
Abstract
Background
Falls from height are associated with significant traumatic injuries and poor outcomes. Improving our understanding of patterns associated with this patient group enables clinicians to improve their patient management in the prehospital and hospital environment.
Objectives
To describe the injury patterns and clinical outcomes of patients presenting to the Emergency Department at University Hospitals Southampton after falling from the Itchen Bridge, Southampton.
Methods
We conducted a retrospective cohort study of thirty patients who attended University Hospital Southampton following a fall from the Itchen Bridge between 2011 and 2023. Twenty-six patients who fell into water from heights of approximately 20-30m were included in the primary analysis. Clinical data were then extracted from medical records.
Results
Hypothermia was the most common presentation (n = 23), followed by pneumothoraces (n = 14), rib fractures (n = 10), thoracic vertebral fractures (n = 9) and lung contusions (n = 8). Lower water temperatures at the time of the incident (p = 0.008) and lower patient body temperatures on arrival to hospital (p = 0.002) were significantly associated with increased 30-day mortality.
Conclusion
Falls from heights of 20-30 m into water frequently results in hypothermia and intrathoracic injuries. Prehospital clinicians attending falls into water from similar heights should recognise the importance of early rewarming to treat hypothermia and be suspicious of intrathoracic injuries.
Introduction
The World Health Organisation reports that there are around 700,000 suicides worldwide every year. 1 In 2021, 5,199 deaths were due to suicide in England and Wales, and the most at-risk groups were men and individuals between the ages of 50–59. 2 Of the 140,000 suicidal attempts in the UK each year, jumping from height makes up approximately 3–15% of the cases. 3 Individuals who jump from height usually have a history of significant psychological disorders, and this suicide method is often associated with poor outcomes, both physically and psychologically. 4 Several sites around the world have gained notoriety as suicide hotspots, 5 and bridges particularly stand out amongst this group, with perhaps the Golden Gate Bridge being the best known. 6
Previous studies on individuals who have fallen from bridges have varied in their approach, with some focussing solely on deceased individuals,7,8 individuals admitted to an Intensive Care Unit 9 and survivors. 10 Demographics of individuals, 11 bridge height,12,13 type of surface fallen onto, 14 depth of water, 12 the velocity at impact, 7 and orientation of body at the time of impact 15 are factors that have been identified that impact patterns of injury and mortality. Numerous studies have identified thoracic injuries as the most common7,16,17 and whilst some found a low incidence of spinal fractures, 7 this is not consistent universally. 12
The objective of this study was to describe the patterns of injury and clinical outcomes of people who fell from the Itchen Bridge (Figure 1) and attended the Emergency Department at University Hospital Southampton (UHS). Additionally, we wanted to see if there was a correlation between water temperature and patient outcomes. We sought to build on previous studies by identifying which injuries and clinical conditions were most common in this patient group to speed up diagnosis and subsequent management of further similar cases.

Itchen Bridge connects the suburb of Woolston with the city centre, across the River Itchen, a major tidal tributary to Southampton Water. 18
Study design
The study was a retrospective cohort analysis of patients who attended the Emergency Department at UHS after a fall from the Itchen Bridge from 1st April 2011 to 31st March 2023. Patients were identified by searching the Trauma Audit and Research Network (TARN) database. TARN was initially searched for patients who presented to UHS between 1st April 2010 and 31st March 2023 following a fall of >2 m, where the incident postcode matched the bridge postcode areas.
Shortly after the TARN searches, a cyber-security event prompted the reorganisation of TARN into the National Major Trauma Registry (NMTR). 19 No further data could be obtained via TARN/NMTR. To ensure all appropriate patients were captured rigorously, additional records were found by auditing the UHS Emergency Department's electronic clinical noting system, Symphony (Figure 2).
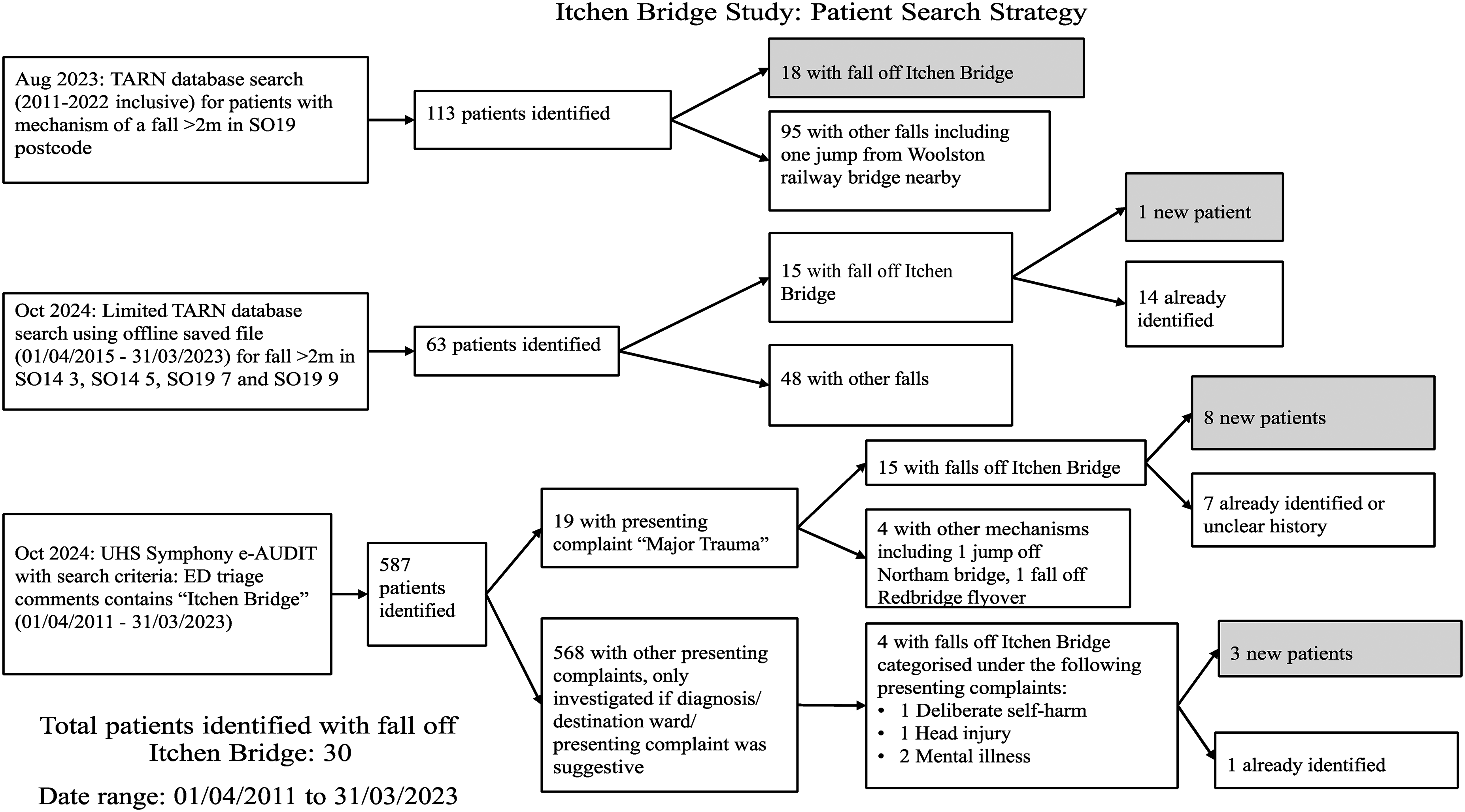
Patient search strategy.
A Symphony e-Audit was completed for the date range 1st April 2010 to 31st March 2023, with the criteria that the phrase “Itchen Bridge” was included in the triage comments. These notes are typically recorded on the patient's arrival to Emergency Department, usually by the triage nurse, to provide a brief summary of the presenting complaint.
Data on the height of tide, water temperature and air temperature at the time of each incident were obtained from two different local weather stations. These stations provide open source, archived weather data from 2009, recording every 5 min, as part of a charity-run weather data collection organisation called Solentmet. 20 The Sotonmet sensor is located at the mouth of the River Itchen, 1.7 km from the bridge, and provides height of tide and air temperature data. Cambermet is located in Chichester Harbour, 36 km from the bridge, and was the closest source of archived, open-access water temperature data available to use. Although local weather and microclimate conditions may mean the temperature under the Itchen Bridge differs from that measured by the Cambermet sensor, both locations are tidal bodies of saltwater, open to the Southwest, with similar depths.21,22 For that reason, Cambermet provided a reasonable approximation of the water temperature under the bridge at each incident. Not all incidents had incident times recorded, and for those that did not, the incident time was taken to be one hour before arrival in the hospital.
Statistical analysis examined the relationship between 30-day mortality and environmental variables, including atmospheric temperature, water temperature, and water depth. Mortality was treated as a binary variable (0 = Alive, 1 = Dead), and point-biserial correlation coefficients were calculated to assess associations with these environmental variables. Statistical significance was determined using two-tailed p-values. Boxplots were generated to visualise differences in environmental conditions between survivors and non-survivors, with overlaid swarm plots for individual data points. Fisher's exact test was used to compare 30-day mortality for males and females. Analyses were performed using Python 3.8.1 (Seaborn, SciPy, Matplotlib, and Pandas libraries) in the Spyder Integrated Development Environment (IDE).23–27
Setting
The Itchen Toll Bridge is a central road bridge in Southampton. Part of the bridge spans the water of the River Itchen, but significant lengths of the bridge on either side overlie concrete or tarmac roads. The bridge's highest point varies (depending on the height of tide) between 26 m to 31 m above the river, with the water depth below that point varying from 3.1 m to 8.1 m.21,28 Approximately 200 people have died falling from the bridge since its opening in 1977. 29 As of December 2024, the sides of the bridge are formed by 58 cm high concrete walls, making jumping from the bridge very accessible. However, there is a plan to install higher physical barriers to prevent these events. 30 There are suicide prevention notices and help points that provide a telephone link to emergency services at regular intervals along both sides of the bridge.
South Central Ambulance Service NHS Trust (SCAS) provide the statutory ambulance service response to trauma incidents within the Hampshire area. Clinicians from the Hampshire and Isle of Wight Air Ambulance service provide an enhanced critical care response. UHS is the leading tertiary centre for major trauma, which is 5.2 miles from the bridge. It is improbable that patients would be transported to any other hospital, given its proximity.
Results
30 patients were included in the final analysis, 26 patients fell from a middle section of the bridge into the water and four fell onto land. Overall, these patients were very seriously injured: six patients were in cardiac arrest on scene or on arrival in the Emergency Department (6/30), and 30-day mortality was 5/30. Overall, ten patients were female, and 20/30 were male, with an average age of 34.1 ± 12.0 years. 30-day mortality for males was 2/10 and for females it was 4/10. However, this difference was not statistically significant (p = 0.151). There was also no significant difference in the frequency of these incidents in different months of the year, days of the week, or times of day
Of the six patients in cardiac arrest either prior to arrival or in the Emergency Department, the mortality rate was high (5/6) and the majority (5/6) fell into water. The patient who survived, landed in water and presented with an isolated hypothermia (29.4°C on arrival to hospital). They had been witnessed to jump into the water and swam for around fifteen minutes before being removed from the water in cardiac arrest. Out of the four other patients who fell into the water in this cardiac arrest subgroup, one presented with multiple thoracic and abdominal injuries and the other three with isolated hypothermia. The patient who fell onto land presented with significant injuries and had multiple long bone, rib and pelvic fractures, multiple thoracic injuries and significant blood loss.
The group that fell into water (n = 26) formed the main focus of this analysis (Table 1). In this group, 30-day mortality was 4/26 and the most common clinical outcome was hypothermia (23/26). Hypothermia was defined either by a prehospital body temperature of <35°C or a documented unrecordable temperature. Notes in the latter case generally mentioned phrases like “cold”, “peripherally shut down” or “unable to record temperature”.
Summary table.
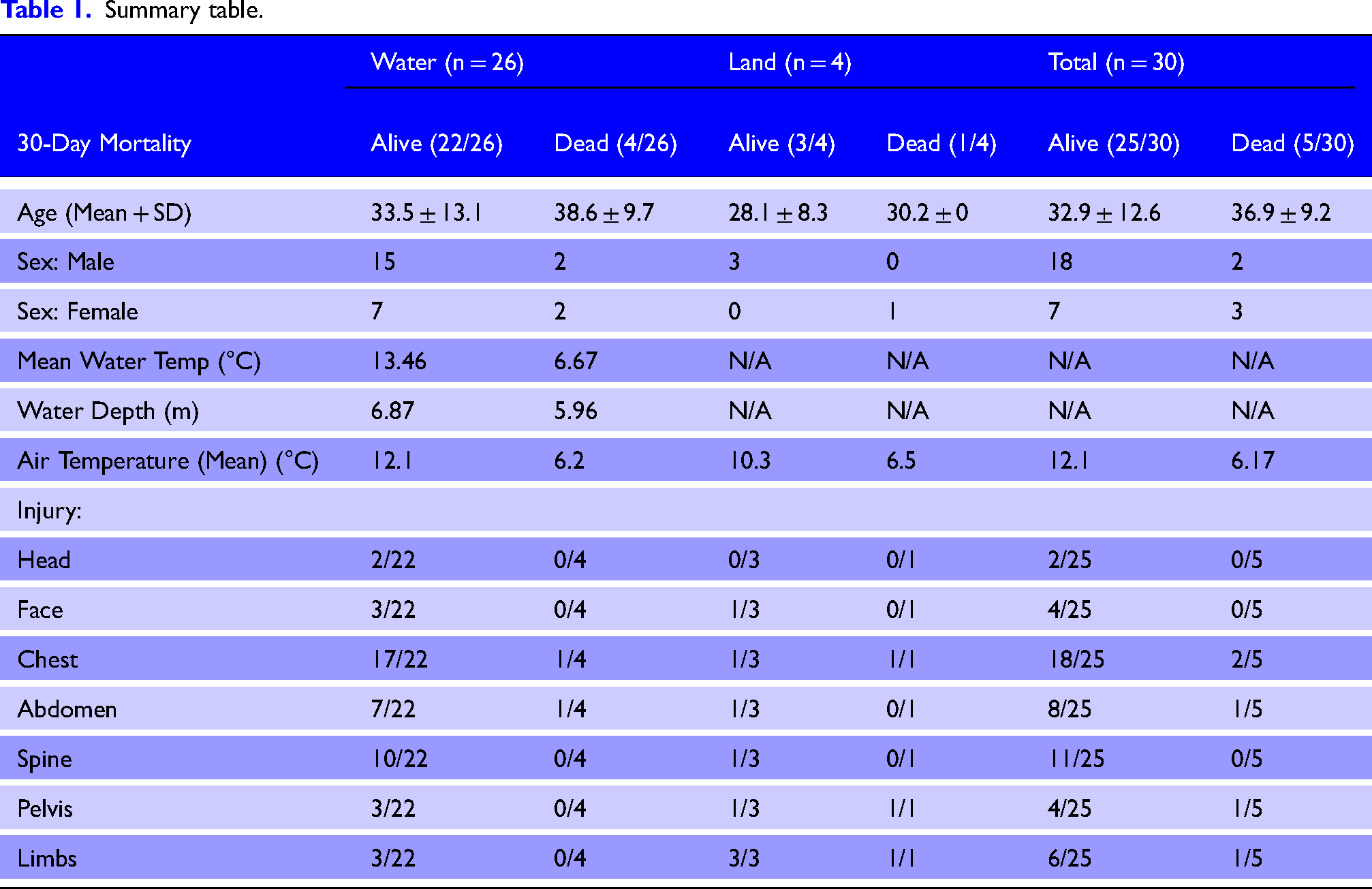
In the 26 patients who jumped into water, 14/26 had recorded pre-hospital temperatures of <35°C, and 9/26 had unrecordable temperatures. Out of the 9/26 with unrecordable prehospital temperatures, 8/26 were then recorded in the Emergency Department, with an average temperature of 32.6°C (range 29.0°C-36.7°C). The remaining patient had incomplete documentation and died shortly after arrival. Three of nine patients with an unrecordable prehospital temperature died within 30 days, meaning that of the 4/26 patients who died from the group who fell into water, three had an unrecordable body temperature prehospitally. Having an unrecordable temperature prehospitally was associated with 30-day mortality, but this did not reach statistical significance (p = 0.116), likely due to low numbers.
On arrival to the Emergency Department only 13/26 patients had temperatures of <35°C. The average first recorded temperature in the Emergency Department was associated with 30-day mortality (p = 0.002, Figure 3). The average first recorded temperature in the subgroup of 22 patients who survived was 34.4°C, whilst the average in the subgroup of four patients who died by 30 days was 29.7°C.
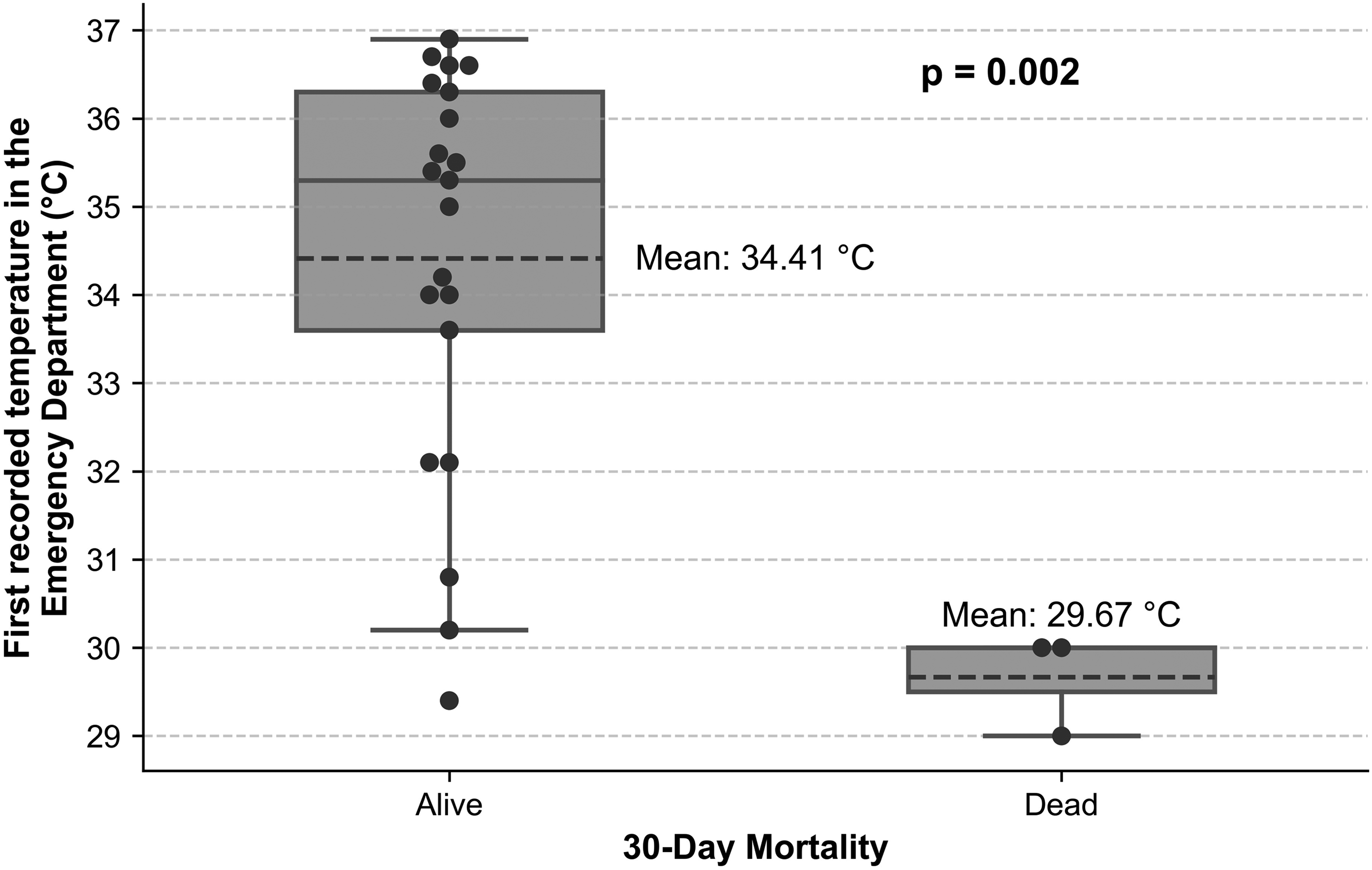
Relationship between body temperature and 30-day mortality in the Emergency Department.
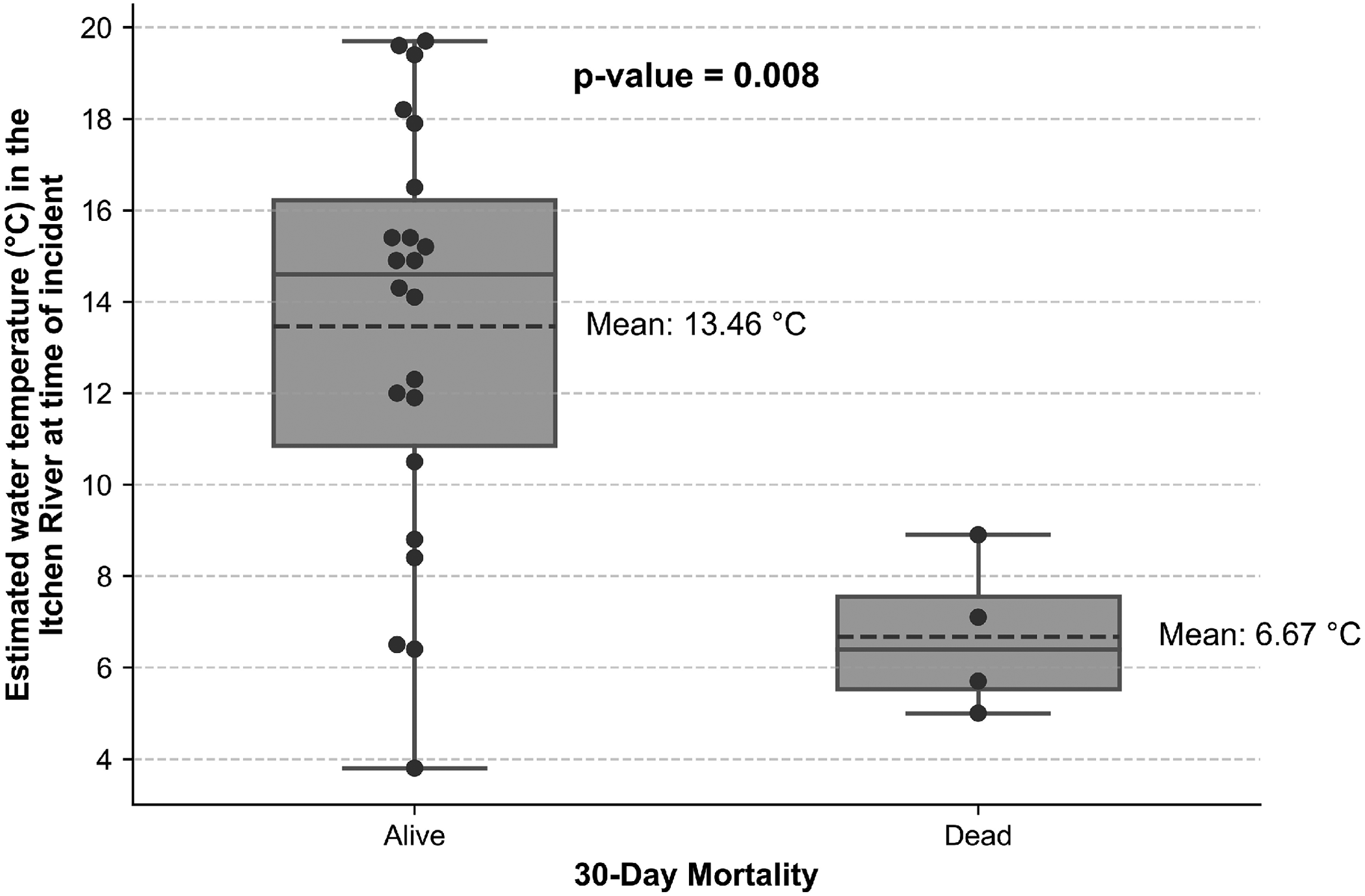
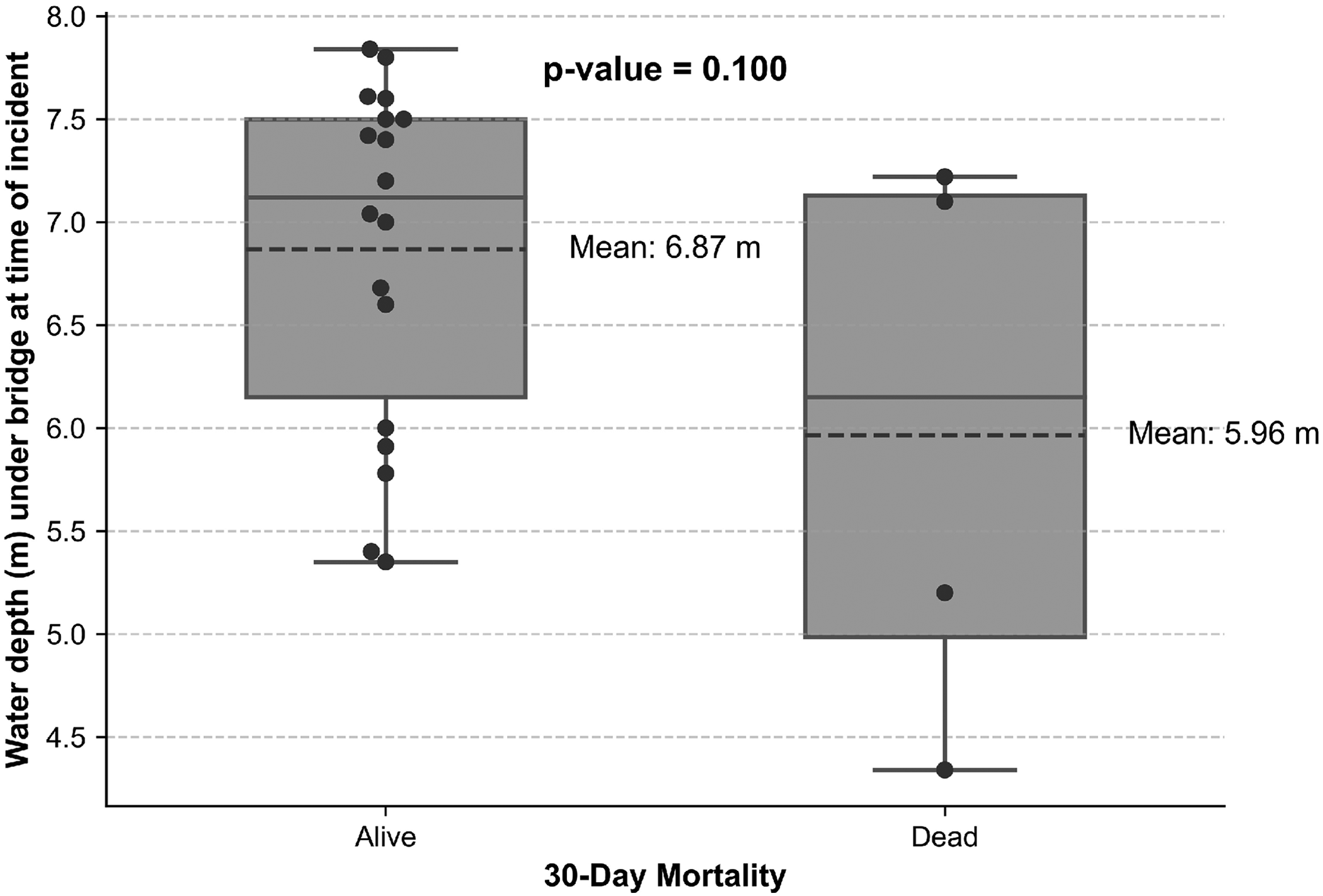
Hypothermia and 30-day mortality were analysed against air temperature, water temperature, and water depth at time of incident. Though patients who experienced colder water or colder air temperatures on the day of the incident were more likely to get hypothermia, neither of these correlations reached statistical significance. The relationship between 30-day mortality and air temperature, water temperature, and water depth is shown in Figures 4–6. In the group who did not survive to 30 days, patients were more likely to have experienced colder water (6.7°C vs 12.1°C, p = 0.008).
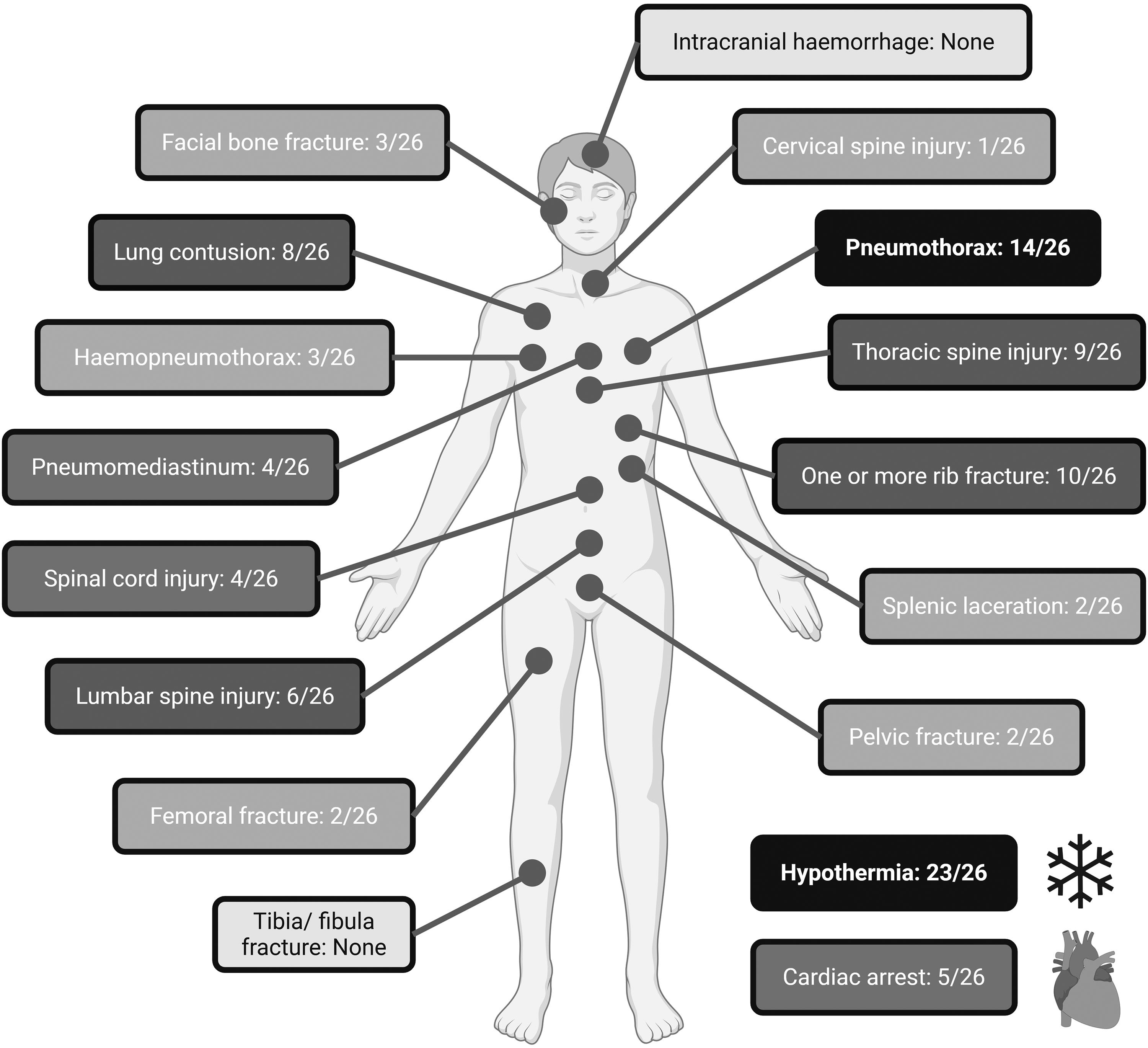
Clinical outcomes seen in the 26 patients who fell from Itchen Bridge into water. Created in BioRender. Nottingham, T. (2025) https://BioRender.com/q10j418.
There was a high rate of injuries to the thorax and thoracic spine. The second most common clinical outcome was a pneumothorax (14/26), at least five of which were bilateral (Table 2 and Figure 3). A total of ten patients exhibited one or more documented rib fractures (10/26). This observation is noteworthy because it indicates that not all patients with pneumothorax presented with rib fractures. Additionally, eight patients sustained lung contusions (8/26), which frequently led to ventilation issues during subsequent intensive care. Vertebral injuries were common, with nine patients presenting with thoracic fractures (9/26), six with lumbar fractures (6/26) and one with cervical fractures (1/26). Commonly, these vertebral fractures involve the transverse processes. There was no data available regarding orientation of the body at the moment of impact and therefore it was not possible to evaluate whether orientation affected patterns of injury.
Clinical outcomes in water and land groups.
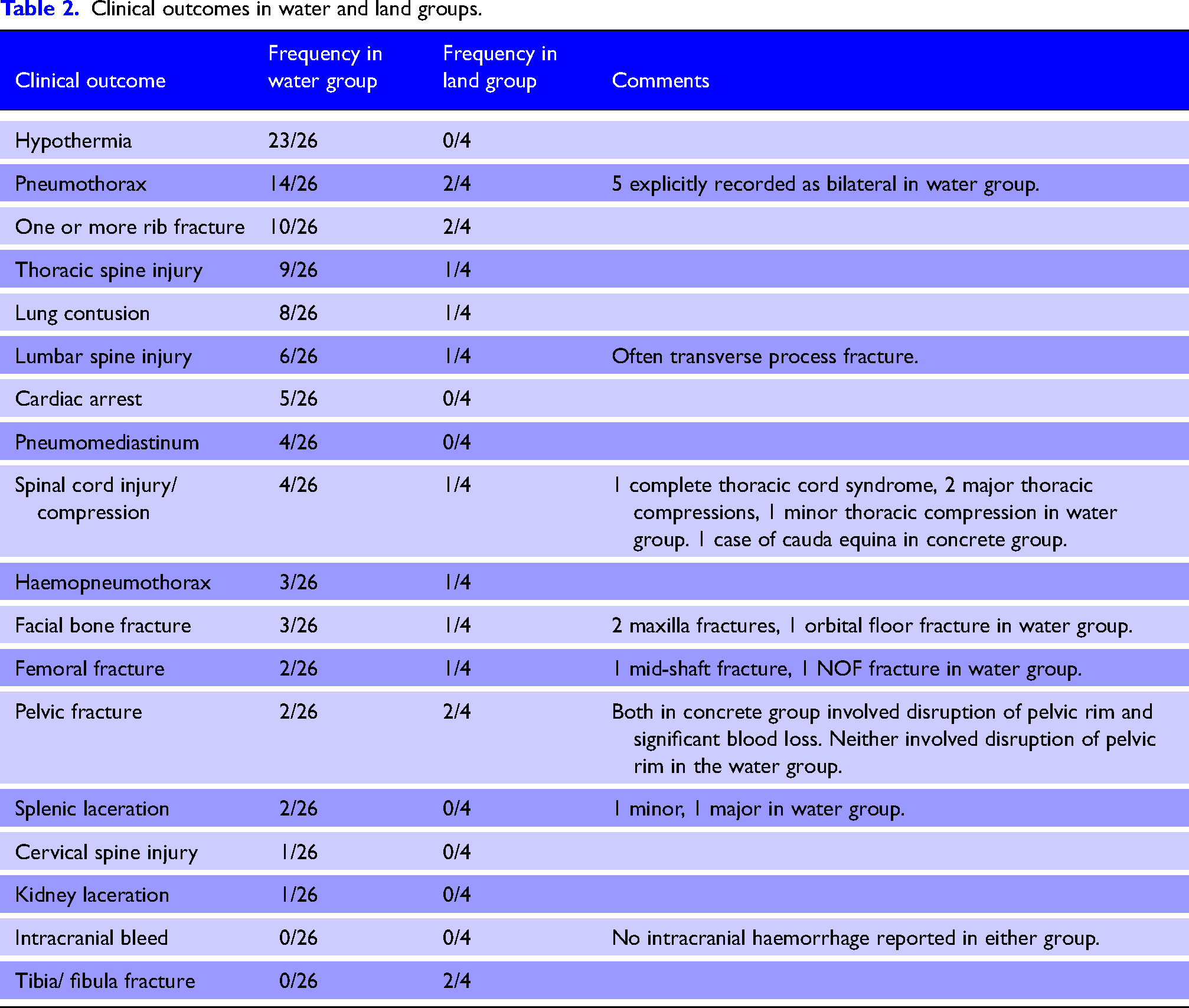
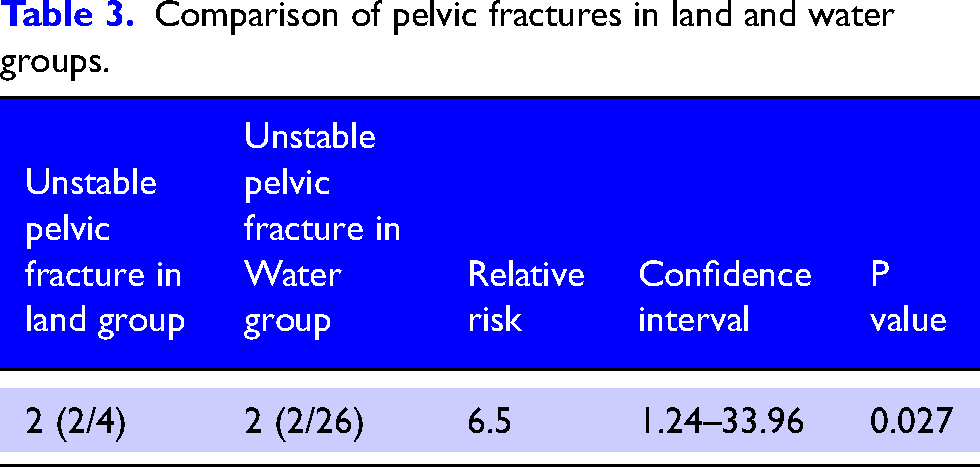
Though the group of patients who fell onto land is small (4/30), injury patterns appear to be substantially different from those who fell into the water. Rib fractures and pneumothoraces were recorded in both these groups, but 2/4 of the group that landed on the ground had unstable pelvic fractures, compared to 2/26 in the water group, neither of which involved pelvic rim displacement (Table 3). Leg fractures were also more common within the group that landed on the ground, with tibia/fibula (2/4) and femoral (1/4) fractures being reported (Figures 5–7).
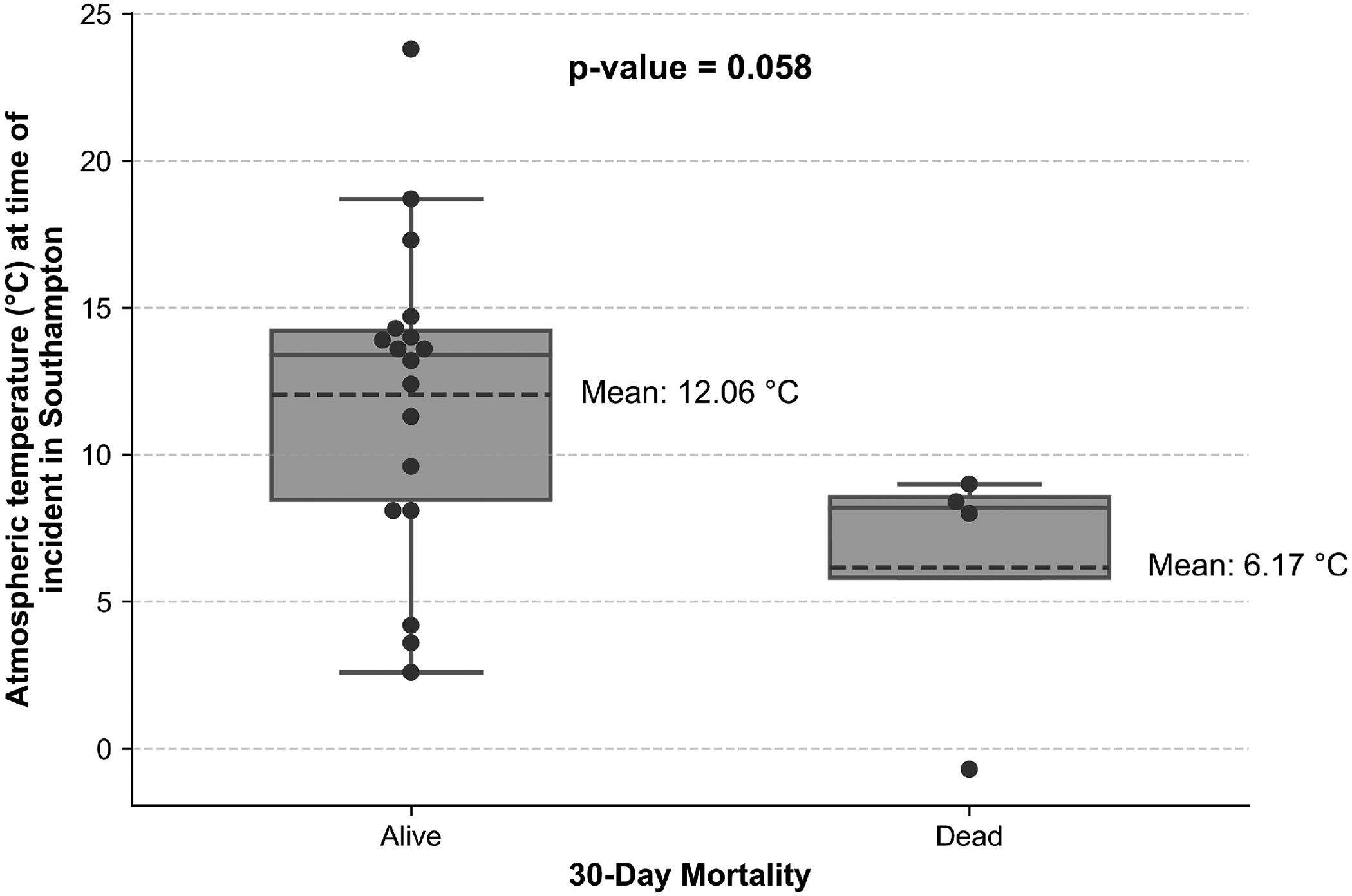
Relationship between 30-day mortality, air temperature, water temperature and water depth under the bridge at the time of each incident. Only the estimated water temperature, which was derived from the Cambermet dataset, 31 reached statistical significance.
Comparison of pelvic fractures in land and water groups.
Discussion
This study demonstrates the severe and complex nature of injuries sustained by individuals who have jumped or fallen from the Itchen Bridge (Table 1) and highlights the diagnostic and therapeutic challenges that pre-hospital clinicians encounter. It is difficult to assert with certainty that all individuals in this study deliberately jumped due to incomplete documentation. However, there was no indication in the documentation reviewed that any patient accidentally fell. Furthermore, the sides of the bridge are not an insignificant height 30 and therefore we believe all individuals intentionally jumped from Itchen Bridge.
Men and young people were disproportionately represented in this patient group, which is consistent with other studies that examine suicide by jumping from bridges or heights.12,32,33 These trends also align with national statistics 34 that identify men as a high-risk group for suicide attempts.
In the patients who fell into the water (26/30), hypothermia emerged as the most common clinical outcome. There was no relationship between sex or age and incidence of hypothermia. This could be related to water temperature, intent, ability to swim, use of alcohol or drugs, distance from the shore, or the time of emergency services’ arrival. In 2024, SCAS reported a mean response time of seven minutes to category 1 cases. 35 The estimated 50% survival time for individuals in water of 5°C (41°F) is one hour, rising to 2 h 12 min for water temperatures of more than 10°C (50oF). 36 Whilst the dataset used did not elucidate total immersion times, it is possible that with the mean water temperature of 6.47°C seen in the non-survivor group and 12.1°C seen in the survivor group, water temperature may account for the significant mortality difference witnessed between the two groups. Given the large injury load seen in some of these patients as well, with sequelae such as hypovolaemic shock, this may have resulted in the lethal triad of hypothermia, coagulopathy and acidosis. A recent systematic review that included seven studies for meta-analysis concluded that accidental hypothermia at admission was associated with significantly higher mortality in trauma patients, with an odds ratio of 5.18 (95% confidence interval) 2.61- 10.28). 37 It is likely that a combination of injuries and rapid cooling due to cold water temperatures had a simultaneous detrimental effect on the outcomes of these patients.
Thoracic and spinal injuries were highly prevalent amongst those who fell into the water, and a similar pattern was found in other similar studies. 12 The severity of the thoracic injuries seen was variable. Pneumothoraces were present in over half of the cases, and a number (5/26) were bilateral. Rib fractures (10/26) also had a high incidence, but the precise nature and severity are difficult to quantify. There are multiple reasons why patients in this cohort may have had pneumothoraxes without overlying rib fractures, including alveolar rupture and barotrauma on impact, and has been described in previous papers. 38 Lung contusions were similarly frequent, reflecting the high-energy transfer during impact and the potential of ventilation issues arising as a result.
The reason behind the high incidence of thoracic and spinal injuries (mainly involving the transverse processes) remains unclear. The depth of the river below the centre of the bridge is between 3.1 m and 8.1 m, depending on the tide, and the riverbed is made up of mud or soft shingle. 21 The depth can be significantly shallower at either end of the bridge. 20 As water is a displaceable medium, it allows for a more extended deceleration period than non-displaceable mediums such as the riverbed. The greater the deceleration, the greater the energy dissipation, which theoretically results in less trauma. 7 However, calculating the depth of water needed to avoid injury when falling from height is difficult to determine due to the large number of variables. 39 World Aquatics, the governing body for competitive diving, lists a safe plunge pool depth of 5.8 m for diving from a 27 m platform, which can be a proxy for the approximate maximum depth someone can reach following a fall from the Itchen Bridge, given the similar height. 40 Using this logic, given that the depth at the lowest astronomical tide 3.1 m, it is possible that some of the patients made contact with the bottom, especially if they were oriented in a streamlined diving position, fell at or close to low tide, or fell closer to the river bank. It is possible that blunt injury resulting from contact with the riverbed contributed to some of the injuries seen in this study. However, similar studies have found a similarly high incidence of thoracic injuries with much deeper water depth. 12 They concluded that the high incidence of thoracic injuries was due to contact with the surface of the water at speed, which predominately affected the thoracic region due to its greater mass. This is also likely to be true amongst our cohort of patients.
There is a significant amount in the literature on the relationship between body position at the time of impact and the resulting trauma.17,41 Studies on professional cliff divers have demonstrated the significant impact that body position can have when someone falls into water from height. 7 This seems to agree with the previous research that the impact with the water is significant for the presence of specific injuries.
Limitations
This study reasonably describes patterns of and clinical outcomes suffered by patients falling from a medium-sized bridge. However, caution should be taken when interpreting the results, particularly regarding the demographics of those who fell. This study excluded individuals who were deceased before admission, which may significantly impact the data and made it impossible to calculate an overall fatality rate for this mechanism of injury. Additionally, inconsistencies in recording appropriate patients on clinical systems hindered the identification of relevant cases. Furthermore, whilst some of the lower temperatures in the Emergency Department were recorded as being rectal or oesophageal, most temperatures were tympanic or oral, which may skew the readings to be lower than the true core temperatures. Therefore, it is highly likely that this sample may not truly represent the broader population of all people who fell from the Itchen Bridge during the study period.
Conclusion
Thirty patients were identified as having presented to the hospital after falling from Itchen Bridge. Those who fell into water tended to present with a distinct trauma pattern, with high rates of hypothermia alongside thoracic and spinal injuries. A large number of patients had a pneumothorax, and not all of these had overlying rib fractures. The high rates of cardiac arrest and 30-day mortality demonstrate the lethality of this mechanism of injury. Patients who fell onto land were statistically more likely to have an unstable pelvis fracture. Injuries in both these groups present a substantial challenge to pre-hospital clinicians attending these patients. Therefore, an emphasis on early retrieval from the water, early and appropriate rewarming strategies and management of thoracic injuries should be emphasised during the prehospital phase of these patients’ care.
Footnotes
Acknowledgements
The authors would like to thank Stephen Bath for permission to use his photography.
Authors contributors
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: PO is undertaking a partnership PhD with the University of West of England. PO is also the recipient of funding from Perioperative & Critical Care Theme, NIHR Southampton Biomedical Research Centre, Southampton, UKC.
Ethical considerations
This study was granted Health Research Authority approval following a favourable review by South West Central Bristol Research Ethics Committee (REC) (IRAS 341085). HRA and Health and Care Research Wales. IRAS: 341085. Protocol Number: RHM MED 2070. Approval Date: 18.09.2024. The study sponsor was University Hospitals Southampton NHS Foundation Trust. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.