
Abstract
Background
Selective conservative management of asymptomatic patients with small pneumothorax (PTX) in the specific setting of thoracic stab wounds (SWs) remains controversial.
Methods
A prospective study was conducted over a 15-year period on patients with isolated thoracic SWs with small PTX on chest radiograph (CXR) (< 2 cm) and who were asymptomatic. These patients did not undergo tube thoracostomy (TT) but rather active clinical observation at a major trauma centre in South Africa.
Results
Two hundred and eighty-four patients were included (91% male, mean age: 24 yrs). Eight (3%) eventually required TT: three deteriorated clinically and five demonstrated radiological progression of PTX on interval CXR. Of these eight patients who required TT, six (75%) had multiple SWs. All eight patients had uneventful recovery. All other patients who were managed successfully with clinical observation alone were discharged home. No patients represented to the hospital following discharge. There was no morbidity or mortality as a direct result of our selective conservative management approach.
Conclusion
Selective conservative management of patients with asymptomatic small PTX < 2 cm following thoracic SWs appeared to be safe. The vast majority of these patients do not require TT. Active clinical observation alone by an experienced clinician is sufficient.
Introduction
Traumatic pneumothorax (PTX) following penetrating thoracic injury is common and most can be managed adequately by tube thoracostomy (TT) alone.1–5 TT, however, is associated with morbidity and prolonged hospital stay and thus a more conservative approach may be beneficial.5–8 In a specific subset of patients with a small PTX following penetrating thoracic injury and who are asymptomatic, active clinical observation alone has been demonstrated to be safe.9–12 This selective conservative approach was first described by Hegarty et al. at King Edward VIII Hospital in Durban, South Africa. 9 Subsequent studies from the same institution further confirmed the safety of this approach and have formed the basis of our institutional management protocol over the ensuing decades.9–11 Although we have followed this approach at our institution over the last five decades, we have been remiss in continuing to document the inherent safety and applicability of such a strategy. International literature documenting or supporting such an approach remains sparse.4,5,12 This study aimed to address this lacuna in the literature on thoracic trauma by reviewing our experience with the selective conservative management of asymptomatic patients with small PTX following thoracic stab wounds (SWs).
Materials and methods
Clinical setting
This was a prospective study undertaken in the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa over a 15-year period from 1 January 2010 – 31 December 2024. The PMTS provides definitive trauma care for the western part of the KwaZulu-Natal (KZN) province and the city of Pietermaritzburg and is one of the largest academic trauma centres in the province covering a catchment population of over 3 million people. Annual admission exceeds 5000 patients, with over 50% related to penetrating injuries.
Inclusion criteria
All patients with isolated thoracic SWs (i.e. SW confined to the thorax with no other injuries outside of the thorax) who were asymptomatic, with a chest radiograph (CXR) taken in the trauma bay at presentation demonstrating a small PTX were eligible for inclusion. In this study, we define a small PTX radiologically, on an anteroposterior view, taken at inspiration, as less than 2 cm in size, measured vertically from the apex of the lung to the highest point of the copula. Those patients in whom CXR demonstrated haemothorax or haemopneumothorax were excluded. All patients with gunshot wounds (GSWs) were excluded.
Management protocol
All patients who sustained isolated thoracic SWs were initially assessed in the trauma bay in accordance to Advanced Trauma Life Support principles. Those who were symptomatic and / or had immediate clinical indications for TT (e.g. severe respiratory distress, tension PTX, etc.) were managed accordingly without prior CXR at the discretion of the duty trauma staff. All other patients who did not have immediate indications for TT underwent an erect CXR taken at full inspiration. We do not perform routine CT for patients with thoracic SWs. All asymptomatic patients with a PTX < 2 cm on CXR were admitted to our designated trauma ward for active clinical observation. All patients were observed clinically for evidence of clinical deterioration (e.g. respiratory distress, dyspnoea, tachypnoea, desaturation etc.). All patients were encouraged to mobilise. We routinely performed a follow-up CXR at 12 h in these patients in order to determine the need for intervention (TT). Those who demonstrated radiological progression of their PTX on subsequent CXRs, or those who had clinical signs of deterioration were treated immediately with TT, which was inserted using standard open technique at the fifth intercostal space under local anaesthesia. The remaining patients who remained asymptomatic with no CXR evidence of progression (or resolution) were discharged from the hospital at 24 h, with advice to return. All the original CXR images were reviewed by the primary author, with a second reading by the duty radiologist.
The study
Basic demographics, site of injury and subsequent need for TT during the period of clinical observation were reviewed.
Statistical analysis
All data were extracted onto a Microsoft EXCEL© and Stata version 18.5 was used to analyse the data. Association between single or multiple SWs and the need for TT was assessed using Fisher's exact two-sided p-values. Odds ratios and 95% confidence intervals were estimated using univariate logistic regression analysis.
Results
Demographics
During the 15-year study period, a total of 284 patients who sustained isolated thoracic SWs with small PTX were included. Ninety-one per cent (258/284) were male, and the mean age was 24 years.
Injury pattern
Sixty-four per cent of wounds were on the left and the remaining 36% were on the right. 80% sustained single thoracic SWs, while the remaining 20% sustained multiple thoracic SWs.
Clinical outcome
Of the 284 patients who underwent clinical observation, eight (3%) eventually required TT: three patients deteriorated clinically and developed respiratory distress, all of whom underwent TT in the trauma ward immediately during the period of clinical observation. CXR following TT demonstrated partial lung re-expansion. The remaining five patients demonstrated radiological progression of PTX on interval CXR and were subjected to TTs. Of these eight patients who required TT, 75% (6/8) had multiple SWs and the remaining 25% (2/8) were a single SW. The clinical pathway for the 284 patients is summarised in
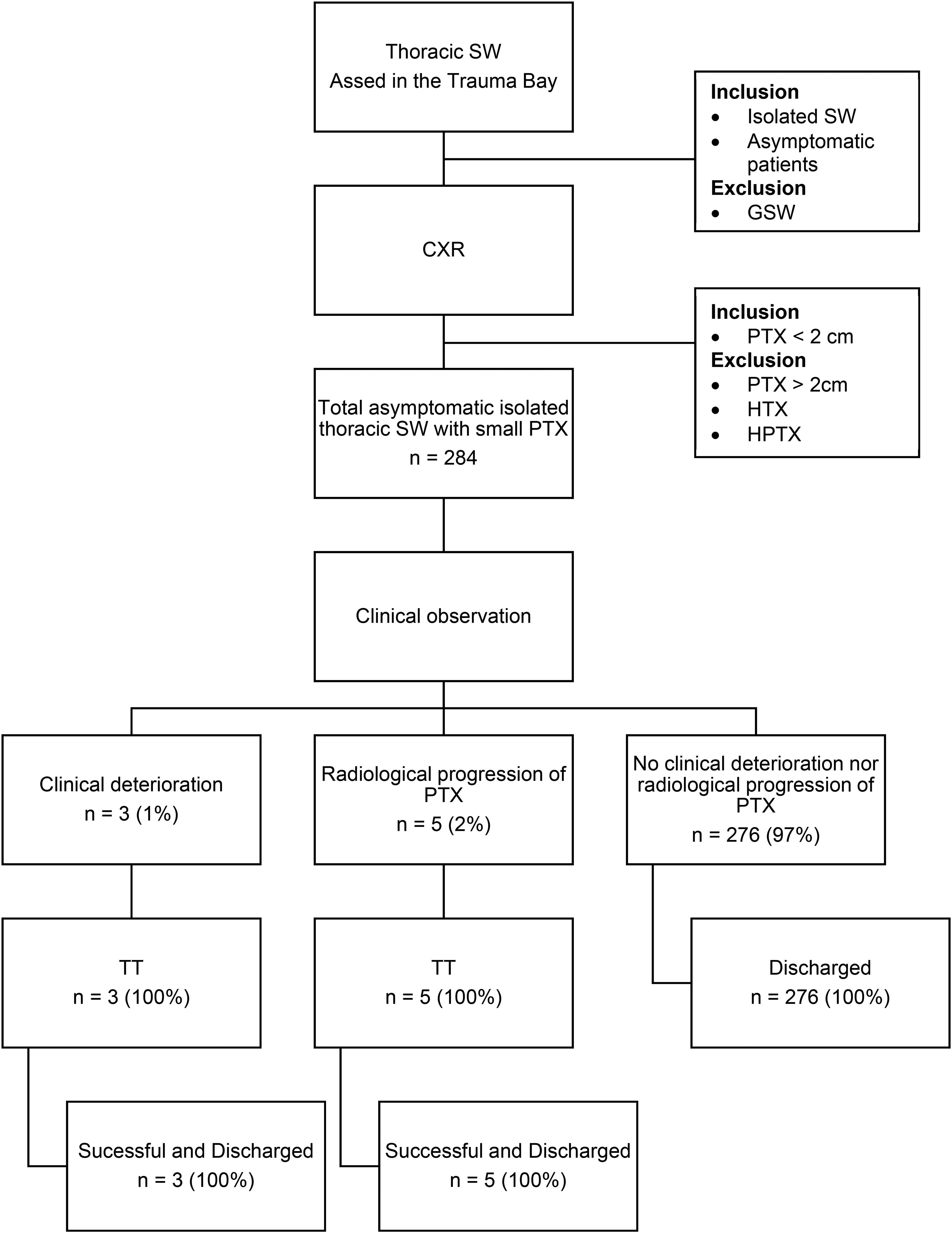
Summary of management of asymptomatic small PTX secondary to thoracic SW.
Discussion
Traumatic PTX is common and has been reported in up to 40% of patients with major thoracic injuries.1,2,13 TT has long been considered the standard management in these patients, and the majority of PTX resolve with TT alone.1,2,13 TT however, is associated with morbidity, with contemporary series reporting an overall complication rate of up to 20%.6–8 The management of penetrating thoracic injury has evolved dramatically over the past four decades, moving away from an aggressive surgical approach to a more conservative one reliant on TT.1–5 Despite the recent advent of so-called minimal invasive techniques to achieve pleural evacuation, such as small-bore percutaneous drains inserted via a Seldinger technique, the primary question remains if intervention is at all required. The philosophy of selective conservatism in the management of penetrating injuries was borne out of necessity in South Africa where the resources available to manage a massive volume of trauma have been perennially insufficient.3,4 This has continued to be our default approach over the preceding half century.
The application of selective conservatism in the management of penetrating thoracic trauma was first practiced at our parent institution, King Edward VIII Hospital in Durban, South Africa.9–11 This experience has continued to form the basis of the contemporary management protocols at our institution. In our current study, 3% of all patients with asymptomatic, small PTX ultimately required TT and was consistent with the previous reports from South Africa. With the increasingly liberal use of CT in centres with less resource constraints, the paradigm of management has once again shifted further, with more recent studies demonstrating that PTX of up to 35 mm (on axial CT images) could be safely managed without TT.14,15 Our study demonstrated that based on CXR alone, these patients could be managed safely, without routine CT. Although CT is available, we have always by necessity adopted a philosophy in selective conservatism due to the overwhelming volume of trauma with resources that are perennially insufficient (e.g. we have at times managed over 200 trauma patients over a 24-h period). Furthermore, chronic staff shortages also added extra pressure on radiological resources. These findings may be applicable for clinicians who practice in a similar resource constrained environment. It should be noted however, that our study focused specifically on the subset of patients with isolated thoracic SWs, which may have contributed to the relatively high success rate of our approach in comparison to studies from other centres. Although the role of selective conservatism should be applicable in selected cases with thoracic GSWs, our experience would suggest that isolated, small PTX are uncommon in this setting. 16
The precise definition of a ‘small pneumothorax’ has remained somewhat controversial. Opinions remain divided in regard to the absolute cut off value and range from 1.5 cm to 3 cm.16–18 Several methods of measurement on CXR have been described in the literature varying from single to multiple parameters and various ratios. 19 The British Thoracic Society (BTS) guideline utilises 2 cm as a cut off for the above definition of small PTX. 17 This is based on the fact that a 2 cm appearance on CXR equates to approximately 50% of PTX by volume. The BTS guideline recommended that the presence of a visible rim of > 2 cm is to be measured from the lung margin to the chest wall at the level of the hilum. 17 On the other hand, the American College of Chest Physicians (ACCP) recommended measurements to be taken from the lung apex to the copula. 18 Based on our experience in management of high volume of thoracic SWs, the vast majority of patients with PTX < 2 cm are seldom symptomatic. 18 We therefore take a pragmatic approach and follow the ACCP definition as it is simple to obtain and easily reproducible.
The management of penetrating thoracic injury has continued to evolve in tandem with rapid advances with technology in diagnostic radiology. The rapid adoption of EFAST in the resuscitation room and the increasingly liberal use of CT have increased the detection of PTX which would otherwise have been missed on CXR. A recent Cochrane review by Chan et al. suggested that EFAST to be superior to CXR in detecting PTX. Furthermore, the notion of occult PTX, which by definition, are absent on CXR are only present on CT have been described. 20 The clinical significance of which in the setting of thoracic SWs in non-ventilated patients appeared to be minimal. Recent evidence has suggested that PTX of up to 35 mm on axial CT images could be managed with clinical observation alone. 14
Our study also demonstrated that a significant proportion of the thoracic SWs were on the left side, which is likely to be related to the right handedness of most assailants. Furthermore, of the eight patients who eventually required TT, 75% of these had sustained multiple SWs. Although it is difficult to prove their association due to the small number of patients in this group, it would appear that those with multiple thoracic SWs who undergo clinical observation may be at higher risk of the need for subsequent TT. These patients with multiple SWs deserve closer care as they appear to need TT at a higher rate.
We recommend clinicians remain extra vigilant when managing this specific group of patients. It would appear that in asymptomatic patients with small PTX secondary to thoracic SW, the vast majority could be managed safely with active clinical observation, provided that they are observed by experienced clinicians within an appropriate facility, and that TT can be performed immediately. A period of clinical observation of 12 h (up to a maximum period of 24 h) appears to be more than sufficient.
One of the limitations of our study is that our management protocol is institution specific. We accept that other centres use different thresholds and definitions of small PTX. Another limitation is that inter-observer agreement was not assessed directly. Our heavy emphasis on clinical assessment and the use of plain CXR reemphasised the resource constraints and pressure in our unique environment. In our study, structured follow-up of patients beyond hospital discharge was not performed and hence the outcomes beyond this point in time are unknown. Without longitudinal data, the possibility of recurrence after discharge may be underestimated. Follow-up of patients in our environment is fraught with challenges primarily due to socioeconomic reasons with historical studies noting attendance rates of well under 50%. Frequently, time lost in attending the hospital leads to fear of loss of earnings and redundancy. Patients who remain well following discharge also seldom see the need to return unless they experience complications. For similar reasons, patients theoretically could have re-presented following to other hospitals, but our experience is that the majority do invariably return to our hospital as this is the only hospital that covers the region.
Conclusions
Selective conservative management of patients with asymptomatic small PTX < 2 cm on CXR following thoracic SWs appeared to be safe. Most of these patients do not require TT. Active clinical observation alone by an experienced clinician is sufficient.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Ethics approval for this study and for the maintenance of trauma registry data was formally endorsed by the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (UKZN) (Reference number: BE 207/09)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.