
Abstract
Introduction
In Ontario, Canada, paramedics use the Field Trauma Triage Standard to identify patients at risk for severe injury. These triage criteria encompass physiologic, anatomic, mechanism of injury, and special considerations to identify patients that should be transported directly to a trauma center. Patients meeting any one of these criteria mandate direct transfer to a trauma center. This study evaluated whether severely injured trauma patients that underwent an interfacility transfer met these triage criteria. The secondary objective was to assess the impact of failed triage application on in-hospital mortality.
Methods
This is a retrospective cohort study of interfacility trauma transfers to an adult trauma center over a 3-year period that were either admitted to the intensive care unit, received an operation within 4 h of arrival, or died within 48 h of arrival. Data were abstracted from the hospital’s trauma registry and chart review of electronic medical records. Frequency of patients meeting pre-hospital triage criteria and which specific criteria were collected. Multivariable logistic regression was performed to assess the impact of missed pre-hospital triage on in-hospital mortality.
Results
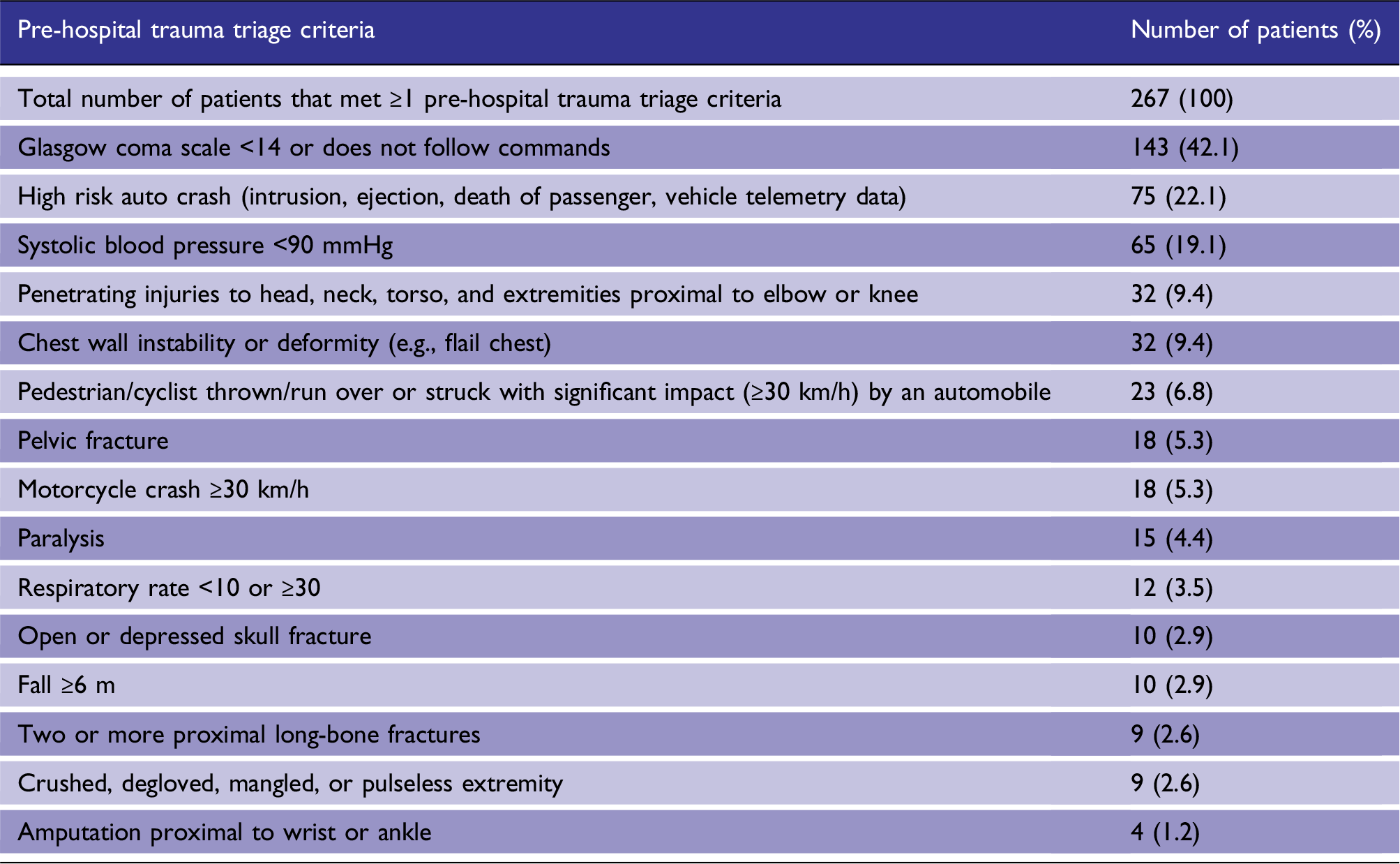
There were 1008 interfacility patients during the study period, of which 340 patients met inclusion criteria; 78.5% (n = 267) of interfacility transports had met at least one triage criteria. Most frequent criteria met were: Glasgow Coma Scale <14 (42.4%), high risk motor-vehicle collision (22.1%), and systolic blood pressure <90 mmHg (19.4%). When adjusted for injury severity score and age, patients who met triage criteria were not at increased odds of death (OR 2.38, 95% CI: 0.87–6.46) compared to interfacility patients that did not meet criteria.
Introduction
Injured patients have lower mortality when cared for at trauma centers compared to non-trauma centers.1–4 Given the impact on mortality, optimizing pre-hospital triage of injured patients is critical, where severely injured patients should be transported directly to the nearest trauma center and bypass closer non-trauma hospitals. However, in North America, 30–60% of severely injured patients are initially admitted to non-trauma centers.5–7 Interfacility transfers of these patients to a trauma center may then later occur so patients can receive definitive trauma care;8–11 however, it has been shown that delays from interfacility transfers are associated with an increase in mortality.9,10,12
Pre-hospital triage of trauma patients is a multi-pronged approach where paramedics must identify patients at risk for severe injury, prioritize patients for transport, and finally choose the appropriate destination for patients to receive trauma care. In Ontario, Canada, bypass of injured patients to go directly to a trauma center is guided by the Field Trauma Triage Standard (FTTS) (Figure 1). The triage standard encompasses physiologic, anatomic, mechanism of injury, and special considerations. Patients meeting any one of these criteria should be directly transported to a trauma center, potentially bypassing a closer non-trauma facility. This protocol is adapted from the Guidelines for Field Triage of Injured Patients, which was established by the American College of Surgeons Committee on Trauma (ACS-COT).
13
Given the geographic barriers to trauma center care in Ontario, if severely injured patients require a transport time >30–60 min to the nearest trauma center, paramedics should request an air ambulance response. If the air ambulance is unable to land along the direct route of the land ambulance and it would result in a significant delay in transport time to the most appropriate hospital, land paramedics will meet with the air ambulance crew at the closest emergency department (ED) as a “modified scene response.”
14
Field trauma triage standard. *If a paramedic is unable to successfully manage the airway or the patient is unlikely to survive transport to the lead trauma hospital, the patient must be transported to the closest Emergency Department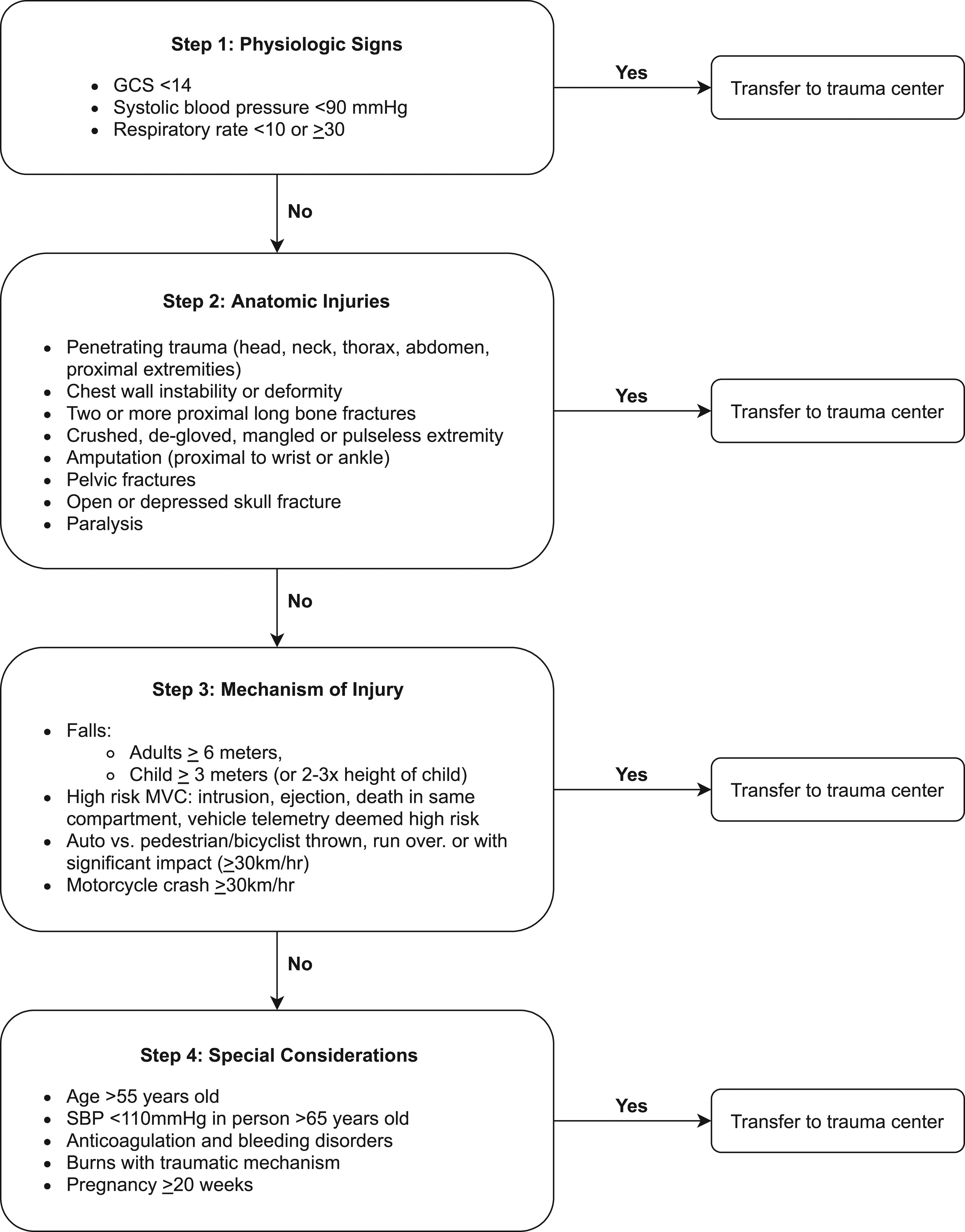
Optimization of a pre-hospital triage system requires a careful balance between under-and over-triage. Under-triage occurs when severely injured patients not transported to a trauma center and may occur if field triage protocols are not sensitive enough or the protocol is not adhered to appropriately. Patients may not demonstrate evident instability at presentation, making the decision especially challenging with the limitations of on-scene assessments. Failure to detect severe injury may cause delayed diagnosis and therapeutic interventions associated with increased morbidity.1–4 Conversely, over-triage creates resource overutilization for patients with minor injuries.
The quality of pre-hospital triage is not based only on the quality of the triage protocol, but also influenced by the adherence to the triage protocol. The primary objective of this study was to evaluate how frequently severely injured trauma patients that underwent an interfacility transport initially met the pre-hospital triage standard and identify the specific criteria met. The secondary objective was to compare in-hospital mortality for transferred patients who met and did not meet pre-hospital trauma triage criteria
Methods
Study design and setting
This is a retrospective cohort study of severely injured trauma patients that underwent interfacility transfer to a level 1 trauma center (St. Michael’s Hospital, Toronto, Ontario, Canada) between 1 January 2017 and 31 December 2019. St. Michael’s Hospital is a 500-bed, urban, academic lead trauma center in Toronto, Canada, with approximately 2000 trauma activations per year. Ontario has nine adult trauma centers and roughly 150 other acute care hospitals that are non-trauma centers. There are no level-2 or level-3 designated hospitals; thus, St. Michael’s Hospital accepts many patients requiring trauma specialist care. Data were abstracted from the hospital’s trauma registry with supplemental information obtained from manual chart review of electronic medical records. This study was approved by the Research Ethics Board of St. Michael’s Hospital (REB # 20-196).
Participants Injured patients (aged 16 years or older) that underwent interfacility transfers as a trauma team activation at St. Michael’s Hospital were included if they met at least one of the following criteria: death within 48 h of arrival to hospital, admitted to intensive care unit (ICU) from trauma bay, or need for surgical intervention within 4 h of arrival. Modified scene response transfers were also excluded as these patients were deemed to have met trauma triage criteria by local paramedics and only brought to a non-trauma hospital due to location or instability.
Variables
Information collected for each patient from the hospital’s trauma registry included age, sex, injury severity score (ISS), mechanism of injury (MOI), initial trauma bay vitals, Glasgow Coma Scale (GCS), and trauma bay interventions including blood transfusion, time of transfer from peripheral non-trauma center to trauma center, and in-hospital characteristics including length of stay, disposition, and mortality.
The primary outcome of interest was the frequency that severely injured patients who underwent an interfacility transfer met the trauma triage standard and identifying which specific criteria were satisfied. The secondary outcome compared in-hospital mortality between transferred patients who met and did not meet the trauma standard using a multivariable logistic regression analysis.
Data sources/measurement
Concurrent manual chart review was carried out for all eligible patients, including review of pre-hospital paramedic call reports for on-scene assessments if report was available. When pre-hospital call reports were available, pre-hospital vital signs, anatomic details, and MOI were used in place of trauma registry data for triage application as this information most accurately captures the criteria used by paramedics. Greater than 90% of all charts had complete pre-hospital call reports. Two study authors reviewed patient records and retroactively determined if the patient’s injuries met physiologic, anatomic, and/or MOI criteria. Frequency of specific criteria was counted. Patients that met >1 triage criteria had counts applied to all criteria satisfied. The “special considerations” criteria were not considered by the study authors as these were not absolute indications for trauma bypass. Additionally, some of the information for assessment of the special consideration criteria may not have been reliably available to paramedics in the pre-hospital environment such as anticoagulant use.
Bias and study size
Inter-rater reliability was assessed using a sample of 20 patient charts that was assessed by both reviewers and found 100% agreement to whether field triage criteria was satisfied or not (kappa statistic 1.0). As the study was primarily descriptive in nature, there was no formal sample size calculation obtained; however, 3 years of data was selected to account for annual and seasonal variations in trauma volumes.
Statistical methods
Descriptive statistics were used to evaluate the distribution of data for all variables of interest. Continuous variables were all found to be non-normally distributed and summarized as medians and interquartile ranges. Wilcoxon Rank Sum tests were used to examine differences across non-normally distributed continuous variables. Categorical variables were displayed as frequency and percentages and compared using Chi-square tests.
A multivariable logistic regression model was used to explore the impact of failure to correctly apply the field trauma triage criteria on in-hospital mortality. Age and injury severity score (ISS) were determined a priori to be included in the model as confounders to mortality. Patients with any missing data for one or more of the predictor variables of interest were excluded from the final model. Missing data resulted in exclusion of <5% of observations.
All statistical analyses were conducted using SAS Studio version 3.4 (SAS Institute, North Carolina, USA).
Results
Frequency of transferred patients meeting triage criteria
There were a total of 3327 trauma patients during the study period, of which 1008 were interfacility transports and 340 were included in our final cohort (Figure 2). Characteristics of the study population are shown in Table 1; of 340 transferred patients, 267 (78.5%) met pre-hospital trauma triage criteria. Study flow diagram detailing the inclusion of interfacility transfers between 1 January 2017, and 31 December 2019. Baseline characteristics of patients who met and did not meet field trauma triage criteria (FTTS). IQR: interquartile range; SMH: St. Michael’s Hospital.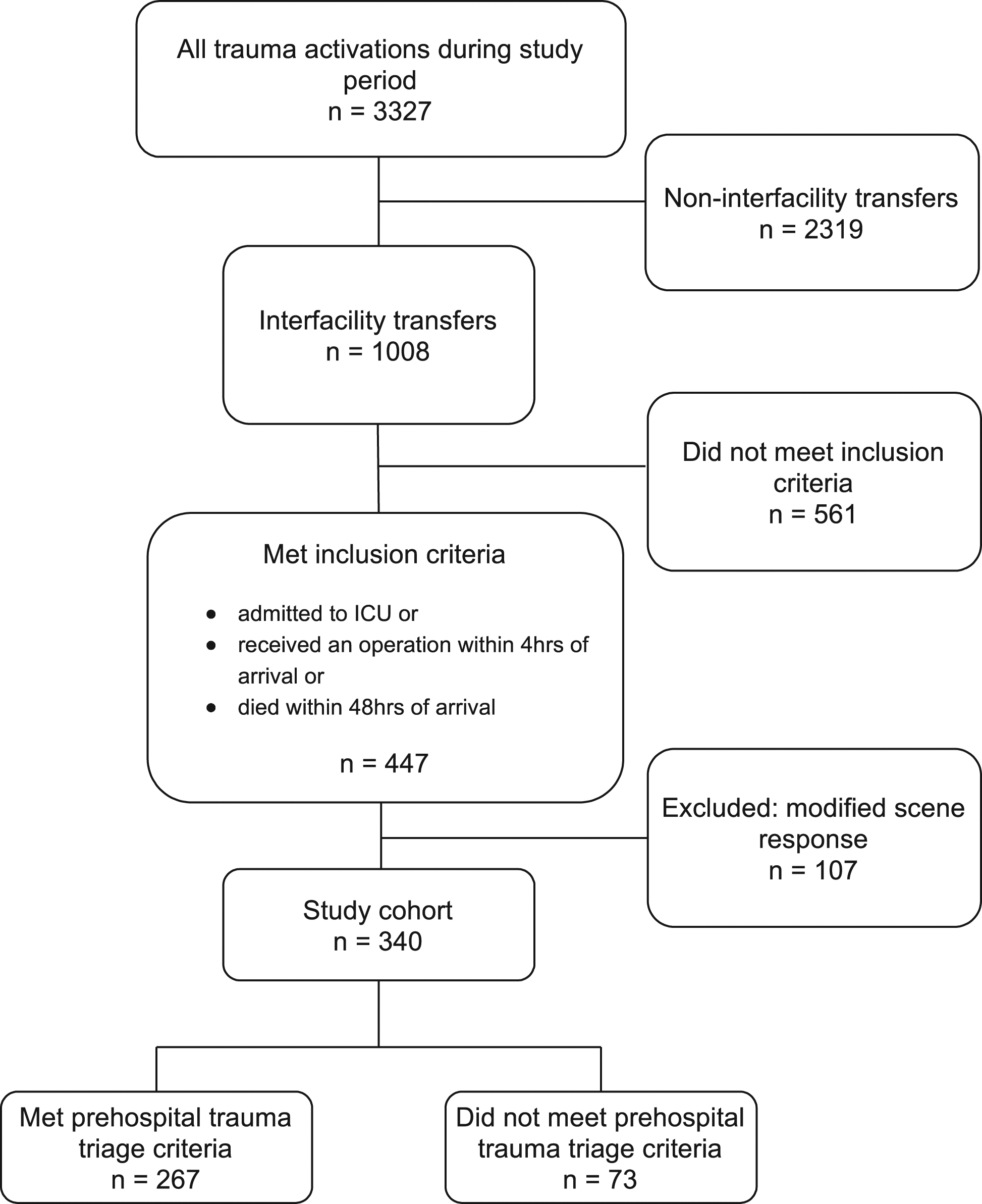
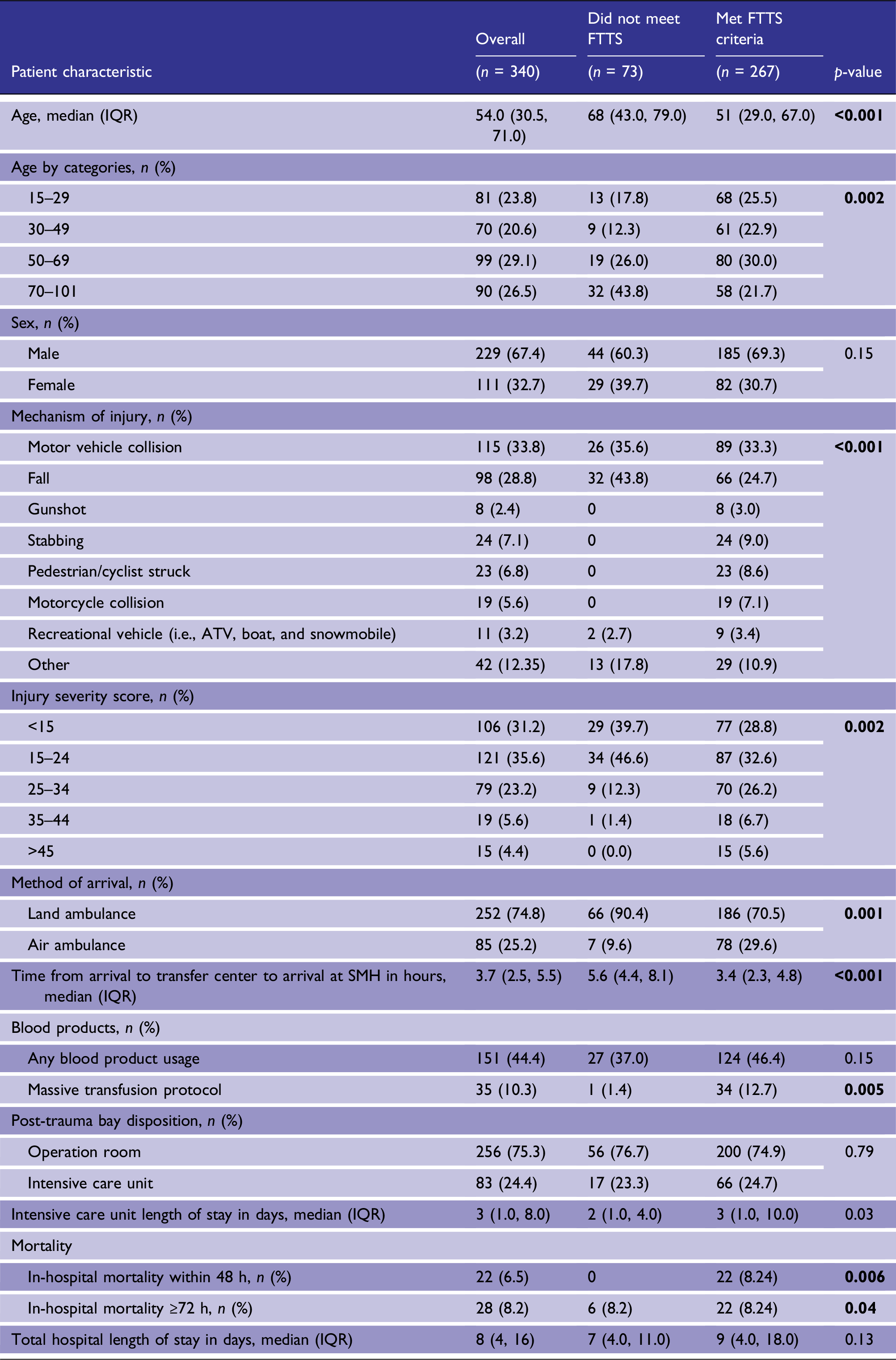
Patients who met triage criteria represented a younger cohort (median age 51 vs 68 years) in those who did not meet triage criteria; however, 21% of patients over the age of 70 had met triage criteria. Patients who met triage criteria had a higher ISS and were more likely to require massive transfusion protocol activation (12.7% vs 1.4%). The time from patient arrival at sending hospital to arrival at trauma center was shorter for patients who met triage criteria, with a median transfer time of 3.4 h vs. 5.6 h. Patients who met triage criteria had longer ICU length of stay with median of 3 days vs. 2 days.
Frequencies of pre-hospital trauma triage criteria met by study population.
Impact on in-hospital mortality
Generalized estimating equation logistic regression model of odds of in-hospital mortality.
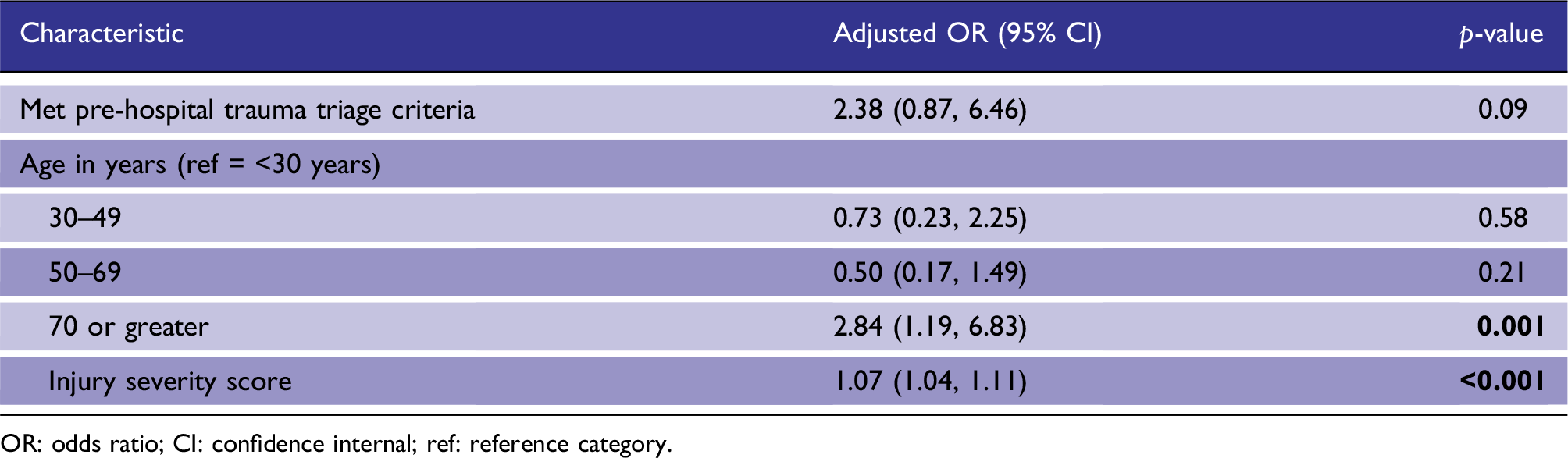
OR: odds ratio; CI: confidence internal; ref: reference category.
Discussion
This study has three important findings. First, >78% of severely injured transferred trauma patients met at least one pre-hospital trauma triage criteria. Secondly, increasing age appears to be associated as a risk factor for failure to apply the triage standard and lastly, there appears to be no increased mortality in this group of severely injured trauma patients that initially met triage criteria.
Our finding of low pre-hospital adherence to pre-hospital trauma triage protocol is similar to what has been previously described in the literature, demonstrating suboptimal adherence rates worldwide, ranging from 21% to 93%.9,10,15–17 There are several factors that might influence adherence to pre-hospital trauma triage protocols, including paramedic expertise and experience, trauma center proximity and preference of the paramedic or patient. 15 A previous study in Ontario showed that paramedics incorporate relative distances into their decision making, where 1–2 mile differential distance to a level-1 trauma center was associated with lower compliance with triage protocols. 17 Alternatively, paramedics may be transporting patients to the closest hospital because the severity of injury is not recognized, especially in the absence of cues relating to an injury. Data suggest that paramedics identify lack of high-level clinical judgment and training, short training and evaluation, and insufficient opportunity for practice and supervision as key issues in pre-hospital patient safety. 18 Our findings suggest that there are opportunities for reducing the gap between ideal and actual application of field trauma triage guidelines. To understand and improve adherence rates further, future research should assess the transparency of triage decisions and reasons and barriers to non-adherence to a pre-hospital trauma triage protocol. Paramedic judgment can be independently evaluated from the triage protocol, allowing for separate evaluation of the quality of the triage protocol, adherence and performance of the system. This study also provided an opportunity to assess how we can modify triage criteria to enhance the sensitivity of pre-hospital triage to capture patients at risk of severe injury. We found that recreational vehicle accidents including all-terrain vehicles (ATV), boat and snowmobile accidents accounted for 11 (3.2%) patients, and 80% of these injured patients had met triage criteria based on anatomic or physiologic criteria, yet this particular mechanism of injury is not captured in the triage criteria. The mechanism of injury for these recreational accidents is similar to those involving unrestrained motorcyclists and cyclists struck by a vehicle and can be considered to be included in future iterations of the triage criteria.
Older age was a significant predictor of triage to a non-trauma center, which is consistent with previous work that identified undertriage in patients over the age of 65 years.9,10,12,15,17 Older adults are a particularly vulnerable population with more cognitive, physical, and physiologic impairments; therefore, low energy trauma mechanisms may result in serious injuries. 11 Undertriage of this population has been associated with higher mortality rates. 19 The adherence rate to pre-hospital trauma triage protocols was especially low for elderly patients meeting only one vital sign criteria, compared to injury type or mechanism of injury criteria. 20 To help explain the under triage of elderly trauma patients to designated trauma centers, a survey of pre-hospital providers identified several factors: lack of training in managing injured elderly patients, unfamiliarly with the triage protocol and feeling that it is not worth it to spend expensive trauma center resources on elderly patients. 20 Owing to the high likelihood of adverse outcomes in this patient population, several bodies of work have aimed to modify pre-hospital triage protocol to emphasize physiological and anatomic differences in the elderly population. 13 Our findings add to the body of evidence that suggest interventions and geriatric specific triage thresholds aimed at reducing the rate of undertriage among severely injured elderly patients should be an important focus.
A considerable proportion of trauma patients in our study population had met pre-hospital trauma criteria based on initial GCS score and blood pressure, which has both been previously shown to be pre-hospital variables associated with an increased risk of undertriage.14,15 Patients with traumatic brain injury may be particularly at risk of undertriage due to challenges in obtaining an accurate GCS score in the pre-hospital setting where patients often present with multi-system injuries and an austere pre-hospital environment that may preclude an accurate assessment of level of consciousness. However, as the physiologic criterion of hypotension is prescriptive in nature and not limited to interpretation, this may be indicative of either paramedics exercising their discretion, or an inaccurate judgment on the severity of injury as mentioned above.
In patients who underwent an interfacility transfer, those who met pre-hospital trauma triage criteria retrospectively did not have higher odds of mortality compared to those who did not meet triage criteria. However, there is evidence of patient harm from secondary interfacility transfers. This was previously demonstrated in Ontario, Canada, with interfacility transfers of trauma patients being associated with a mortality increase of approximately 25% compared to patients seen directly at a trauma center. 8 This trend is also supported by previous literature that demonstrates non-adherence to pre-hospital trauma triage protocol is associated with higher secondary transfer and mortality. 21
We found that the average length of time for transfer was shorter for those who met triage criteria, likely owing to their severity of injury and urgency to transfer to a level 1 trauma center. Given that 20% of trauma deaths occur during the first 6 hours after injury, efforts aimed at reducing emergency department and transport time might lead to improved survival in these patients where undertriage is unavoidable. 22
Limitations
This study has several limitations. The impact on mortality was a secondary outcome and the resulting small sample of patients that died may have resulted in a Type II error. This is reflected in the wide confidence interval for odds of mortality. A larger sample size may have been able to better delineate any association between meeting triage guidelines and mortality. Determination of adherence to trauma triage was based on retrospective evaluation of pre-hospital patient care records, and in some cases, when these reports were not available, initial hospital vital signs and nursing notes were used as a surrogate for on-scene patient parameters. Therefore, some physiologic parameters that were used were recorded at the time of arrival at the trauma center, not at the time of initial paramedic contact. Therefore, some instances of physiologic inclusion may not have represented a patient’s initial condition. Additionally, we could not account for other geospatial variables that might impact pre-hospital transport decisions. Furthermore, our study design precluded us from directly exploring pre-hospital provider rationale accounting for the observed triage decisions.
Conclusion
Pre-hospital trauma triage standards exist to identify patients that would most benefit from direct transfer to a trauma center. This study found that 78% of severely injured patients that were eventually transferred to a trauma center met one or more triage criteria. Hypotension and GCS <14 were the two physiologic criteria commonly missed. This delay to care was not associated with increased mortality.
Footnotes
Acknowledgments
The authors would like to thank Rosane Nisenbaum for her statistical support for the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Research Ethics Board of St. Michael’s Hospital (REB # 20-196).
Informed Consent
Informed consent was not sought for the present study because the study included de-identified patient data gathered from a trauma registry.
Guarantor
Brodie Nolan
Contributorship
B.N., W.L., and G.M. conceived and designed the study and obtained research ethics approval. BN, WL, and GM performed data collection. B.N., W.L., and G.M. analyzed the data. W.L. and G.M. drafted the manuscript, and all authors contributed substantially to its revision. B.N. takes responsibility for the paper as a whole.