
Abstract
Background
Distal radius fractures are the most common fractures among adolescents and young adults. In addition to Kirschner wires, after growth plate closure anatomical volar or dorsal radius plates may also be used for fixation. Current volar plates have been designed to fit the wrist of an average adult patient. The aim of this article was to review the use and the suitability of anatomical plates in the treatment of teenagers.
Methods
Retrospective data from patient records was collected on 59 patients, aged from 13 to 19 years, who underwent a plate fixation of distal radius at a tertiary center (level one university trauma hospital). An anatomical plate had been used in 32/59 (54.2%) of the patients. We reviewed and analyzed patient characteristics, injury mechanisms and types, post-operative complication, and pre- and post-operative radiological parameters.
Results
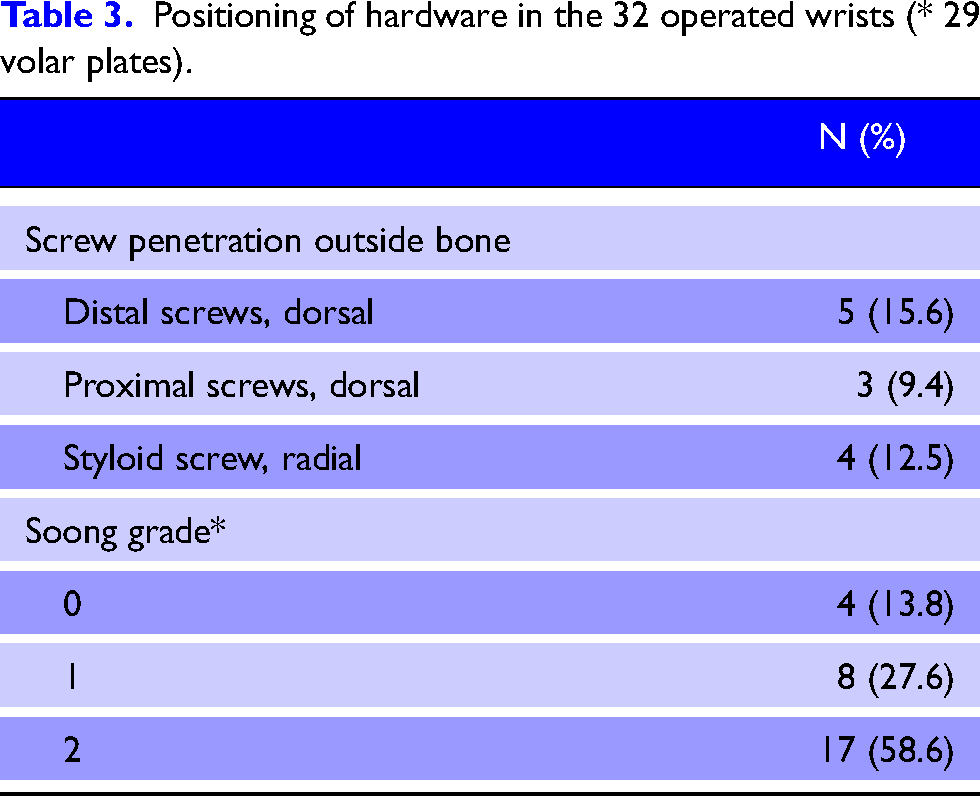
29 wrists were operated using volar and 3 using a dorsal anatomical plate. Anatomical plates had not been used in patients aged ≤14 years. Out of the 29 cases, in 17 (58.6%) wrists the plate positioning corresponded to Soong gr II. In our follow-up period, the incidence of the post-operative complications was not greater than reported among adults. The plate was removed post-operatively in two cases. One removal was done due to inadequate plate positioning causing tendon irritation, and the other due to superficial wound infection.
Conclusions
Kirschner wires should be considered the first line of treatment when operating distal radius fractures in teenagers. Hardware protrusion seems to be common when anatomical volar plates are used. Further research is required to assess the long-term safety and the cumulative rate of complications from the use of anatomical volar plates in teenagers.
Introduction
In recent decades, the use of anatomical volar plates has virtually replaced the use of external fixation in the treatment of distal radius fractures in adults. 1 In adolescents with open growth plates, Kirschner wires are utilized when fracture alignment cannot be maintained by casting alone.2,3 For older adolescents, non-anatomical plates that can be contoured individually and placed proximal to the physis are an option. 4 Anatomical volar fracture plates are designed to fit the volar distal radius of an average adult. The palmar cortical angle is narrower in adolescents, and this difference may persist even to early adulthood and may create special challenges in fitting a volar plate to the palmar cortical angle of the radius. 5 Growth plate closure is a gradual process occurring in a duration of a few years and occurs later in males than in females. Currently the optimal age for switching to anatomical volar plates is not known. Still, few studies have analyzed the use of volar plates specifically in adolescents and young adults.
In our institution, pediatric orthopedic surgeons tend to most often utilize pinning in the treatment of adolescents ≤15 years, whereas patients ≥16 years are treated in the adult department where anatomical plates are most often used. This motivated us to find out if the anatomy of the teenage wrist poses specific challenges in fitting the volar plate in teenagers’ distal radius fractures.
Methods
We collected retrospective data from a level one University trauma hospital. A search for all patients ages 13–19 who had undergone plate fixation for distal radius fracture in Turku University Hospital from 1 Jan 2010 to 30 April 2021 was performed using codes NCJ62 and NDJ62 (plate fixation of distal radius fracture, plate fixation of hand fracture) and ICD-10 codes S52.5, S52.6 (distal radius fracture, distal antebrachium fracture). A total of 59 patients were identified. Screening post-operative X-rays was performed to identify 32 (54.2%) patients who had been fitted with an anatomical plate. Our primary outcome measures were screw penetration and Soong grade measured from plain X-rays. The use of patient data for this study was approved by the management of Turku University Hospital (Project code: Distal_Radius_Fract-TYKS-1.1).
Results
Patient characteristics are shown in Table 1. Volar plates had not been used in patients aged 13 to 14. The median age of patients was 17 (range 15–19, interquartile range (IQR 16–18). Of 32 operated wrists, volar anatomical plate using a modified Henry approach was used in 29 cases (Aculock 28, Synthes 1), and a dorsal anatomical plate was used in three cases. One case underwent simultaneous pinning of the scapholunate interval, and a headless compression screw was used to fix a scaphoid fracture in one case. One patient underwent simultaneous volar plating of the fracture of the distal ulna. The ulnar styloid was fractured in 21/32 cases, of which 6 (28.6%) underwent operative repair (5 with K-wires, 1 with K-wires and tension band). There were no open fractures.
Patient characteristics of 32 patients operated with anatomical distal radius plates.
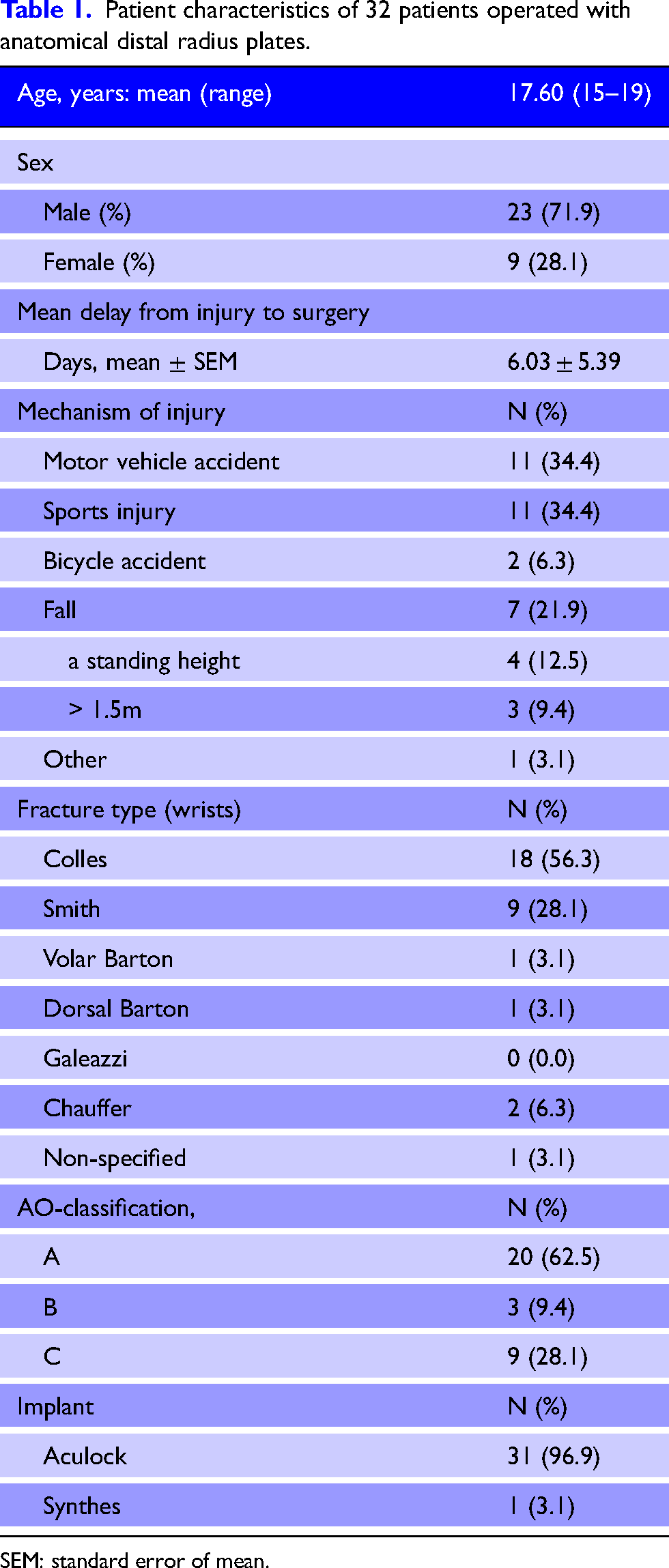
SEM: standard error of mean.
Post-operative X-ray images were available from all patients. Radiological parameters before and after the procedure are presented in Table 2. Of the 29 wrists operated with a volar plate, the positioning of the plate corresponded to Soong gr II in 17 wrists (58.6%).
Radiological parameters before and after surgery (32 wrists).
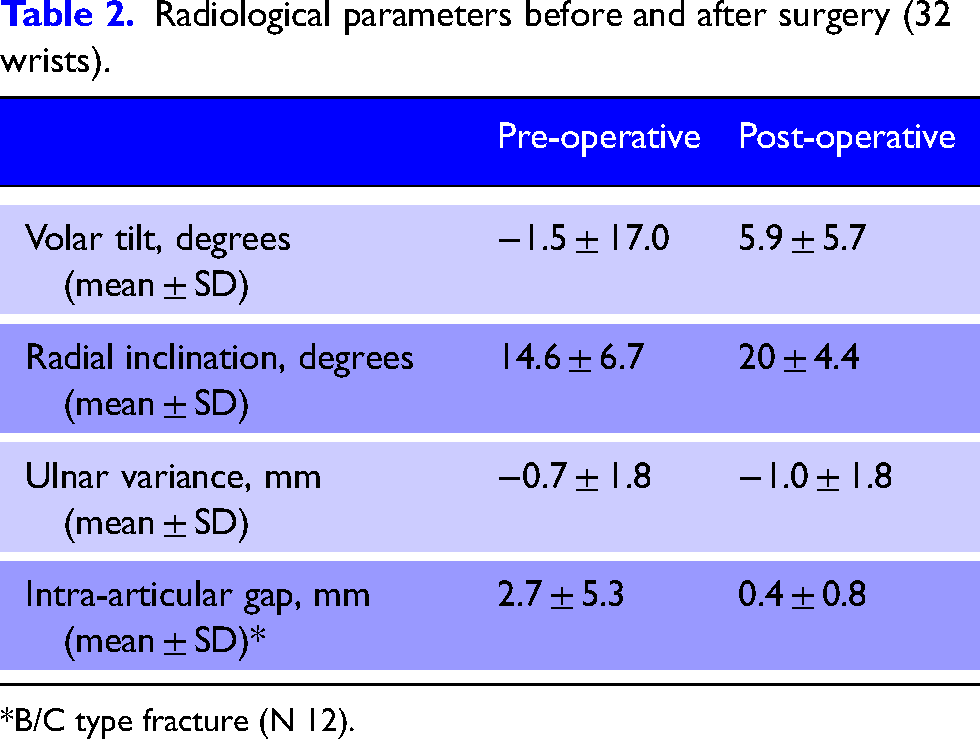
*B/C type fracture (N 12).
Only one patient—a 15-year-old male—with open radial physis underwent surgery using an anatomical volar plate. Figure 1 shows that the anatomical volar plate positioned proximal to the physis does not fit the palmar cortical angle causing the distal end of the plate to diverge from the palmar cortex. The patient later had the plate removed due to tendon irritation caused by the protruding plate. Among the patients with closed physis, one patient had undergone plate removal (after a superficial wound infection) making the total number of plate removals 2/32 (6.7%).
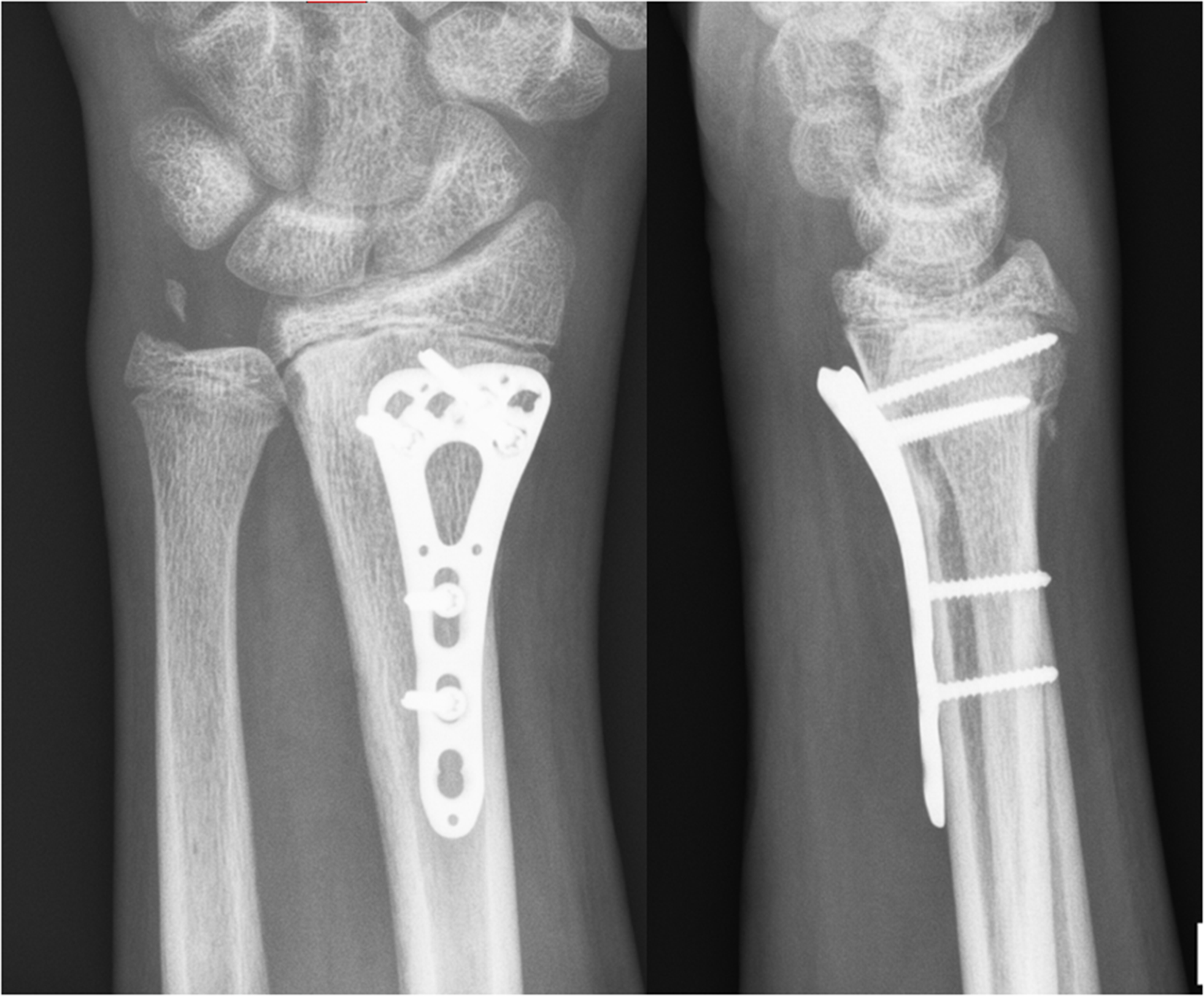
A 15-year-old male underwent volar plating of a distal radius Smith fracture at age 15. An anatomical plate was used, which was positioned proximal of the radial physis. The palmar cortical angle of the patient at the proximal level was less than that of the anatomical volar plate causing the plate to protrude from the radial cortex. Patient later underwent removal of the plate due to tendon irritation and pain.
Superficial wound infection developed in one case; another patient developed a pyogenic granuloma. Other complications were one case each of non-union, neurapraxia, and chronic regional pain syndrome. There were no cases of deep infection/osteomyelitis and no nerve, tendon or arterial lacerations. There were no cases of malunion.
Discussion
Distal radius fractures occur in all age groups but are especially common in children and adolescents. Still, the optimal surgical treatment in teenagers remains somewhat controversial and up for debate.6,7 Pediatric orthopedic surgeons treat dislocated fractures in children with open growth plates with pinning, while adult orthopedic surgeons utilize anatomical volar plates. In this study, we report 32 distal radius fractures of adolescents aged between 15 and 19 years treated using an anatomical plate.
A common method of evaluating the risk of tendon rupture after volar plate application is the Soong grade8–10 The position of the volar plate is given a grade of 0,1 or 2 based on the location of the plate in relation to the volar critical line and watershed of the distal radius.8,10 The important implication of the Soong grade is that especially patients with plate position corresponding to grade II are especially prone to develop flexor tendon rupture in long-term follow-up.8–10 An interesting finding was that 17 of 29 (58.6%) wrists operated using an anatomical volar plate were classifiable as Song grade II (Table 3). This means greater plate prominence leading to the plate passing the volar critical line hypothetically causing flexor tendon strain in the long run and a more probable need for a plate removal in the future. 8 Tendon ruptures due to protruding volar plates may develop slowly even after several years. 9 In a 2020 study with average patient age of 56.5 years and a mean follow-up period of 9.1 months, the authors found incidences of tendon rupture in 0.5%, tendon irritation in 2.5%, and need for plate removal in 6.5% of the cases. 9 In our patients during the fairly short follow-up period of our study only 6.7% of the patients required plate removal, but it should be noted that there was only one patient in the series with an open physis (Figure 1). This patient had a significantly protruding plate that caused tendon irritation requiring plate removal. Based on this experience, we strongly recommend against the use of anatomical plates in patients with open physis. Considering the relatively young age of our sample patients and presumably numerous years ahead of them, there is a high probability of complications related to flexor tendons in the future. 10 Penetrating screws may cause irritation and require revision surgery. In our series screw penetration was encountered less frequently than Soong grade 2, and during our short follow-up period we did not encounter complaints due to penetrating screws.
Positioning of hardware in the 32 operated wrists (* 29 volar plates).
There is no consensus regarding the exact age at which the fractures needing surgical fixation begin to favor treatment with anatomical volar plate instead of Kirschner wires. In many cases, the choice of procedure depends on varying factors including the operating surgeon's field of specialty, experience, and preference as well as resources available and the age at which patients treatment transitions to the adult department. 11 For example, in our setting adolescents under 16 years are treated in children's clinic mainly by pediatric orthopedic surgeons, while adolescents 16 years or older are treated in the adult department which explains the preference of using volar plate among adolescents of said age group. The volar tilt of radius sees a significant increase from childhood to adulthood which may affect the suitability of volar anatomical plates designed for adults among adolescents. 12 However, in our study, there were no complications related to plate positioning requiring reoperation, except in one case where volar plate was positioned proximal to the growth plate (Figure 1). Clinicians should be cautioned not to use anatomical plates in patients with open growth plates.
The common mechanisms of fractures among adolescents are also considerably different when compared to adult population. In our study focusing on adolescents treated with volar anatomical plate, the two biggest mechanisms of injury among the 32 cases were high-energy injuries, in either sports (11 cases) or in traffic (11 cases), while among adults most injuries were caused by a simple fall.13,14 The significant difference when comparing fractures between adolescents and adults should be noted, hence the type of fracture also affects the choice of management of distal radius injuries. 15
There are several limitations to this study. The sample was relatively small with 32 wrists analyzed, which limits the generalizability of the results. Due to the retrospective nature of the study, there can be events and consequences unknown to the researchers. Furthermore, all the wrists in our study were operated during the previous and the current decade and, hence, the follow-up period was relatively short and limited to what was in the charts. Thus, our main outcome was plate protrusion in X-rays. Only by reviewing the status of these patients after 20–30 years from today, we will be able to assess the complications caused by the plates in the long run.
Conclusions
Fixation using an anatomical volar plate is an option to achieve immediate stable fixation when operating distal radius fractures in adolescents with fused growth plates, but is associated with a significant rate of hardware protrusion. The use of Kirschner wires avoids complications related to hardware, but can equally allow early mobilization of the wrist, as described in recently by Passiatore et al.16,17 The literature on the use of plate fixation for unstable displaced distal radius fractures in children is still limited. 18 Our main findings were a strong recommendation against the use of anatomical volar plates in patients with open physis. The positioning of volar plates in the teenage wrist does seem challenging with high proportion of plate positionings corresponding to Soong gr II. A longer follow-up period is required to determine long-term applicability of a standard anatomical volar plate and cumulative rate of complications from fitting it into a teenager's wrist.
Footnotes
Author Contributions
MP conceptualized the manuscript. AS was responsible for cleaning and analyzing the data, AGS wrote the draft manuscript, and MP contributed by providing feedback, interpreting results, and refining the manuscript. Both authors reviewed and edited the manuscript and both authors have read and approved the final version of the manuscript.
Consent to participate
Waived for retrospective chart review.
Consent for publication
Waived for retrospective chart review.
Data availability statement
Original data is stored in the research archive of Turku University Hospital, Turku, Finland. Due to Finnish legislation on the secondary use of health and social data the original data is not available for public use.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Pääkkönen: KSL Martin, speaker reimbursement.
Ethical approval
The use of patient data for this study was approved by the management of Turku University Hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not required for retrospective chart review.
Project code
Distal_Radius_Fract-TYKS-1.1.