
Abstract
Background
Selective conservative management of asymptomatic patients with small pneumothorax (PTX) in the specific setting of thoracic stab wounds (SWs) has been demonstrated to be safe. However, the optimal timing in obtaining interval chest radiograph (CXR) remains unknown.
Methods
A prospective study was conducted over a 14-year period on patients with isolated thoracic SWs who were asymptomatic with small PTX on CXR (< 0.5 cm) that underwent active clinical observation at a major trauma centre in South Africa.
Results
Fifty patients were included (87% male, mean age: 24 years). 43 (86%) were male and the mean age was 27 years. All 50 were successfully managed without tube thoracostomy (TT), with no adverse outcome. 35 (70%) had their interval CXR obtained at 12 hours, 7 (14%) at 12–16 hours, 4 (8%) at 16–20 hours and 3 (6%) at 20–24 hours. All patients demonstrated complete resolution of PTX at each of the time intervals and remained asymptomatic.
Conclusion
In patients with asymptomatic small PTX <0.5 cm, interval CXR at 12 hours invariably demonstrates complete resolution. As all patients remained asymptomatic, this may facilitate earlier patient discharge.
Introduction
Pneumothorax (PTX) following a stab wound (SW) of the chest is a potentially life-threatening condition, and tube thoracostomy (TT) has long been the standard treatment for the majority of these patients.1–7 In a well-defined cohort of patients with small PTX, a selective conservative approach may be appropriate.8–12 This highly selected cohort can simply be actively observed. Seminal studies by various authors from King Edward VIII Hospital in Durban, South Africa have supported such an approach.8–10 This approach is reliant on clinical assessment, coupled with interval chest radiograph (CXR), to determine the need for subsequent intervention (i.e., TT) during the period of active clinical observation.8–10 The optimal timing of the interval CXR in this setting however, has never been clarified.8–12 Historically, the practice at our institution has been to obtain an interval CXR at approximately 12 hours following admission. Due to resource and logistical constraints, we commonly experience lengthy delays in obtaining an interval CXR.12,13 These challenges in obtaining an interval CXR may translate into delayed discharge of patients, thereby compounding ongoing issues of hospital ward overcrowding. The aim of this study was to review the timing of interval CXR in a specific subset of patients who were asymptomatic, with a small PTX < 0.5 cm following thoracic SWs that were managed conservatively, and to determine the rate of complete resolution of PTX on CXR at various time intervals. It is hoped that this may allow streamlining our discharge protocols and optimise patient flow in our high volume trauma centre.
Materials and methods
Clinical setting
This prospective study was undertaken in the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa, over a 14-year period from January 2010 to December 2024. The PMTS provides definitive trauma care for the western part of the KwaZulu-Natal (KZN) province and the city of Pietermaritzburg, and is one of the largest academic trauma centres in the province, covering a catchment population of over three million people. Annual admission exceeds 5000, over 50% of which are penetrating injuries.
Inclusion criteria
All patients with isolated thoracic SWs who were asymptomatic, with a CXR taken in the trauma bay at presentation, which demonstrated a small PTX < 0.5 cm were eligible for inclusion. At our institution, we define a small PTX radiologically, on an anteroposterior (AP) view on CXR, taken at maximal inspiration, as less than 2 cm in size, measured vertically from the apex of the lung to the highest point of the copula. In our experience, asymptomatic patients with a PTX < 0.5 cm almost never require TT. This study focuses on those with small PTX < 0.5 cm, as the primary purpose was to review the timing of interval CXR in order to determine the complete resolution rate in these patients. Those patients whose CXR demonstrated haemothorax (HTX) or haemopneumothorax (HPTX) were excluded. All patients with gunshot wounds (GSWs) were excluded.
Management protocol
All patients who sustained an isolated thoracic SW were initially assessed in the trauma bay in accordance with Advanced Trauma Life Support (ATLS) principles. Those who were symptomatic and/or had immediate clinical indications for TT were managed accordingly without prior CXR. All other patients underwent an erect CXR taken at full inspiration. We do not perform routine CT for patients with thoracic SWs. More recently we have begun to make use of chest sonography. We still request a CXR to confirm our sonar findings. All asymptomatic patients were admitted to our designated trauma ward for active clinical observation. All patients were observed clinically by the senior trauma residents for evidence of clinical deterioration. All patients were instructed and encouraged by the trauma ward staff to mobilise. We routinely request an interval CXR at 12 hours. However, the timing of CXR is primarily determined by the workload of the radiographers. Due to the volume of trauma managed at our centre, delay is common. Provided the interval CXR demonstrated complete resolution of PTX, and the patient remained asymptomatic, they were discharged from the hospital at 24 hours, with advice to return.
The study
All patients who underwent clinical observation with a PTX < 0.5 cm were reviewed. The timing from admission to interval CXR was categorised into the following time periods: 12 hours, 12–16 hours, 16–20 hours and 20–24 hours. In this study, we divided the resolution of PTX radiologically as either complete (PTX not visible on interval CXR) or incomplete (PTX remained visible on interval CXR regardless of size). All CXRs were reviewed by the primary author, and by the duty consultant trauma surgeon.
Statistical analysis
All data were extracted onto a Microsoft EXCEL© spreadsheet and imported into SPSS version 27 (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp.) for processing and analysis.
Results
Overview
During the 14-year study period, a total of 50 patients who sustained isolated thoracic SWs with small PTX < 0.5 cm were included: 86% (43/50) were male and the mean age was 27 years; 76% (38/50) of patients had wounds on the left side; 80% (40/50) of patients sustained single SWs and the remaining 20% sustained multiple SWs.
Interval CXR timing
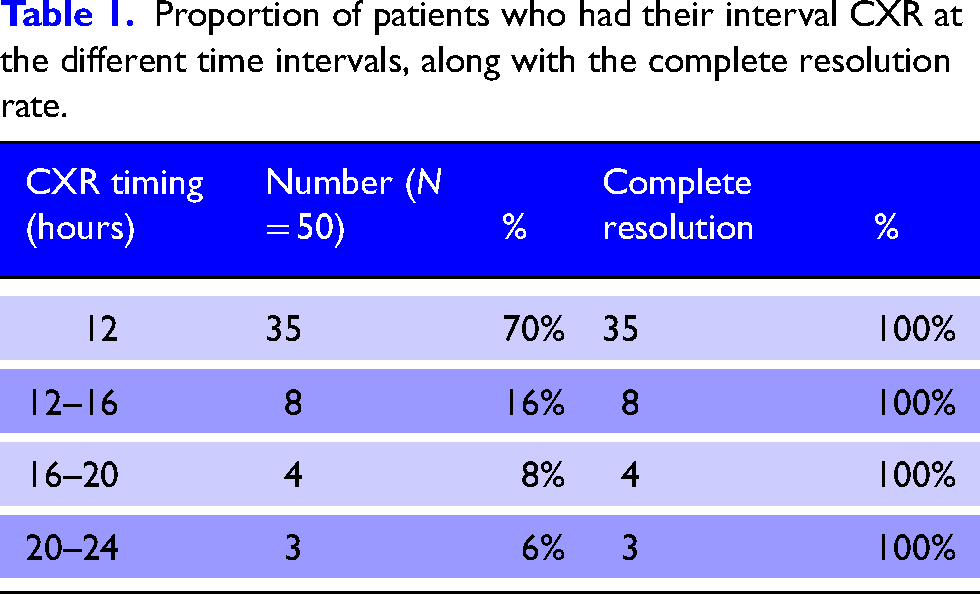
Of the 50 patients, 70% (35/50) had their interval CXR performed at 12 hours. Table 1 summarises the proportion of patients who had their interval CXR at the different time intervals, along with the complete resolution rate.
Proportion of patients who had their interval CXR at the different time intervals, along with the complete resolution rate.
Clinical outcomes
All 50 patients who were observed demonstrated complete resolution of PTX during their hospital stay. None required TTs. There was no morbidity or mortality. All 50 patients were discharged home at 24 hours and no patient represented to our hospital following discharge.
Discussion
Evidence predominantly from high volume trauma centres in South Africa has supported the safety of selective conservative management of small PTXs following SWs of the chest.8–12 Provided the patient remains asymptomatic and interval CXR demonstrates resolution, then the patient can be safely discharged.8–12 Historical studies from our parent institution at King Edward VIII Hospital in Durban, South Africa, have documented the safety of such an approach.8–10 Furthermore, the success rate of conservative management of small PTX appeared to be related to the actual size, and in those between 0.5 and 2 cm (on CXR), the risk of requiring a TT is approximately 3%. 12 What remains unclear however, is the optimal timing of interval CXR. With the ever-increasing pressure on hospital beds and resources in our environment, it is advantageous to reduce delays in interval CXR and facilitate earlier discharge. Our study demonstrated significant variation in the precise timing of interval CXR and that patients, who had their interval CXR as early as 12 hours following admission in fact, demonstrated complete resolution of their PTX. A small subset of patients obtained their interval CXR between 12 and 24 hours. In all these delayed cases, there was also complete resolution on interval CXR.
PTX denotes air within the pleural space and is one of the most common sequelae of a thoracic SW.8–10,14,15 There remains a great deal of confusion over the applicability of evidence in the management of patients with traumatic PTX. Many studies cross reference evidence from the treatment of spontaneous PTX.16–19 Spontaneous PTX cannot be considered analogous to traumatic PTX as their pathophysiology are significantly different.16–18 A point often cited from this heterogeneous evidence is that the rate of resolution of PTX is estimated to be 1.25% to 2.2% of thoracic volume every 24 hours. 18 This evidence was originated from studies on spontaneous PTX and cannot be extrapolated directly to PTX in the setting of thoracic SWs.18,19
One of the major limitations of this study is the lack of randomisation regarding the timing of CXR, as this study was not designed with such methodology. Furthermore, the selective management protocol is specific to our institution and the practice may differ elsewhere. Nevertheless, interval CXR at 12 hours invariably demonstrates complete resolution of PTX < 0.5 cm and waiting up to 24 hours to perform an interval CXR is unnecessary.
Conclusions
In patients with asymptomatic small PTX < 0.5 cm, interval CXR at 12 hours invariably demonstrates complete resolution and waiting up to 24 hours is unnecessary.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethics approval for this study and for the maintenance of trauma registry data was formally endorsed by the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal (UKZN) (Reference number: BE 207/09
Correction (June 2026):
This article has been updated to correct a typesetting error in the Abstract. Within the Methods section of the Abstract “(<mpa#lt; 0.5 cm)” now reads “(<0.5 cm)”.