
Abstract
Background
Blunt cerebrovascular injuries (BCVIs) are associated with high risk of ischaemic strokes during hospital admission. Understanding of high-risk factors associated with inpatient stroke and treatment characteristics may help with preventing stroke outcomes. The aim of this study was to report the incidence, risk factors and treatment characteristics of inpatient stroke outcomes in patients diagnosed with BCVI at an adult level 1 trauma centre.
Methods
All patients from Alfred Health Trauma Registry who presented from January 2014 to June 2021 and recorded to have BCVI were included in the study. Patient and trauma characteristics, clinical measures on admission and grades of vessel injuries were recorded. Choice and duration of treatment and inpatient stroke outcomes were also extracted.
Results
There were 300 BCVI patients during the study period and 56 patients had stroke on arrival. Of the remaining 244 patients, 24 patients had stroke during admission and thus the incidence of inpatient stroke in BCVI patients was 9.8%. Eighteen patients died during admission, of which five patients had stroke. Severe trauma, low Glasgow Coma Scale and higher grade BCVIs were associated with the increased risk of ischaemic stroke. Anti-thrombotic therapy was associated with reduced stroke outcomes.
Conclusions
The incidence of inpatient stroke in BCVI patients is high and potentially preventable. The risk of stroke was highest in the first 72 h and associated with several high-risk features. Blunt cerebrovascular injuries involving these high-risk features should alert the clinician to strongly consider initiating anti-thrombotic therapy. Early anti-thrombotic therapy may reduce stroke outcomes although often challenged by concurrent bleeding risks.
Introduction
Blunt cerebrovascular injuries (BCVIs) are relatively rare1–3 but carry a risk of in-hospital ischaemic strokes (IS), which are potentially preventable. 4 The overall risk of BCVI-related IS has been reported to be up to 33%2,5 with more severe injuries conferring a higher risk.6,7 Blunt cerebrovascular injury-related IS is also associated with significant mortality, with evidence suggesting rates of up to 15–31%.8–10 The mean age of blunt trauma is generally reported to be less than 55,11,12 and so BCVI is an important aetiology of IS in the young.
Primary preventative treatment approaches following BCVI are generally thought to reduce IS but randomised trial evidence is lacking. Most guidelines13,14 recommend anti-thrombotic therapies for BCVI, with endovascular surgical intervention generally reserved for secondary stroke prevention in the setting of high-grade BCVIs.14–16 Commencing anti-thrombotic therapy early, particularly in the first 24–48 h may reduce the IS incidence10,17 as the majority of IS occurs early.4,18 This time window is also when anti-thrombotic therapy is most often contraindicated, either due to heightened risk of bleeding from other traumatic injuries or due to staged definitive surgeries. Such a scenario is not uncommon and poses a real clinical treatment dilemma.
In addition, the optimal choice of anti-thrombotic therapy or the treatment duration has not been clearly established. Earlier studies recommended heparin as first-line therapy8,19; however, more recent studies noted anti-platelets are likely equivalent to anti-coagulation.20,21 Due to the lack of direct comparison studies and randomised trials, current guidelines do not provide any specific recommendations on treatment choice but suggest using either heparin or anti-platelets.13,17,22 As a result, there is considerable difference among clinicians’ preference and practice in terms of treatment choice. 23
The aim of this study was to evaluate the incidence, risk factors and treatment-related outcomes of inpatient IS in BCVI patients from a large, single-centre cohort. It is a planned analysis following a previously published report on the incidence of BCVIs at a single large tertiary trauma centre. 1
Methods
This was a single centre, retrospective cohort study conducted at Alfred hospital – a large Level 1 trauma centre and a tertiary neuroscience centre. The trauma unit provides 24-h emergency and trauma service for the state and admits over 5000 patients annually. All adult patients who were recorded in the Alfred Health Trauma Registry from January 2014 to June 2021 with a diagnosis of BCVI were included in the study. Our institution-specific BCVI screening criteria (developed based on modified Denver criteria) were used to screen blunt trauma patients. 1 The diagnosis of BCVI was confirmed by two independent neuroradiologists who also graded the injuries, according to Biffl criteria. 15 Patients whose BCVI diagnosis was not independently confirmed were excluded from the study. All imaging modalities including CT angiogram, magnetic resonance angiogram and digital subtraction angiography within 3 days from the trauma were accepted. The study was approved by the local Ethics Research Governance Office (Project no 445/19).
Patient and trauma characteristics including baseline demographics, nature and severity of trauma, high-risk features and mechanism of injuries were collected. Clinical measures on arrival including injury severity score (ISS), Glasgow Coma Scale (GCS) and blood pressure were also recorded. Evidence of traumatic brain injury (TBI) and IS found on initial trauma scans was noted. Vessel injuries, according to the location and grades using Biffl Grading, 15 were documented. Blunt cerebrovascular injuries with mild to moderate injuries (Grade I and II) and moderate to severe injuries (Grade III and IV) were grouped together for analysis. Choices of therapies commenced for BCVI during the admission were recorded, along with the timepoints and duration. Clinical outcomes during hospital stay including stroke, duration of admission and death were collected.
Characteristics of BCVI patients and stroke outcomes were summarised using descriptive statistics, including relative frequencies for categorical variables and measures of central tendency and dispersion for continuous variables. Risk ratio (RR) and event rate were also calculated as a measure of association. The associations between demographics, risk factors, treatment and stroke outcomes were analysed using one-way ANOVA for continuous variables, Mann–Whitney U test was used for non-normally distributed variables and Chi square or Fisher exact test for categorical variables. Holm–Bonferroni correction was used to account for multiple comparisons. A p-value of <.05 was considered as statistically significant.
Results
Between January 2014 and June 2021, a total of 20,954 patients were admitted to our institution with blunt trauma. Among those patients, 300 (1.4%) were confirmed to have a total of 428 BCVIs. Fifty-six BCVI patients (18.6%) had stroke on arrival as evidenced by admission CT, 13 (4%) of them had IS and 43 (14%) had intracranial haemorrhage (ICH). Of the remaining 244 BCVI patients, 24 (9.8%) patients had IS during admission. Three of 244 (1.2%) had ICH during admission. Thus, a total of 37 (12%) patients in our total study cohort (n = 300) had IS and 9.8% of this was during admission. A total of 43/300 (14%) patients died, 18 during admission (6%), of which five had IS.
Patient baseline demographics, clinical characteristics and trauma mechanisms of BCVI patients who had a stroke are compared with those who did not have a stroke in Table 1. The sex distribution was similar between groups. The median age was 46.5 (interquartile range [IQR] 41.5–57) in stroke population and 51 (IQR 35–66) in non-stroke population, and this difference was not significant (z-score 0.86, p = .39). The median ISS was significantly higher (31, IQR 36–41.5) in stroke patients, compared to non-stroke patients (20, IQR 13–29) (z-score −3.89, p < .001). The mean GCS was significantly lower in stroke population compared to non-stroke population (9 ± 5.64 vs. 12 ± 4.46, p = .002). There was no significant difference in mean initial systolic blood pressure between two groups (132 ± 23.59 vs. 132 ± 32.01, p = .95). The mean length of stay was significantly higher in stroke patients (15 days vs. 10 days, p = .009). A total of 5 (21%) inpatients died in the stroke group, while 13 (6%) patients died in the non-stroke group and this difference was significant (RR 3.48, confidence interval [CI] 1.35–8.91).
Basic demographics and risk factors of stroke and non-stroke BCVI patients.
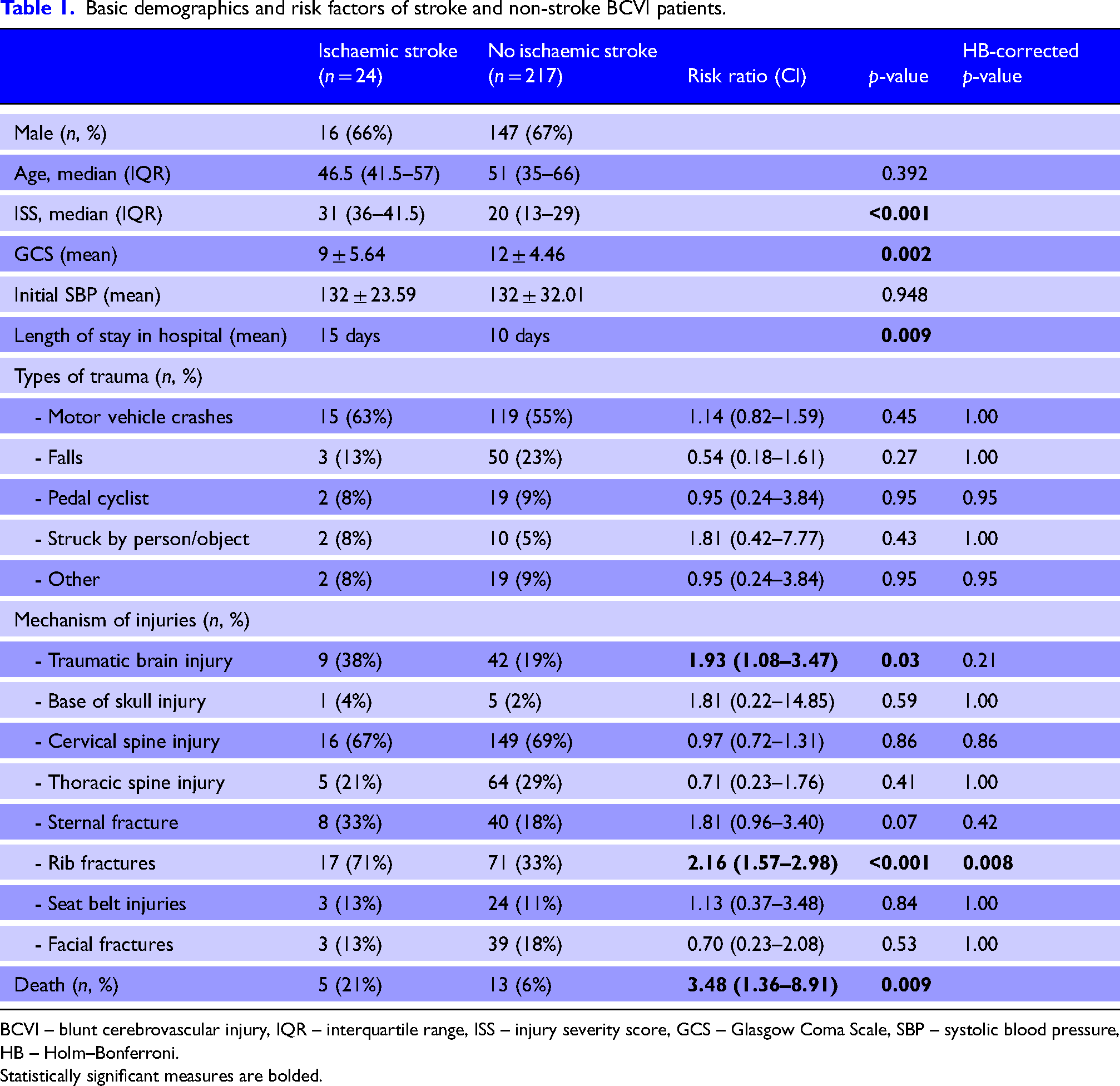
BCVI – blunt cerebrovascular injury, IQR – interquartile range, ISS – injury severity score, GCS – Glasgow Coma Scale, SBP – systolic blood pressure, HB – Holm–Bonferroni.
Statistically significant measures are bolded.
There was no difference in the mechanism of trauma between the stroke and non-stroke groups. Motor vehicle crashes were the commonest type of trauma in both groups and were present in more than 50% in both groups. In terms of associated injuries, the percentage of stroke patients with TBI and rib fractures was higher than non-stroke patients (RR 1.93, CI 1.08–3.47 and RR 2.16, CI 1.57–2.98, respectively); however, only rib fractures were significantly different after accounting for multiple comparisons using Holm–Bonferroni correction.
The association between stroke outcomes according to the location and number of BCVIs is shown in Table 2. There were 71 patients with carotid artery injuries (CAIs) and 11 of them had IS. Similarly, there were 151 patients with vertebral artery injuries (VAIs) and 11 of them had IS. Nineteen patients had both and two of them had IS. Carotid artery injuries were associated with a higher percentage of strokes compared to VAI (15% vs. 7%) but this difference was not statistically significant (p = .16). In stroke population, there were 15 patients with one vessel injury, eight patients with two vessel injury and one patient with three vessel injury. Similarly, in the ‘no stroke’ population, there were 175 patients with one vessel injury, 37 patients with two vessel injury and five patients with three vessel injury. None of the patients in either group had all four vessels injured. The percentage of stroke did not significantly differ based on the number of the vessels injured (p = .12).
Stroke outcomes based on the location and number of vessels injured.
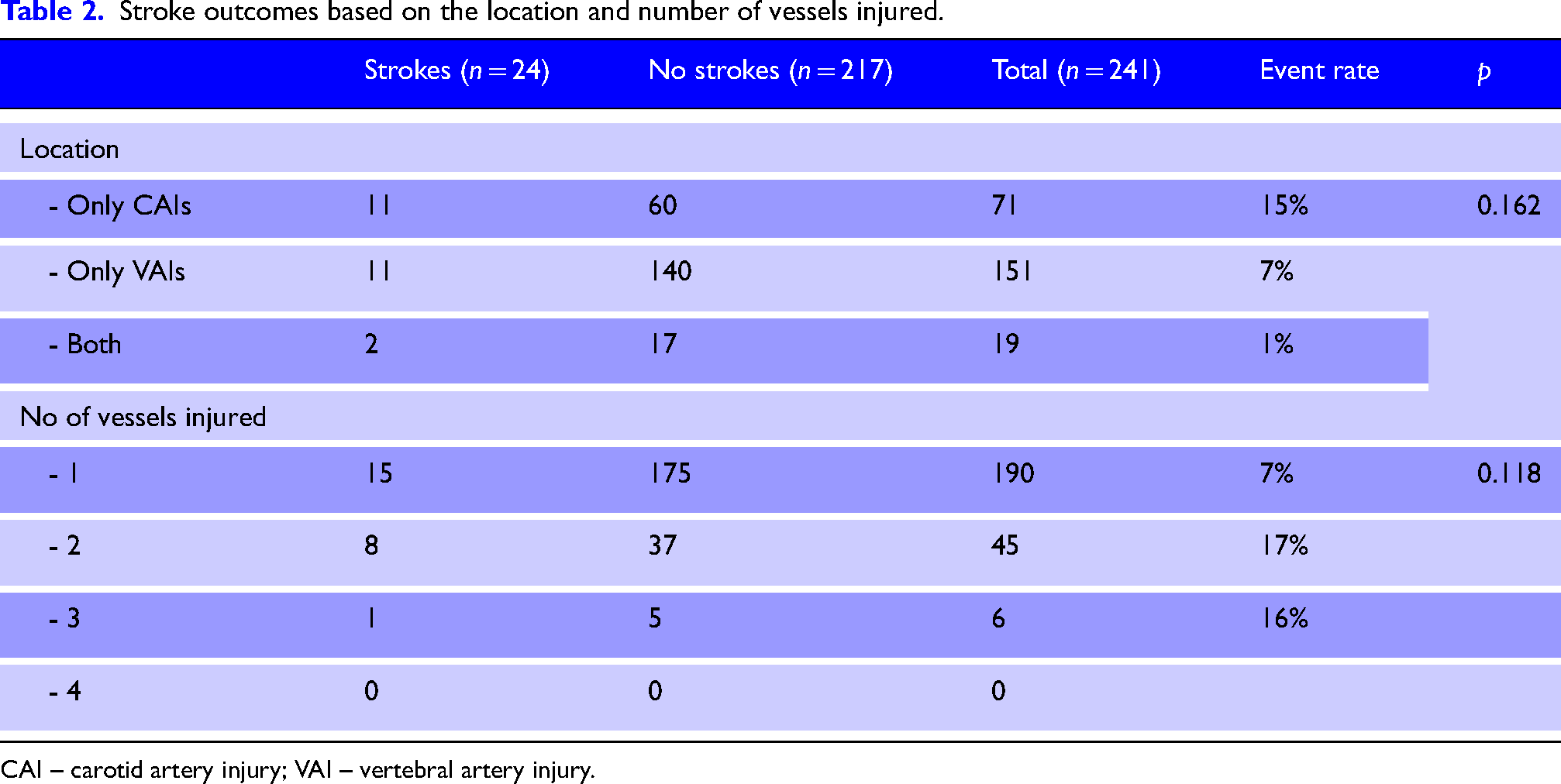
CAI – carotid artery injury; VAI – vertebral artery injury.
The association between BCVI grades and stroke outcomes is shown in Figure 1. There was an increasing trend in the number of IS observed with worsening grades in all vessels; however, this was not statistically significant. In CAI patients, there were 57 with mild to moderate injuries and eight of them had IS (14%), while 3 of 14 patients (21%) with moderate to severe injuries had IS (p = .49). Similarly, there were 67 patients with mild to moderate VAIs and three of them had IS (4%), while 8 of 84 patients (9.5%) with moderate to severe VAIs had IS (p = .27). In patients who had both CAI and VAI, the highest grade of injury was taken for analysis. Among patients who had both CAIs and VAIs, there were 13 patients with mild to moderate injuries and one had IS (7.7%) and six patients with moderate to severe injuries and one had IS (16.7%) (p = .60).
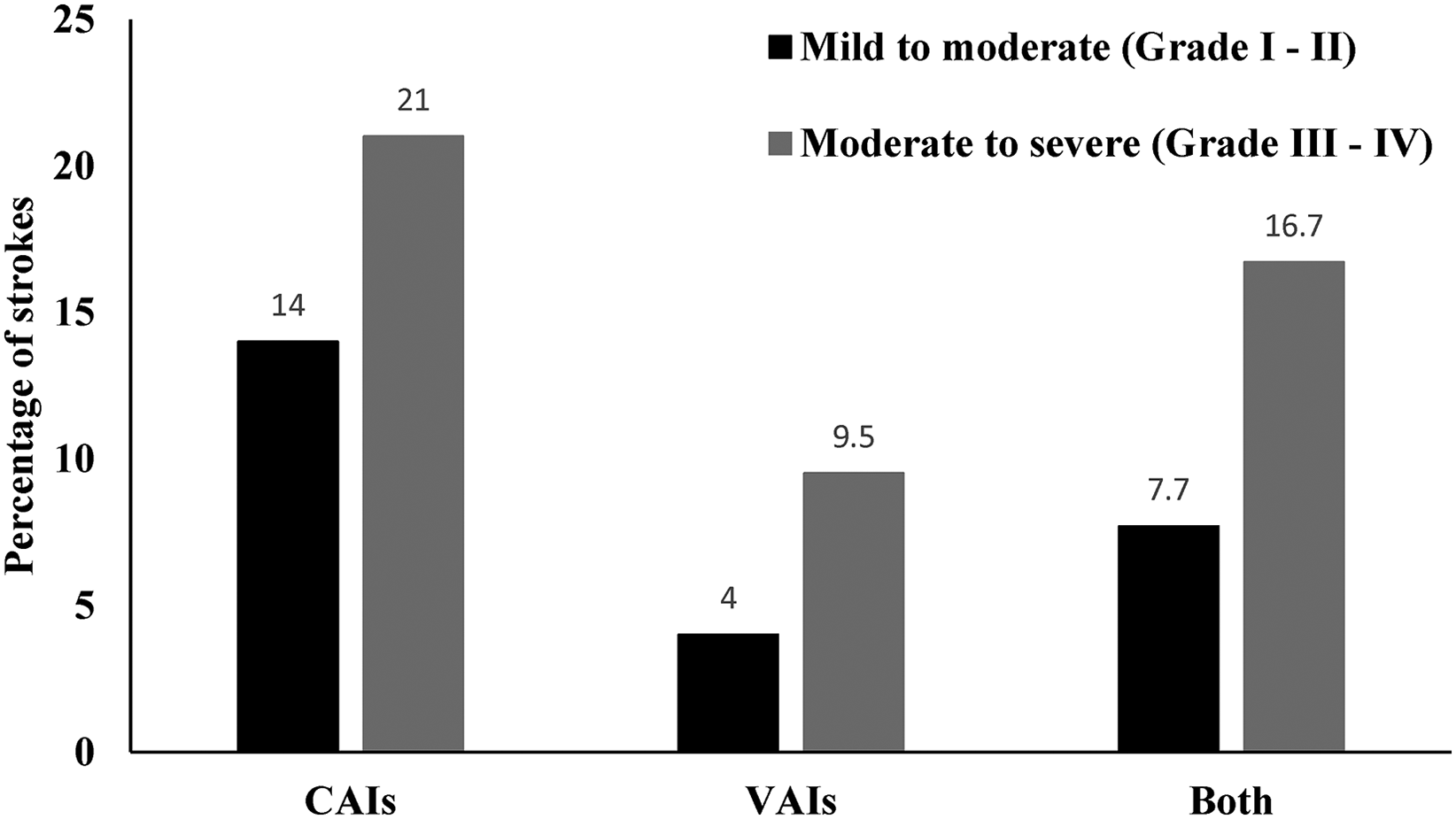
Stroke outcomes according to the grade of vessel injuries.
Figure 2 shows the timing of stroke occurrence from the day the patients were admitted. Three quarters (18/24) of strokes occurred in the first 72 h, although some strokes still occurred up to day 10. One patient had a stroke more than a month post-admission.
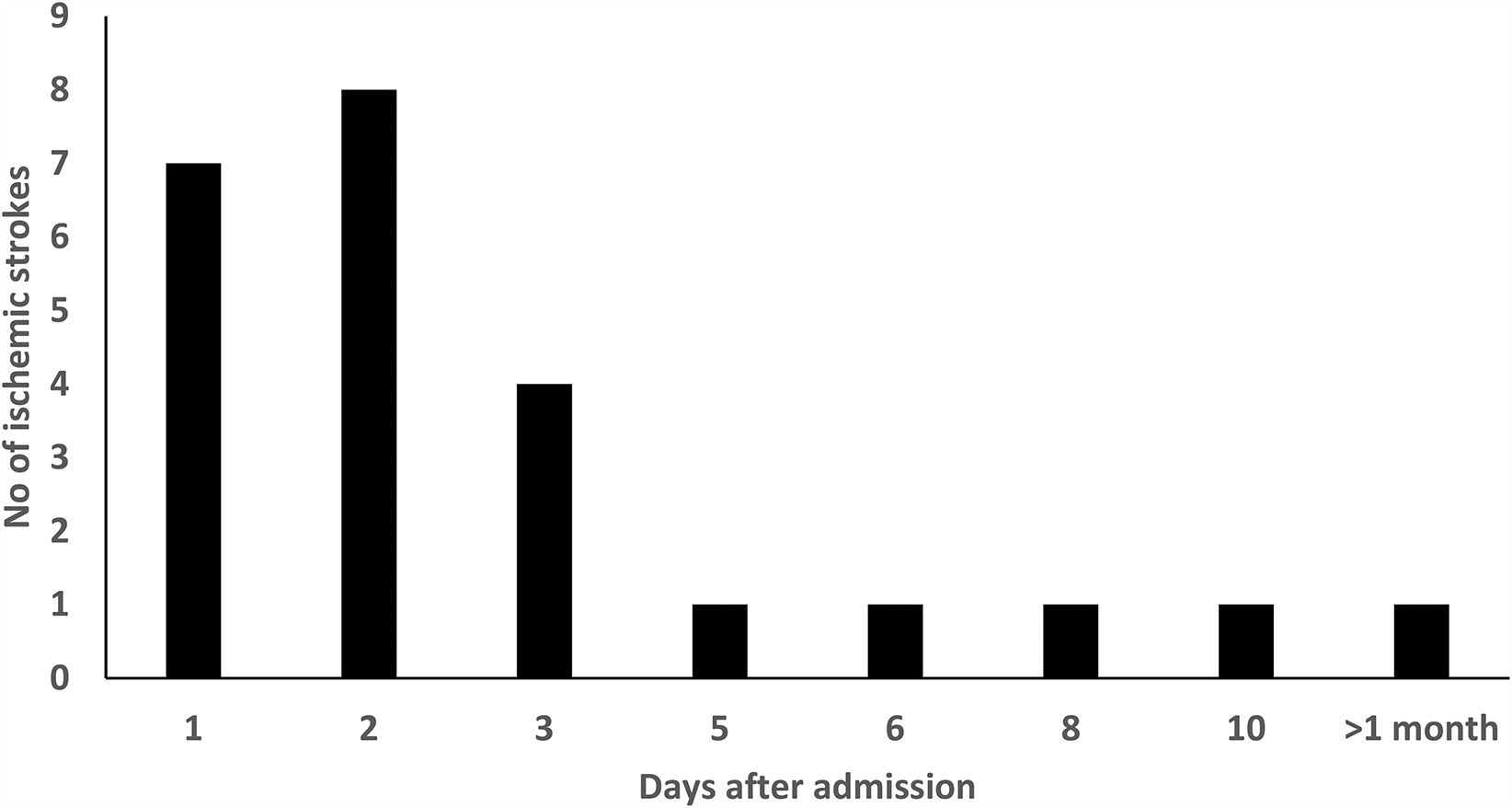
Timing of stroke occurrence from the day of admission.
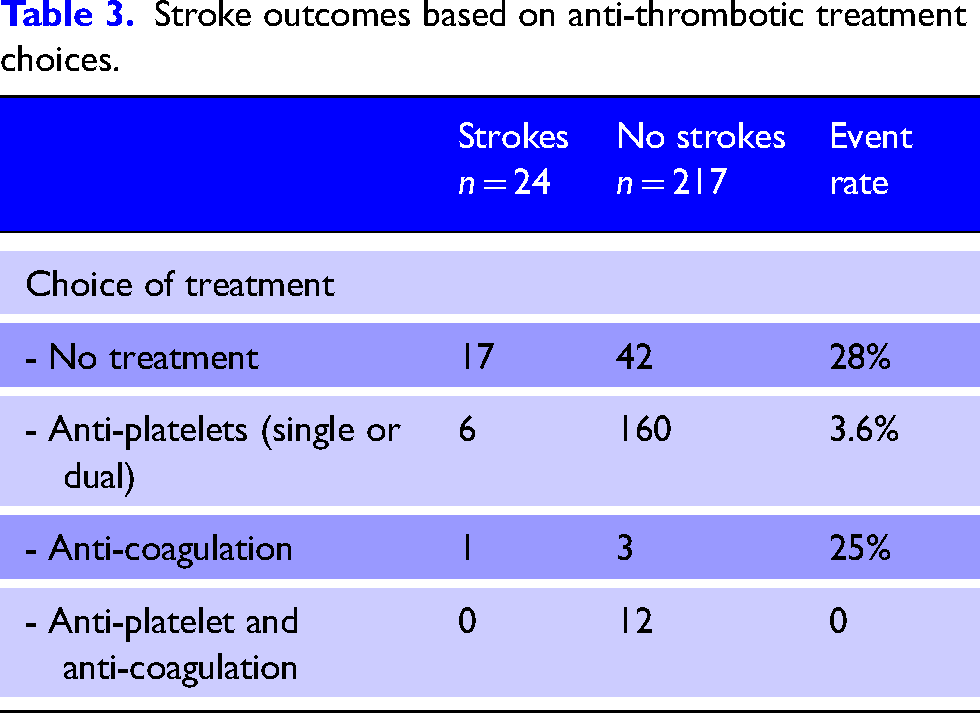
The choice of anti-thrombotic treatment options used across both groups is compared in Table 3. Fifty-nine patients were not on any treatment and 17 of them had IS. Thus, the stroke event rate of patients who were not on any treatment at the time of IS was 28%. There were 166 patients treated with single or dual anti-platelets and six patients (3.6%) had IS. Four patients were treated with anti-coagulation, and one patient (25%) had IS. The most common reasons for not starting an anti-thrombotic therapy were concurrent haemorrhage, increased haemorrhagic risks and planned surgeries. Aspirin was the most common anti-platelet used. Clopidogrel and prasugrel were the other choices. Anti-platelet was used with anti-coagulation when there was a concurrent indication such as venous thromboembolism or atrial fibrillation.
Stroke outcomes based on anti-thrombotic treatment choices.
The effect of treatment-related outcomes is shown in Figure 3. Of 24 patients who had a stroke during inpatient stay, 17 were not on any treatment at the time of stroke (71%), 6 patients were on single or dual anti-platelet therapy (25%) and 1 patient was on anti-coagulation (4%).
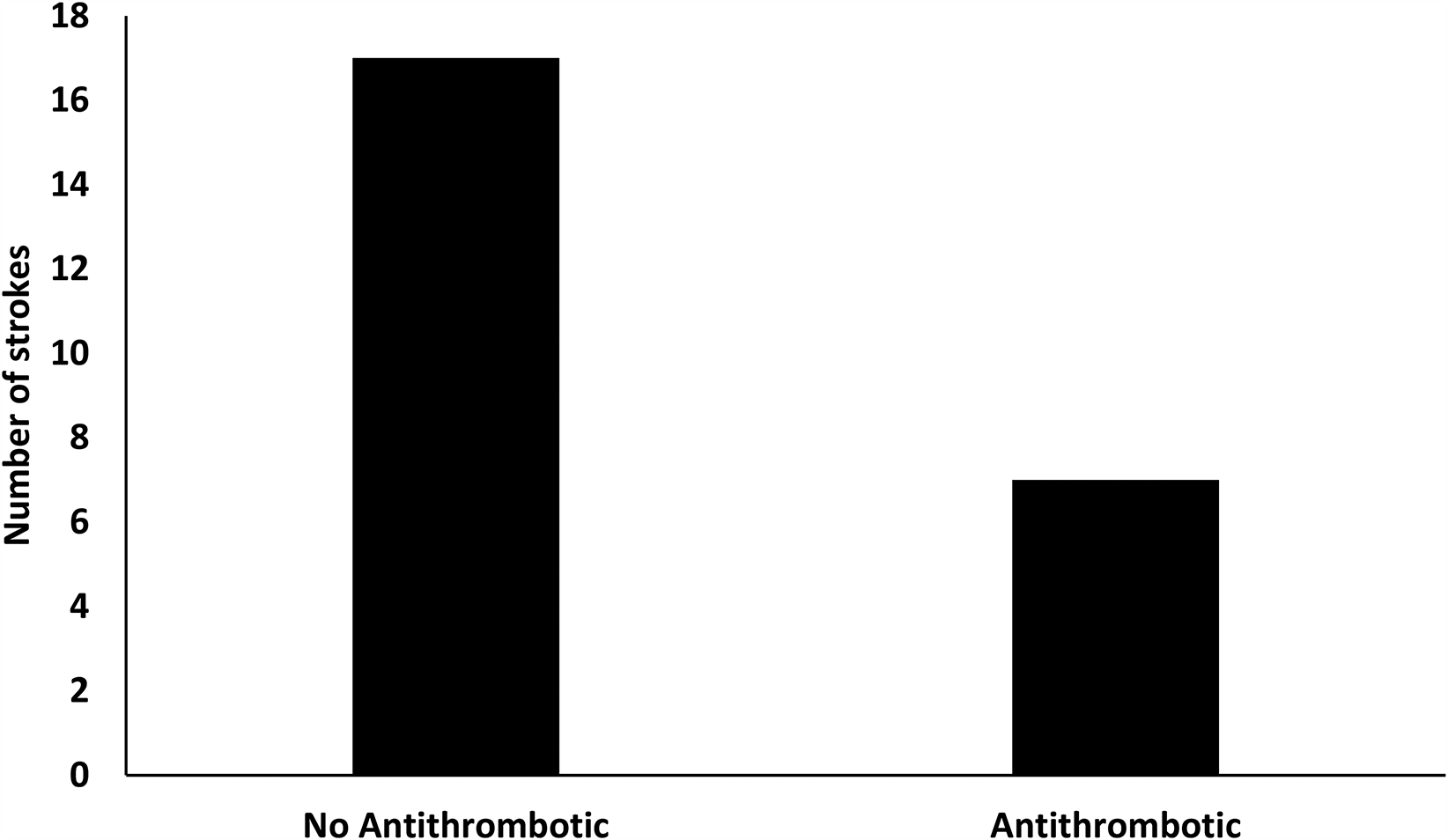
The effect of no anti-thrombotic treatment versus on-treatment on stroke outcomes.
Discussion
Despite a low contemporary incidence of BCVI in trauma patients, 1 our study shows that the overall incidence of inpatient or post-acute hospital admission IS in BCVI patients was not uncommon, at 9.8%. The risk of IS was highest in the first 72 h. Blunt cerebrovascular injury-related stroke rates have been reported in the literature as up to 25%4,5,18,19,24–29 but typically include strokes occurring after injury but prior to presenting to hospital. In keeping with previously published results,22,30,31 at our centre, the rate of inpatient IS in patients not treated with anti-thrombotic medication was 28% compared to 3.6% in patients treated with anti-thrombotics. Overall, our results highlight the increased acute risk of inpatient IS in BCVI patients, particularly in patients not treated with anti-thrombotic medication.
The underlying mechanism of IS in BCVI patients is complex. The sudden acceleration-deceleration movement due to blunt trauma can cause intimal tear and dissection of the cervical arteries.11,21,32 Vertebral fractures seem to confer high risk of such injuries due to the close anatomical proximity of these vessels.32–34 Intimal tearing promotes intramural haematoma, vessel stenosis or occlusion and pseudoaneurysm formation.17,35 An in situ thrombogenic process can then develop after BCVI, due to direct activation of platelets, platelet aggregation and local stasis. 36 Subsequently, IS occurs either via hemodynamic compromise or artery-to-artery thromboembolism.7,37 This is not exclusive however, as other mechanisms can also co-exist. Polytrauma is a prothrombotic and hypercoagulable condition 38 and thus systemic thrombosis risk can concurrently increase. Polytrauma can also promote other thrombotic risk factors including cardiac arrhythmias and plaque rupture.
Our study identified several factors that are more commonly associated with the risk of inpatient IS. For example, severe trauma, lower GCS and rib fractures are all seemingly associated with an increased likelihood of inpatient IS. While VAIs are a more common occurrence, CAIs are more commonly associated with IS, likely reflecting the compensatory collateral supply of the posterior circulation. Not surprisingly, higher grade BCVIs are associated with the increased number of strokes. Similar results have been reported before.15,39
Our results reaffirm previous reports that anti-thrombotic therapy is associated with reducing inpatient IS incidence than conservative management. 30 Among treatment choices, anti-platelet therapy clearly shows reduced IS rates however due to small size, a comparison with anti-coagulation is not possible. Anti-platelets may be better suited in preventing IS in BCVI patients due to its direct role in preventing platelet activation and aggregation. Several publications have found anti-platelets to be better than or equivalent to anti-coagulation in preventing BCVI-related IS5,20,26,40 and associated with reduced haemorrhagic risks.21,41 Anti-platelet therapy is the first-line treatment in our institution and anti-coagulants are generally used when there is another concurrent indication such as pulmonary embolism or evidence of propagating thrombus.
There are several limitations in the current study. Firstly, this is a single centre, retrospective, cohort study and thus contains inherent error and bias related to this. Secondly, it is not always possible to establish a direct causative effect of BCVIs to IS 37 and associations obviously do not imply causation. However, supportive findings can be derived from our study. For example, similar to previous studies, a higher degree of vessel wall damage as measured by Biffl grading, was seen with an increased number of IS suggesting a direct relationship between BCVIs and IS. The number of IS was also lower in patients who were on anti-thrombotic treatment suggesting a therapeutic effect. Another limitation is the lack of data from the non-BCVI trauma population admitted concurrently and hence a direct control comparison was not possible. Finally, most of our results, such as individual treatment effects, did not reach statistical significance, primarily reflecting the small sample size.
Conclusion
In summary, BCVIs are associated with the increased risk of inpatient IS, particularly in the first 72 h after admission. Early treatment initiation with anti-thrombotic therapy may reduce the incidence of strokes; however, commencing treatment can be challenging if there is a competing ongoing bleeding risk due to other trauma. The presence of high-risk factors including high ISS, low GCS and high-grade BCVIs may assist clinicians in their estimates of individualised risk to benefit in anti-thrombotic prescribing decision-making in patients with BCVI.
Footnotes
Contributorship
GC, MF, JM and AM devised the study and design. WZ, VS, TR and NN collected and organised the data. AM and BP analysed and reported the neuroimages as blind assessors. VS wrote the initial draft of the manuscript and all the authors edited the manuscript. ZC assisted with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.