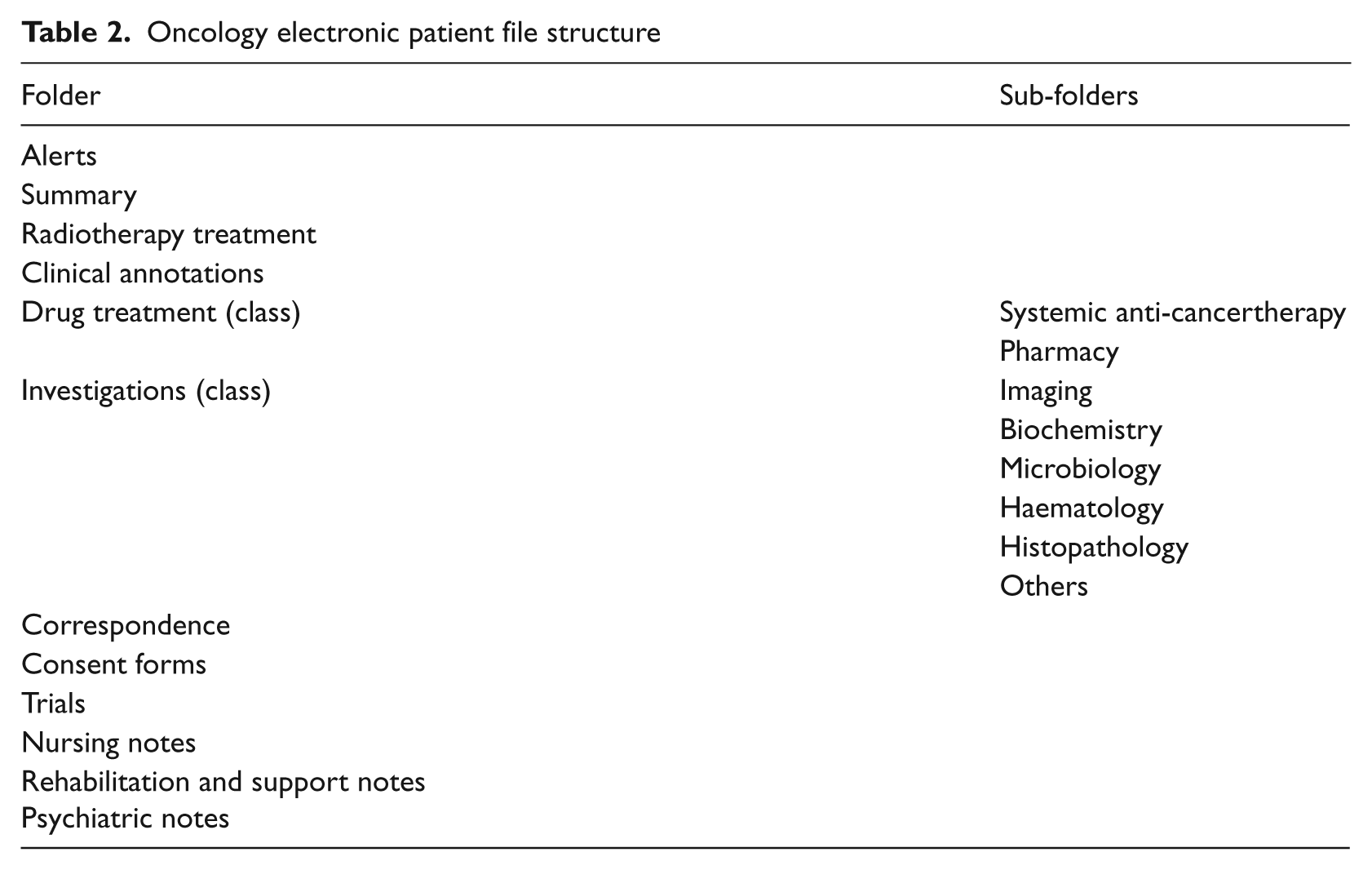
A small group of stakeholders attended the design workshop, including the clinical directors of the radiotherapy and chemotherapy departments, and medical and clinical oncologists. Using a participative design approach, 22 informatics specialists from Kainos and the hospital’s IM&T department demonstrated the Evolve system and led discussions about design and configuration options. The structure of the existing paper-format oncology patient record was reviewed and changes were identified to configure an electronic case file. Through group discussion, the clinicians agreed that their preferred structure for electronic documents would contain 12 classes, 2 of which would include sub-folders for specific categories of information, as depicted in Table 2.
Oncology electronic patient file structure
The survey questionnaire was issued to all staff at the research site and requested qualitative data on the use of paper medical notes, use of the current EPR system and on perceptions of the impact of moving to fully electronic patient records on clinical, medical and administrative job roles. The questionnaire included 20 questions and took 5–10 minutes to complete. System usability questions were based on established IBM Computer Usability Satisfaction Questionnaires. 23
Findings-to-date
Although the analyses are not yet complete, it is possible to draw some basic conclusions from this phase of the research programme. First, regarding the research methodology, the conceptual framework is proving adequate both in structuring questions and categorising responses. Similarly, many of the theoretical antecedents are useful in analysing the results.
Second, the workshop approach has demonstrated willingness of the hospital’s clinical and medical practitioners to be involved in system re-design activities. This in itself is a positive outcome, as early and frequent involvement from system users is considered an essential socio-technical design principle. In the next phase of the project it will be possible for users to gain first-hand experience of the EDRM sub-system through the deployment of a ‘model office’ environment, which comprises an implementation of the configured solution offline—that is not for use in live operation. This will provide a tangible basis for further assessment of the socio-technical aspects of the system. Over the course of the model office operation, a sample of clinical, administrative and technical users will be asked to complete a questionnaire that addresses the usability of the system, with particular reference to the interface and integration of the system with other sub-systems. The questionnaires will be supplemented with data gathered in a series of semi-structured interviews with a smaller sub-set of users, primarily to gain a more rounded view of usability.
Response rate
Finally, the questionnaire responses highlighted the significance of the EDRM component of CICERO. It is estimated, based on advice from senior managers at the hospital, that a total of 627 staff were eligible to participate in the survey, as users of either paper-based or EPRs. Of these, 130 staff participated in the survey (response rate = 21%).
Sample characteristics
Table 3 provides the numbers of respondents and the response rates for each staff group.
Survey response rates
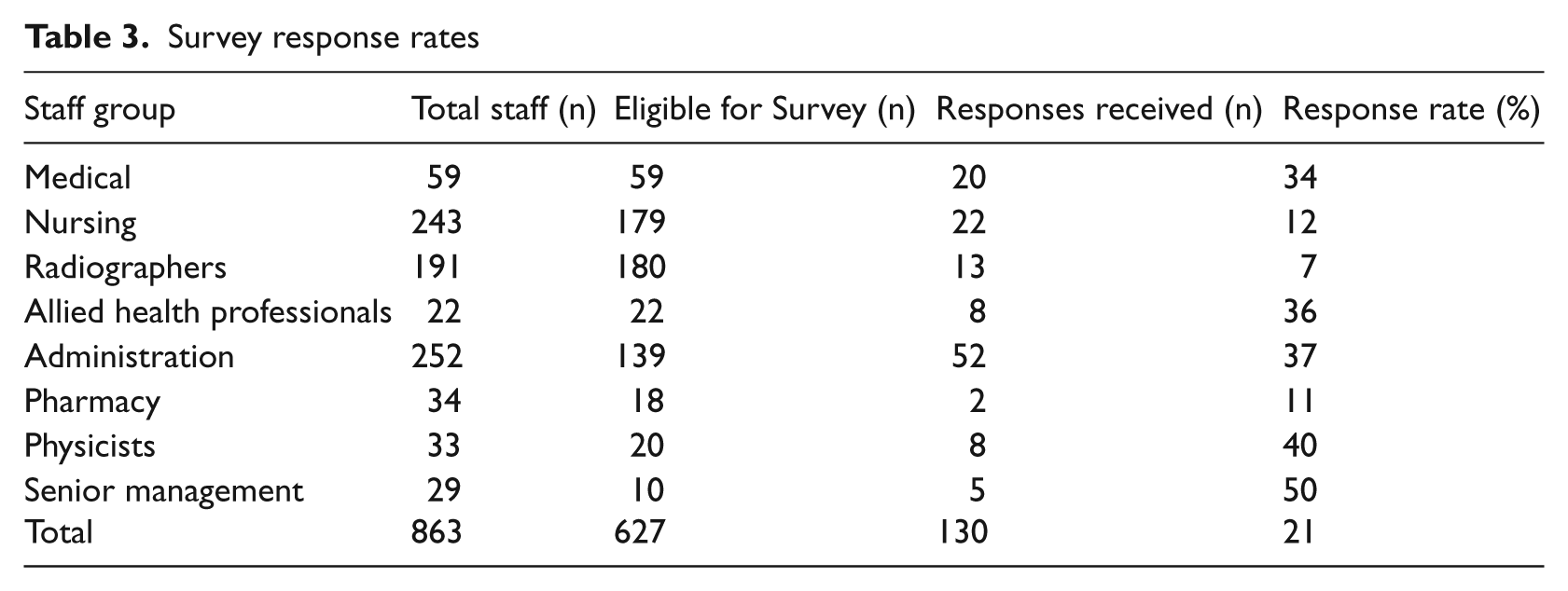
It can be seen from Table 3 that the largest number of responses came from administrative staff (n = 52), followed by nursing (n = 22) and medical (n = 20) staff. The response rate differed across the staff groups, the highest being among senior management (50%) followed by physicists (40%) and administrative staff (37%).
To facilitate data analysis, radiographers, allied health professionals, pharmacists and physicists were included in a single category (‘Allied and other health professions’), and senior management and administrative staff were included in a separate single category (‘administration and management’). Overall, 51 respondents (39.2%) had been working for CCO more than 10 years, 32 (24.6%) had been working for the Trust for 6–10 years, 35 respondents (26.9%) had been working for the Trust for 1–5 years and 12 respondents (9.2%) had been working for the Trust for less than a year.
Preliminary analysis of the survey results has focused on the relationship between different staff groups, their access to, and use of, paper-based medical notes and their views on the potential impact of implementing fully electronic patient record systems.
Use of paper-based medical notes
Overall, 98% (n = 127) of respondents used paper-based medical notes in their job roles. Of these, 98 respondents reported using paper-based notes on a daily basis, 17 respondents used them occasionally (e.g. on weekly basis) and 12 respondents reported using paper-based notes rarely (e.g. for audits). There was a significant association between staff group and frequency of using paper-based notes (χ2 = 21.10; df = 2; p < 0.001). Of the 42 clinical staff (nursing and medical), 40 used paper-based notes on a daily basis (98%), whereas only 15 of the 31 allied and other professions used paper-based notes on a daily basis (48%) and 43 of the 57 administrative/management staff (75.4%) used paper-based notes on a daily basis. There was no association between length of time working for the Trust and frequency of using paper-based notes (χ2 = 4.235; df = 2; p < 0.237).
Access to patient medical notes
More than half of respondents (n = 66; 52.8%) reported that they do not always have access to a patient’s medical notes file when they need them. There was no significant association between the staff group and whether respondents always had access to a patient’s medical notes file when they needed it (χ2 = 2.63; df = 2; p = 0.268). Of the 42 clinical staff, 20 (47.6%) reported that they always had access to a patient’s medical notes file when they needed it, compared with 11 of the 31 allied and other health professional (35.5%) and 28 of the 52 administrative/managerial staff (53.8%).
When respondents who said that files were not readily available were asked how long they had to wait for access, 27% (n = 23) said they had to wait for a whole day or longer. When asked how long they kept files in their possession, 22% (n = 29) of respondents selected ‘three days or more’.
When asked what action they would take in an event where a patient’s file was not available, more than half of medical staff respondents (n = 12) stated that they would locate the last clinical letter in order to proceed with a consultation. Other medics responded to say that they would ‘continue without notes’ or ‘piece information together from memory’. Other clinical staff indicated they were less likely to continue working with a patient, with both nursing and radiographers reporting that they ‘cannot work without the complete record’ and ‘cannot treat [the] patient’ or that they would ‘defer seeing that patient and treat another patient instead’.
Participants reported that a range of different tasks are carried out using the medical notes. All medical staff respondents reported using the medical notes to review the patient’s problems and seek out specific information, with 80% (n = 16) using them to obtain the results from tests or investigations. Ninety-five percent (n = 19) reported using the medical notes file to record daily notes about the patient; 80% (n = 16) of medical staff reported using the notes for clinical audits and 70% (n = 14) used them for research purposes; 15% (n = 3) stated that they used the notes to facilitate subject access requests.
Administration staff reported using the notes for a variety of other purposes, including clinical coding (15%, n = 8), filing Trust documents (63%, n = 33) and filing documents originating from referring hospitals (46%, n = 24).
Perhaps the most concerning finding though, was that 64% (n = 84) of all respondents said they suspect that a patient’s medical notes file that they are working with is not fully up-to-date (i.e. clinical letters not present or recent documents have not yet been filed).
Use of current EPR systems and potential impact of EDRM
Further analysis is required regarding the use of EPR systems by participants, 86% (n = 112) of whom reported using the Trust’s existing EPR systems.
Preliminary analysis found no significant association between staff group and overall satisfaction with the current EPR systems (χ2 = 18.16; df = 8; p = 0.20). Medical staff appeared to have the widest variation in views, in that an equal number of respondents (37%) were satisfied and dissatisfied with the existing systems. This may indicate a wide variation in requirements and expectations about how an EPR system should support the work of medical staff.
In order to establish their views on the potential impact of patient records becoming fully electronic, participants were asked to respond to eight questions using a Likert scale rating. Table 4 provides a summary of the results from four positive statements used for this question—these were balanced in the questionnaire with similar negative statements about the impact of fully electronic records to avoid response bias arising from respondents ticking the same category across a set of positive statements.
Perceived impact of EDRM
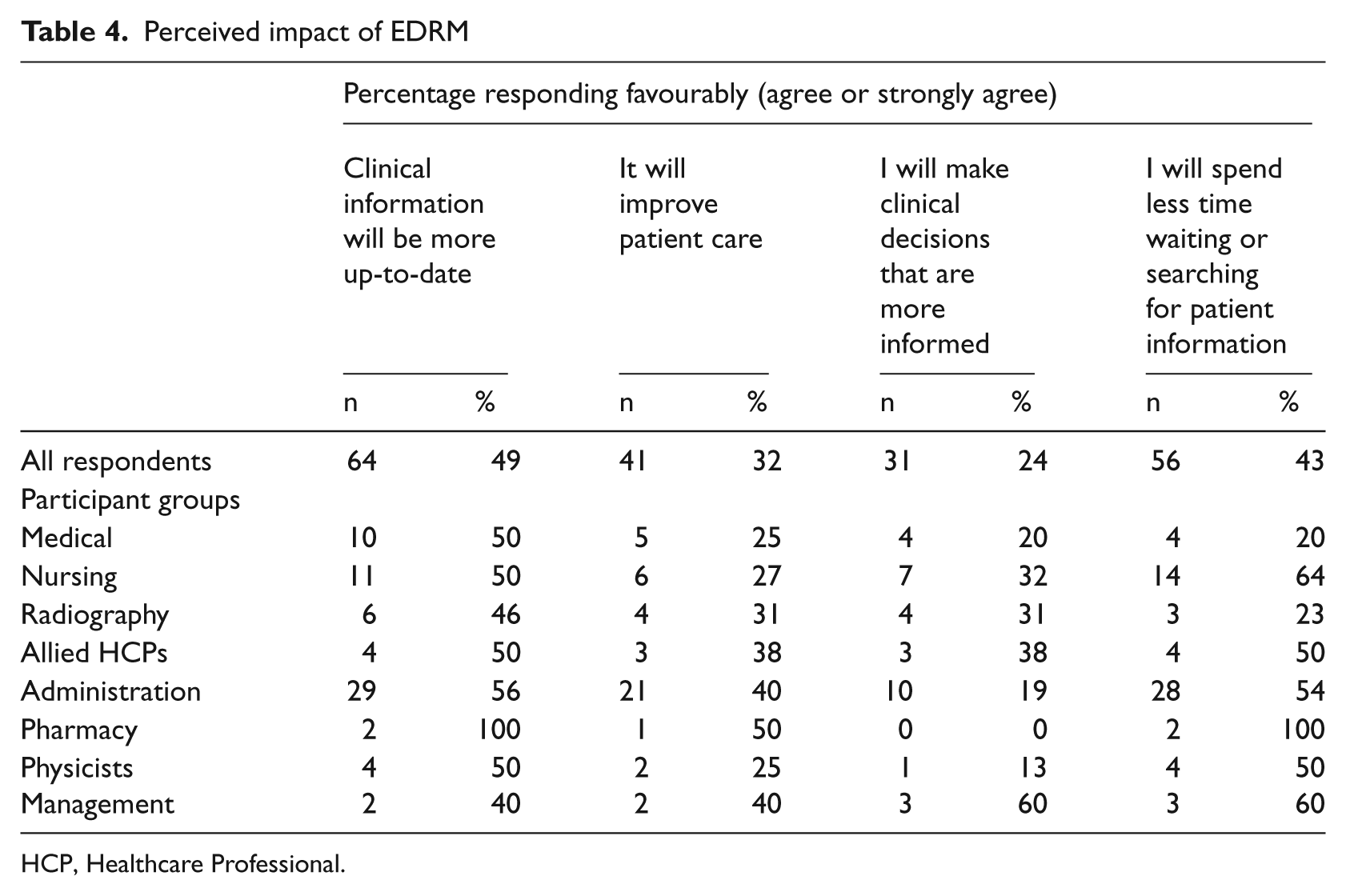
HCP, Healthcare Professional.
Although the initial analysis indicates a good case for EDRM, with just under half (43%) of respondents reporting that they think they will spend less time waiting or searching for patient information when patients records are fully electronic and half (49%) expecting that clinical information will be more up-to-date, the results relating to information security, efficiency when completing clinical tasks and interaction with patients are less clear and require further analysis to understand possible different perspectives from different staff groups. It is intended to conduct a follow-up survey once the EDM component of the CICERO model is fully deployed, which will enable a comparison of perspectives pre- and post-implementation.
Further research in this field
In this study, we assessed the potential benefits of the EDRM component of the oncology EPR suite. In further research, the CICERO model will be developed fully and published for use by informatics professionals, researchers and software vendors, with a view to improving the quality, efficiency and overall success of EPR system implementations for the benefit of clinicians and patients.
The next stage will involve further development and elaboration of CICERO and case studies relating to the development and implementation of other EPR sub-systems within the model. This will be based on empirical findings from this project, the researcher’s professional knowledge and findings from the literature. It will emphasise particularly the socio-technical aspects of the design and lean heavily on experience gained from interaction with clinical users. To this end, further engagement with oncology clinicians at the primary research site (CCO) will obtain feedback (using questionnaires, semi-structured interviews, and other related techniques) to establish their perspectives and system requirements. This will allow consolidation of views and the subsequent refinement of the conceptual model, which will then be validated by soliciting responses from clinicians at other dedicated cancer centres in the UK using a questionnaire-based survey. Triangulation of the quantitative survey results with qualitative interview data will help develop a final version of CICERO.
Future research on CICERO will also explore the validity and use of socio-technical assessment tools such as STAT-HI in more detail. At present, the tool appears to have some validity, but there is little evidence of its utility in terms of its application to current or recent HI projects. The authors acknowledge that further research is needed to determine effectiveness and suggest that essential content for the checklist may also be added from analysis of case studies of failed HI projects.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.