
Abstract
Background
Damage control surgery (DCS) is a life-saving strategy for critically injured patients in extremis. Identifying predictors of mortality in this population may help guide clinical decision making and resource allocation in low- and middle-income countries. This study aimed to identify independent predictors of in-hospital mortality following DCS.
Methods
We conducted a retrospective analysis of 219 consecutive patients who underwent DCS at a trauma centre, over 3 years, between June 2021 and June 2024. Patient demographics, physiological parameters, laboratory values, transfusion requirements, operative details and outcomes were compared between survivors and non-survivors. Multivariable logistic regression analysis was performed to identify independent predictors of mortality.
Results
The overall in-hospital mortality rate was 11.0% (n = 24). Patients were predominantly male (93.5%) with penetrating trauma (84.5%). Non-survivors demonstrated significantly lower Glasgow Coma Scale scores (13.0 vs. 15.0, p < 0.001), lower arterial pH (7.07 vs. 7.29, p < 0.001), higher lactate levels (13.4 vs. 6.3 mmol/L, p < 0.001) and greater transfusion requirements (p < 0.001). Multivariable analysis identified three independent predictors of mortality: elevated lactate (OR 4.33 per SD increase), lower Glasgow Coma Scale (OR 0.56 per SD increase) and lower arterial pH (OR 1.34 per SD decrease). The predictive model demonstrated excellent discrimination (AUC 0.912).
Conclusions
Lactate, Glasgow Coma Scale and arterial pH are independent predictors of mortality following DCS. These readily available clinical parameters may assist in prognostication and guide resuscitation efforts in this high-risk patient population.
Introduction
Damage control surgery (DCS) marks a significant shift in managing critically injured patients, focusing on physiological stabilisation rather than anatomical repair.1–3 First introduced by Stone and colleagues in 1983 and later formalised by Rotondo and Schwab in 1993, this phased approach has become the standard care for patients exhibiting the ‘lethal triad’ of hypothermia, acidosis and coagulopathy.4–6 Recognising that extended surgery in physiologically unstable patients causes irreversible metabolic exhaustion has fundamentally altered surgical decision-making in trauma.
The fundamental principle of DCS involves a shortened initial surgery focused on controlling haemorrhage and limiting contamination, followed by intensive care unit (ICU) resuscitation to correct physiological imbalances, and then definitive repair once the patient has been stabilised.7–9 This three-phase approach, initial abbreviated surgery, ICU resuscitation and planned reoperation, has clearly improved survival rates in patients who would otherwise have succumbed to the irreversible physiological effects of prolonged surgery.10–12 The operative phase emphasises quick control of haemorrhage through packing, shunting and vessel ligation, with gastrointestinal contamination managed by stapling or resection without anastomosis.
Despite widespread adoption of damage control principles across trauma centres worldwide, mortality rates following DCS remain significant, ranging from 10% to 50% depending on patient population and injury severity.13–15 This variation reflects differences in case selection, injury patterns and available resources. The ability to identify patients at the highest risk of death is essential for several reasons: it facilitates informed discussions with families during the critical early hours following injury, guides resource allocation in settings with limited critical care capacity and may help identify therapeutic targets for intervention.16–18
Previous studies have identified various predictors of mortality following DCS, including injury severity scores, transfusion requirements, degrees of acidosis, core temperature and the presence of coagulopathy.19–22 However, many of these studies were conducted at single institutions with heterogeneous patient populations, and the relative importance of individual predictors remains controversial. Furthermore, the optimal combination of readily available clinical parameters for prognostication has not been well established, limiting the practical utility of existing prediction models.
Lactate, as a marker of tissue hypoperfusion and anaerobic metabolism, has become a particularly important prognostic indicator in trauma patients.23–25 Elevated lactate indicates inadequate oxygen delivery at the tissue level and the resulting shift to anaerobic glycolysis. Similarly, the Glasgow Coma Scale (GCS), originally developed for traumatic brain injury assessment, has been shown to correlate with outcomes across a broad range of critical illnesses, acting as a surrogate marker of overall physiological impairment.26–28 The interaction between these parameters and their relative roles in predicting mortality in the DCS population warrants further exploration.
The primary aim of this study was to identify independent predictors of in-hospital mortality in patients undergoing DCS at a high-volume urban trauma centre. Secondary aims included characterising differences in clinical presentation, physiological parameters and resource use between survivors and non-survivors. We hypothesised that markers of metabolic disturbance, especially lactate and pH, would be significant predictors of mortality in this patient group.
Methods
Study design and setting
This retrospective cohort study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting observational studies. The study was conducted at an urban trauma centre that serves as a regional referral centre for major trauma. The study protocol was approved by the Human Research Ethics Committee (Reference Number: M250705, approved 25/07/2025) and was conducted in accordance with the Declaration of Helsinki as revised in 2024. The requirement for informed consent was waived, given the analysis's retrospective nature and the use of de-identified data. All patients who underwent DCS between June 2021 and June 2024 were identified from the institutional trauma registry and operating room records.
Patient selection
All adult trauma patients aged ≥18 years who underwent DCS, defined as abbreviated laparotomy with planned temporary abdominal closure and an intention for a subsequent relook procedure, were included in the study. Exclusion criteria included isolated thoracic or vascular damage control procedures without abdominal involvement, patients transferred from other facilities after initial DCS, and those with incomplete medical records precluding outcome determination. Patients who died intraoperatively during the initial damage control procedure were included in the analysis.
Data collection
Data were extracted from the Medibank form, patient files and the REDCap database of electronic medical records by trained research personnel using a standardised case report form. Variables collected included patient demographics (age, sex), injury characteristics (mechanism, time of presentation), initial physiological parameters (heart rate, blood pressure, Glasgow Coma Scale), Injury severity score (ISS), laboratory values on presentation (arterial blood gas including pH and lactate, complete blood count, basic metabolic panel), transfusion requirements (pre-operative and intraoperative red blood cells and fresh frozen plasma), operative details (procedure duration, organs injured, haemostatic techniques employed) and postoperative course (ICU admission, relook laparotomy, in-hospital mortality).
The shock index was calculated as heart rate divided by systolic blood pressure. Penetrating injuries comprised gunshot and stab wounds, whereas blunt injuries comprised motor vehicle collisions, falls and assaults. Night-time presentation was defined as arrival between 18:00 and 06:00 h. The primary outcome was in-hospital mortality, defined as death during the index hospitalisation, regardless of cause.
Statistical analysis
Continuous variables were assessed for normality using the Shapiro-Wilk test and visual inspection of histograms. Given the non-normal distribution of most variables, continuous data are presented as medians with interquartile ranges (IQRs) and compared using the Mann-Whitney U test. Categorical variables are presented as frequencies and percentages and compared using the chi-square test or Fisher's exact test as appropriate.
Multivariable logistic regression analysis was performed to identify independent predictors of in-hospital mortality. Variables with p < 0.10 on univariable analysis were considered for inclusion in the multivariable model. Continuous variables were standardised (mean = 0, SD = 1) to allow comparison of effect sizes across variables with different units. The final model was constructed using backward stepwise elimination with a retention threshold of p < 0.05. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC). Model calibration was evaluated using the Hosmer-Lemeshow goodness-of-fit test.
Results are reported as odds ratios (OR) with 95% confidence intervals (CI). All statistical tests were two-tailed, and p < 0.05 was considered statistically significant. Statistical analyses were performed using STATA version 16.0.
Results
Patient demographics and baseline characteristics
During the study period, 219 patients underwent DCS and met the inclusion criteria. The overall in-hospital mortality rate was 11.0% (n = 24). The median age was 33.5 years (IQR 27.5–41.0), with no significant difference between survivors and non-survivors (34.0 [27.0–41.0] vs. 33.0 [29.5–40.5] years, p = 0.890). Most patients were male (93.5%, n = 201), and this proportion did not differ significantly between groups (93.7% vs. 91.7%, p = 0.660).
Penetrating trauma was the predominant mechanism of injury, accounting for 84.5% (n = 185) of cases, with similar rates observed in both survivors and non-survivors (86.2% vs. 91.7%, p = 0.749). Most injuries occurred at night (71.4%, n = 125), with no significant difference between outcome groups (70.8% vs. 76.2%, p = 0.797). Detailed mechanism-of-injury breakdown was as follows: Gunshot 164 (74.9%); MVC 10 (4.6%); Assault 4 (1.8%); Mixed mechanism 3 (1.4%); PVC 17 (7.8%); Stab 21 (9.6%).
Initial clinical presentation and physiological parameters
On presentation, patients demonstrated significant physiological derangement (Table 1) with elevated heart rate and decreased systolic blood pressure although there was no difference between groups.
Clinical presentation and laboratory values at admission.
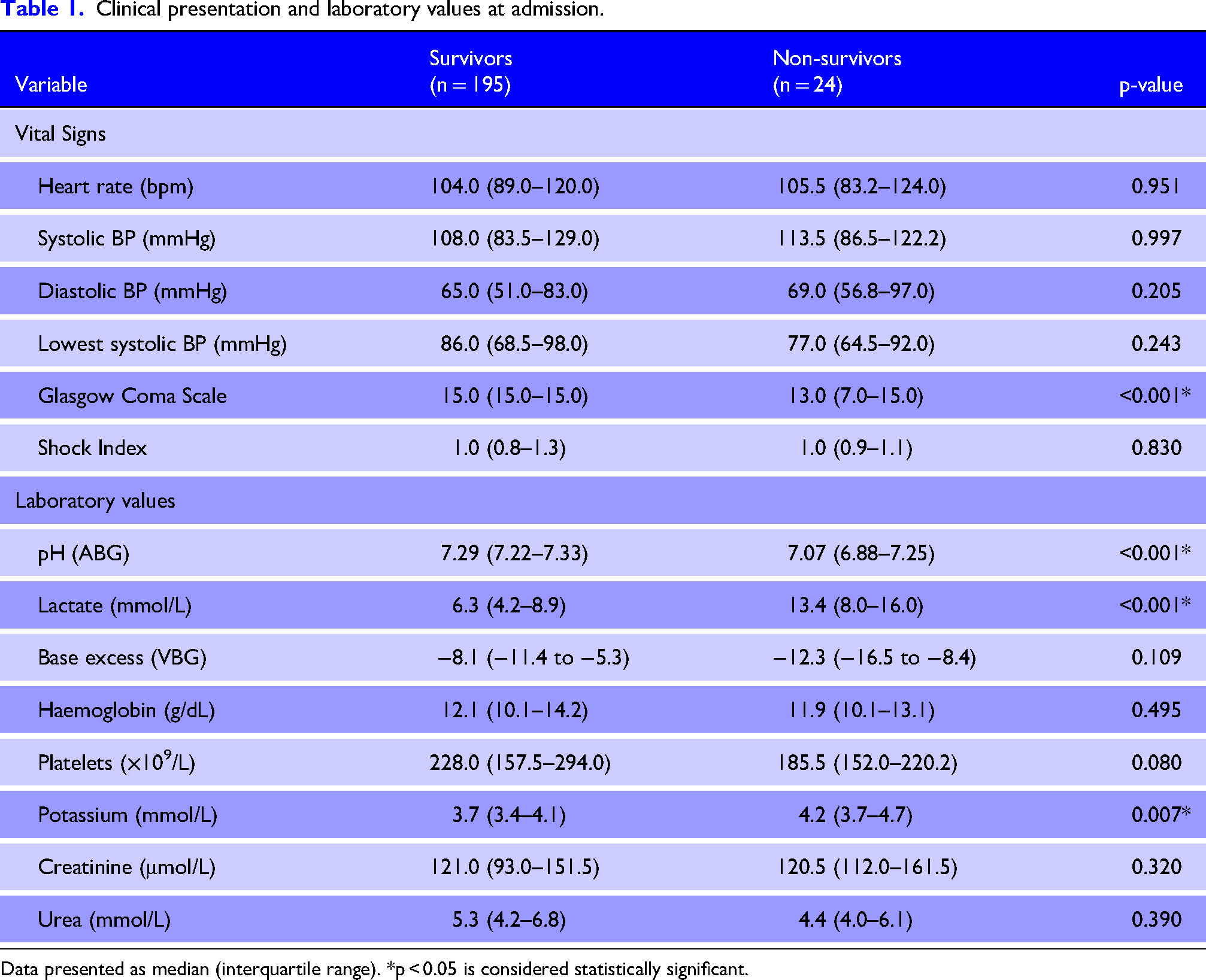
Data presented as median (interquartile range). *p < 0.05 is considered statistically significant.
The Glasgow Coma Scale (GCS) score was significantly lower in non-survivors compared to survivors (13.0 [7.0–15.0] vs. 15.0 [15.0–15.0], p < 0.001), indicating more severe physiological derangement in patients who died (Figure 1). The median shock index was 1.0 (IQR 0.8–1.3) for the entire cohort, with no significant difference between outcome groups (p = 0.830).
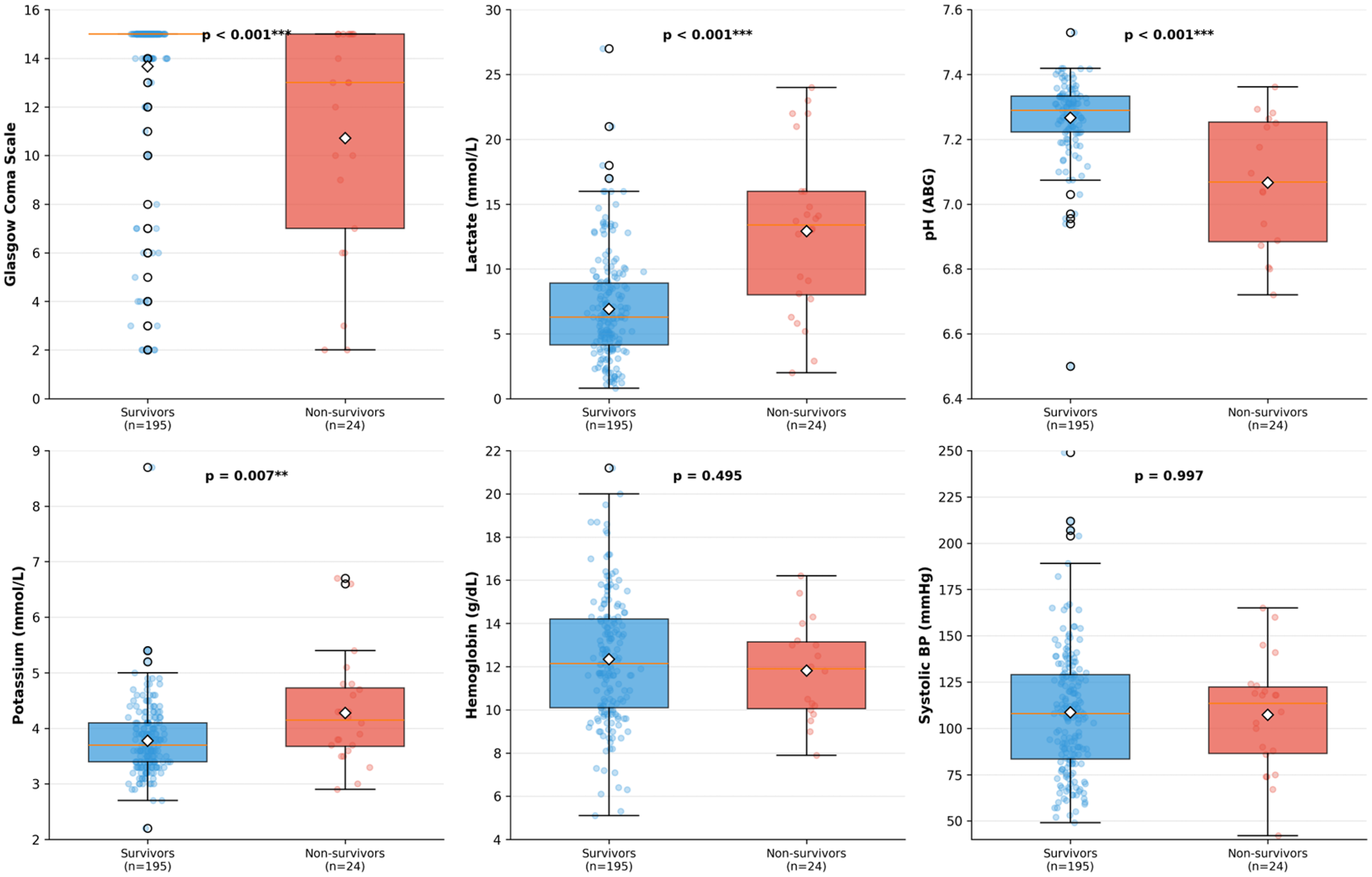
Comparison of physiological variables between survivors and non-survivors. Box plots comparing Glasgow Coma Scale, arterial pH and lactate levels between survivors (blue) and non-survivors (red). Horizontal lines represent median values, and boxes represent interquartile ranges. ***p < 0.001.
Arterial blood gas analysis revealed profound acidosis in non-survivors and significantly elevated lactate indicative of severe tissue hypoperfusion and metabolic derangement (Figure 1). Serum potassium was significantly higher in non-survivors (4.2 [3.7–4.7] mmol/L) compared to survivors (3.7 [3.4–4.1] mmol/L, p = 0.007), likely reflecting cellular injury and metabolic acidosis. Other laboratory parameters, including haemoglobin, platelet count, white cell count, creatinine and urea, showed no significant differences between groups (Table 1).
Intraoperative management and transfusion requirements
Transfusion requirements differed significantly between survivors and non-survivors (Figure 2). Pre-operative red blood cell (RBC) transfusion was significantly higher in non-survivors, with a median of 2 units (IQR 1.0–2.8) compared to 1 unit (IQR 1.0–2.0) in survivors (p = 0.002). This difference became more pronounced intraoperatively, with non-survivors requiring a median of 4.5 units (IQR 4.0–6.8) of RBCs compared to 4.0 units (IQR 2.0–4.0) in survivors (p < 0.001).
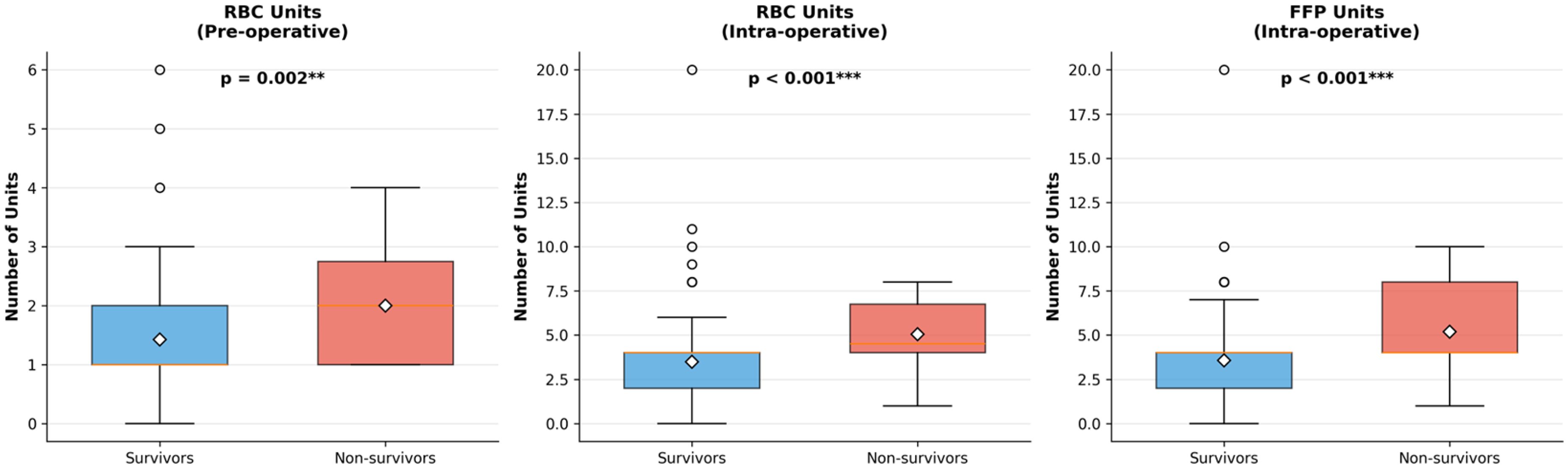
Transfusion requirements in survivors versus non-survivors. Box plots comparing pre-operative RBC, intraoperative RBC and intraoperative FFP transfusion between survivors and non-survivors. **p < 0.01, ***p < 0.001.
Fresh frozen plasma (FFP) transfusion during surgery also differed significantly, with non-survivors receiving a median of 4 units (IQR 4.0–8.0) compared to 4 units (IQR 2.0–4.0) in survivors (p < 0.001). The median operative time was 85 min (IQR 60–120), with no significant difference between groups (p = 0.885).
Inotropic support was required significantly more frequently in non-survivors (91.7%) compared to survivors (50.9%, p = 0.010), reflecting more profound cardiovascular compromise (Figure 3).
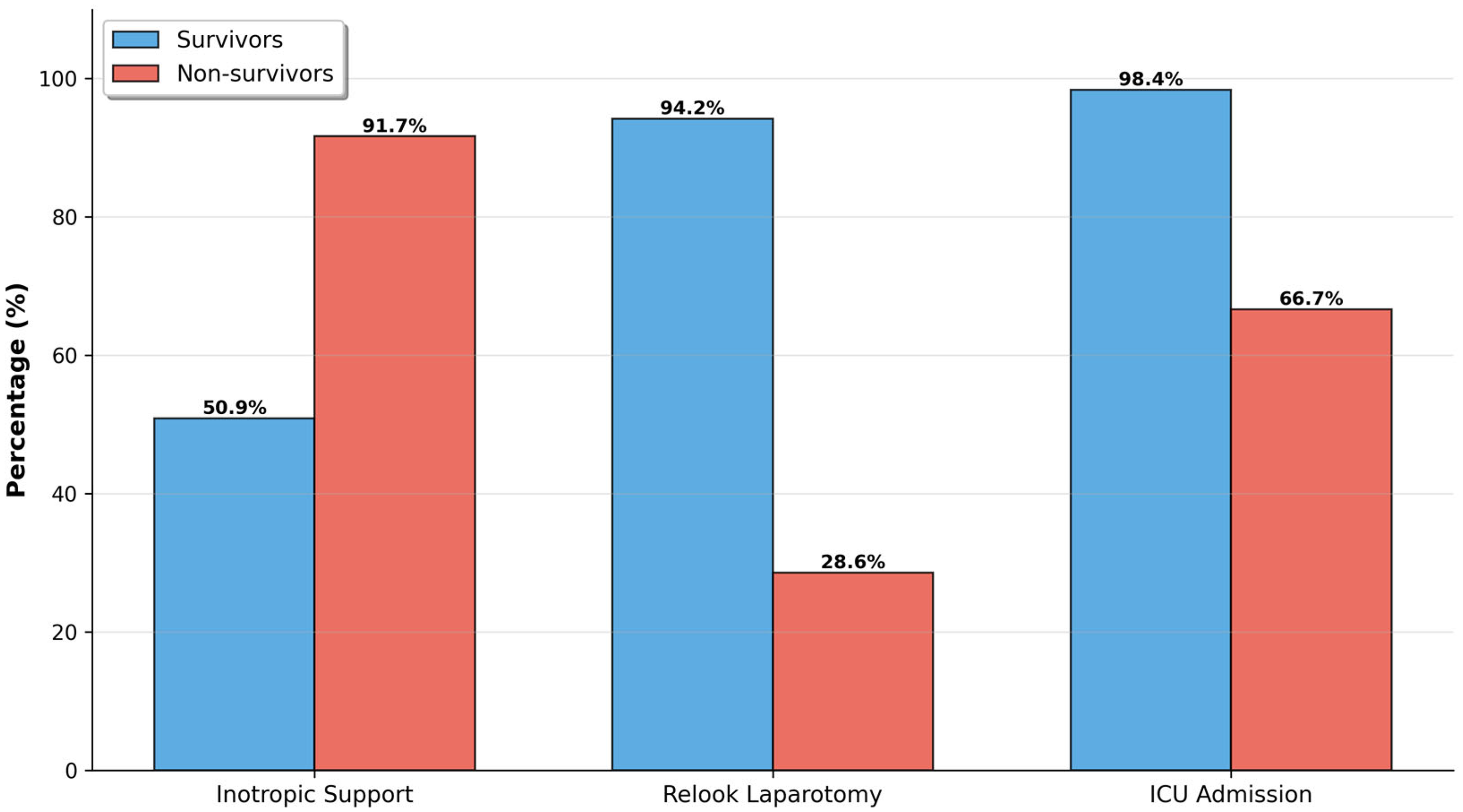
Categorical outcomes: inotropic support, relook laparotomy and ICU admission. Bar charts comparing rates of inotropic support, relook laparotomy and ICU admission between survivors and non-survivors. *p < 0.05, **p < 0.01, ***p < 0.001.
Organ injuries and postoperative outcomes
The pattern of organ injuries is detailed in Table 2. Liver injury was the most common solid organ injury, present in 36.4% of survivors and 54.2% of non-survivors, though this difference did not reach statistical significance (p = 0.119). Pancreatic injury was significantly less common in non-survivors (0% vs. 16.0%, p = 0.015), likely due to the small sample size in this subgroup. The distribution of injuries according to composite anatomical region was: head 4 (1.8%); neck 1 (0.5%); chest 36 (16.4%); abdomen 218 (99.5%); pelvis 3 (1.4%) and extremities/musculoskeletal 30 (13.7%). The injury severity score (ISS) was higher in non-survivors than in survivors: 25.0 (16.0–26.0) versus 16.0 (13.0–25.0), p = 0.122.
Anatomic distribution of organ injuries.
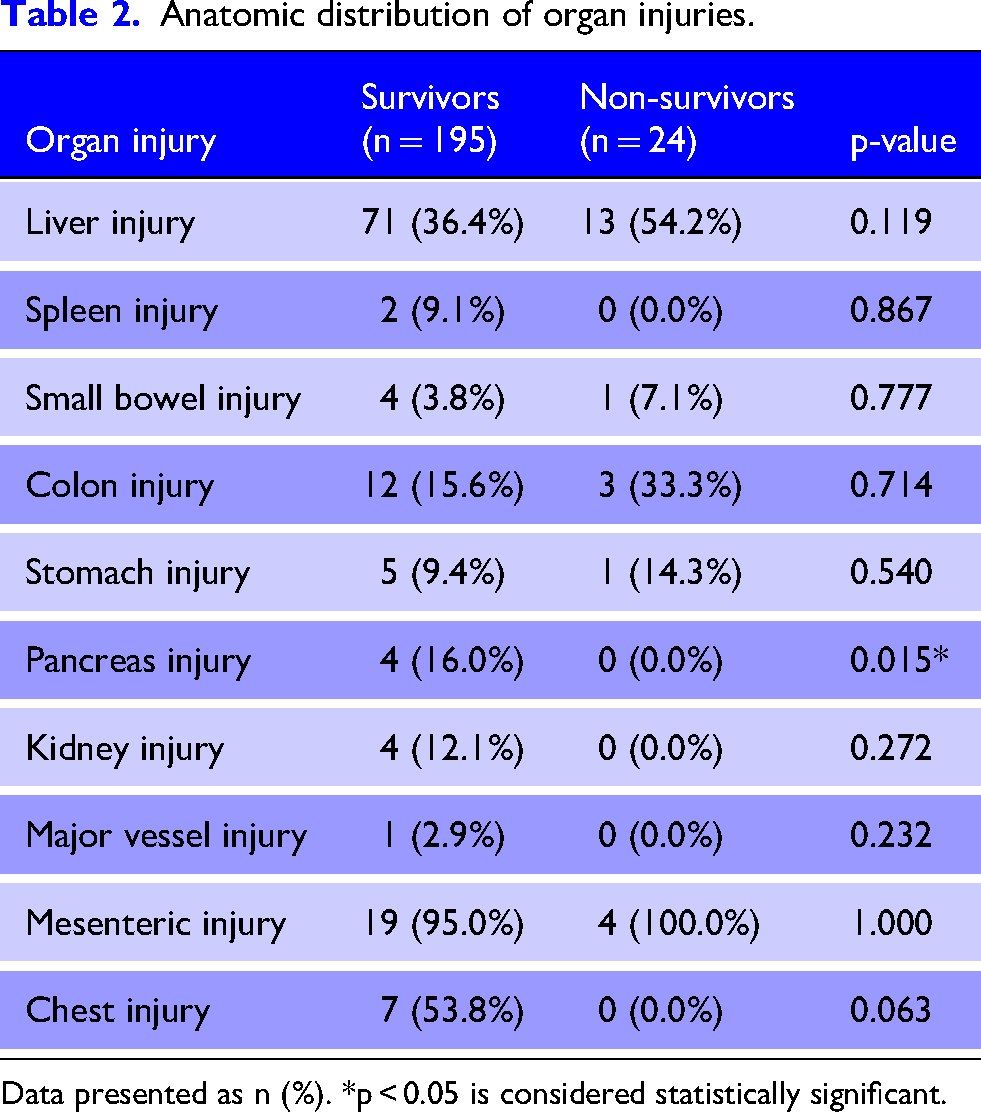
Data presented as n (%). *p < 0.05 is considered statistically significant.
Most survivors were admitted to the intensive care unit (98.4%) compared to 66.7% of non-survivors (p = 0.008), with the lower rate in non-survivors likely reflecting early mortality. Relook laparotomy was performed in 90.6% of the cohort, with survivors significantly more likely to undergo relook (94.2% vs. 28.6%, p < 0.001), suggesting that non-survivors succumbed before planned reoperation could occur. Additional procedures performed included 17 thoracotomies (7.8%), six sternotomies (2.7%) and 10 Emergency Room thoracotomies (4.6%); no burr holes or vascular embolisations were performed.
Independent predictors of mortality
Multivariable logistic regression analysis identified three independent predictors of in-hospital mortality (Table 3, Figure 4). The final model demonstrated excellent discriminatory ability with an area under the curve (AUC) of 0.912.
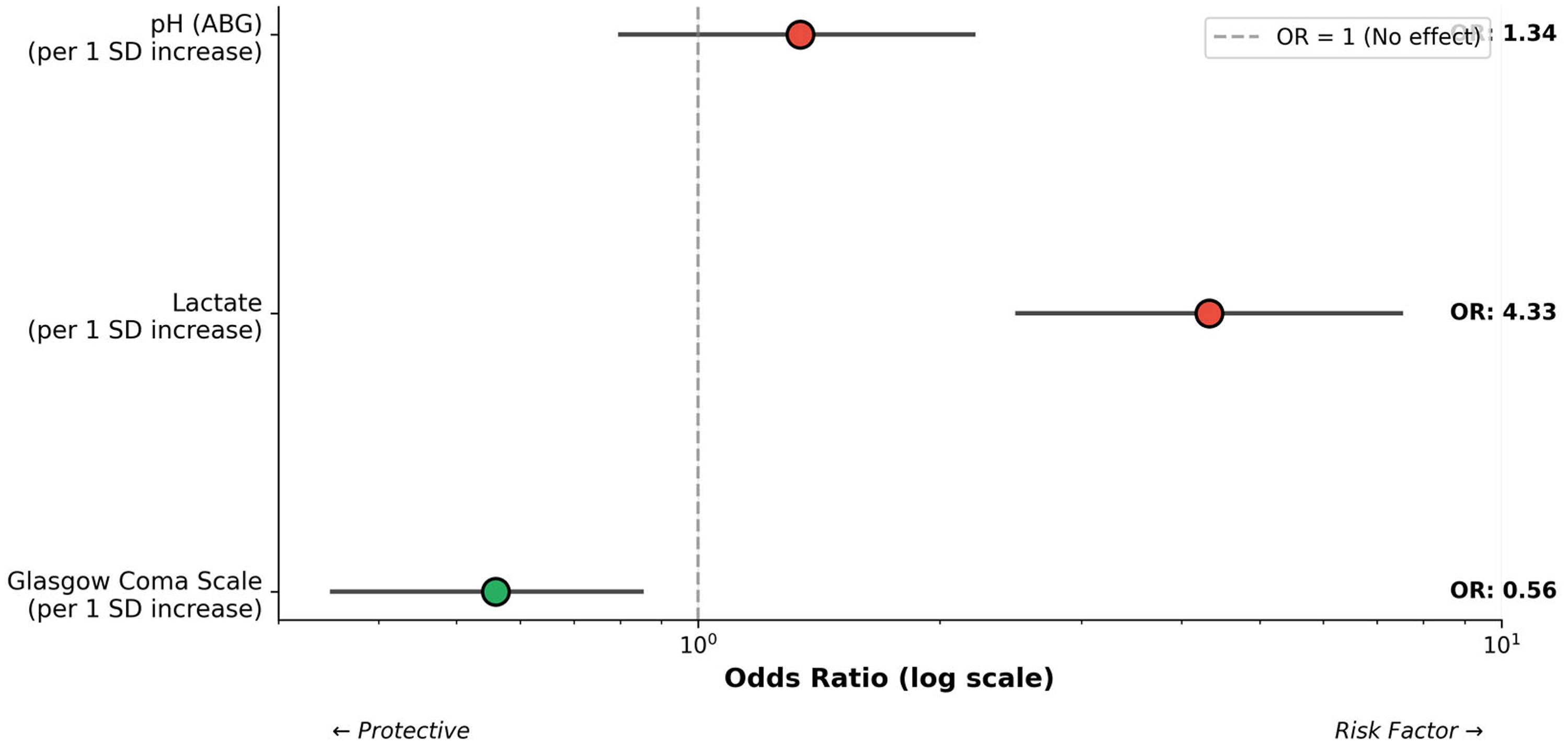
Forest plot of independent mortality predictors. Forest plot displaying odds ratios with 95% confidence intervals for independent predictors of mortality from multivariable logistic regression analysis. Odds ratios are expressed per standard deviation change in the predictor variable. AUC = 0.912.
Multivariable logistic regression analysis: independent predictors of in-hospital mortality.
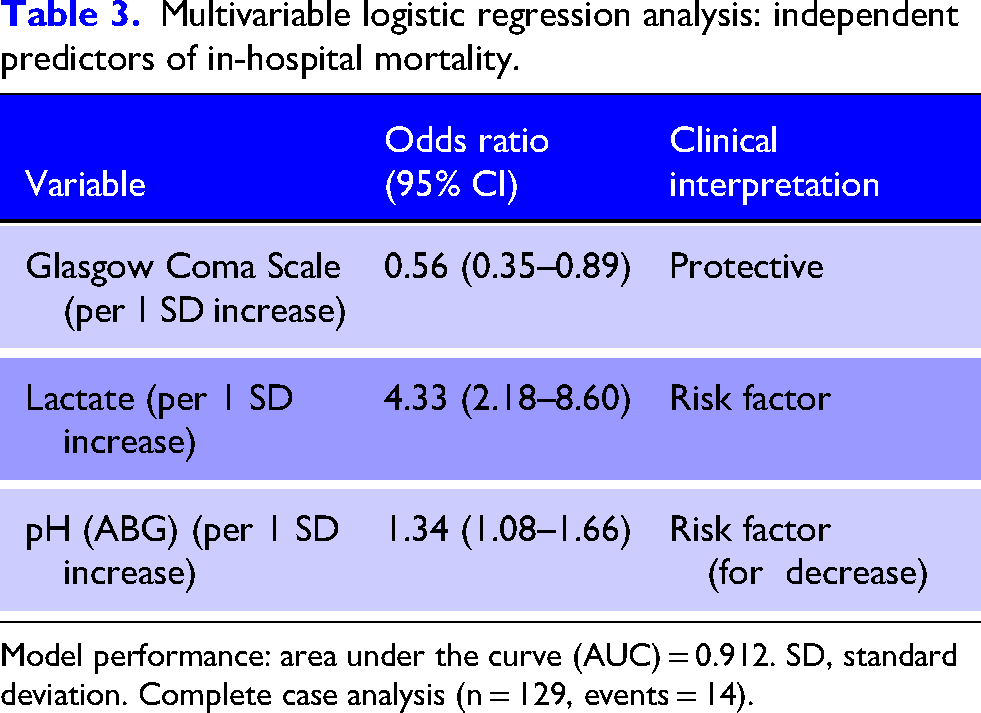
Model performance: area under the curve (AUC) = 0.912. SD, standard deviation. Complete case analysis (n = 129, events = 14).
In the multivariable model, elevated lactate emerged as the strongest independent predictor of death (OR 4.33 per standard deviation increase, 95% CI 2.18–8.60, p < 0.001). Higher Glasgow Coma Scale scores were independently protective against mortality (OR 0.56 per SD increase, 95% CI 0.35–0.89, p = 0.014), while lower arterial pH was associated with increased mortality risk (OR 1.34 per SD decrease, 95% CI 1.08–1.66, p = 0.008).
These findings highlight the critical importance of severe metabolic derangement, particularly lactic acidosis and impaired consciousness, as key determinants of survival following DCS.
Discussion
This retrospective analysis of 219 patients undergoing DCS identified lactate, Glasgow Coma Scale and arterial pH as independent predictors of in-hospital mortality. Our observed mortality rate of 11.0% aligns with contemporary series reporting outcomes following DCS in high-volume trauma centres, which typically range from 10% to 25%.13–15 The predictive model incorporating these three variables demonstrated excellent discrimination (AUC 0.912), indicating potential clinical utility for risk stratification in this high-acuity population.
The identification of lactate as the strongest predictor of mortality (OR 4.33 per SD increase) aligns with the fundamental pathophysiology of traumatic haemorrhagic shock. Lactate elevation indicates inadequate tissue oxygen delivery and the resultant shift to anaerobic metabolism.23–25 Our finding that non-survivors had markedly elevated lactate levels (13.4 vs. 6.3 mmol/L) emphasises the severity of physiological insult in this population. The extent of lactate elevation in non-survivors is more than double that of survivors, highlighting the profound metabolic derangement present at the time of surgical intervention. Previous studies have similarly identified lactate as a powerful prognostic marker in trauma, with serial lactate measurements and lactate clearance providing additional prognostic information.29–31 Notably, failure to clear lactate within 24 h has been associated with significantly increased mortality rates. 31
Higher GCS scores demonstrated a significant protective effect (OR 0.56 per SD increase), with survivors presenting with better mental status than non-survivors (median GCS 15.0 vs. 13.0, p < 0.001). While altered consciousness in trauma is traditionally attributed to traumatic brain injury, in haemorrhagic shock it predominantly reflects cerebral hypoperfusion and systemic physiological compromise.26–28 Patients maintaining preserved consciousness likely harbour less severe injury burden and greater physiological reserve to withstand operative stress and subsequent resuscitation. Notably, even modest GCS decrements were associated with substantially worse outcomes, reinforcing the prognostic value of this readily available assessment across the full consciousness spectrum – not merely in comatose patients.
In our predominantly penetrating-trauma cohort, low GCS among non-survivors was a marker of global physiological derangement rather than an isolated traumatic brain injury. This interpretation is supported by converging evidence: (1) the complete absence of neurosurgical intervention (burr holes 0 [0.0%]), indicating no significant intracranial mass lesions; (2) an inverse correlation between GCS and serum lactate (Spearman ρ = −0.309, p < 0.001); and (3) a strong positive correlation between GCS and arterial pH (Spearman ρ = 0.492, p < 0.001). These physiological associations indicate that impaired mentation primarily reflected shock severity and metabolic acidosis rather than structural brain injury. In low- and middle-income countries (LMIC) settings where penetrating trauma predominates and access to advanced neuroimaging is limited, admission GCS functions as an integrated whole-body severity indicator, capturing both neurological status and the cumulative physiological impact of haemorrhagic shock.
The link between arterial pH and mortality underscores the clinical importance of metabolic acidosis in this population. The severe acidaemia observed in non-survivors (pH 7.07 vs. 7.29) reflects a combination of acidosis from tissue hypoperfusion, dilutional acidosis from resuscitation fluids, and consumption of bicarbonate buffer.32–34 This degree of acidosis has direct adverse physiological effects that create a cycle of worsening deterioration. Severe acidosis causes myocardial depression with reduced contractility and cardiac output, worsens coagulopathy by impairing clotting factor function and induces vasoplegia, making patients resistant to vasopressor therapy.35–37 These effects may contribute to the failure to restore normal physiology despite successful surgical haemorrhage control.
Our finding that non-survivors required significantly larger transfusion volumes aligns with extensive literature linking massive transfusion to adverse trauma outcomes.38–40 The higher pre-operative and intraoperative RBC and FFP requirements in non-survivors likely indicate more severe haemorrhage, greater shock levels and potentially more extensive injuries necessitating complex damage control procedures. The markedly higher rate of inotropic support in non-survivors (91.7% vs. 50.9%) further supports the idea of more profound cardiovascular compromise in this group. It suggests that many of these patients had advanced beyond the point of reversibility by the time of surgical intervention.
The lower rates of ICU admission (66.7% vs. 98.4%) and relook laparotomy (28.6% vs. 94.2%) in non-survivors suggest that many did not survive long enough to undergo these interventions. Rather than implying that ICU care or reoperation are harmful, these findings likely reflect that many non-survivors died before these procedures could be performed, either intraoperatively or in the immediate postoperative period. This emphasises the importance of early mortality as a competing outcome in DCS populations and highlights the narrow therapeutic window for intervention in these critically ill patients.
Limitations
Several limitations of this study warrant acknowledgement. The retrospective design introduces the potential for selection bias and limits our ability to establish causality between identified predictors and mortality. The single-centre nature of this study may limit generalisability to other settings with different patient populations, injury mechanisms, or practice patterns. Our sample size was adequate for the primary analysis, but sample size constraints limited subgroup analyses (e.g., organ-specific injury patterns) and should be interpreted with caution. We did not have data on injury severity scores, abbreviated injury scales, or other trauma-specific scoring systems that may provide additional prognostic information. Finally, the study population was predominantly young males with penetrating trauma, which may not be representative of DCS populations in other geographic or demographic settings where blunt trauma or older patients may predominate.
Clinical implications
Despite these limitations, our findings carry significant clinical relevance for trauma surgeons and intensivists managing this challenging patient group. The three identified predictors: lactate, GCS and pH are easily accessible at the bedside and do not require complex calculations or specialised equipment beyond standard point-of-care testing. Clinicians can utilise these parameters to identify patients at the highest risk of death, potentially guiding early and honest discussions with families regarding prognosis, aiding resource allocation decisions in mass casualty situations, and recognising patients who might benefit from more aggressive or innovative resuscitation strategies, including extracorporeal life support. Future prospective multicentre studies should validate these results across diverse populations and investigate whether interventions targeting these parameters, such as goal-directed lactate clearance resuscitation or pH-guided buffer administration, can enhance outcomes in this high-risk group.
Conclusion
This retrospective analysis of 219 patients undergoing DCS identified lactate, Glasgow Coma Scale and arterial pH as independent predictors of in-hospital mortality. Elevated lactate emerged as the strongest predictor of death, followed by lower GCS and lower pH. These easily obtainable clinical parameters, integrated into a predictive model with excellent discrimination (AUC 0.912), may help clinicians in prognostication and guide resuscitation efforts in this critically ill patient group. Future prospective studies are needed to validate these findings and to explore targeted interventions for improving outcomes in high-risk patients undergoing damage-control surgery.
Footnotes
Acknowledgements
We acknowledge the surgical and nursing teams who care for trauma patients at our institution. No individuals received compensation for their contributions to this work.
Ethical approval
This study was approved by the University of Witwatersrand Human Research Ethics Committee (Reference Number: M250705, approved 25/07/2025). The study was conducted in accordance with the Declaration of Helsinki as revised in 2024. Given the retrospective nature of the analysis using de-identified data extracted from medical records, the ethics committee waived the requirement for individual informed consent. Patient privacy and confidentiality were maintained throughout the study.
Informed consent
As this was a retrospective observational study and did not involve any prospective intervention or assignment of treatment, trial registration was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.