
Abstract
Introduction
This narrative review explores the findings of randomized controlled trials (RCTs) in terms of timing and the components of ankle rehabilitation.
Method
We reviewed RCTs since 1986 and categorized them by the timing and the components of the intervention. The timing of intervention was classified as immediate, early and delayed ankle rehabilitation. The component of intervention was categorized based on whether ankle motion or weight bearing was assessed individually against “no intervention” or as an additional component compared to the control arm.
Results
A total of 20 RCTs were included. Four evaluated immediate/early ankle motion against immobilization and five assessed the efficacy of immediate/early weight bearing versus delayed weight bearing. Six RCTs assessed the additional benefit of immediate/early ankle motion programs on weight bearing and four evaluated the additional benefit of immediate/early weight bearing on ankle motion programs. One RCT compared combined “early ankle motion and early weight bearing” with delayed rehabilitation.
Conclusion
This review suggests that both ankle motion and weight bearing lead to improved function and faster return to work compared with no intervention. Adding ankle motion to weight bearing programs did not show significant functional benefit, while adding weight bearing to ankle motion programs significantly improved function and lead to earlier return to work. Immediate/early rehabilitation programs appear safe regarding the risk of reduction loss and deep vein thrombosis (DVT) except in syndesmotic fractures. However, they were associated with a higher incidence of superficial wound complications compared with delayed rehabilitation.
Keywords
Introduction
Ankle fractures are the most common lower extremity fractures, occurring at an annual rate of 170–180 per 100,000 persons.1,2 Falls from standing height account for 61% of ankle fractures, followed by sports activity at 22%. 1 Of all ankle fractures, 35% occur in patients over the age of 65 years, with women accounting for two thirds of these fractures. 2 Ankle fractures including uni-malleolar, bimalleolar and trimalleolar fractures with and without syndesmotic diastasis can be managed through different rehabilitation protocols after operation. These protocols vary in timing, ranging from immediate, early (2–3 weeks), to delayed (4–12 weeks) ankle rehabilitation. Rehabilitation may involve weight-bearing exercises alone, ankle motion exercises alone, or a combination of both. 3 It is believed that early rehabilitation programs cause compressive mechanical inputs that facilitate bone union compared to patients with delayed weight bearing.4,5 However, orthopedic surgeons often proceed with caution, favoring delayed rehabilitation programs. A survey of 702 orthopedic surgeons revealed that, on average, a five weeks non-weight bearing period is recommended for young patients with ankle fractures, extending to eight weeks for older patients with comorbidities and trimalleolar fractures. 6
Systematic reviews assessing the efficacy of early ankle motion programs, with high degrees of heterogeneity, suggest no significant differences in functional outcomes or time to return to work compared to delayed ankle motion programs.7–11 In comparison, those reviews with lower heterogeneity suggested that early ankle weight-bearing programs starting immediately or up to 3 weeks post operation, can benefit patients in terms of functional outcomes and earlier time to return to work compared with delayed weight bearing.7,8,10,12 Regarding complications, concerns still exist with both types of early rehabilitation programs as studies included in those reviews were not powered enough in terms of sample size to report complications. Most reviews showed higher rates of wound infection in patients with early ankle motion or early weight bearing programs compared with delayed ankle rehabilitations.9,10 Complications related to loss of reduction and fixation failure were not reported individually in previous reviews. Only one review concluded a higher rate of fixation failures in early ankle motion particularly when combined with early weight bearing, compared with immobilization programs. 9
Previous systematic reviews have pooled findings from studies that were heterogeneous in designs, participants age, methodology and fracture types. Data were pooled from studies with both randomized and non-randomized designs, introducing a risk of bias associated with intention to treat. Additionally, these reviews lacked sub-analyses based on the timing of ankle rehabilitation. For example, studies offering immediate and early ankle motion were grouped as early ankle motion programs ranging from 24 h to 3 weeks after surgery. Furthermore, no attempt was made to elucidate the findings of studies based on the methodology of interventions. For example, studies that compared weight bearing with delayed weight bearing were grouped with studies that assessed the additional benefit of weight bearing component to ankle motion programs. This comprehensive review of randomized controlled trials (RCTs) will detail the findings of studies based on the timing and methodology of rehabilitation programs while providing information about the type of fractures included in those studies.
Literature search method
Primarily, the reference lists of previous systematic reviews were searched for any possible RCTs comparing immediate or early ankle motion or weight bearing interventions with delayed ankle motion or weight bearing. Additionally, a supplementary search was conducted in databases including PubMed and Google scholar with the following keyword: (“ankle surgeries” OR “ankle fractures”) AND (“early mobilization” OR “weightbearing” OR “immediate weight” OR “range of motion” OR “immobilization” OR “ non-weight bearing” OR “weight bearing”).
A comprehensive review of RCTs focusing on rehabilitation programs following ankle surgeries was conducted. The studies were reviewed if they recruited participants with various fracture severity “with or without syndesmotic fractures”, requiring open reduction internal fixation (ORIF) surgical management. We included studies with operative treatment of ankle fractures including Weber A/B/C or uni- bi- and trimalleolar fractures. We excluded studies with non-randomized and retrospective designs and those that followed participants with non-operative management. Additionally, studies that recruited participants with pilon fractures or reported the findings of both operative and non-operative management together were excluded from this review.
The rehabilitation protocols were categorized into 1) immediate ankle motion, 2) early ankle motion, 3) immediate weight bearing, 4) early weight bearing. The timing of rehabilitation was defined “immediate” if the intervention was introduced immediately or before one-week post-operation, “early” if it was introduced between one and three weeks post-operation and “delayed” if the initiation of intervention was more than four weeks post-operation. 3 In each category, we reported the findings of each study in terms of function scores (Patient Reported Outcome Scores), time to return to work, ankle range of motion (ROM) and complication rates.
We also grouped the findings of each study based on the methodology of the intervention and whether the component of intervention was assessed against “no intervention” in the control arm or included as an additional component of the intervention to the control arm. Furthermore, a limited overview of the type of fractures recruited in the studies and quality of reporting was undertaken alongside. The quality of reporting was rated with the Cochrane Risk of Bias tool in domains including selection bias (i.e., random sequence and allocation concealment), detection bias (assessor blinding), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other resources of bias. 13
Results
Overall, 20 RCTs published since 1986 were included in this review. The studies were grouped in three categories. Category 1 comprised 10 studies suggesting ankle motion programs. This included four RCTS compared immediate or early ankle motion with immobilization protocols lasting six weeks14–17 and six RCTs assessed the additional benefits of ankle motion programs on weight bearing.18–23 Category 2 included nine studies suggesting ankle weight bearing programs. This comprised four RCTs compared immediate or early weight bearing with delayed weight bearing15,24–26 and five RCTs assessed the additional benefits of ankle weight bearing on ankle motion programs.27–31 Category 3 consisted of a single study comparing combined early ankle motion and weight bearing versus “delayed ankle motion and weight bearing.” 32 Table 1 summarizes the categorization of studies based on their intervention methodologies. In this table, one study reported the findings across three groups including (a) immediate ankle motion, (b) early weight bearing and (c) delayed WB and immobilization for 6 weeks, therefore this study appeared in both categories 1 and 2. 15
Categorization of studies based on their intervention methodologies.
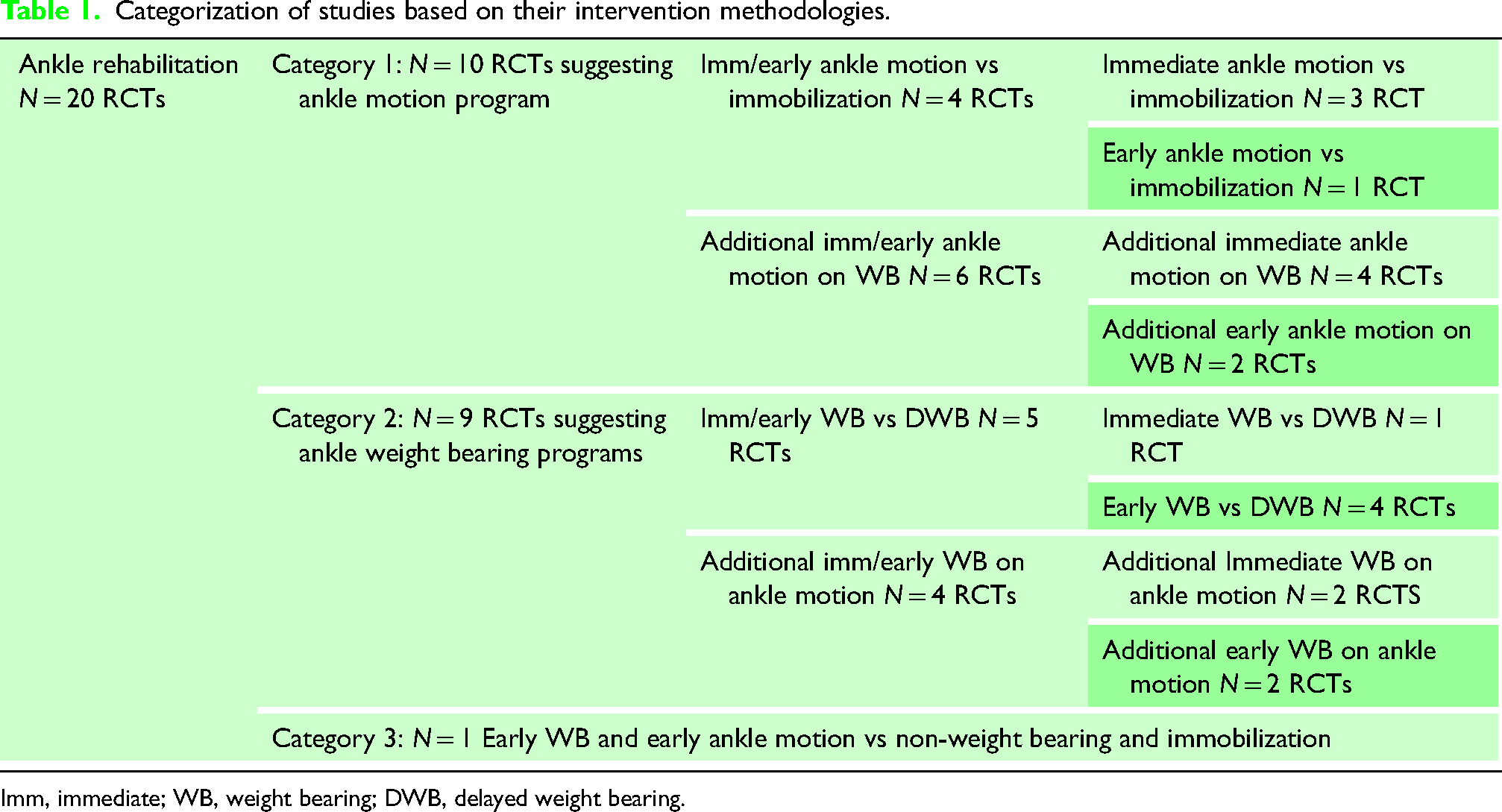
Imm, immediate; WB, weight bearing; DWB, delayed weight bearing.
In the reviewed studies, immediate ankle rehabilitation was offered within 4 days post-operation, early ankle rehabilitation initiated between 1- and 2-weeks post-operation, and delayed ankle rehabilitation introduced at 6 weeks post-operation. Regarding the type of fractures, for studies offering ankle motion programs, Dogra and Rangan 18 and Lehtonen et al. 19 excluded syndesmotic and type C fractures while other studies included all fracture patterns such as Type A-C or uni- bi- and trimalleolar fractures (Online Supplementary Material Table 2). For studies in the “weight bearing” category, Park et al. 31 recruited only patients with uni-and bimalleolar fractures, whereas other studies recruited all fracture types (Online Supplementary Material Table 3).
Efficacy of ankle motion program on function scores and time to return to work
Of the four studies comparing the individual efficacy of immediate/early ankle motion in comparison with immobilization programs,14–17 two with substantial sample sizes of about 60 patients demonstrated ankle motion programs lead to a better short term function and shorter time to return to work compared to immobilization programs.14,17 Egol et al. 14 evaluated the individual efficacy of “immediate ankle motion” while Vioreanu et al. 17 reported the efficacy of early “ankle motion” compared to delayed ankle motion. Conversely, Finsen et al. 15 found no significant difference in time to return to work between immediate and delayed ankle motion program, and Søndenaa et al. 16 did not report these outcome measures. Despite variation in studies power and reporting, it can be concluded that initiating an ankle motion program either immediately or within two weeks postoperatively improves function and time to return to work in comparison with delayed ankle motion.
Six studies assessed the additional efficacy of “immediate or early ankle motion” on weight bearing component.18–23 Among these, three studies demonstrated that ankle motion could offer additional benefits, in terms of function and return to work,20–22 specifically “immediate ankle motion”20,21 and “early ankle motion” 22 programs. However, three other studies did not report significant differences in function or time to return to work from the addition of immediate ankle motion18,19 or early ankle motion on weight bearing component. 23 The inconsistency in findings highlights the need for further investigation to determine whether ankle motion provides added benefits to the weight bearing component. Online Supplementary Material Table 2 provides the characteristics of studies offering ankle motion programs.
Efficacy of “ankle motion program” on ankle range of motion
Eight studies reported the effect of immediate or early ankle motion on ankle ROM. Among these, two studies comparing immediate/early ankle motion versus immobilization programs16,17 and two more with having ankle motion program as an additional component to ankle weight bearing20,23 showed better ankle ROM in the intervention groups compared with the control groups. However, four other studies reported no differences in ankle ROM when comparing “immediate ankle motion with immobilization” 15 or assessing the additional efficacy of ankle motion programs on weight bearing component.18,19,22 Reviewing the quality of reporting of ankle ROM in those studies revealed that studies with blinded assessors and larger sample sizes showed no difference in ankle ROM,18,19 whereas, studies with non-blinded assessors or unclear assessor blinding, or smaller sample sizes resulted in a better ankle ROM in favor of “immediate” or “early ankle motion.”16,17,20,23 Therefore, it is likely that the judgment of the assessor during the measurement was influenced by their knowledge of intervention. Additionally, the accuracy of measurement methods and the unit of measurements needs to be considered as ankle ROM was reported in various forms including degrees of ankle ROM at the injured side, the differences in degrees between injured and uninjured side, the percentage of injured ankle ROM to uninjured side, or ankle impairment severity scale. The efficacy of the early ankle motion on ankle ROM is still unclear and it is highly recommended that future studies report ankle ROM using an accurate tool while the assessor remains blinded to the group allocation.
Efficacy of ankle motion programs on complication rates
Eight studies compared the complication rates between patients undergoing “immediate” or “early ankle motion” and those following immobilization protocols.14,16–19,21–23 Among these, two studies reported a total of seven cases of fixation failures, Lehtonen et al. 19 found one case of fixation failure among 50 patients with Weber A or B or C ankle fractures (excluding syndesmotic diastasis) in the group of patients incorporating “immediate ankle motion with weight bearing” while Tropp and Norlin 23 reported six fixation failures among 15 patients with syndesmotic diastasis in early ankle motion with weight bearing programs. No fixation failures were reported in immobilization groups.
Wound complications were more frequent in groups following “immediate” and “early ankle motion” programs compared to immoblization programs. Out of 213 patients undergoing immediate/early ankle motion, 32 (15%) experienced wound complications compared to 6/209 (2.8%) in immobilization groups.14,16–19,21–23 Among these studies, Lehtonen et al., 19 specifically assessed the additional efficacy of “immediate ankle motion” program on weight bearing, and reported 23/50 cases (16 superficial infection, four deep infection and three dehiscence) in patients with “immediate ankle motion” compared with 4/50 cases of superficial wound infection in the control group . Other studies in this category did not consistently report wound complications as high.
Regarding deep vein thrombosis (DVT), none of patients in “early” or “immediate ankle motion” programs developed DVTs, however, four cases occurred in the patients with immobilization programs.17,19
In summary, “immediate” and/or “early ankle motion” especially when combined with weight bearing in cases with syndesmotic fixation may increase the risk of fixation failures, although further investigation is required due to limited data on syndesmotic fixation in these studies. Patients with immediate and early ankle motion represented with higher rates of wound complication in comparison with immobilization programs especially when motion begins before wound healing. Ankle motion programs may reduce the risk of DVTs.
Efficacy of weight bearing program on function scores and time to return to work
Four studies compared immediate/early ankle weight bearing with delayed weight bearing.15,24–26 One 26 evaluated “immediate weight bearing” versus delayed weight bearing, but did not report on function score and time to return to work. Two studies24,25 found improved function favoring early weight bearing with Van Laarhoven et al. 25 indicating a shorter time to return to work favoring “early weight bearing” while Bretherton et al. 24 found no difference in the time away from work between early and delayed weight bearing programs. Finsen and colleagues 15 did not report function scores but found no difference in time to return to work. Overall, strong evidence suggests that “early weight bearing” improves function which may contribute to a shorter time to return to work. The mixed findings regarding return to work could be due to the diversity in physical job demands among patients. Future studies should consider classifying the time to return to work based on the physical demands of different job types for more tailored insights.
Two studies assessed the added effects of “immediate weight bearing” on ankle motion.27,28 One high-quality study reported better short-term function scores (at 6 weeks), and a 3-week earlier time to return to work for “immediate weight bearing.” 28 However, another with a smaller sample size did not support these findings. 27 In studies examining the efficacy of “early weight bearing” on ankle motion, three29–31 demonstrated significantly improved short-term function scores (from 6 to 12 weeks) compared with “ankle motion program.” Additionally, Park et al. 31 reported 3 weeks earlier return to pre-injury activities in the intervention group compared with the control group. These findings suggest that incorporating weight bearing on ankle motion programs either immediately or early post-operation can improve short-term function scores and quicker return to work than ankle motion programs alone. Further investigation into this is required to solidify our conclusion. Online Supplementary Material Table 3 provides an overview of studies offering ankle weight bearing programs.
Efficacy of “weight bearing program” on ankle range of motion
Five studies examined the effect of early or immediate weight bearing on ankle ROM, each using different measurement tools.15,25–27,29 Three of these compared immediate or early weight bearing with delayed weight bearing and found no significant difference in ankle ROM between groups,15,25,26 although three different measures were used (percentage of loaded dorsi & plantar flexion compared to uninjured side, loss of dorsiflexion compared to uninjured side and the ankle impairment severity scale).
Two studies with small sample sizes assessed the additional benefit of immediate/early weight bearing on the ankle motion program and reported better ankle ROM in the intervention group compared with control groups.27,29 Honigmann et al. 27 reported that patients with “immediate weight bearing” had up to 10° greater ankle plantar flexion and inversion than patients in the delayed weight bearing group, while Ahl et al. 29 reported a significantly better loaded ankle dorsi and plantar flexion, expressed as a percentage of the uninjured ankle, than the non-weight bearing group. Both studies utilized blinded assessors for reporting ankle ROM.
Despite variation in measuring methods, the findings suggest that weight bearing component alone does not result in greater ROM than delayed weight bearing. However, when it is used as an additional component to ankle motion programs, weight bearing is more likely to lead to an improved ankle ROM.
Efficacy of weight bearing program on complication rates
In studies comparing immediate or early weight bearing with delayed weight bearing, fixation failure was reported in 4/571 cases (0.7%) in “immediate or early weight bearing” groups,15,24–31 compared to only one case of fixation failure in 570 patients with delayed weight bearing (0.2%). 24 Wound complications occurred in 35/531 cases (28 superficial wound infections and seven deep infections) (6.6%) in immediate or early weight bearing arms and 26/528 patients (20 superficial and six deep wound infections) (4.9%) with delayed weight bearing arms.24–31 For other complications, four cases of DVTs and one pulmonary embolism were reported in patients with immediate or early weight bearing and six DVTs, and one non-union occurred in delayed weight bearing arms.24,28,30
In summary, although it is clinically believed that weight bearing before bone healing can risk fixation failures, “immediate” and “early weight bearing” appears to pose a low risk of fixation complications compared to that of delayed weight bearing. The risk of wound infection was almost 2% more in patients’ groups with immediate and early weight bearing compared with delayed weight bearing. Overall, the incidence of DVTs was almost equal between the two protocols, making it difficult to associate weight bearing status with the reduced risk of thrombosis.
Efficacy of a combined early ankle motion and weight bearing versus immobilization and non-weight bearing
The combined effect of early ankle motion and weight bearing is still unclear. Some reviews have presented conflicting theories for the combined clinical effect of early ankle motion and early weight bearing. One stated that the combined ankle motion and weight bearing can accelerate the return to work 8 ; however, another showed adding a weight bearing component to ankle motion can lower the functional outcome due to increased risk of fixation failure. 9 Only one high quality study so far has tested the clinical outcome of “combined early ankle motion and weight bearing” against an “immobilization and non-weight bearing” protocol. 32 The findings of that study indicated better short-term (6 weeks) function, greater ankle ROM at 6 weeks, and better physical and mental quality of life at 6- and 12-months post-surgery in favor of the “combined early ankle motion and weight bearing group.” That study also demonstrated no additional complications (wound and implant related complications) associated with early weight bearing and ankle motion intervention. They also showed a lower number of patients in the intervention group were re-operated at 12 months due to hardware irritation compared with the control group (2% vs 19%). 32 Conducting more research in this regard will ultimately clarify the combined effect of early weight bearing and ankle motion and help to design a standardized guideline for treatment.
Discussion
This narrative review did not adhere to the methodologies required for selecting, analyzing and summarizing systematic reviews, such as those recommended by the PRISMA checklist. 33 Instead, we sought to provide a critical overview of existing RCTs in this field. The idea of narrative review was conceived as no systematic reviews to date have analyzed findings of studies based on intervention methodology. We categorized studies according to the following comparisons: (1) weight bearing versus non-weight bearing, (2) weight bearing added to ankle motion programs versus ankle motion alone, (3) ankle motion alone versus immobilization, and 4) ankle motion added to weight bearing versus weight bearing alone. This categorization highlights several key aspects that previous systematic reviews have not addressed. This review is important for identifying future research questions and summarizing the limitations of the past work.
In this review, we included only RCT studies which offer higher statistical power than non-randomized prospective and retrospective review studies. However, these studies indicated limited evidence in terms of the quality of reporting, blinding, and outcome measures consistency. Within the framework of these limitations, we analyzed clinical outcomes based on timing of rehabilitation (immediate and early) and component of the intervention. Generally, immediate or early “ankle motion” and “weight bearing” in post ankle fracture rehabilitations were associated with beneficial effects compared with immobilization or non-weight bearing protocols respectively. Ankle motion program did not show additional benefits when added to weight bearing protocols. However, adding a weight bearing component to ankle motion led to better outcome than ankle motion alone. This review has highlighted the lack of high-powered studies addressing the complication rates across different types of fractures leaving the uncertainty as to whether the reported complications are influenced by fracture types. For example, if weight bearing is safe for patients with syndesmotic fractures as for those without. This may explain why surgeons still prefer traditional rehabilitation programs with delayed weight bearing and immobilization over early rehabilitation programs. 3
Limitations and recommendations
Function, time to return to work, ankle ROM and complication rates were the most common reported outcome measures in studies. However, more consistency in the details of these outcome measures is required. The reviewed studies often had limitations in data presentation which limits the assessment of the clinical significance of the treatment effect. Data in some studies were either presented as categorical variables, graphical format or without measures of dispersion.14–16,21,22,25,27,32 Future studies are highly recommended to provide data as means and SDs in all follow-up time points. It is important that studies clarify the status of returning to work and whether it was with or without walking aids or to report data based on physical demands required in patients’ work. Similarly, it is necessary to accurately collect data on postoperative complications as the details of complications were inconsistently recorded in the studies reviewed. The missing details of complications could be due to (a) the complications not occurring, or (b) not being reported in those studies. Having such a list will encourage more consistency in reporting, helping to understand if there is any association with the type of a post-surgery rehabilitation plan and complication occurrences. It is highly recommended to develop a core outcome measurement set for assessing future ankle studies. The existing diversity has necessitated this narrative review rather than a meta-analysis, as direct comparison between studies was difficult. Consistent outcome measures with similar scales will facilitate pooling of data in meta-analysis to identify the clinical significance of interventions and will help researchers monitor the clinical course of improvement in each intervention. 34
It is required that future studies investigate whether the rehabilitation program starting immediately can make any difference than the rehabilitation programs starting 2 weeks later. A study conducted by Smeeing, Houwert 28 was the only high-quality study that showed immediate weight bearing (24 h post-operation) can create better results in terms of function scores and time to return to work to patients who started weight bearing at 10 days post-operation. Due to limited evidence, systematic reviews often grouped data from “immediate and early ankle motion” or “immediate and early ankle weight bearing” together,7,8,10 thus we still need more knowledge to decide if the intervention initiated immediately after intervention can make differences than the intervention which starts at two weeks later (after wound healing). Additionally, severity of injuries needs to be considered for recruiting participants. The reviewed studies showed a wide diversity of injuries including dislocated lateral malleolar fractures (including type A, B and C in Weber classification),16,17,20,22,23 bimalleolar fractures18,21 and varying degrees of fracture severity (uni/bi/-or trimalleolar fractures).14,15,19,25,27,31,32 Subgrouping of findings based on the type of fractures may help consistent findings.
In terms of risk of bias, the reviewed studies were rated as unclear or high risk of bias in one or more domains. Unblinding of studies in terms of randomization sequence and allocation concealment would risk the unpredicted distribution of participants in groups and bias in effect estimate. 35 Blinding of assessors was rated either unclear or high risk in studies,14–16,20,22,25,27,28,30 therefore they may risk biases for subjective outcome measures such as ankle ROM, muscle atrophy or ankle swelling. Future studies are recommended for blinding of assessors to minimize the bias. Except for a limited number of studies that analyzed in accordance with intention to treat,19,28,31,32 the reviewed studies in this category were unclear in terms of attrition bias and intention to treat analysis. Future studies need to use multiple imputation to deal with the missing data and to report based on intention to treat analysis. 36
Conclusion
The findings of this review can be outlined as bellow;
“Immediate/early ankle motion” can improve function and potentially contribute to quicker return to work in comparison with delayed ankle motion. The additional benefits of “early or immediate ankle motion” on weight bearing component still needs more investigation. Evidence regarding the benefits of ankle motion programs on ankle ROM remains inconsistent. Immediate/early weight bearing whether used individually or incorporated into an ankle motion program, is more likely to result in improved function scores, quicker return to work compared to delayed weight bearing or programs that solely focus on ankle motion. A weight bearing component was shown to benefit ankle ROM if it is combined with ankle motion programs. No study has compared immediate weight bearing with early weight bearing. Except for one study involving patients with syndesmotic fractures, the reviewed studies provided no evidence of reduction loss following immediate or early post-operative ankle weight bearing or motion programs. The incidence of DVT was significantly lower in studies’ arms with early and immediate ankle rehabilitation than delayed rehabilitation programs. The risk of wound complications was higher in studies implementing immediate or early ankle motion programs (15%) compared to a significantly lower incidence in studies involving immediate or early weight-bearing (6.6%).
It is presumed that the temporary harm associated with immediate/early ankle motion or weight bearing approaches significantly fall behind the beneficial effects on function and return to work specifically in studies offering immediate/early weight bearing programs compared with traditional approach. Based on findings presented in this review, the early weight bearing program is strongly recommended to become standard rehabilitation after ankle ORIF surgeries. The studies reviewed in this literature review often recruited participants with various types of ankle fractures including type C and syndesmotic fractures. Therefore, the conventional belief that patients with severe fractures may require more time before weight bearing could be questioned. Further investigation is needed to determine whether immediate/early weight bearing can benefit patients with type C and syndesmotic fractures.
Supplemental Material
sj-docx-1-tra-10.1177_14604086251352075 - Supplemental material for Rehabilitation protocols after ankle surgeries: A narrative literature review
Supplemental material, sj-docx-1-tra-10.1177_14604086251352075 for Rehabilitation protocols after ankle surgeries: A narrative literature review by Zohreh Jafarian Tangrood, Gary Hooper, Jessica Mowbray, Mansur Halai and Andrew Powell in Trauma
Supplemental Material
sj-docx-2-tra-10.1177_14604086251352075 - Supplemental material for Rehabilitation protocols after ankle surgeries: A narrative literature review
Supplemental material, sj-docx-2-tra-10.1177_14604086251352075 for Rehabilitation protocols after ankle surgeries: A narrative literature review by Zohreh Jafarian Tangrood, Gary Hooper, Jessica Mowbray, Mansur Halai and Andrew Powell in Trauma
Footnotes
Contributorship
The idea was conceptualized by Dr AP and Dr JM. ZJT and JM performed the literature search and reviewed abstract and full papers. ZJT wrote the first draft of the manuscript. All authors contributed to the revision of the manuscript. The final version was approved by all authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study as it was a narrative review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The data in this manuscript was collected from reviewing the literature therefore informed consent was not sought for the present study.
Trial registration
Not applicable because this was a literature review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.