
Abstract
Objective
Serum C-reactive protein (CRP), as a reflection of early brain injury at onset, is a prognostic factor in aneurysmal subarachnoid hemorrhage (aSAH). However, in some severe cases, patients exhibit a good prognosis despite their elevated serum CRP level. Therefore, we examined the relationship between serum CRP transitions in the acute phase of aSAH and the prognosis.
Methods
We recruited 63 patients with aSAH and retrospectively analyzed the relationships between the serum CRP transitions during the acute phase and the prognosis, patient background, and clinical course.
Results
Serum CRP values on days 1, 3, and 14 were significantly lower in the good prognosis group than those in the poor prognosis group. Moreover, serum CRP values on days 1 and 14 significantly affected the prognosis in the multiple regression analysis.
Conclusions
A low serum CRP value on day 14, in addition to that on day 1 as reported previously, is associated with a good prognosis of aSAH. Furthermore, a good prognosis of aSAH is determined not only by absence of early brain injury at onset but also by appropriate management to obtain a low serum CRP value on day 14.
Keywords
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is associated with a high mortality rate, and survivors often suffer from severe neurological deficits.1–16 Additionally, early brain injury (EBI) at onset and delayed cerebral ischemia (DCI) have been associated with a poor prognosis.1–10,15–18 Among patients with aSAH, elevation of serum C-reactive protein (CRP), a widely used and nonspecific inflammatory marker, reflects EBI during the acute phase.2–5,8,9,12,15–18 Moreover, serum CRP, as an indicator of inflammatory cytokines that induce vasospasm leading to DCI, is reportedly a prognostic factor for aSAH.1,3–5,7–10,15–19 The acute phase of aSAH includes the cerebral vasospasm phase after the onset of aSAH (day 0), beginning on day 3, passing the peak on days 6 to 8, and fading on days 12 to 14.1,5,10 Elevation of serum CRP during the early phase (days 1–4) of aSAH correlates with the severity and prognosis and reflects EBI.1,4,8,9,12,15,16,18 However, we have sometimes experienced that patients with severe cases of aSAH obtain a good prognosis, despite their highly elevated CRP values, by appropriate disease management, consisting of surgery and postoperative general management in the acute phase. In addition, the relationships between the serum CRP transition during the entire acute phase (days 0–14), including the cerebral vasospasm phase, and the clinical course during this phase as well as the prognosis have rarely been reported.
Therefore, we examined and retrospectively analyzed the relationships between the serum CRP transition and the clinical course during the acute phase and prognosis. Furthermore, we identified the factors affecting this transition.
Methods
Ethics
We conducted this study in accordance with the Helsinki Declaration of 1975 as revised in 2013. 20 This study was a retrospective, single-center, observational study that was reviewed and approved by the ethics committee of the Clinical Examination Support Center of Yokohama City Minato Red Cross Hospital (approval number: 2021-6). The requirement for informed consent was waived because of the retrospective nature of this study. The opt-out method on our official website was used, which was approved by the institutional review board of our facility. The reporting of this study conforms to the STROBE guidelines. 21 All patient details were de-identified in this observational study to protect personal data.
Clinical data assessment
We defined the primary endpoint according to the modified Rankin Scale (mRS) at 90 days after onset and categorized all patients into two groups: the good prognosis group (mRS: 0–2) and the poor prognosis group (mRS: 3–6). We retrospectively evaluated the transition of serum CRP during the acute phase (on days 1, 3, 7, 10, and 14) and compared each group of patients with respect to their basic characteristics (age, sex, aneurysm location, World Federation of Neurosurgical Societies [WFNS] grade, Fisher score, and past history of chronic inflammatory disease such as rheumatoid arthritis); their clinical course during the acute phase; treatment selection of clipping or coiling; DCI identification using magnetic resonance imaging; attenuation of time of flight intensity or stenosis in the main trunk of the cerebral artery; infectious diseases treated with antibiotics; and rehabilitation with respect to the start of ambulatory exercise.
Pre- and postoperative treatment
We selected clipping or coiling for ruptured aneurysms according to the characteristics of each aneurysm and the patient’s general condition via discussion with skilled neurosurgeons and endovascular neurosurgeons. Postoperative patients were managed with the help of intensivists in the intensive care unit or high care unit within the acute phase, and DCI was prevented by administration of fasudil hydrochloride (60 mg/day) and hydration depending on the fluid in–out balance measured every 8 hours during the acute phase.
Statistical analyses
Data are presented as the mean ± standard deviation and were compared using Fisher’s exact test or the chi-square test for categorical variables and the Mann–Whitney U test for continuous variables. Multiple regression analysis was used to evaluate the influence of CRP values on days 1, 3, and 14 on the prognosis and to identify influential factors on day 14.
Statistical significance was set at a p value < 0.05. Data analyses were performed using js-STAR XR+ (1.1.0 j; created by Satoshi Tanaka and Hiroyuki Nakano).
Results
We recruited 74 patients with aSAH between April 2018 and December 2022 who underwent treatment within 24 hours of onset (day 0). Of these, eight patients died during the acute phase of aSAH (up to day 14), and another three had missing clinical data; therefore, data from 63 patients were finally included in the study (Figure 1).
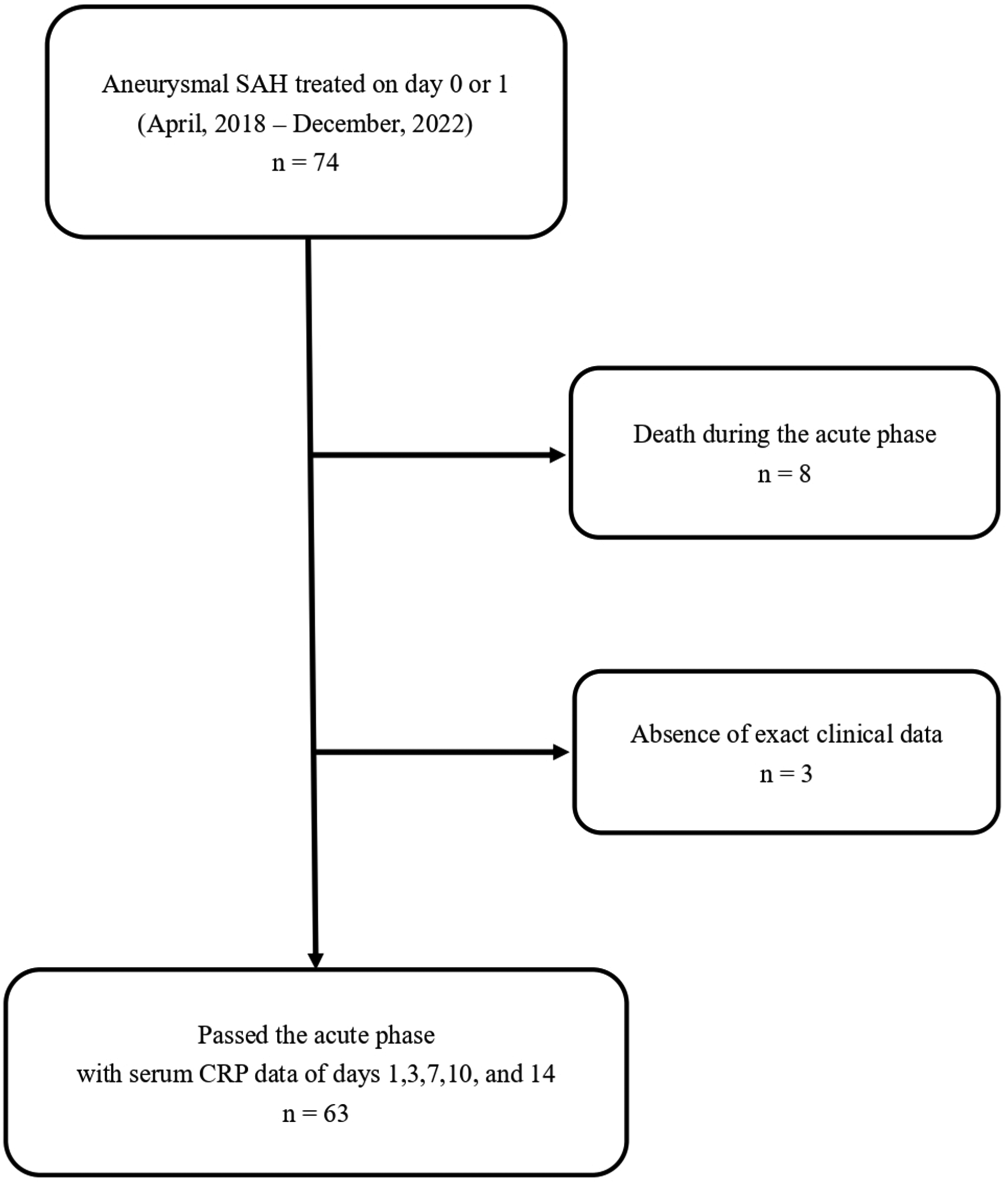
Characteristics of the study sample of 63 patients. Among the 74 patients with aneurysmal SAH who were treated within the 24 hours of onset (day 0 or 1), 11 were excluded because they were inappropriate for the study. SAH: subarachnoid hemorrhage, CRP: C-reactive protein.
Comparison of the prognosis groups
A good prognosis was obtained in 31 of 63 patients (Table 1). The patient age (p < 0.01); WFNS grade (p < 0.05); serum CRP value on day 1 (p < 0.01), day 3 (p < 0.05), and 14 (p < 0.01); prevalence of DCI (p < 0.05); prevalence of infectious disease (p < 0.01); and rehabilitation (p < 0.01) were significantly associated with a good prognosis 90 days after onset. In contrast, no significant association of sex (p = 0.30), aneurysm location, Fisher group, treatment (p = 0.45), chronic inflammatory disease, and serum CRP on day 7 (p = 0.52) and 10 (p = 0.39) was found. Although the serum CRP levels on days 1, 3, and 14 among patients with a good prognosis were significantly lower than those of patients with a poor prognosis, the CRP levels in both groups passed their peaks on day 3 and similarly declined on days 7 through 10 (Figure 2(a)).
Characteristics of patients in different prognosis groups.
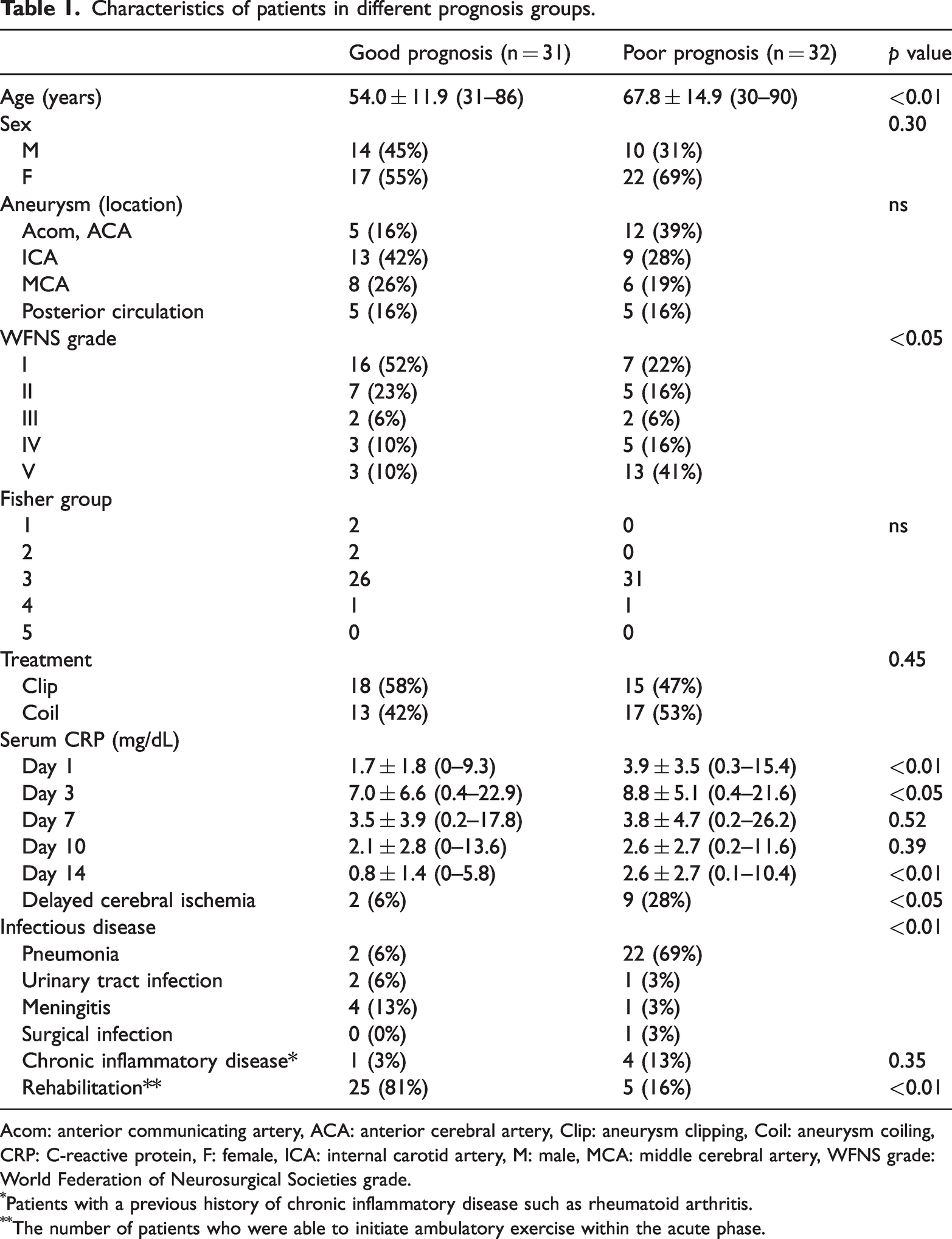
Acom: anterior communicating artery, ACA: anterior cerebral artery, Clip: aneurysm clipping, Coil: aneurysm coiling, CRP: C-reactive protein, F: female, ICA: internal carotid artery, M: male, MCA: middle cerebral artery, WFNS grade: World Federation of Neurosurgical Societies grade.
Patients with a previous history of chronic inflammatory disease such as rheumatoid arthritis.
The number of patients who were able to initiate ambulatory exercise within the acute phase.
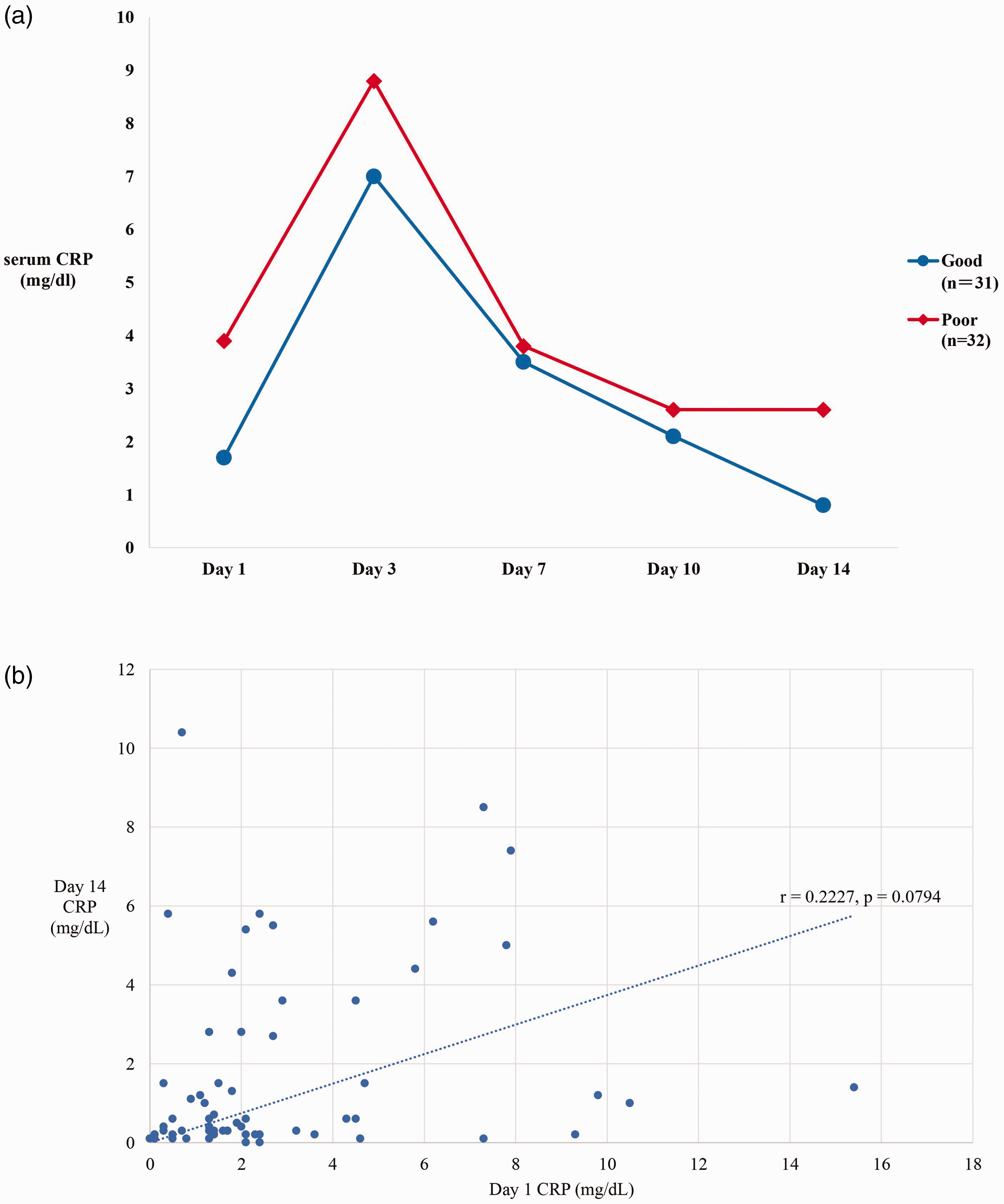
(a) Comparison of serum CRP transition during the acute phase between the good prognosis group (n = 31, mRS 0–2 at 90 days after onset) and the poor prognosis group (n = 32, mRS 3–6 at 90 days after onset). The mean serum CRP values on days 1 and 3 significantly differed between groups but shifted similarly without significant differences between days 7 and 10. However, the value significantly differed again on day 14 and (b) correlation between serum CRP on days 1 and 14. The correlation coefficient was 0.2227, and the p value was 0.0794; no significant correlation was found. CRP: C-reactive protein, mRS: modified Rankin scale, r: correlation coefficient, p: p value.
Influence of serum CRP value on days 1 and 14 on the prognosis
To evaluate whether the serum CRP values on days 1, 3, or 14 (which were significantly correlated with the prognosis in the univariate analysis) affected the prognosis, we used multiple regression analysis, defining the mRS score at 90 days as the objective variable and serum CRP values on days 1, 3, and 14 as the explanatory variables (Table 2). The results showed that serum CRP levels on days 1 and 14 significantly affected the prognosis (β: 0.0545, 0.0716; p = 0.007, 0.013; 95% confidence interval [CI]: 0.0158–0.0931, 0.0159–0.1272). Additionally, the serum CRP values were not correlated with each other (r = 0.2227, p = 0.0794) (Figure 2(b)).
Multiple regression analysis of the prognosis and the serum CRP levels on days 1, 3, and 14.
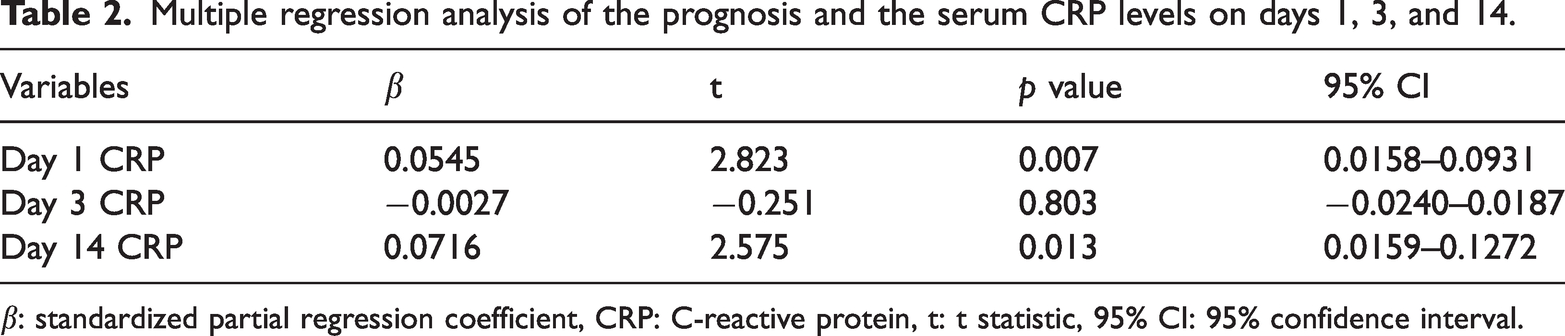
β: standardized partial regression coefficient, CRP: C-reactive protein, t: t statistic, 95% CI: 95% confidence interval.
Patient characteristics and clinical course factors affecting serum CRP levels on day 14
To identify factors that affected the serum CRP values on day 14, which affected the prognosis and were independent of those on day 1, which have been previously reported to reflect EBI, we evaluated the patient characteristics and clinical course (Table 3). Infectious disease (p = 0.0091) and rehabilitation (p = 0.0022) were significantly correlated with serum CRP levels on day 14. In contrast, no significant association with age (p = 0.3043), WFNS grade (p = 0.7597), or treatment (p = 0.52) was found. In contrast, DCI was considered partially correlated with the serum CRP value on day 14 (p = 0.06 [0.05 < p < 0.10]). Next, multiple regression analysis based on those clinical course factors was conducted. The values for each factor considered are listed in Table 4.
Correlations with the serum CRP level on day 14.
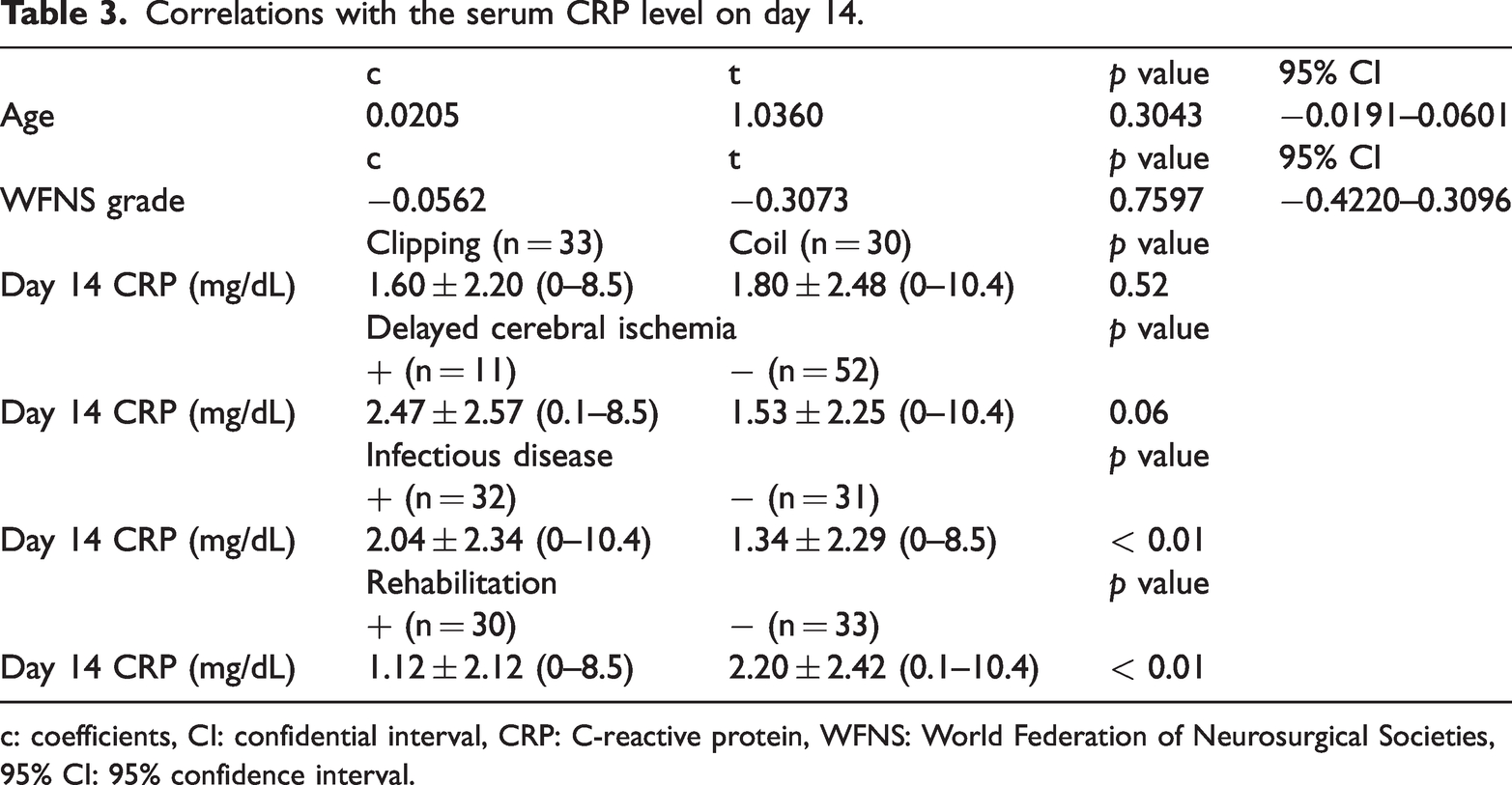
c: coefficients, CI: confidential interval, CRP: C-reactive protein, WFNS: World Federation of Neurosurgical Societies, 95% CI: 95% confidence interval.
Factor values assigned in the multiple regression analysis for serum CRP value on day 14.

Rehabilitation significantly affected the serum CRP value on day 14 (β = −1.5681, t = −2.1521, p = 0.0356, 95% CI: −3.0266–0.1095). However, DCI and infectious disease had no significant effect (β = 0.8023, −0.3744; t = 1.0304, −0.5105; p = 0.3071, 0.6116; 95% CI: −0.7563–2.3610, −1.8423–1.0936, respectively) (Table 5).
Multiple regression analysis of the serum C-reactive protein value on day 14.
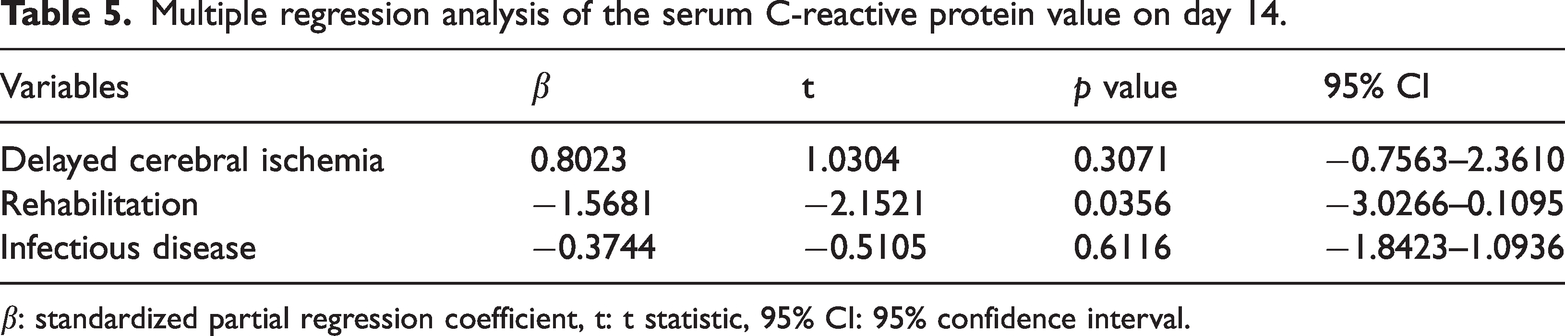
β: standardized partial regression coefficient, t: t statistic, 95% CI: 95% confidence interval.
Discussion
Transition of serum CRP in the hyperacute phase and the entire acute phase as a prognostic factor of aSAH
The serum CRP level, widely used as a nonspecific inflammatory marker, during the acute phase of aSAH has been reported as a prognostic factor that reflects pro-inflammatory cytokines (such as interleukin-6) and the presence of EBI at onset and is associated with cerebral vasospasm leading to DCI.1,3–5,7–9,12,15–19 Therefore, the serum CRP transition during the hyperacute phase has previously been reported to be a prognostic factor for aSAH.4,8,12,15,17,18
In this study, serum CRP values on days 1, 3, and 14 were significantly correlated with aSAH prognosis in the univariate analysis. Moreover, serum CRP values on days 1 and 14 influenced the prognosis and were indicated as possible prognostic factors according to the multivariate analysis. Serum CRP values on day 1, which is devoid of surgical stress, are considered a reflection of EBI solely because they begin to elevate (up to 1000-fold) within a few hours in response to inflammatory stimulation, and following this achieve a peak at 48 hours after the initial stimulation.5,15,17,22 Therefore, the serum CRP level in the hyperacute phase including day 1 is a prognostic factor of aSAH and reflects EBI at onset.3,4,6,9,15,17,18 In contrast, the serum CRP value on day 14 was independent of that on day 1 (Figure 2(b)), which was considered to reflect the clinical course during the early post-hyperacute phase.4,16,18 Additionally, we found that the mean serum CRP values on days 7 and 10 did not differ between the good and poor prognosis groups, but this value was significantly lower in the good prognosis group on day 14 (p < 0.01, Table 1 and Figure 2(a)). In other words, the mean serum CRP value from days 7 to day 14 did not decline in patients with a poor prognosis. Some previous reports have indicated that an increased CRP level between days 8 and 14 is related to unfavorable outcomes among patients with aSAH and induces DCI.15,16 As shown in Table 3 and in this study, DCI was affected by an increased CRP level in the post-hyperacute phase to some extent.
Therefore, we considered that the occurrence of EBI at aSAH onset influenced the prognosis to some extent; however, the total management during the entire acute phase was more important for a good prognosis in aSAH treatment.
Factors among patient characteristics and the clinical course that influenced serum CRP levels on day 14
Early mobilization and rehabilitation are deemed important in the management of the entire acute phase of aSAH.11,14,23–25 Exacerbation of disuse might deteriorate the general condition, leading to perioperative complications such as aspiration pneumonia and urinary tract infection.11,14,23,24 In particular, patients with indwelling ventricular or spinal drainage tend to have restricted mobility and be at risk for meningitis. 26 In this study, rehabilitation influenced the serum CRP level on day 14 in both the univariate and multivariate analyses. Although infectious disease was assessed only in the univariate analysis, related complications seemed to influence the serum CRP level during the entire acute phase of aSAH. However, as previously reported, 16 if appropriate and prompt control via antibiotic administration was achieved, the influence of this factor on serum CRP values seemed to be minor. Moreover, rehabilitation and early mobilization can prevent infectious disease complications.11,14,23,24
Additionally, the severity indicated by the WFNS grade, as a reflection of EBI occurrence, had no significant influence on the serum CRP level on day 14. In other words, even in cases of severe initial damage, early mobilization and rehabilitation by appropriate management (including surgery for ruptured aneurysms as well as postoperative management) may increase the likelihood of a good prognosis with aSAH treatment.
Consistent with previous studies, the patient age was significantly lower in the good prognosis group (p < 0.01). Advanced age is considered a factor associated with a poor prognosis in aSAH cases.11,24,25
The treatment selection was not correlated with the prognosis, as reported previously.3,5,8,9,13 However, in patients with early mobilization and rehabilitation, the incidence of complications such as perforators and branched artery infarctions should be minimized.5,6 Therefore, the selection of surgery (clipping or coiling) should be considered carefully according to the characteristics of each aneurysm.
Limitations of this study
This study was limited by its retrospective single-center design. Therefore, to better characterize the relationship between a good prognosis of aSAH and serum CRP transition during the acute phase, additional considerations, such as a randomized controlled study of patients, including those being administered anti-inflammatory drugs, may be required.
Conclusion
Serum CRP may represent a useful prognostic factor for the appropriate management of the acute phase of aSAH. A good prognosis of patients with aSAH depends on the appropriate surgical treatment of ruptured aneurysms and whether clipping or coil embolization is performed. Additionally, management aiming to achieve a low serum CRP value on day 14 appears to be important. Finally, even if EBI is severe at onset, good general management (including surgery and postoperative management) through the entire acute phase can result in a good prognosis.
Footnotes
Acknowledgements
We thank EditageR for editing a draft of this manuscript.
Author contributions
Writing, editing, data collection, and conceptualization: Fukutaro Ohgaki; Review and editing, supervision: Junya Tatezuki; Review and editing, supervision: Yasunori Takemoto; Review and editing: Kazuki Miyazaki; Review and editing: Yasuhiko Mochimatsu
Declaration of conflicting interest
All authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.