
Abstract
Background
Damage control laparotomy may be used to manage abdominal trauma. UK damage control laparotomy guidelines are limited and non-specific, suggesting its use may be attributed to a surgeon's experience rather than consistent parameters. This study aimed to determine the incidence of, and factors associated with, damage control laparotomy in adult patients undergoing emergency laparotomy following abdominal trauma, at a major trauma centre (MTC) in the UK.
Methods
A single-centre retrospective cohort study was undertaken, in which the UK Trauma Audit and Research Network (TARN) database was used to select eligible patients who suffered abdominal trauma and underwent an emergency laparotomy within 12 h of arrival to a MTC in the UK, between 01/01/2021 and 31/01/2023. The factors associated with management by damage control laparotomy compared to definitive laparotomy were reported and logistic regression analysis used to investigate associations between age, Glasgow Coma Scale (GCS), injury severity score (ISS), and shock index, metabolic acidosis and requirement for blood products with the outcomes of management by damage control laparotomy and subsequent mortality.
Results
Of the 63 patients eligible for this study, 21% (n = 13) underwent damage control laparotomy with a median age of 25, and 92% (n = 58) were male. The most common mechanism of injury in patients that underwent DCL were road traffic collisions (46%) and stabbings (46%) with mortality at 30 days of 23% (n = 3). Lower GCS and higher ISS were significantly associated with mortality.
Conclusions
A fifth of trauma patients with abdominal injuries had damage control surgery, and this associated with lower GCS. Lower GCS and higher ISS were associated with mortality, this may be due to the presence of systemic shock and critical illness, which are likely contribute to a higher physiological burden and poorer outcome.
Introduction
Emergency trauma laparotomies are used for patients with traumatic abdominal injury who present with peritonitis, uncontrolled haemorrhage, or shock.1,2 Trauma laparotomy may provide access to injured organs within the abdomen and pelvis, including life-threatening bleeding from vessels, for exploratory diagnostic purposes and where imaging may be unavailable or not feasible. Definitive laparotomy is when complete anatomical repair is achieved in a single laparotomy but these operations may be time-consuming and delay the physiological resuscitation of patients and may not be appropriate for patients who have features of the ‘lethal triad’ (coagulopathy, acidosis, and hypothermia), since these patients may need urgent correction of physiology rather than anatomy.3–5
An alternative surgical method is damage control laparotomy, a type of damage control surgery (DCS), where physiological recovery of patients is prioritised over anatomical repair. It consists of an emergency abbreviated primary operation with the purpose of arresting haemorrhage and preventing contamination and a temporary dressing is applied to the wound. Multiple operations may be required over the next few days and weeks, but in the final procedure, definitive abdominal wall closure is achieved.6–8 Appropriate damage control laparotomy reduces mortality compared to definitive laparotomy by facilitating earlier physiological resuscitation,9–11 however, it still carries a notable risk of mortality and morbidity9–11 from potential complications such as wound infection, abscesses, fistulae, sepsis, and multi-organ failure.11–13 Reports also show an increased risk of readmission, number of operations, and reduced quality of life of survivors7,13 and therefore, it is crucial that performance of damage control laparotomy is fully justified.
Regarding UK practice, DCS is referenced in the NICE Major Trauma guidelines 14 and the Clinical Guidelines for Major Incidents and Mass Casualty Events. 15 The NICE guidelines state: ‘Use damage control surgery in patients with haemodynamic instability who are not responding to volume resuscitation’. The major incident guideline recommends DCS for major haemorrhage, blast injuries, vascular, abdominal, and thoracic injuries. These guidelines are vague and lack physiological or anatomical parameters. This implies that they assume the reader to be well-versed in damage control procedures. No guidelines have been identified containing more specific indications for the use of damage control laparotomy. This suggests that current UK practice of damage control laparotomy is dependent on surgeon-experience and knowledge, rather than an agreed upon set of indications.
Consequently, determining the incidence of damage control laparotomy is challenging, as are the factors influencing the decision to perform this technique over definitive laparotomy. This study aimed to determine the incidence of, and factors associated with, damage control laparotomy in adult patients undergoing emergency laparotomy following abdominal trauma, at a major trauma centre (MTC) in the UK.
Methods
Study design and setting
This study was a single-centre retrospective observational cohort study, and has been reported according to the STROBE guidance for observational studies. 16 The study was conducted at an adult (but not paediatric) MTC in the UK (equivalent to US Level 1), servicing a population of 2.9 million people. This study included patients presenting to the service between 01/01/2021 and 31/01/2023 that required emergency laparotomy following trauma. Data were collected from the Major Trauma Service database and institutional approval was granted prior to data collection (Ref: CARMS-21756). Ethical approval was not required for the study as it was a retrospective clinical audit.
Patient selection
A summary of the definitions used to identify patients that have undergone a damage control laparotomy is provided in Online Supplementary Material 1. This study included all adult patients who underwent emergency laparotomy following abdominal trauma at a UK MTC. Eligible patients for this study were identified from the major trauma service (MTS) database, which includes all UK Trauma Audit and research network (TARN) eligible patients, those identified as a code red, pre-hospital trauma alerted patients, and those referred from other wards and networks. 17 TARN eligible patients must have TARN eligible injuries, experience injuries resulting in a hospital stay of >72 h, a critical care admission, specialist transfer, or 30-day mortality. 18
Eligible patients were filtered based on the anatomical location of their injuries using TARN coded abbreviated injury scale (AIS) scores, which are positively correlated with severity. 19 To ensure all abdominal injury patients were included, those with chest and pelvic injuries were also screened to allow for coding errors and injuries spanning adjacent anatomical regions. Patients without an AIS score for chest, abdominal, or pelvic injuries were excluded. Given the high incidence of polytrauma expected in the cohort, this method was preferred over excluding patients with other injuries (such as head, neck, or limb), as this may have inappropriately excluded those with concurrent abdominal and non-abdominal injuries.
Patients were eligible for inclusion to this study if they underwent at least one abdominal surgical operation, the first of which began within 12 h of arrival to hospital. For this study, an operation was defined as a surgical procedure for interventional rather than monitoring purposes and patients were excluded if they did not comply with this definition. Case note review was performed to further refine the cohort to identify those who underwent emergency laparotomy for abdominal trauma. There were no restrictions to patient inclusion regarding age, sex, or survival of injuries.
Data collection
For each patient, data on demographics (age, sex), physiological and biochemical parameters (heart rate (HR), respiratory rate (RR), systolic blood pressure (SBP), lactate, base excess, pH), mechanism of injury (including penetrating or blunt), injury related scores [Glasgow Coma Scale (GCS), Injury Severity Score (ISS)], transfusions (requirement of packed red blood cells and fresh frozen plasma), 30-day mortality and time and number of operations were extracted. Data were collected and analysed from the MTS database between 01/07/24 and 17/07/24. Any data unable to be collected from the database were obtained from electronic hospital records. When required values were missing from this information, the earliest pre-surgery value recorded was used. Data were anonymised and stored on the encrypted hospital computer system.
Outcomes
The outcomes of interest were the management of abdominal trauma by damage control laparotomy and 30 day mortality.
Data analysis
Continuous data were summarised using median and interquartile range (IQR) whilst categorical data were summarised using whole numbers with percentages. The Mann-Whitney U Test was used to compare the distribution of the continuous variables between the damage control laparotomy and definitive laparotomy groups. The Fisher's Exact test was used to measure the association between the categorical variables and the two types of surgery. Neither of these statistical tests adjust for confounders or measure the size or direction of association. Therefore, logistic regression analysis was performed for both outcomes using pre-determined variables. Age, metabolic acidosis, requirement of blood products, shock index, ISS, and GCS were used to assess both outcomes. To investigate the outcome of mortality after damage control laparotomy, these variables were used with the addition of management by damage control laparotomy. Inclusion of these variables in logistic regression was justified as they were expected to be associated with the outcomes. Any variables with very wide confidence intervals were excluded from the model to preserve its stability. Any missing data from independent variables were excluded from logistic regression analysis. Statistical analysis was undertaken using GraphPad Prism V10.3.0 (GraphPad Software, San Diego, USA) and R (R Foundation for Statistical Computing, Vienna, Austria). A p-value of <0.05 was considered statistically significant in all analyses.
Results
Patient selection
A total of 4297 patients were recorded on the database between 01/01/2021 and 31/01/2023. After application of the inclusion criteria, 189 patients were potentially eligible. After case note review, 63 patients complied with all inclusion criteria, having undergone an emergency laparotomy for abdominal trauma over the study period. Of the 63 patients included in the study, 21% (n = 13) underwent damage control laparotomy (Figure 1).
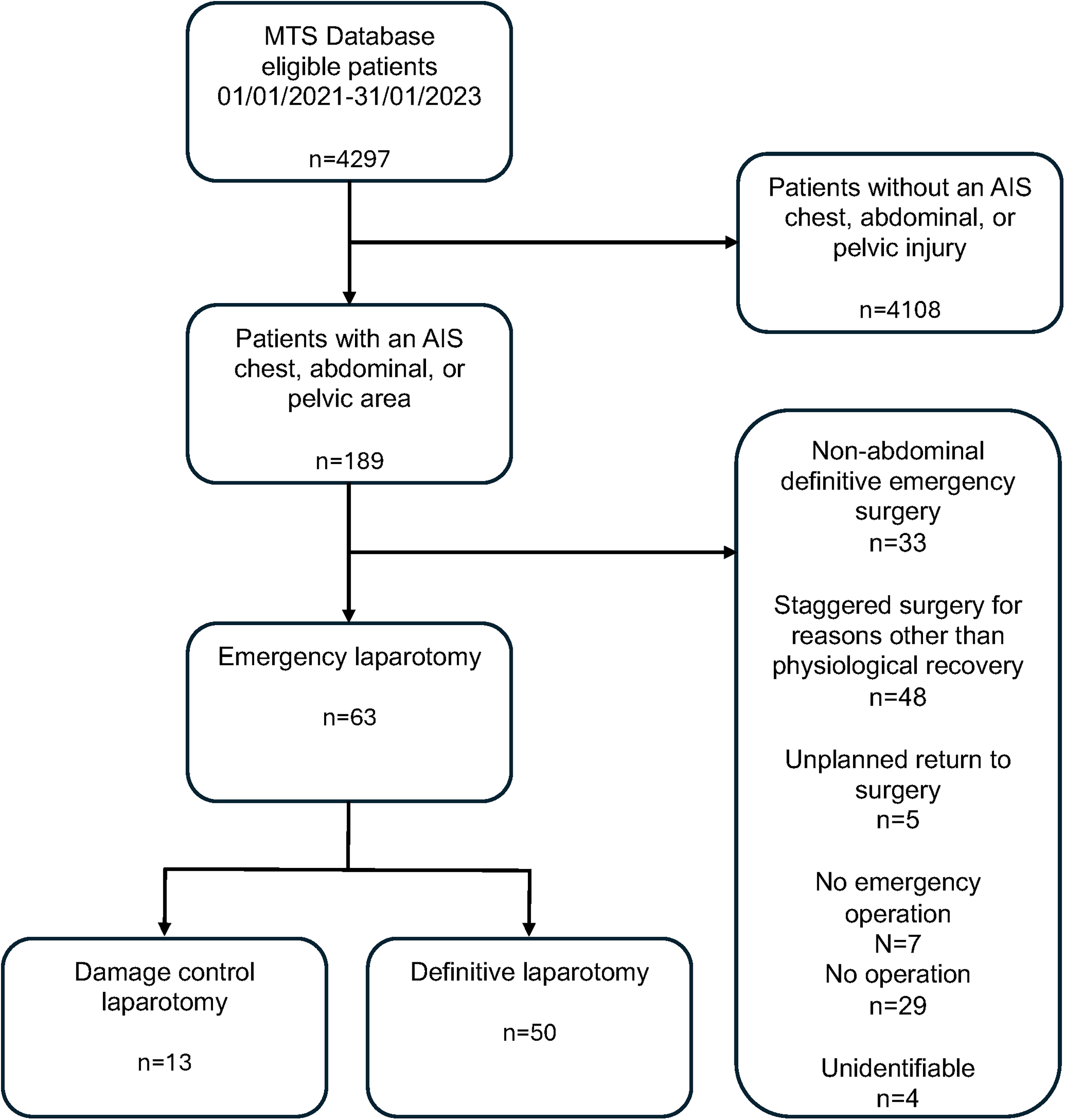
Flowchart of patient selection.
Study patient characteristics
The majority of patients were male in both groups, comprising 92% in the damage control laparotomy group and 82% of the definitive laparotomy group with a median age of 25 and 42 years, respectively. Road traffic collisions (RTCs) were the most common mechanism of injury, with the frequency of stabbings being as high as RTCs in the damage control laparotomy group.
There were no significant differences in HR or RR between the two groups, but damage control laparotomy patients presented with a significantly lower SBP and higher shock index, and a significantly lower GCS than the definitive laparotomy group (Table 1). Lactate, base excess, pH, and acidosis also exhibited significant differences between the two groups (Table 1), with 100% of damage control laparotomy patients requiring transfusion compared to 60% of definitive laparotomy patients.
Study patient characteristics with comparison between management by damage control laparotomy (DCL) and definitive laparotomy (DL). RTC road traffic collision; GCS Glasgow Coma Scale; PRBC packed red blood cells; FFP fresh frozen plasma; ISS injury severity score; ITU intensive therapy unit.
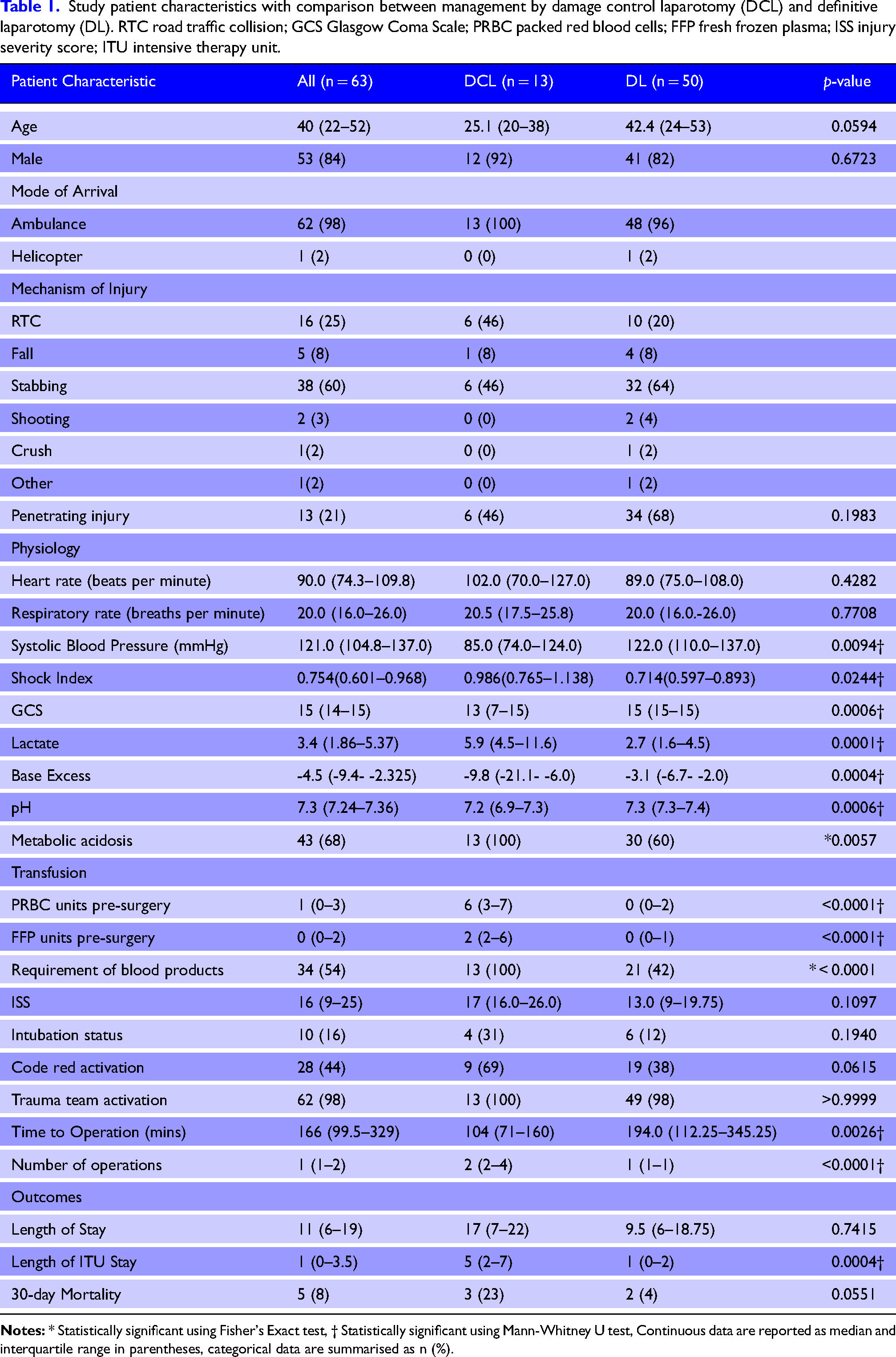
No significant differences were observed in ISS between the patient cohorts, or in intubation status, code red activation, trauma team activation, or length of hospital stay between damage control laparotomy and definitive laparotomy patients (Table 1). Damage control laparotomy patients underwent surgery faster than definitive laparotomy patients, with a significant difference in time to operation between the groups. Damage control laparotomy patients also underwent significantly more procedures than definitive laparotomy patients (median of 2 vs 1, p < 0.0001). No significant difference in mortality between the groups was identified.
Outcomes
Damage control laparotomy
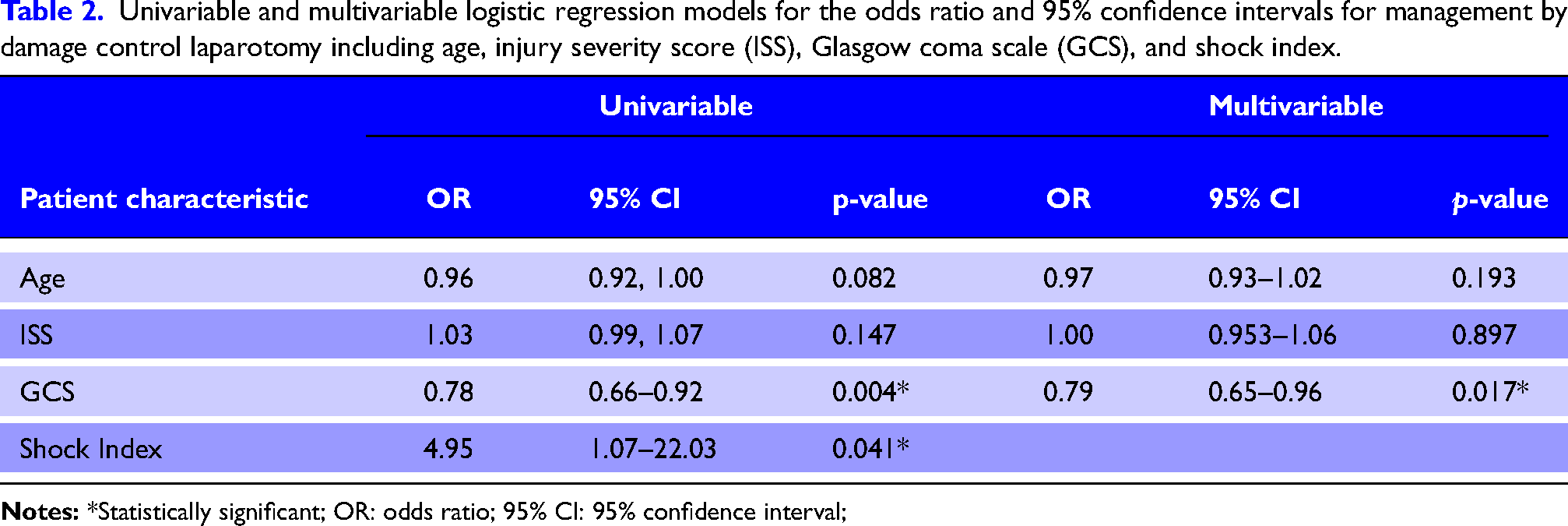
Of the 63 patients who underwent an emergency laparotomy for abdominal trauma, 21% (n = 13) were identified who underwent damage control laparotomy. Univariable logistic regression analysis showed that age and ISS were not significantly different, but GCS was significant (Table 2). The OR of <1 signified that likelihood of management by damage control laparotomy decreased as GCS increased. GCS remained statistically significant after adjustment for other variables included in the model. Shock index (SI) was also significant, however, since SI was associated with wide confidence intervals, this variable was excluded from the multivariate regression analysis. The metabolic acidosis and blood transfusion variables are not presented because the confidence intervals were too wide, rendering the data unreliable.
Univariable and multivariable logistic regression models for the odds ratio and 95% confidence intervals for management by damage control laparotomy including age, injury severity score (ISS), Glasgow coma scale (GCS), and shock index.
Mortality
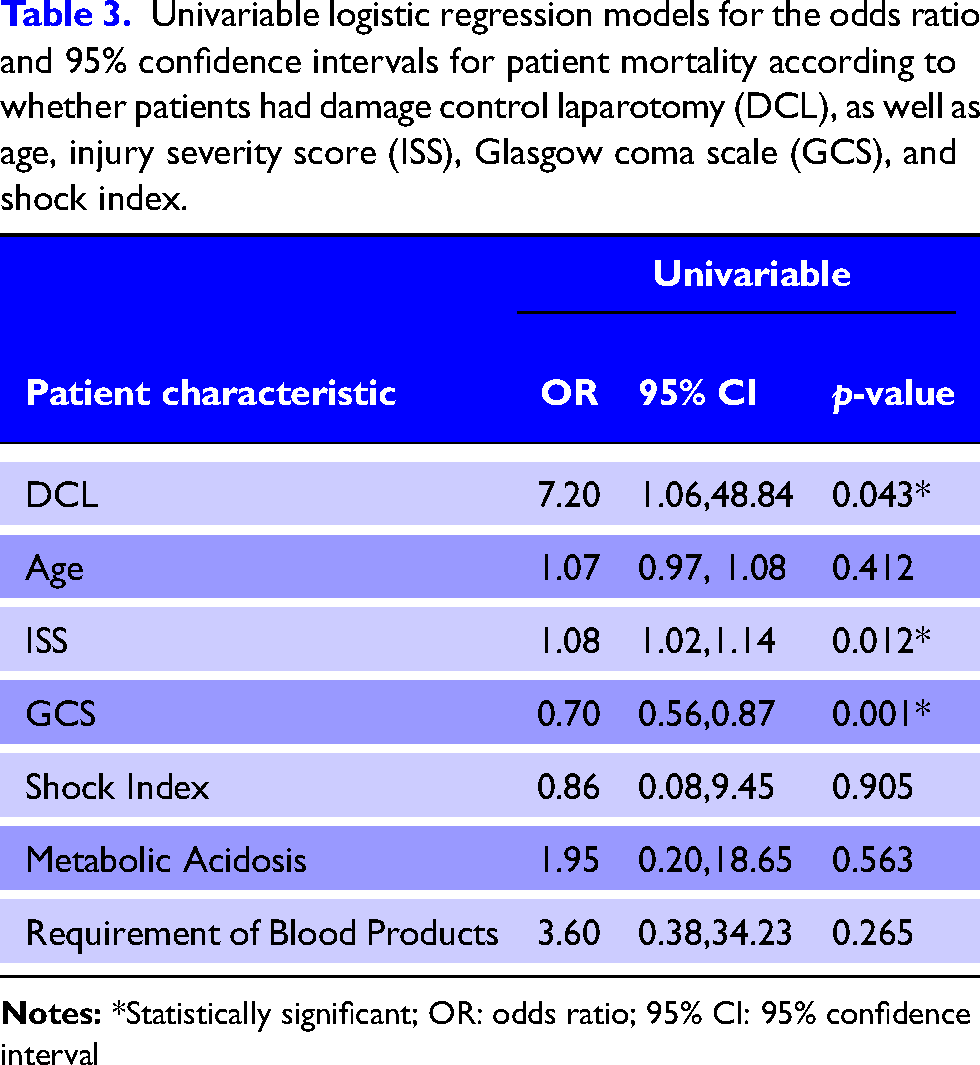
Although damage control laparotomy was significantly associated with mortality in univariable analysis, the wide confidence intervals produced suggested this result was uncertain (Table 3). Higher ISS and lower GCS were also associated with mortality (Table 3). Multivariable analysis could not be undertaken due to low patient numbers.
Univariable logistic regression models for the odds ratio and 95% confidence intervals for patient mortality according to whether patients had damage control laparotomy (DCL), as well as age, injury severity score (ISS), Glasgow coma scale (GCS), and shock index.
Discussion
The primary aim of this study was to identify the incidence of patients who underwent management of abdominal trauma by damage control laparotomy at a large MTC in the UK over a two-year period. Of the 63 patients analysed in this study, 21% of those who underwent an emergency laparotomy for abdominal trauma were found to have undergone damage control laparotomy. This group had 23% (n = 3) mortality at 30 days. The most common mechanisms of injury in patients who underwent damage control laparotomy were RTCs (46%) and stabbings (46%). Lower GCS and higher ISS were significantly associated with mortality. These variables are indicators of potentially more severe brain injury, worse systemic shock and critical illness, which would be expected to contribute to a higher physiological burden, and an increased risk of multi-organ dysfunction and death.
Our study found that 21% of eligible patients underwent a damage control laparotomy, which is consistent with a reported incidence of damage control laparotomy, ranging from 6%-52% in the literature. 14 20–22 However, the percentage of damage control laparotomy patients who experienced penetrating trauma in our study was just 46%, which is lower than the 68.1% to 84% reported in other studies.14,20,23,24 We also observed that 23% of damage control laparotomy patients had an outcome of mortality at 30 days as compared with the reported mortality of damage control laparotomy patients which varies between 8%-66.2%.13,14,20,24,25
Interestingly, our study identified GCS to be significantly associated with management by damage control laparotomy and mortality after damage control laparotomy. This differs from published studies where the predictive abilities of GCS do not seem to be as well explored as variables such as temperature, acidosis, or haemodynamic stability.14,22 It is possible that GCS has been overlooked as it is a measure of neurological function, and not directly descriptive of abdominal injuries. Our findings do align with those of Leonardi et al., 24 who also identified GCS to be significantly associated with mortality after damage control laparotomy. Therefore, we speculate that in the absence of concurrent brain injury, a low GCS may indicate secondary brain injury or shock resulting from abdominal trauma, thereby providing valuable information about the patient's physiology. However, our findings of a low GCS, in general, correlating with mortality is in line with previous studies.26,27
Strengths and limitations
To our knowledge, no other study has investigated the incidence of damage control laparotomy at a MTC in the UK. Our study was conducted at a level 1 MTC in the West Midlands, UK, meaning it is likely to be generalisable to other UK hospitals with dedicated emergency general surgery and trauma services, including a DCS capability. 27 Therefore, this is a unique study which may be used for hypothesis generation and as a comparator for future studies.
A key limitation of this study was the small sample size of 63 patients which prevented the inclusion of some variables in the logistic regression analysis, thus limiting the utility of the results. For example, metabolic acidosis and the requirement of blood products are associated with management by damage control laparotomy 22 but as these variables provided wide confidence intervals in our study, we excluded them to preserve stability of the model. Additionally, a small sample size may have increased the potential for type II errors, preventing the identification of existing associations. Multivariable logistic regression could not be undertaken for mortality as an outcome due to the low numbers.
A further limitation of this study was the inability to measure subjective factors associated with the decision to perform damage control laparotomy, such as ‘clinical gestalt’, 28 which is difficult to quantify or standardize. Body temperature was not considered in this study due to poor recording of temperature in patient notes, resulting in more than 50% of the damage control laparotomy patients not having a temperature measurement on admission. However, it is well established in the literature that hypothermia is a justified indication for damage control laparotomy.20,25
Conclusion
This study demonstrated that damage control laparotomy was performed in 21% of emergency laparotomies for abdominal trauma with our multivariate analysis showing that GCS was the only significant variable associated with management by damage control laparotomy. Mortality was associated with expected variables of worse physiological burden of injury. These findings may help to remind clinicians during surgical decision-making that GCS is an important variable as a marker of worse physiology and potentially worse outcome even for abdominal injuries.
Supplemental Material
sj-docx-1-tra-10.1177_14604086251396430 - Supplemental material for Incidence of and factors associated with damage control laparotomy in adult patients undergoing emergency laparotomy following abdominal trauma: A retrospective cohort study from a UK Major trauma centre
Supplemental material, sj-docx-1-tra-10.1177_14604086251396430 for Incidence of and factors associated with damage control laparotomy in adult patients undergoing emergency laparotomy following abdominal trauma: A retrospective cohort study from a UK Major trauma centre by Charlotte A Needham-Bennett, Zubair Ahmed, Justine J Lee and David N Naumann in Trauma
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.