
Abstract
Whereas in most sectors, technology has taken over trivial and labour consuming tasks, this transformation has been delayed in the healthcare sector. Although appropriate technology is available, there is general resistance to substituting ‘warm’ hands with ‘cold’ technology. In the future, this may change as the number of elderly people increases relative to the people in the work force. In combination with an increasing demand for healthcare services, there are calls for efforts to increase productivity in the sector. Based on experience data from previous studies on information and communication technology efforts in the healthcare sector, we quantitatively assess the use of smart house technology and video visits in home care. Having identified healthcare providers, hospitals and relatives as the main affected groups, we show that smart house technology is cost-effective, even if only relatives gain from it. Video visits, which have higher implementation costs, demand effects on both relatives and health care providers in order to be a cost-effective tool in home care. As the analysis is purely quantitative, these results need to be complemented with qualitative effects and with more thorough discussions of the ethical, medical and legal aspects of the use of technology in home care.
Introduction and background
In most industrial sectors, machines and technology have taken over trivial and labour consuming tasks and have thus released human labour to more demanding tasks. In the healthcare sector, however, this move has been delayed. Although appropriate technology is available, there is huge resistance to implementation in the sector’s activities,1,2 but this may change in the future. One of the future demographic challenges is a shortage of ‘hands’ to carry out nursing care tasks, especially in elderly care. 3 As a consequence, technology will probably be a necessary supplement if the sector is to remain capable of taking care of its current tasks. One argument used to explain the delay of technology implementation in the healthcare sector is the lack of studies demonstrating economic gains of such projects.4–7
In this article, we use results from previous studies on the use of information and communication technology (ICT) in general, and smart house technology (SHT) and video visits in particular, to discuss the use of these technologies in home care, with a special focus on elderly home care patients. We show that both technologies may be cost-effective but, owing to lower implementation costs, we should expect to see more widespread use of SHT than of video visits in home care. The fact that we still only see limited use of these technologies in home care is probably a result of ethical and medical considerations, and qualitative aspects of the use of these technologies, and not economic considerations.
Smart house technology (SHT)
SHT is especially promising when considering patients with dementia, an illness that an increasing share of the population will suffer from, according to demographic trends. SHT implies installing devices such as fall sensors, global positioning system (GPS), and smoke detectors to enable elderly people to live longer in their homes. The devices are connected to a personal computer (PC) at the home care providers’ offices and then further to the on-call nurse’s mobile phone. Each time unusual scores on the devices arise in the home of a patient, the phone alarms the nurse.8,9 West Lothian, a community in Scotland, may serve as an illustration. Every person above the age of 60 years was offered a technology package to be installed at home. The sensors and detectors were connected to a call centre, which registered unusual (high or low) values. An evaluation of the project showed that a large majority of the elderly people in the community accepted the technology package and that using it increased their quality of life. The community spending on elderly care did not increase, even though the technology package was offered for free; in some instances, the costs were even reduced. 10 SHT has also helped reduce hospital admissions, promote earlier discharge and reduce the length of stay in hospitals. Interestingly, and very relevant for this article, delayed entry into nursing homes and a reduction in need for home care are reported, but quantification of these effects is not given. 11
In contrast to this, a Finnish study of technology use in home care concluded that the use of ICT does not necessarily satisfy the needs of the elderly. 12 The argument is that the effects of ICT are assessed too positively because it is not taken into account that the health conditions of the patients may prevent them from efficient use of the devices. It is necessary to adjust the technology to the patients’ level of coping capabilities for it to be useful and efficient in home care. One has to be concerned about the relationship between the problem the patient is facing, the functional ability of the patient, and the ICT solution chosen. Not everyone will be able, or willing, to use the technology. 13
Video visits
Video visits imply that the nurse calls the patient via the television. A two-way video camera enables the nurse and the patient to communicate and see each other at the same time. The nurse can then instruct the patient to perform simple tests by themselves, such as measuring the blood sugar, and report the result back, and thus the nurse saves travel time and costs. The patient groups most eligible for this technology are those with chronic diseases and patients in need of constant surveillance of body functions.
Several studies show that patients are satisfied with the quick and comprehensive information they receive through video visits, and that elderly people are also very satisfied with such visits.14–16 However, most patients preferred a combination of home and video visits.17,18
There are a few studies demonstrating economic gains from video visits. One shows that, whereas the costs of a physical visit varied between US$126–141, the cost of a video visit was U $29. 19 One of the most cited studies of the effects of video visits is the ‘Kaiser-Permanente tele home health research project’. 20 Patients diagnosed as having chronic diseases, e.g. chronic obstructive pulmonary disease (COPD), were eligible for the study, and those selected were patients newly referred to home care at one of Kaiser Permanente’s home care agencies for a limited period of at least four weeks. The average age of patients was 70 years. Patients were randomly assigned to a control and an intervention group. Both groups had access to routine home care and the intervention group received video visits in addition. The study showed no differences in quality indicators and patient satisfaction. The average direct costs for home health services were US$1830 for patients in the intervention group and US$1167 for patients in the control group. However, after considering the costs of rehospitalisation, there was a cost saving of US $63 per patient in the intervention group.20,21 This study was the first to demonstrate that tele home care is capable of maintaining quality of care while producing cost savings. Later, this result was supported by another study of the use of tele home care in a large urban home health care company. 21
However, evaluation of a Swedish experiment with the use of video conferences in home care was more sceptical, even though some positive results were reported. 22 The Swedish study is not entirely comparable to the Kaiser Permanente case, as it is concerns communication between hospitals and home care services with patients involved. Nevertheless, it points out that most patients were rather passive during the video conference due to high age and/or diminished mental or physical health, the way the video media affected their communication and the quality of the technology. Also, the staff did not spend less time on video conferences than on face-to-face meetings, and as a result, the experiment did not reach the goals set.
Method and data
We applied a cost-effectiveness analysis to assess whether ICT in the form of SHT and video visits may be cost-efficient tools for use in the home care sector. 23 Using experience data from previous studies and from the actual use of the technologies, we derived the net costs of the implementation of the technologies and related the costs to the assumed effects. We concentrated on quantitative and measurable effects, being aware that, in addition, there were non-measurable effects that were not taken into account in our analysis. The identified effects we concentrated on were: 1) time and resource savings for the home care providers; 2) time savings for relatives; and 3) resource savings for hospitals. There are also effects on the police and fire departments, where there are several anecdotal examples, but little scientific evidence on how SHT may prevent fire and flood in the homes of elderly people and prevent search operations for disoriented elderly people by triggering an alarm if they go out at unusual times of the day. Such effects are not taken into account. Neither have we taken into account qualitative effects, such as feeling safer when living with SHT, which can be the case both for the home care patients and their relatives 8 , and the feeling of having more control over your own body functions, as reported in studies of video visits.14–16
Crucially, the results depend on the alternative to increased use of ICT and on how new technology is introduced. The alternative to SHT is either that the home care patients live at home without this technology or they live in a nursing home. Video visits can either substitute some physical visits, or they can be in addition to physical visits (as in the Kaiser Permanente experiment).
Capital costs
Both SHT and video visits are characterised by relatively low capital costs. Costs for acquiring SHT are collected from the Norwegian department of an international company that produces and markets such devices (Siemens Norway, N-596 Oslo). Costs for equipment for home based video visits are acquired from the Norwegian partners of a European Union (EU) project a that analysed the effects of using video visits between home living patients with COPD and hospital nurses.
SHT incurs capital costs in the form of a standard package of devices specially constructed for elderly people that costs €1920 including installation. Assuming a duration of four years and a 4% annual discount rate, yields an equivalent annual cost b of €529. The home care provider only needs PCs and mobile phones to receive signals, and as this is standard equipment not especially acquired for operating the SHT, we did not include it in the analysis.
Video visits require equipment both at the home care provider and at the patient’s home. The price of television and video for private use is €2500, and assuming a four year duration and 4% annual discount rate, yields an equivalent annual cost of €688. The home care provider must invest in camera equipment in addition to television and video, and, altogether, this costs €7000. They must also provide training for home care employees in operating the equipment. We have assumed that each nurse performing video visits needed five hours of training. c The hourly labour costs for a nurse are €44, and an average municipal home care provider encompasses 25 nurses. Total investment costs to the health care provider for video visits are thus €12,500, which gives an equivalent annual cost of €3444 when the duration of the equipment is four years and the annual discount rate is 4%.
Operational and time costs
In an organised housing facility for the elderly in the municipality of Tromsø in Northern Norway, smart house devices are installed in each of the apartments and connected to the home care office. At the home care office, one nurse handles 20 apartments (patients) with SHT. Annual total labour costs for one nurse in the home care sector are €43,750, such that annual operational costs per patient equal €2187.
Previous studies indicate that video visits are shorter than physical visits, and estimates on the duration of a video visits are as low as 10 minutes. 21 We assumed that the duration of a video visit, including the setting up of the equipment at the home care providers and the eventuality of problems with handling the technology for the patient, is 1 h. For simplicity, we assumed that this is the same as the duration of a physical visit, excluding transportation time. We set the transportation time at 1 h. Additionally, there are operational costs, which we set at €6. Hence, total costs for one video visit equal the cost of one nurse for 1 h: €44. Transportation costs are involved in a physical visit, yielding a total cost of €94 d . This estimate is in line with the estimate Dansky et al reported in a study from the USA. 21
In the Kaiser-Permanente study, video visits were introduced in addition to physical visits, and the patients in the intervention group had, on average, 9.8 physical visits and 3.9 video visits. 20 This means that video visits constituted 40% of the physical visits. Data from Norwegian municipalities show that the average number of physical visits per week to a patient is about seven. e Based on these data, and taking the possibility that video visits may substitute physical visits into account, we assumed a weekly distribution of home care visits as shown in Table 1.
Allocation of physical visits and video visits per week divided on disability group, number of visits
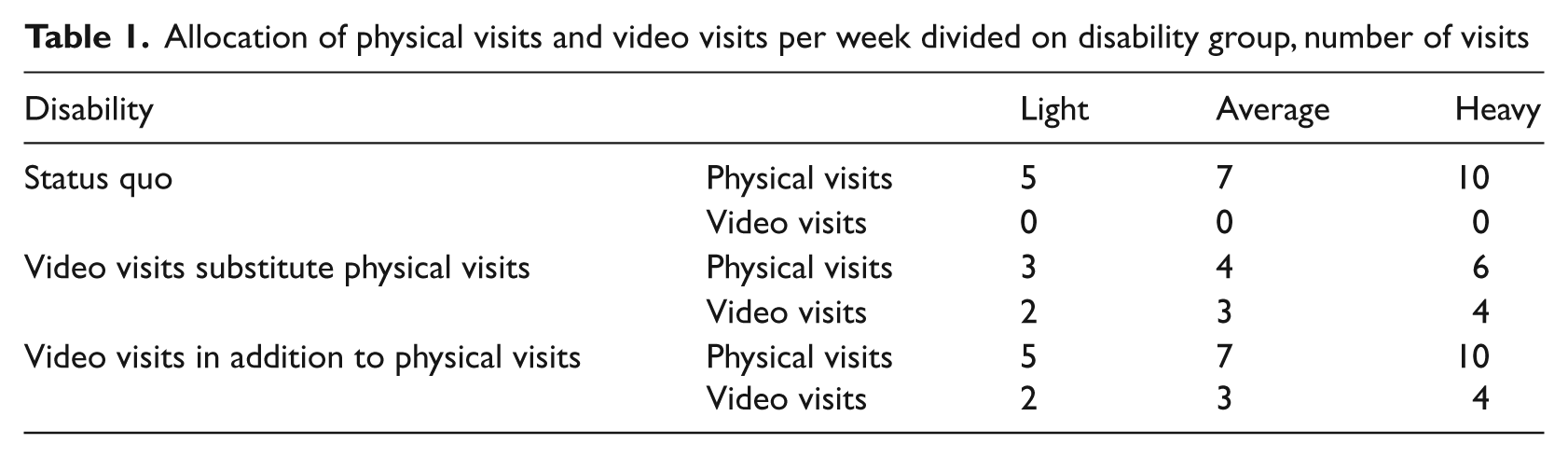
The cost savings of substituting physical visits with video visits consist of transportation costs, which we estimated above at €50 per visit. This is between the $100 (€75) estimate reported in Doolittle et al. 19 and the lowest estimate of $50 (€37.5) reported by Dansky et al. 21 When video visits substitute physical visits, the home care provider saves €100, 150 and 200 per week per lightly, averagely and heavily disabled patient, respectively. f When video visits come in addition to physical visits, this increases the health care provider’s costs by €88, 132 and 176 per week per lightly, averagely and heavily disabled patient, respectively.
Effects
Based on scores on 15 functions g every person needs in daily life, the patients in the Norwegian home care system are categorised as lightly, averagely or heavily disabled. 25 Lightly disabled patients may well live in their homes and have a low demand for care, whereas heavily disabled patients often live in nursing homes. Table 2 shows average annual gross wage (time) costs for a home care provider for providing the necessary care to one patient divided on functionality group, and the corresponding costs for a patient living in a nursing home. h
Annual average wage costs per patient for home care services divided on disability group. €

That technology may improve the functionality of frail elderly patients and patients with chronic diseases, is supported in a few evaluations.26–28 The challenge is to convert the qualitative statements on functionality improvements, which save (nursing) time, into monetary savings to the home care provider. As we have no experience data on how much SHT and video visits may reduce the need for home care, we turn the question around and ask: given the costs of implementing a specific technology in home care, how much must the (nursing) time costs of the home care provider be reduced in order to make the effort cost-effective? We calculated this as % of annual average wage costs per patient given in Table 2.
Relatives
Implementing SHT in home care patients’ homes may reduce the need for relatives’ care in the form of ‘checking that everything is all right’. On the other hand, if such technology enables elderly home care patients to live at home instead of in a nursing home, the need for care from relatives may increase. Similarly, when video visits come in addition to physical visits, this may reduce the need for relatives’ care, whereas when video visits substitute some of the physical visits, this may increase the need for relatives’ care, as the relatives then have to perform services the home care nurse would otherwise do during the physical visit. However, video visits also make the elderly more self sufficient and reduce the need for relatives’ care. For simplicity we assume that the two effects cancel each other out.
There are a few studies on care-giving efforts among the children of older, functionally-limited parents.29,30 They estimate that informal (family) care for elderly parents amounts to between 15 and 16.5 hours per week. We are not aware of any studies on how technology may substitute relatives’ care, and thus we assumed a uniform 10–15% decrease (two hours). However, when SHT is an alternative to the patient living in a nursing home, this will increase the need for relatives’ care. We assumed that the need for care increases with increasing disability and assumed an increase of two hours per week for a lightly disabled patient, five hours for an averagely disabled patient and eight hours for a heavily disabled patient.
We transformed the hours relatives spend assisting elderly family members into monetary units by using the average hour wage rate after tax, as recommended in the literature; 31 in Norway this amounted to €28 (2006). However, this assumes that the relatives’ alternative to visiting elderly family members is working. If they do it as part of their spare time, the relevant time costs for the relatives would be lower. Hence, our estimate on effects on relatives may be seen as an upper limit.
Hospitals and general practitioners (GPs)
A few studies report effects on hospitalisation costs of SHT and video visits.11,20,21 When substituting half of the home visits with video visits, this reduces hospitalisation costs during a treatment period of 60 days with US$866 (€650) per patient 21 , which is 62% of total hospitalisation costs without video visits. i Results from the Kaiser Permanente study 20 show that the hospitalisation costs were US$853 (€640), or 44%, lower per patient for the intervention group (video visits in addition to physical visits) compared to the control group (only physical visits) over an average treatment period of 53 days. For SHT there are reported effects on hospital admissions, discharges and length of stay in hospitals, but these effects have not been quantified.11,19
We have used the 10 most frequent diagnosis related groups (DRG) for persons above 60 years in Norway for all (three) types of hospital treatment j . Using the cost weights attached to each diagnosis, we calculate a weighted average cost for each type of hospital treatment, where the relative frequency of each DRG is used as weights. Finally, we took a weighted average of the costs of each hospital treatment to get an estimate of average annual hospital costs. We used data for 2010. Estimated hospital treatment costs per year for persons above 60 years in Norway were in 2010 €2446. The large reduction in hospitalisation costs reported in the studies above cannot be assumed to be representative for longer periods, e.g. one year, as they refer to a relatively short treatment period. Thus, we used a more conservative estimate on 10% reduction in hospitalisation costs. This implies a reduction in hospitalisation costs equal to €245 per patient per year. We used this estimate for both SHT and video visits.
Results from the Kaiser Permanente study indicated that outpatient costs for physician visits and costs for laboratory and pharmacy tests did not differ significantly between the control and the intervention group. 20 Hence, we did not include the effects of SHT and video visits on GPs and laboratories.
Results
Smart house technology (SHT)
Introducing SHT has an estimated cost equal to € 2,716 per patient per year. Possible effects, as presented above, have the potential to be far higher, as is shown in table 3.
Costs for introducing smart house technology (SHT) in the homes of elderly home care patients when the alternative is living at home without this technology, and possible quantified effects, € per patient per year
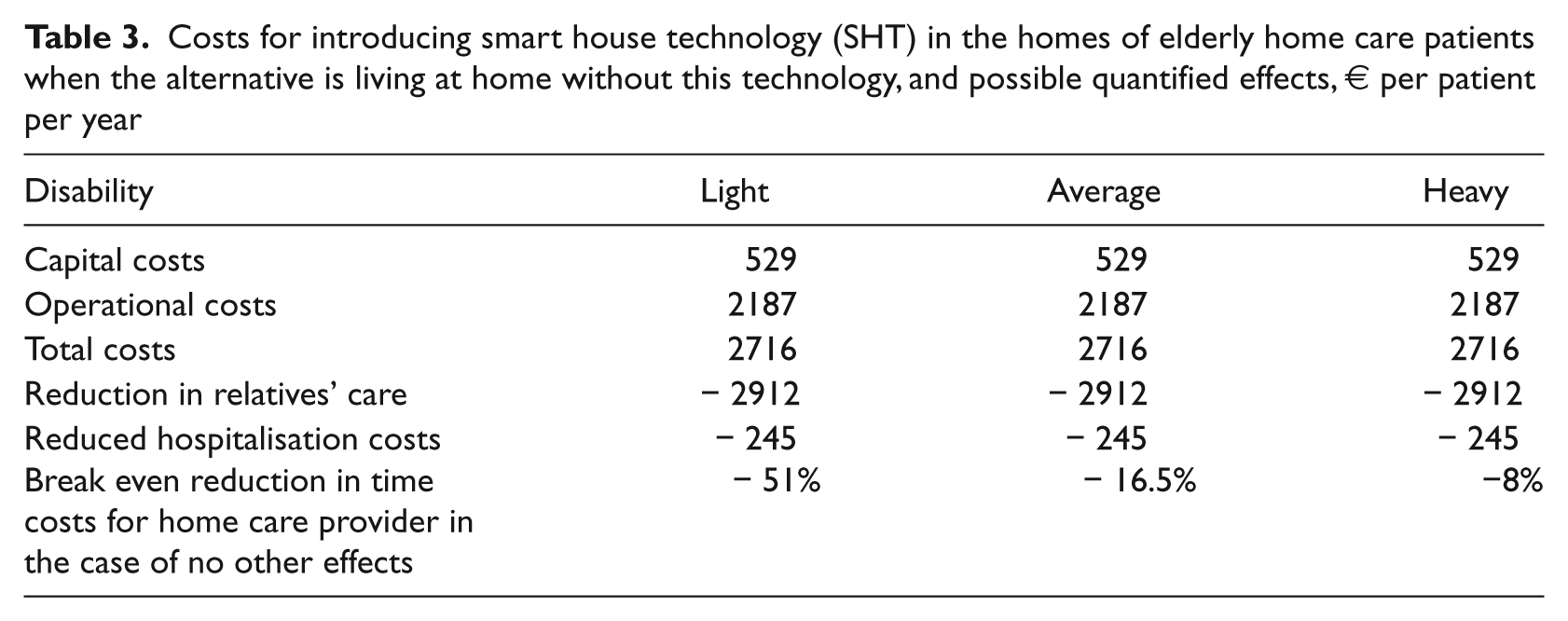
Table 3 shows that if we assume that equipping elderly home care patients living at home with SHT relieves their relatives of inspection time equal to two hours per week, and value these with the average wage rate, then this is a cost-effective effort, even without effects on hospitalisation costs and home care providers. If the alternative use of the inspection time for the relatives is spare time, it has to be valued by a lower hourly rate, and thus the effect would be lower. However, taking into account that SHT also reduces hospitalisation costs, the effort may still be cost-effective without effects on the home care provider.
Table 3 also shows the break even percentage reduction in time (wage) costs per patient per year for the home care provider when no other effects are taken into account. The actual time costs divided on functionality group are given in Table 2, and the numbers show how much the effort costs (€2716) constitute these costs. As the home care provider’s wage costs increase with the patient’s disability (see Table 2), the necessary per cent reduction decreases the more disabled a patient is. The annual (nursing) time costs for a lightly disabled patient are €5296, which is twice as much as annual costs of introducing SHT. Hence, the time costs for this group of patients must be reduced by about 50% in order for the effort to be cost-effective.
An alternative scenario implies letting a patient move out of a nursing home and into his/her own home and equipping his/her with SHT. As it is less likely that this is relevant for heavily disabled patients, we have not included effects for this group.
Table 4 shows that if SHT enables a home care patient to live in his/her own home instead of in a nursing home, there is a reduction in costs equal to the annual costs of keeping a patient at a nursing home, which is €75,134. However, we have to add the costs for the home care provider, relatives and hospitals but the cost savings for the nursing home are so high that not only do they cover increased costs for relatives and hospitals, in addition they may also cover the home care provider’s (nursing) time costs by several times.
Costs for introducing smart house technology (SHT) in the home of elderly home care patients when the alternative is living in a nursing home, and possible quantified effects, € per patient per year
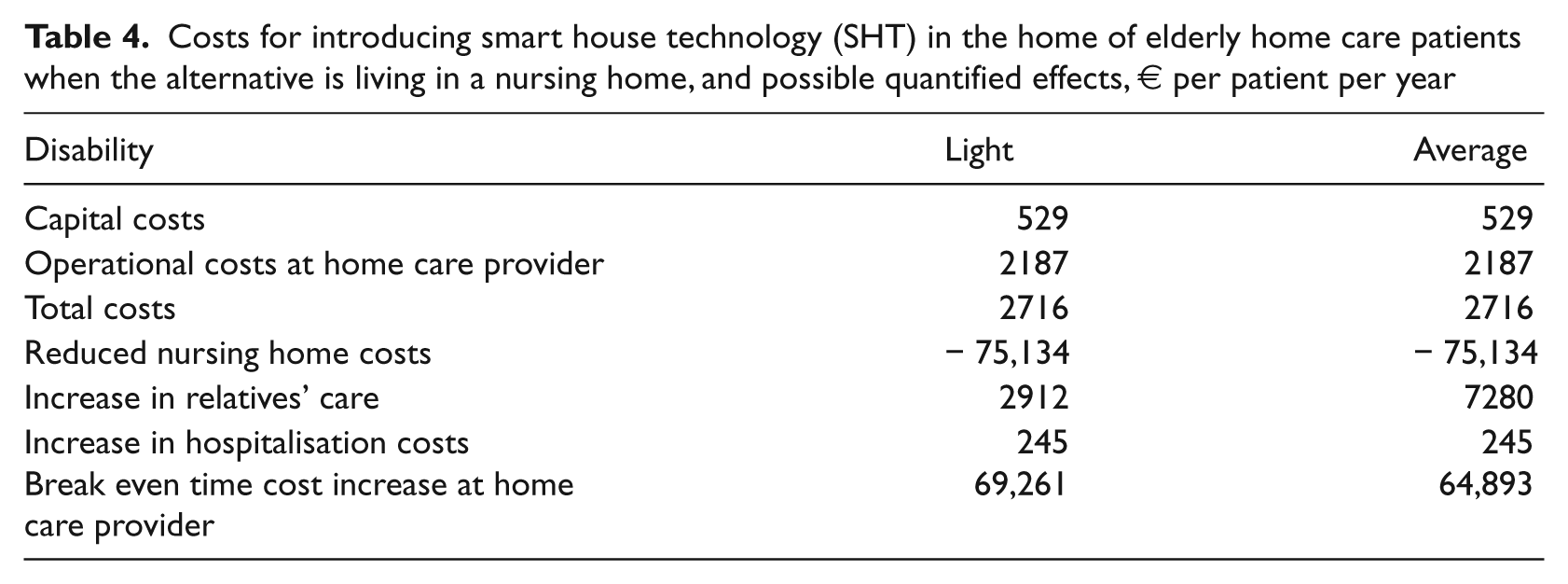
One may ask how likely it is that a lightly or averagely disabled patient lives in a nursing home? Although not typical, there are examples where home care nurses have more than an hour of transportation time to reach one single patient. 19 In these cases, where there is also a probability that the patient cannot be reached because of bad weather, it may be preferable to move the patient to a nursing home. Then, SHT may be a good alternative to letting the patient move to a nursing home, at least a very cost-effective one.
Video visits
The costs of introducing video visits depend on whether they come in addition to or substitute physical visits. When they substitute physical visits, the operational costs decrease, whereas when they come in addition, operational costs increase. Previous studies indicate that video visits not only reduce the costs for the home care provider, but also affect hospitalisation costs and the demand for relatives’ care.11,20,21
Table 5 shows that when video visits substitute some physical visits the effect on hospitalisation costs is far from large enough to offset the effort costs. Constituting less than 10% of net effort costs, it is necessary that the home care providers realise time cost reductions in order for the effort to be cost-effective. k The time cost savings at the home care provider must be 76% for lightly disabled patients, 24% for averagely disabled patients and 11% for heavily disabled patients for the effort to break even when assuming no other effects (Table 5). Taking into consideration the reduction in hospitalisation costs, the break even cost savings for the home care provider are 71%, 22% and 10%, respectively, for lightly, averagely and heavily disabled patients.
Costs for introducing video visits when they substitute some of the physical visits, and possible quantified effects, EUR per patient per year
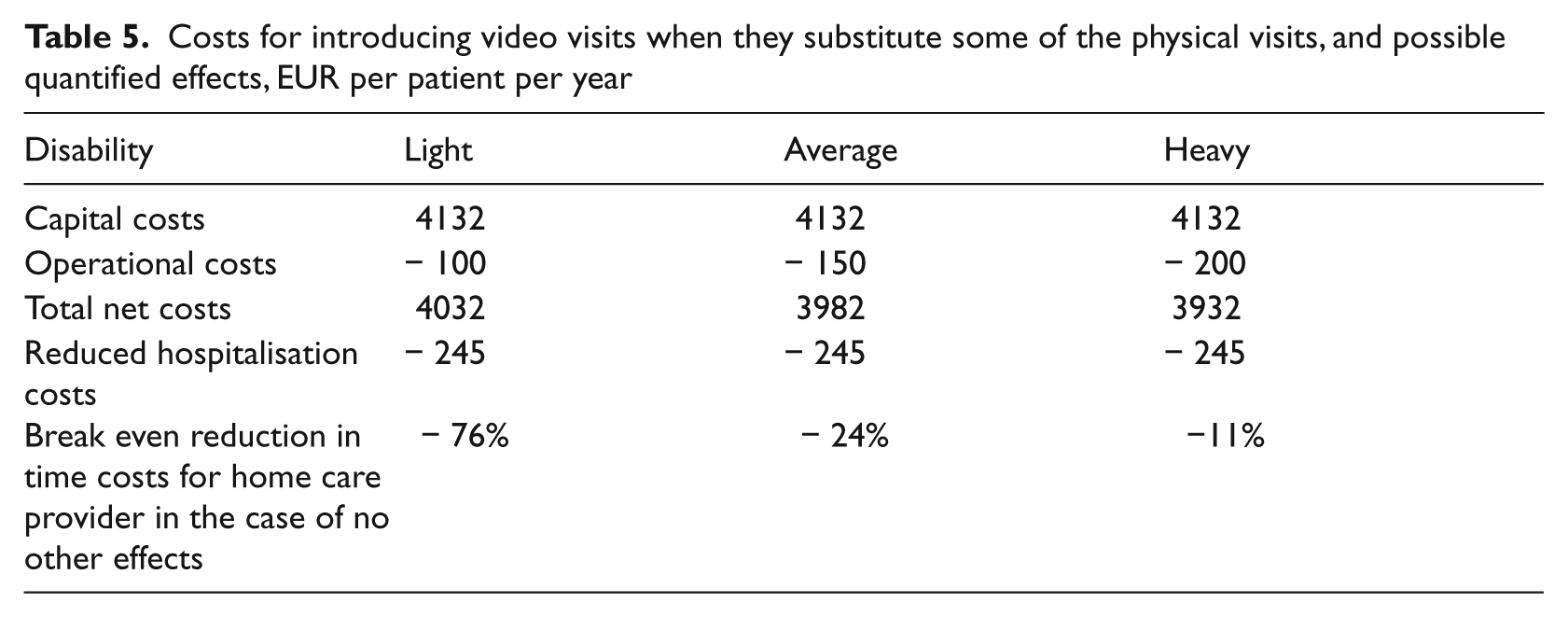
This result rests on the assumption that half of the physical visits to lightly and averagely disabled patients, and 40% of the visits to heavily disabled patients, can be substituted by video visits. This may be realistic for the two former groups of patients, but may be questionable for the last group. Reducing the number of physical visits that can be substituted by video visits reduces the savings in operational costs and thus increases the effort costs net of operational costs at the home care provider. In turn, the necessary reduction in (nursing) time cost savings at the home care provider must be higher.
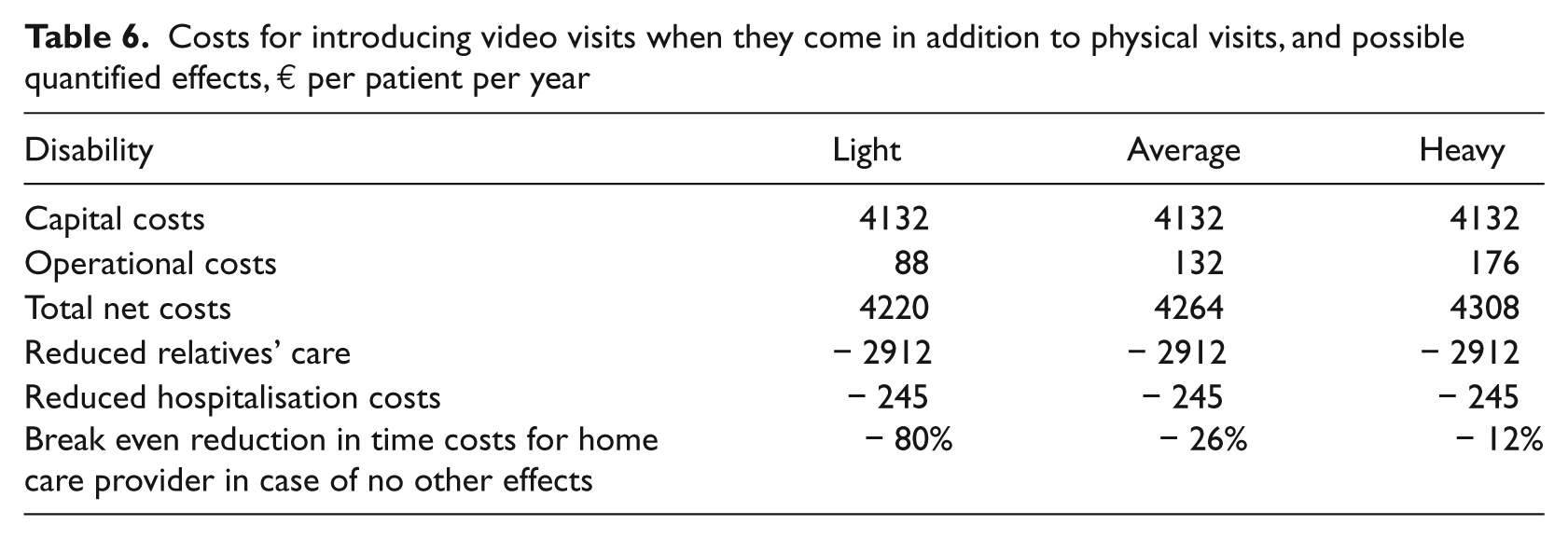
When video visits are in addition to physical visits, the costs of the effort increase compared to when they substitute some physical visits. Table 6 shows that reduced inspection time for relatives and reduced hospitalisation costs are not sufficient to make the use of video visits in home care cost-effective. When taking into account the effects on relatives and hospitals, the home care provider’s time costs must be reduced by at least 20% for a lightly disabled patient in order to make the effort cost-effective. The corresponding numbers for averagely and heavily disabled patients are 6.5% and 3%, respectively. If we assume no effects on relatives and hospitals, the home care providers’ costs must be reduced by 80%, 26%, and 12% for lightly, averagely and heavily disabled patients, respectively, in order to make the effort cost-effective (Table 6).
Costs for introducing video visits when they come in addition to physical visits, and possible quantified effects, € per patient per year
Discussion and conclusions
In this article, we have documented costs for two ICT efforts in home care (SHT and video visits) and asked whether the effects that can be expected are sufficient to make the efforts cost-effective for society. We show that SHT, which has very low costs, may be cost-effective, even if we only assume effects on relatives. No reduction in (nursing) time costs to home care providers and to hospitals is needed. For video visits, which imply far higher costs, we show that significant reductions in the time costs for home care providers are needed to defend the effort costs. This is true independently of whether video visits substitute physical visits or are in addition. However, when they are in addition, and we can expect a reduction in the need for relatives’ care, this substantially reduces the demand for time cost reductions at the home care provider.
This is a quantitative analysis encompassing only the most obvious and easily measurable effects. We have identified groups that would obviously benefit from the efforts discussed in this article, but owing to lack of data and measurement methods, we have not quantified these effects. Also, each of the identified groups may have positive and negative effects of a more qualitative character that we have not taken into account. Hence, it is important to bear in mind that the results from this analysis cannot stand alone in guiding policy decisions with respect to the use of SHT and video visits in home care. We have only substantiated the likelihood of ICT efforts, such as SHT and video visits in home care to be cost-effective. Other professions: health care workers, technologists, and people who will consider the ethical sides of technology, must give their input to the discussion before good decisions on this matter can be made.
Footnotes
Acknowledgements
This work was funded by The Norwegian Association of Local and Regional Authorities (KS). It was carried out in parallel with a project aiming to discuss new and existing technologies relevant for use by home care providers in Norway. We would like to thank Rune Devold, from Rune Devold Ltd. for making available data on home care wage (time) costs for patients with different degrees of disabilities. Many of the results in this paper rest on his data. We would also like to thank Elin Breivik, Norwegian Centre for Telemedicine, for invaluable assistance in the literature search. All results, viewpoints, and arguments in the article are the responsibility of the authors.