
Abstract
Introduction
Neck of femur (NOF) fractures are a common injury, particularly in older patients. Pre-hospital treatment guidelines are largely absent, and little is known about how Australian paramedics manage this potentially life-threatening injury. This study aims to garner insights on pre-hospital care that may inform paramedic practice, education, and policy for the pre-hospital treatment of suspected NOF fractures.
Methods
A purpose designed anonymous online cross-sectional survey was developed and administered to Australian paramedics using Qualtrics software. Demographic data including education and training, along with confidence, beliefs, and behaviours related to immobilisation techniques, pain management strategies, cognitive assessment tools, and transport decisions were collected.
Results
From 258 completed responses available for analysis an apparent lack of education and training specific to NOF fracture care, and the absence of dedicated guidelines were observed. Respondents lacked confidence in both fracture assessment and management and reported mixed views regarding the perceived importance of key treatment priorities. There was also considerable variability in fracture immobilisation methods, with no clear consensus reached on the best approach. While standard pain management techniques were widely accepted, alternative methods, such as cold therapies showed notable heterogeneity.
Conclusion
The management of NOF fractures by Australian paramedics varies, influenced by differences in clinical confidence, underlying beliefs, and practice behaviours. This highlights the need for clear, evidence-based guidelines and education to standardise paramedic practice. Addressing the gaps in education and protocol development could enhance paramedic confidence, ensure more consistent care, and improve patient outcomes.
Keywords
Introduction
Neck of femur (NOF) fractures, often referred to as hip fractures, are significant and debilitating injuries, particularly among older patients.1,2 The impact of NOF fractures extends beyond the immediate injury, influencing the overall health and quality of life of the affected individuals, with a 26% mortality rate within the first 12 months of injury. 3 Neck of femur fractures are particularly prevalent in the community, where paramedics frequently encounter and manage these injuries. 4 The challenges associated with NOF fractures are further compounded by systemic challenges faced by emergency departments, such as patient ramping, which can significantly delay the delivery of effective care. 5 Patients with suspected NOF fractures are typically older and often experience extended treatment delays due to ramping. Both advanced age and prolonged delays in care are associated with a heightened risk of in-hospital mortality. 5 Optimising pre-hospital care can potentially assist in reducing mortality rates by ensuring that interventions are started promptly, leading to positive patient outcomes even when there are potential treatment delays. 6
Despite the critical nature of this injury, a gap exists in understanding how paramedics manage patients with a suspected NOF fracture, including their confidence and preparedness in making decisions about patient assessment and treatment, and the factors that influence these decisions. A recent review of publicly available Australian and New Zealand ambulance service guidelines failed to identify a standalone treatment protocol or clinical practice guideline (CPG) for the pre-hospital management of a suspected NOF fracture 7 ; which raises the questions: how do paramedics determine the appropriate approach to managing this injury? How confident are paramedics in delivering this care? Which aspects of care do they prioritise? And what practices are currently employed?
Utilising a cross-sectional study design, the aim of this study was to explore the practices and protocols employed by Australian paramedics in the pre-hospital assessment and management of NOF fractures, focusing on their training, education, perceived confidence, preparedness, and perspectives on key treatment aspects. A secondary aim was to examine their knowledge and application of guidelines, as well as their current and future training needs specific to NOF fractures. The insights gained from this investigation are crucial for enhancing patient outcomes, especially when faced with potential factors such as ramping, and may also serve as valuable input for future guideline development for this condition.
Methods
Survey design
In the absence of any previously published study examining paramedics treatment of NOF fractures, a purpose designed online cross-sectional survey was developed and administered using Qualtrics software. 8 Survey questions were developed based on a review of the relevant literature, and discussion with the research team, with additional input sought from industry paramedics and peers. The survey comprised 34 questions organised into four primary categories: (1) demographics, (2) education and training, (3) assessment, and (4) treatment. To allow for a structured examination of the data, question based around assessment and treatment were examined using the three domains: confidence, belief and, behaviour (Figure 1). The complete survey is available as Online Supplementary Material 1.
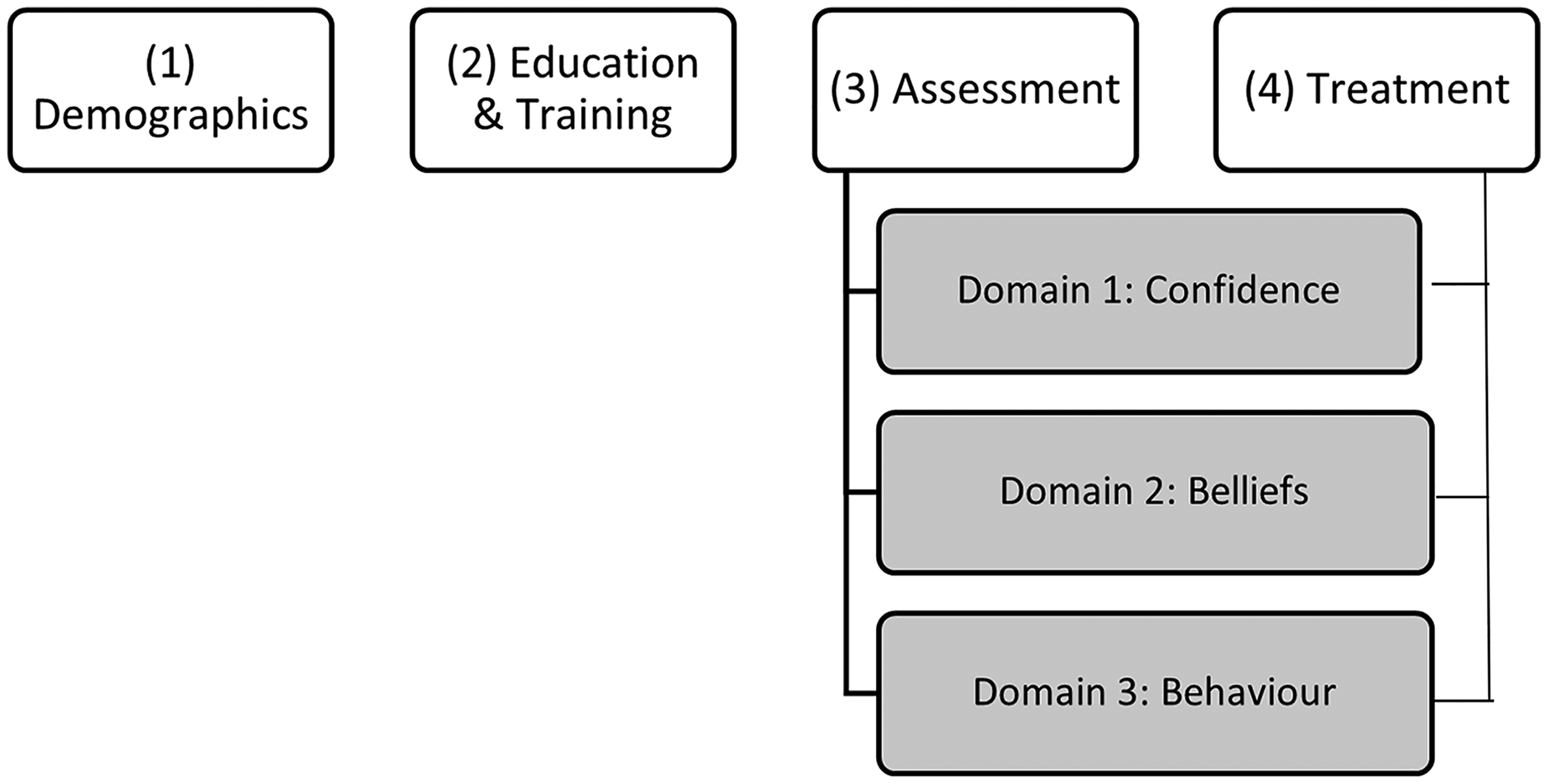
Overview of the survey structure, which includes 34 questions divided into four main categories: demographics, education and training, assessment, and treatment. Questions related to assessment and treatment were further analysed across three domains: confidence, belief, and behaviour.
A 4-point Likert scale was used for a total of eleven questions. Although a 4-point scale eliminates the opportunity for a neutral response, it also reduces ambivalence by encouraging respondents to take a definitive stance. 9 To assess confidence, Likert scale response options were ‘very confident’, ‘confident’, ‘somewhat confident’ and ‘not confident’. For evaluating beliefs, the response options were ‘very important’, ‘important’, ‘somewhat important’ and ‘not at all important’. Lastly to measure behaviour, response options were ‘always’, ‘often’, ‘sometimes’ and ‘never’. Only surveys with 100% completion were included in the analysis to avoid missing data.
Prior to release, the survey was piloted by ten Australian paramedics. Feedback validated the estimated completion time, confirmed the accurate functioning of survey logic, and ensured that the questions were relevant and easily understood. Following piloting, minor amendments to the wording of several questions were undertaken prior to release. This included adding another response for the question regarding factors impacting the ability to transport directly to a hospital that has orthopaedic surgical capabilities: “There are hospitals in my area that have orthopaedic surgical capabilities; however, organisation policy states that I must transfer to the closest hospital.” Data from survey piloting were not included in the data set for analysis.
Participants and recruitment
Participants were recruited using professional association approved direct mailouts (e.g., Australasian Paramedic Association), social media posts (e.g., Facebook), and personal networks (e.g., email). Sample size calculations for population surveys using a 95% confidence interval and a 5% margin of error, indicate an ideal sample size of 378 respondents. Eligibility questions at the commencement of the survey confirmed respondents self-identified as an Australian registered paramedic and had attended at least one suspected NOF fracture in the preceding 12 months. To improve response rates, respondents were provided with an opportunity to enter a random prize draw for one of three AUD100 vouchers upon submission of survey responses. To preserve anonymity, personal details were collected in a separate survey, linked to the main survey. To minimise non-human responses a CAPTCHA verification was included at the start of the survey. 10 The survey also included check questions, that were not used in the analysis, which required a specific response to help identify non-human respondents.
The study adhered to ethical guidelines and approval was obtained through the Institutional Human Research Ethics Committee Central Queensland University (Approval #: 0000024239). An online participant information sheet was provided on the landing page of the survey and informed consent was confirmed via participants selecting a checkbox response prior to commencing the survey.
Data analysis
Since this is an exploratory study, quantitative data were analysed using descriptive statistics, including means, standard deviations, and frequencies to provide an overview of the data.
Results
Survey responses
A total of 365 respondents attempted the survey and of these 107 were excluded from analysis (n = 3 did not provide consent; n = 19 did not meet the eligibility criteria; and n = 85 were incomplete) resulting in a final sample of 258 completed surveys for analysis. Given the broad recruitment strategy involving the use of social media, organisation distribution channels, and targeted emails, coupled with the eligibility criteria of being a registered paramedic having attended at least one suspected NOF fracture in the previous 12 months, it is not possible to determine the population size and subsequently the proportional response rate. However, according to the Paramedicine Board of Australia's Registrant data for 2023 there were 23,686 general registered paramedics in Australia. 11
Demographics
Respondent demographics are presented in Table 1. There was an even distribution of both male and female respondents, with a broad range of age and experience. Most respondents were in full time employment (n = 221, 86%) and were employed with state ambulance service provider (n = 254, 98%). Just over half of the respondents (n = 133, 52%) reported working in a non-metropolitan location and 69% (n = 178) had a Master's degree or higher.
Respondent (n = 258) demographics.
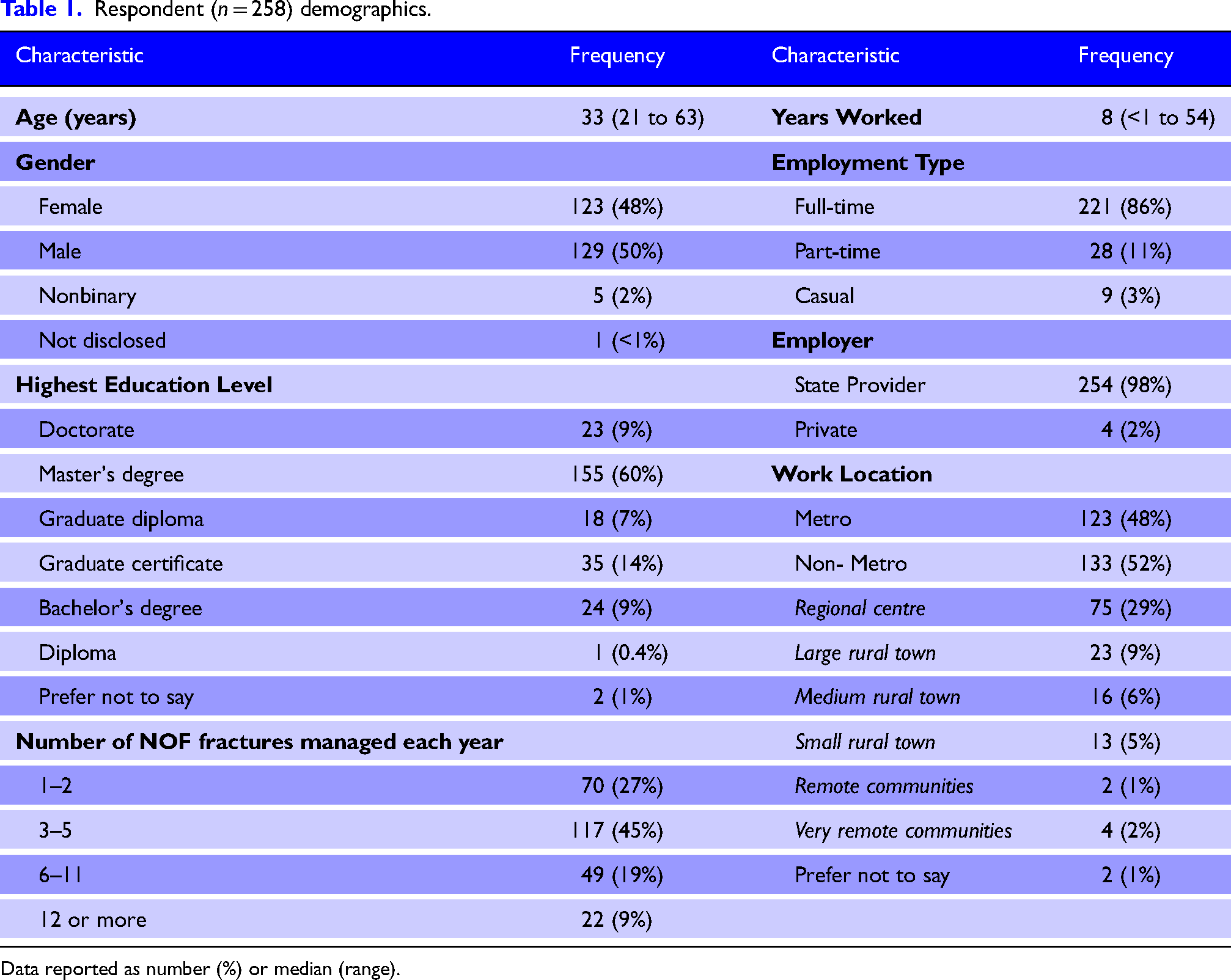
Data reported as number (%) or median (range).
Education and training
Specific neck of femur fracture guideline
Seventy one percent (n = 183/258) of respondents stated they do not refer to a specific CPG or policy when treating someone with a suspected NOF fracture.
Specific neck of femur fracture education and training
Less than one-quarter (24% n = 63/258) reported receiving specific education and training for treating patients with a NOF fracture. Of those who received training, most reported this to be delivered via workplace training days, hands on practice (learning from others on the job), and university courses (Figure 2). When asked to state which education source they found the most helpful and/or informative, hands-on practice (learning from others on the job) was the most common response (35% n = 22/63) followed by workplace training days (27% n = 17/63).
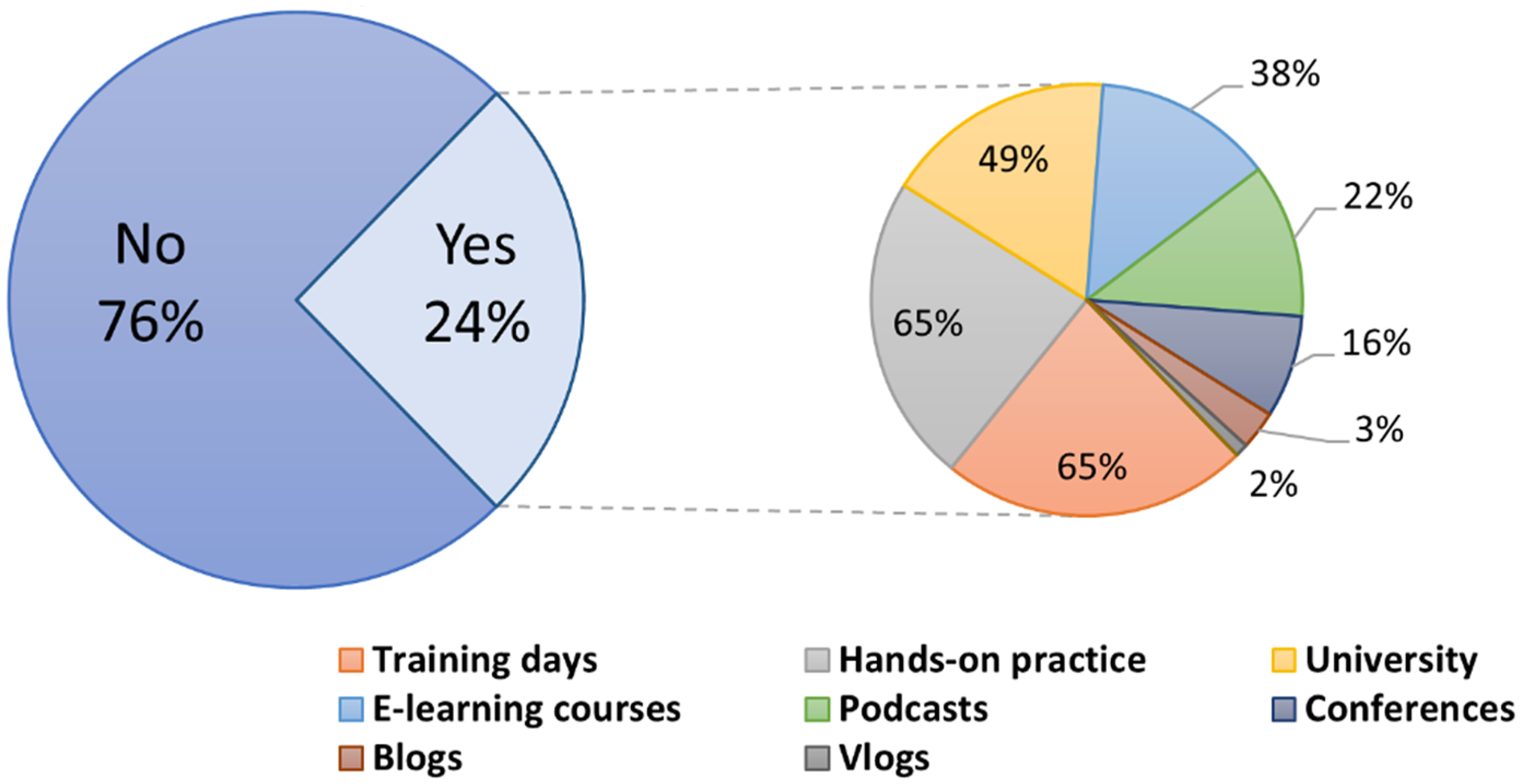
Pie-in-pie chart illustrating the sources of specific NOF management education. The main pie chart shows the proportion of respondents who have received specific education versus those who have not. For those who have received education, the secondary pie chart details the various sources of this education, including workplace training days, hands-on practice (learning from others on the job), and university courses.
Confidence
Confidence in aspects of NOF fracture management
Respondents identified obtaining a patient history and managing pain as the areas in which they report the highest level of confidence with 61% (n = 158/258) and 54% (n = 139/258) respectively reporting ‘very confident’ (Figure 3). Conversely, fracture assessment and care were the areas in which the respondents reported the lowest level of confidence with 26% (n = 66/258) and 24% (n = 63/258) reporting either ‘somewhat’ or ‘not confident’ respectively. When asked what factors cause doubt when managing a patient with a NOF fracture, the absence of a specific guideline was identified as the most common factor (44% n = 128/294). In contrast, independent research was identified as the most popular method to find appropriate information for treating a patient with a NOF fracture to improve knowledge (24% n = 179/745). The full list can be found in Table 2.
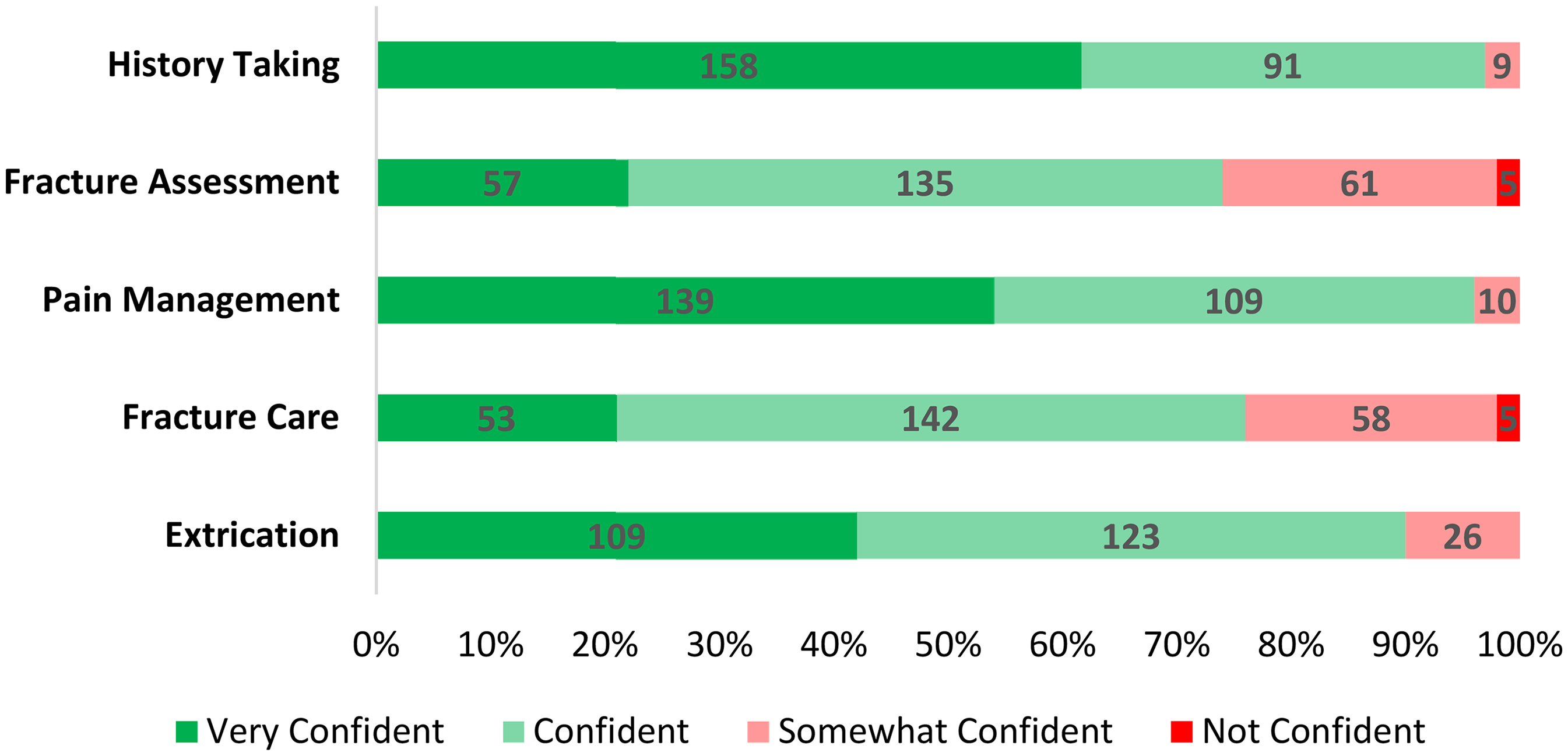
Confidence levels in various aspects of NOF fracture management among respondents.
Reported elements that cause a lack of confidence and sources used to find appropriate information to improve knowledge.
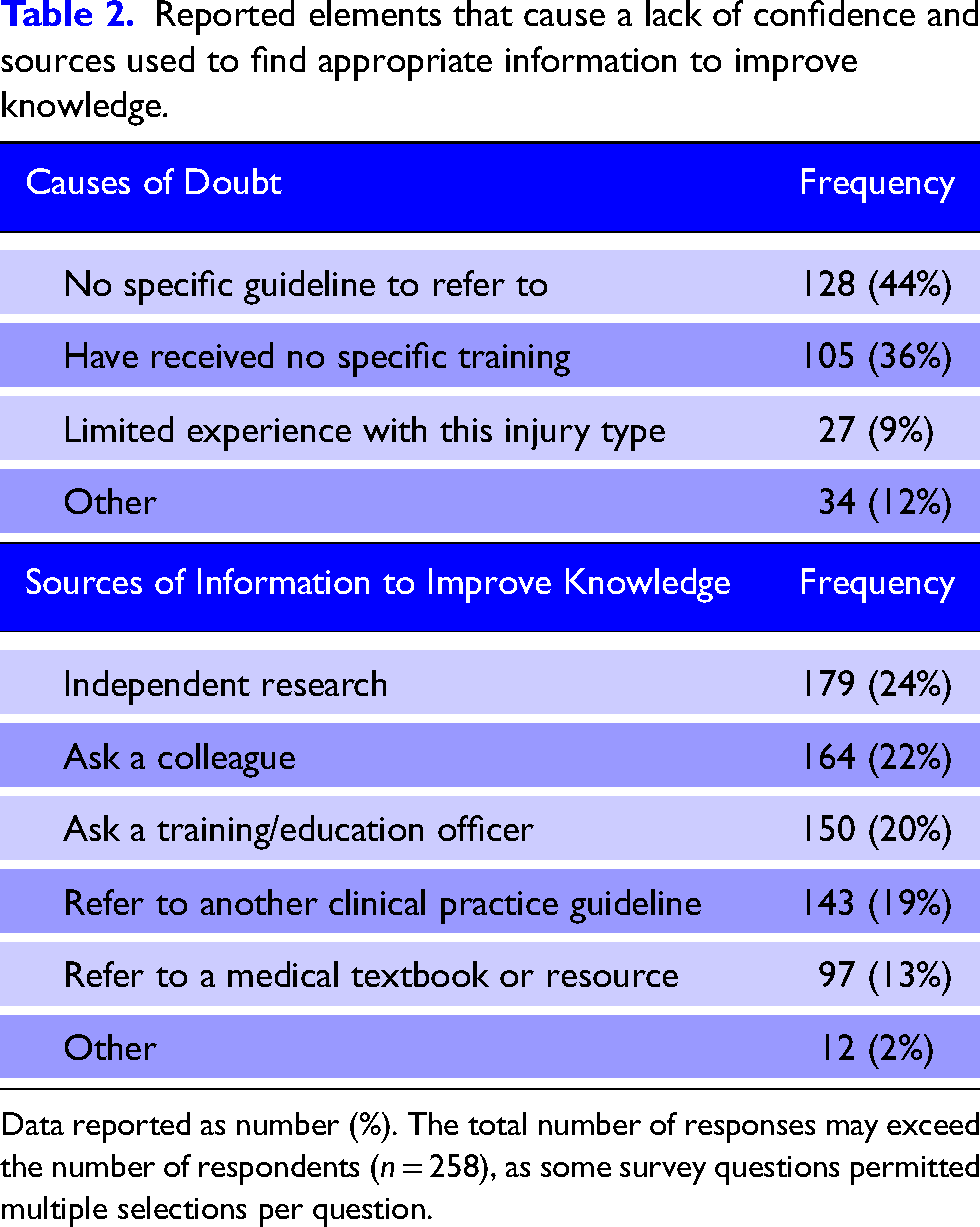
Data reported as number (%). The total number of responses may exceed the number of respondents (n = 258), as some survey questions permitted multiple selections per question.
Beliefs
Importance of risk factors when making a provisional diagnosis of a NOF fracture
Low bone mineral density (BMD) due to osteoporosis or osteopenia (78%, n = 200/258), frailty status (71%, n = 184/258), and patient age (63%, n = 163/258) were rated as most important risk factors to assist with diagnosis of a NOF fracture (Figure 4(a)). Conversely, current tobacco smoker (23% n = 60/258), sex (16%, n = 41/258), and poor vision (8%, n = 20/258) were rated as being of lowest importance.
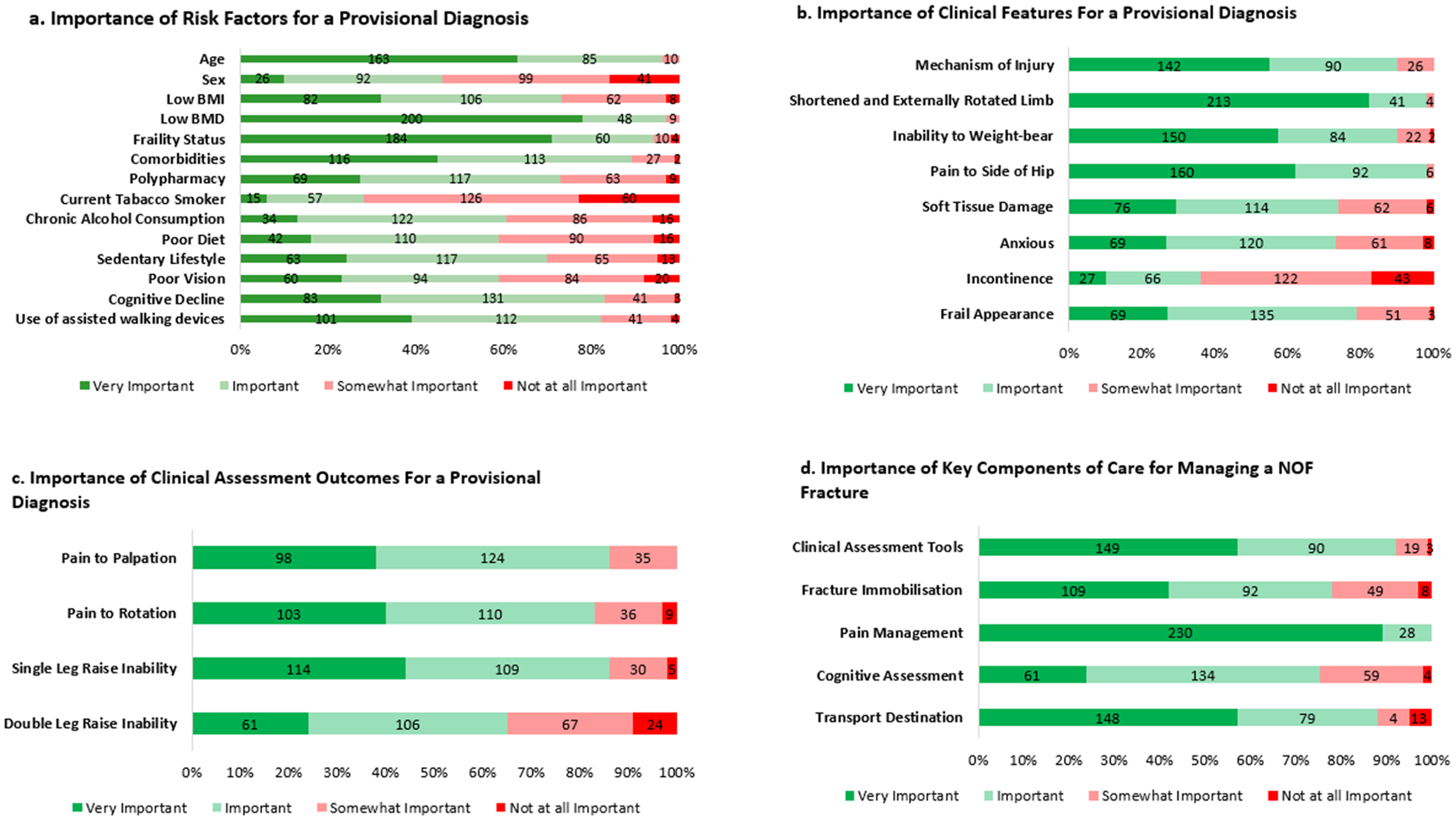
Overview of responder belief regarding elements of NOF management. Figure 4(a): Importance of various risk factors in diagnosing a NOF fracture among respondents. Figure 4(b): Perceived importance of various clinical features in making a provisional diagnosis of a NOF fracture among respondents. Figure 4(c): Perceived importance of various clinical assessment outcomes in making a provisional diagnosis of a NOF fracture among respondents. Figure 4(d): Perceived importance of key components of care when managing a NOF fracture among respondents.
Importance of clinical features when making a provisional diagnosis of a NOF fracture
A shortened and externally rotated limb (83%, n = 213/258), pain/discomfort to the side of the hip (62%, n = 160/258), and inability to weight-bear (58%, n = 150/258) were rated as the most important clinical features for assisting with making a provisional diagnosis (Figure 4(b)). Conversely, evidence of incontinence (17% n = 43/258), anxious/distressed presentation (3%, n = 8/258), and soft tissue damage (bruising and/or swelling) around the injured location (2%, n = 6/258) were rated as being of lowest importance.
Importance of clinical assessment outcomes when making a provisional diagnosis of a NOF fracture
Almost half of the respondents (44%, n = 114/258) rated an inability to perform a single leg raise as a ‘very important’ clinical assessment outcome when making a provisional diagnosis of a NOF fracture (Figure 4(c)). In contrast 24 respondents (9%) rated inability to perform a double leg raise as ‘not at all important’.
Importance of key treatment priorities when managing a NOF fracture
Figure 4(d) shows respondents’ perceived level of importance for the various components of care when treating a patient with a NOF fracture. Almost all the respondents (89%, n = 230/258) rated pain relief as a ‘very important’ treatment priority, followed by clinical assessment tools (57%, n = 149/258). In contrast, transport destination (5% n = 13/258), and fracture immobilisation (3%, n = 8/258) were rated as being of lowest importance.
Behaviour
The use of immobilisation for NOF fractures and the different types
Almost three quarters of respondents (74%, n = 190/258) indicated that they use some form of immobilisation for NOF fractures. Among those respondents who do not employ immobilisation techniques, the predominant reason cited was the absence of a specific guideline to demonstrate how to immobilise this type of fracture (34%, n = 23/66) (Figure 5). Of the 190 respondents who did indicate that they perform some form of immobilisation, the use of a wide sheet across the hips was commonly reported (‘Always’ = 12%, n = 23/190; ‘Often’ = 23%, n = 43/190) (Figure 6). Notably, 32% (n = 60/190) of respondents reported using a method other than the survey options provided, with free text responses including methods such as ‘vacuum splints’ and ‘packing on either side of the injured limb with blankets’.
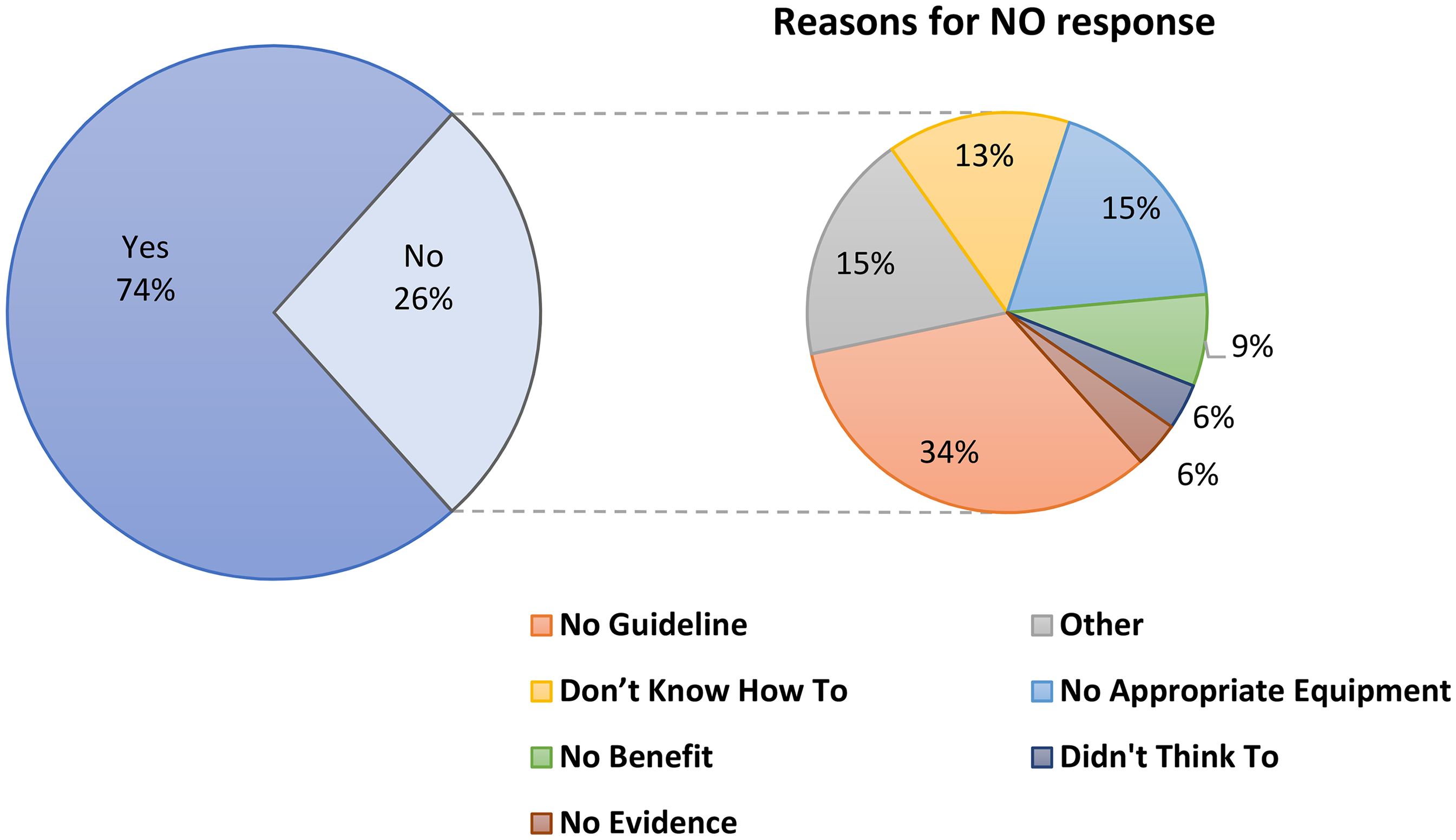
Pie-in-pie chart illustrating the use of immobilisation for NOF fractures. The main pie chart shows the proportion of respondents who do provide some form of immobilisation versus those who do not. For those who do not, the secondary pie chart breaks down their reasons for not performing immobilisation.
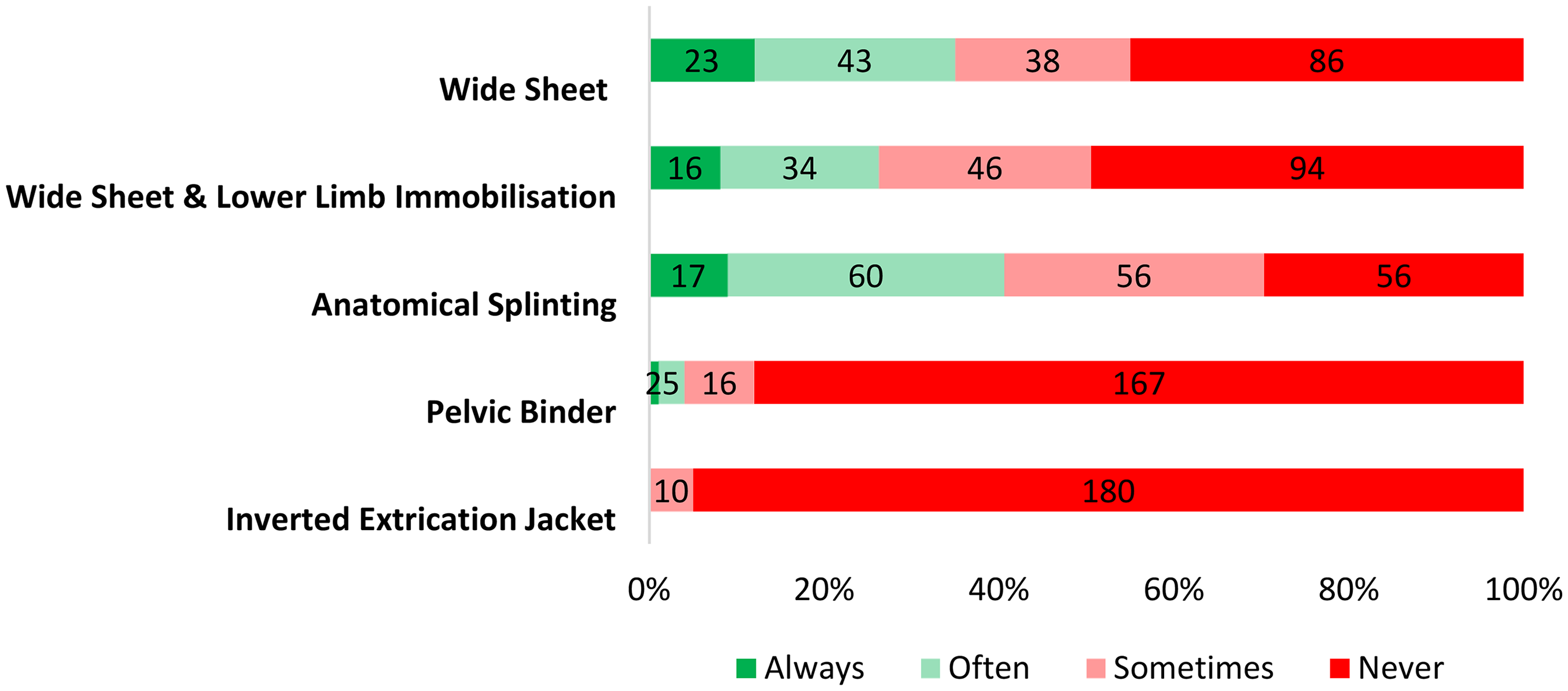
Frequency of use of immobilisation methods for managing a NOF fracture among respondents.
The use of pain relief for NOF fractures and the different types
All respondents (100% n = 258/258) indicated that they consider providing some form of pain relief when treating patients with a suspected NOF fracture. Figure 7(a) shows respondents’ frequency for the utilisation of various methods of pain relief when managing a NOF fracture, with rest and reassurance (92%, n = 237/258), positioning (82%, n = 211/258), and narcotic analgesics (51%, n = 131/258) receiving the highest amount of ‘always’ responses. When asked about the frequency with which specific factors influence their decision-making process for administrating pain relief, over a quarter of respondents (26%, n = 66/258) identified patient refusal as the factor most frequently rated as ‘always’ influential. Conversely, having a short transport time to the hospital received the highest proportion of ‘never’ responses (72% n = 187) as seen in Figure 7(b).
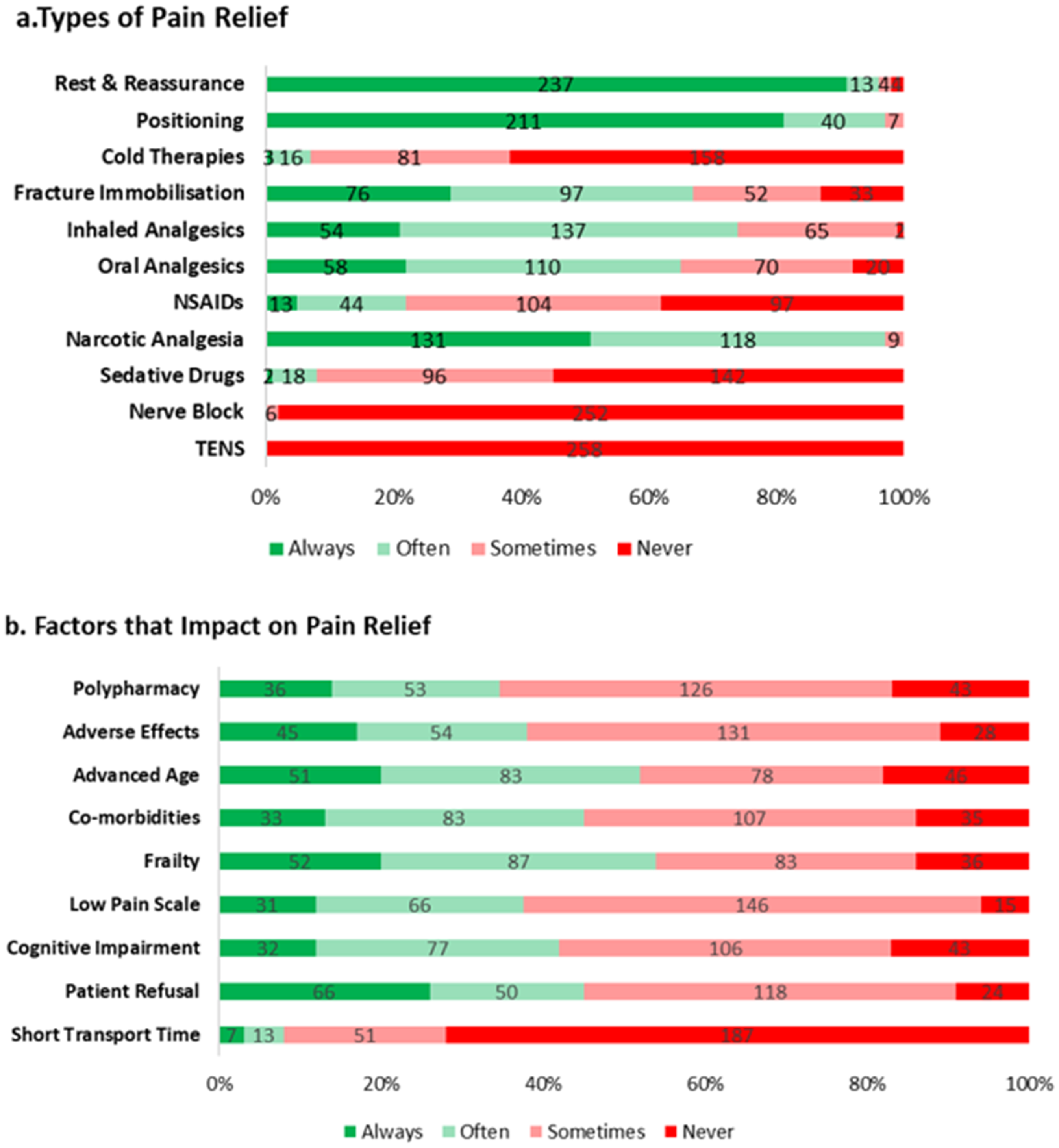
Overview of responder behaviour regarding pain relief. Figure 7(a): Frequency of use of various pain relief methods for managing a NOF fracture among respondents. Figure 7(b): Frequency of factors that impact on the decision-making process for providing pain relief when managing a NOF fracture among respondents.
The use of cognitive assessment when managing a NOF fracture
Figure 8 shows respondents’ frequency for the utilisation of various cognitive assessments when managing a NOF fracture. The use of the Glasgow Coma Scale (GCS) as a cognitive assessment for a patient with a suspected NOF fracture received the highest amount of ‘always’ responses (91%, n = 235/258). Alternatively, 78% of respondents (n = 201/258) indicated that they ‘never’ use the 4AT assessment when managing a patient with a suspected NOF fracture.
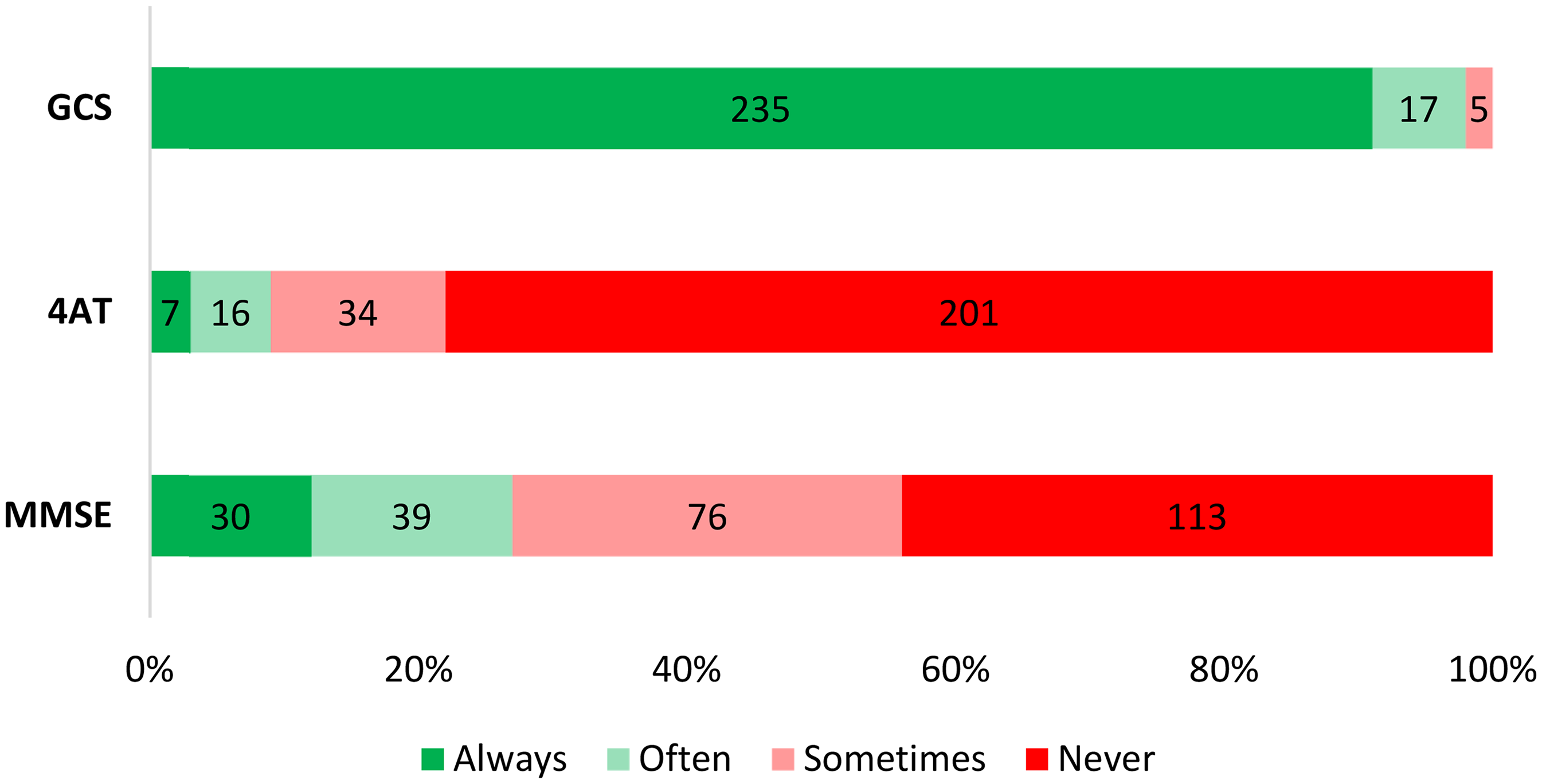
Frequency of use of various cognitive assessments for managing a NOF fracture among respondents. GCS Glasgow Coma Score, 4AT 4 A's test, MMSE Mini mental state examination.
Discussion
This is the first study to explore how Australian paramedics manage NOF fractures, offering important insight into clinician training, education, and their confidence, beliefs, and practices. The survey revealed significant gaps in targeted education and training for NOF fractures, along with a perceived lack of confidence in fracture assessment and management. Additionally, there was notable variation in the methods used to immobilise NOF fracture sites. These findings collectively highlight potential inconsistencies in care and underscore the need for a dedicated clinical guideline. 7
Adherence to guidelines and standardisation of care
A key finding was that 71% of respondents reported that they do not refer to a specific CPG when treating patients with a suspected NOF fracture. This finding aligns with a recent review of publicly available Australian and New Zealand ambulance service guidelines, which found a lack of a standalone treatment protocol or CPG specific to a suspected NOF fracture. 7 Interestingly, 19% of respondents reported referring to a CPG for information about NOF fracture care; though it was unclear which CPG respondents were referring to. When respondents were provided with a free-text response to list the CPG's utilised, responses were generalised and not specific to NOF management, for example, “organisational CPG's”, “limb injuries and fractures”, “pain management”. A fracture that occurs at the NOF differs from standard long bone fractures due to its unique anatomical location, structural characteristics, and blood supply, which can increase the potential risk of complications such as avascular necrosis or malunion. 12 As a result, NOF fractures may benefit from specialised guidelines that incorporate a nuanced approach, distinct from the strategies used for most long bone fractures. This absence of a standalone guideline may contribute to substantial variability in treatment approaches, potentially impacting patient outcomes. 13 Research indicates that the use of standardised guidelines improves the quality of care by reducing clinical variability. 14 The lack of a standalone guideline use highlighted in this study suggests that NOF fracture management may be more reliant on individual practitioner discretion, increasing the risk of inconsistent care. This variability highlights the importance of formal education and training, which can play a crucial role in ensuring standardised, evidence-based approaches to treatment.
Education and training
A high level of education was evident among respondents, with 69% reporting holding a master's or doctoral degree. Despite this, less than 25% reported receiving formal training that focused on the management of NOF fractures. Instead, many stated that they relied on informal, experiential learning through hands-on practice and workplace training. While experiential learning has long been recognised as a critical component of healthcare education, 15 reliance on informal methods can lead to inconsistencies in knowledge and practice. Studies suggest that structured training programs, such as simulation-based learning or formal clinical workshops, are more effective in ensuring competency. 16 Expanding access to formal, evidenced-based training programs could help mitigate knowledge gaps, reduce inconsistency and enhance the confidence of clinicians to manage NOF fractures.
Confidence
Confidence plays a critical role on a paramedics ability to make timely, effective clinical decisions, influencing patient outcomes. 17 Understanding the areas where respondents feel confident in their abilities and where they do not, helps identify potential gaps and allows for educational support to be tailored accordingly. 18
A notable finding from this study is the variability in respondents’ confidence levels across different aspects of NOF fracture management. While most respondents expressed high confidence in obtaining patient history and managing pain, uncertainty was identified in NOF fracture assessment and immobilisation techniques. This lack of confidence may stem from the absence of clear, specific guidelines and education, as noted by most respondents. Previous research supports a link between healthcare providers’ confidence and their familiarity with established protocols. 19 Insufficient familiarity or experience following established protocols could lead to uncertainty and/or inconsistency in clinical decision-making. 19 Addressing this gap in confidence, requires not only the establishment of clear and evidence based guidelines, but also a deeper understanding of the beliefs and treatment priorities which influence decision making and clinical practice.
Beliefs
Exploring the beliefs of paramedics is essential in understanding how they approach practice and make critical decisions in high-stakes environments. Beliefs influence clinical judgments, interactions with patients, and adherence to protocols, directly impacting the quality and consistency of care provided.20,21 By examining respondent beliefs, we can potentially identify factors that may support or hinder best practice adherence and allow for tailored education and interventions that reinforce evidence-based approaches and professional standards.
Respondents highlighted the importance of key risk factors such as low bone mineral density, frailty, and age in diagnosing a potential NOF fracture; however, factors like gender and poor vision were perceived as less important. The ability to perform a single leg raise was highly valued as a diagnostic tool, and respondents emphasise the necessity of direct transport to hospitals with orthopaedic surgical capabilities. These beliefs impact patient care by shaping the approach paramedics take when treating patients with NOF fractures. Recognising the importance of risk factors supports early identification and intervention, while overlooking others may reduce diagnostic vigilance.22,23 The high value placed on the single leg raise test underscores its role in diagnosing NOF fractures. 12 Additionally, the importance placed on transport to specialised hospitals aligns with best practices, ensuring that patients receive timely surgical intervention, which is crucial for reducing complications and improving recovery outcomes. 6
Pain relief was rated the highest treatment priority, ensuring that patients experience immediate comfort and reduced distress, which is crucial in the acute phase of injury management. 24 Effective pain management can also facilitate better cooperation from patients during subsequent assessments and treatments. 25 Clinical assessment outcomes was also rated as having high importance. By prioritising these clinical assessments, paramedics can make informed decisions about the severity of the fracture and the most appropriate course of action, leading to more effective and individualised patient care. 12 Conversely, the comparatively low importance placed on fracture immobilisation may impact patient care by potentially overlooking the benefits of stabilising the fracture early on. 26 While pain relief and clinical assessments are critical, proper immobilisation can assist with a reduction in pain, preventing further injury. 27 These findings highlight the need for further education to promote a comprehensive approach, including potential fracture immobilisation, to optimise patient outcomes. Understanding how these beliefs influence behaviour during prehospital care is crucial for identifying areas where practice can be aligned with evidence-based guidelines.
Behaviour
Investigating paramedic behaviour is crucial in understanding how clinical skills and knowledge are applied in real-world settings. Paramedic behaviour can directly influence patient outcomes, team dynamics, and adherence to professional standards, making it a key focus for improving prehospital care quality. 28 By investigating respondents behaviours, we can identify potential strengths and areas for improvement. It is important to note that the pre-hospital environment is inherently unpredictable, with paramedics often encountering a wide range of scenarios and patient conditions. Despite this variability, maintaining consistent key behaviours, is pivotal to ensure high-quality care and improved patient outcomes.
Consistency in care is especially crucial in managing the significant pain associated with orthopaedic fractures, where untreated pain can lead to adverse outcomes such as delirium and depression.29,30 All respondents indicated that they always consider pain relief, with standard pain management being widely accepted; however, variations in alternative methods like cold therapies and nerve blocks were noted. The literature supports multimodal pain management strategies, with nerve blocks being particularly effective in reducing opioid use and side effects. 31 The lack of consensus on these approaches suggests a need for standardised pain management that promotes multimodal strategies and caters to varied pain levels and clinical skill levels.
Unlike other aspects of care, such as providing pain relief, not all respondents indicated that they would consider providing some form of fracture immobilisation, and there was no consensus on the best method. The immobilisation methods identified ranged from anatomical splinting to full pelvic and lower limb immobilisation, with some respondents reporting the use of techniques discouraged by certain state ambulance services. 32 Immobilisation is critical for stabilising the injury, reducing pain, and limiting further damage, 26 but the variation in techniques could lead to inconsistent practice and potentially negative patient outcomes. Developing clear, evidence-based protocols and training programs could help ensure more consistent and effective care.
There was a clear preference among paramedics for the Glasgow Coma Scale (GCS) as the primary cognitive assessment tool for patients with a suspected NOF fracture, with over 90% of respondents indicating a “always” response. The GCS's widespread use across emergency services in Australia likely contributes to its popularity, while more targeted tools like the 4AT and Mini-Mental State Examination (MMSE) were less favoured. This discrepancy suggests that while the GCS is well-integrated into paramedic protocols, there may be a need for review and education on the utility of diverse cognitive assessment methods. Additionally, over a quarter of respondents indicated that limited hospital options affected their ability to transfer patients to facilities with orthopaedic surgical capabilities. This highlights the logistical constraints to timely care and suggests a need for policy changes to enhance hospital network accessibility and improve coordination between emergency services and healthcare facilities.
Limitations and strengths
There are several limitations to consider when interpreting the results of this study. One limitation is the absence of a validated survey instrument specifically designed to evaluate paramedic practices in the care of NOF fractures. Due to this gap in existing research tools, we were required to design our own survey instrument. While we took care to develop a tool that accurately reflects the key aspects of NOF fracture care, the lack of prior validation means our findings should be interpreted with caution. Another limitation is the relatively small sample size, which may impact our findings. The limited survey responses may not fully capture the confidence, beliefs, and behaviours of all Australian paramedics. Finally, due to the anonymous nature of the online survey, we were unable to verify whether respondents were registered paramedics. However, the recruitment strategies employed and clarity in the survey information sheet regarding inclusion criteria are likely to have mitigated the issue to a large degree.
There are also strengths to this study. It is the first study to examine the confidence, beliefs and behaviours of Australian paramedics regarding the management of NOF fractures. The findings have implications for the development of future training and practice guidelines for this common yet debilitating condition. Additionally, it may prompt further research into the prehospital management of NOF fracture that positively impact patient care.
Recommendations
There continues to be a need for more research regarding the pre-hospital management of NOF fractures. Education providers should be informed of paramedics reduced confidence when assessing and immobilising NOF fractures and address them in an evidence-based manner, helping to ensure that these injuries are adequately assessed and managed. Ideally, the inclusion of standalone CPG that addresses fracture assessment and management for NOF fractures using evidence-based information should be developed. Future research should explore deeper into paramedics’ confidence, beliefs, and behaviours, actively seeking their insights on the educational tools and guidelines that would most effectively support their practice and enhance patient care. Additionally, it should incorporate a range of stakeholder perspectives related to NOF fracture care, ensuring that any resultant policies and practice guidelines are thoroughly evaluated for comprehension and effectiveness.
Conclusion
This study it the first to examine Australian paramedics confidence, beliefs, and behaviours in prehospital NOF fracture care. The findings highlight a critical issue in the pre-hospital management of NOF fractures: the lack of standardised education and guidelines. This gap could explain the variability in paramedic practices, particularly in fracture immobilisation. Without clear, evidence-based protocols, paramedics may lack confidence in their techniques, leading to inconsistent application and potentially suboptimal patient outcomes. Addressing this issue through the development and implementation of evidence-based guidelines and comprehensive training programs could enhance paramedic confidence, standardise care practices, and ultimately improve patient outcomes in the unpredictable pre-hospital environment.
Supplemental Material
sj-docx-1-tra-10.1177_14604086251350629 - Supplemental material for Fractured care? Exploring Australian paramedics’ approach to neck of femur fractures – a cross-sectional survey
Supplemental material, sj-docx-1-tra-10.1177_14604086251350629 for Fractured care? Exploring Australian paramedics’ approach to neck of femur fractures – a cross-sectional survey by Emma Moore, Luke Heales, Katie Clift, Steven Obst and Robert Stanton in Trauma
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.