
Abstract
Lumbar artery pseudoaneurysms are a rare complication of penetrating trauma that can result in devastating retroperitoneal hemorrhage or embolic complications if left untreated. Prompt recognition in the trauma setting can lead to timely definitive diagnosis via spinal angiography and treatment via endovascular embolization. We present a case of lumbar artery pseudoaneurysm secondary to a gunshot wound to the spine treated via coil embolization.
Introduction
Lumbar artery pseudoaneurysms are rare vascular complications of penetrating trauma, with only a few cases reported in existing literature.1,2 However, if undiagnosed, lumbar artery pseudoaneurysms can lead to devastating hemorrhages. This case study aims to add to the body of literature on pseudoaneurysms secondary to lumbar spinal penetrating injury. This report describes, with the patient's permission, a 22-year-old male who developed a lumbar artery pseudoaneurysm secondary to a gunshot wound (GSW) through the L2 vertebral body.
Case report
A 22-year-old male arrived at the trauma bay following a single GSW to his lower back just left of the midline. He had no movement in bilateral lower extremities with a T12 sensory deficit and no rectal tone, consistent with a T12 American Spinal Injury Association (AISA) Impairment Scale class A traumatic spinal cord injury (TSCI).
X-rays of the abdomen showed bullet shrapnel over the L2 vertebral body (Figure 1) and X-rays of the pelvis showed no acute fracture or dislocation. Computed tomography (CT) of the abdomen and pelvis with contrast completed in the trauma bay demonstrated a bullet trajectory through the spinal canal with bone and bullet fragments in the vertebral body of L2, anterior to the L2 vertebrae, within the spinal canal, and in the posterior spinal column and soft tissue of his back. There was injury to anterior, middle, and posterior columns of L2, as well as comminuted fracture of the L1 spinous process (Figure 2(a) and (b)). There was no abdominal viscus injury or injury to the descending aorta or inferior vena cava noted on imaging. Contrasted sequences noted a focus of hyperattenuation posterior to the L2 vertebral body, concerning for contrast extravasation, or possibly a small pseudoaneurysm (Figure 2(c)). Acute neurosurgical intervention was not deemed necessary given the patient had an ASIA A neurological injury, no evidence of mechanical instability, and was hemodynamically stable with no definitive evidence of a vascular injury. The patient was admitted to the neurological intensive care unit and managed with pain medication, wound care, and hemodynamic monitoring pending planned repeat vascular imaging.
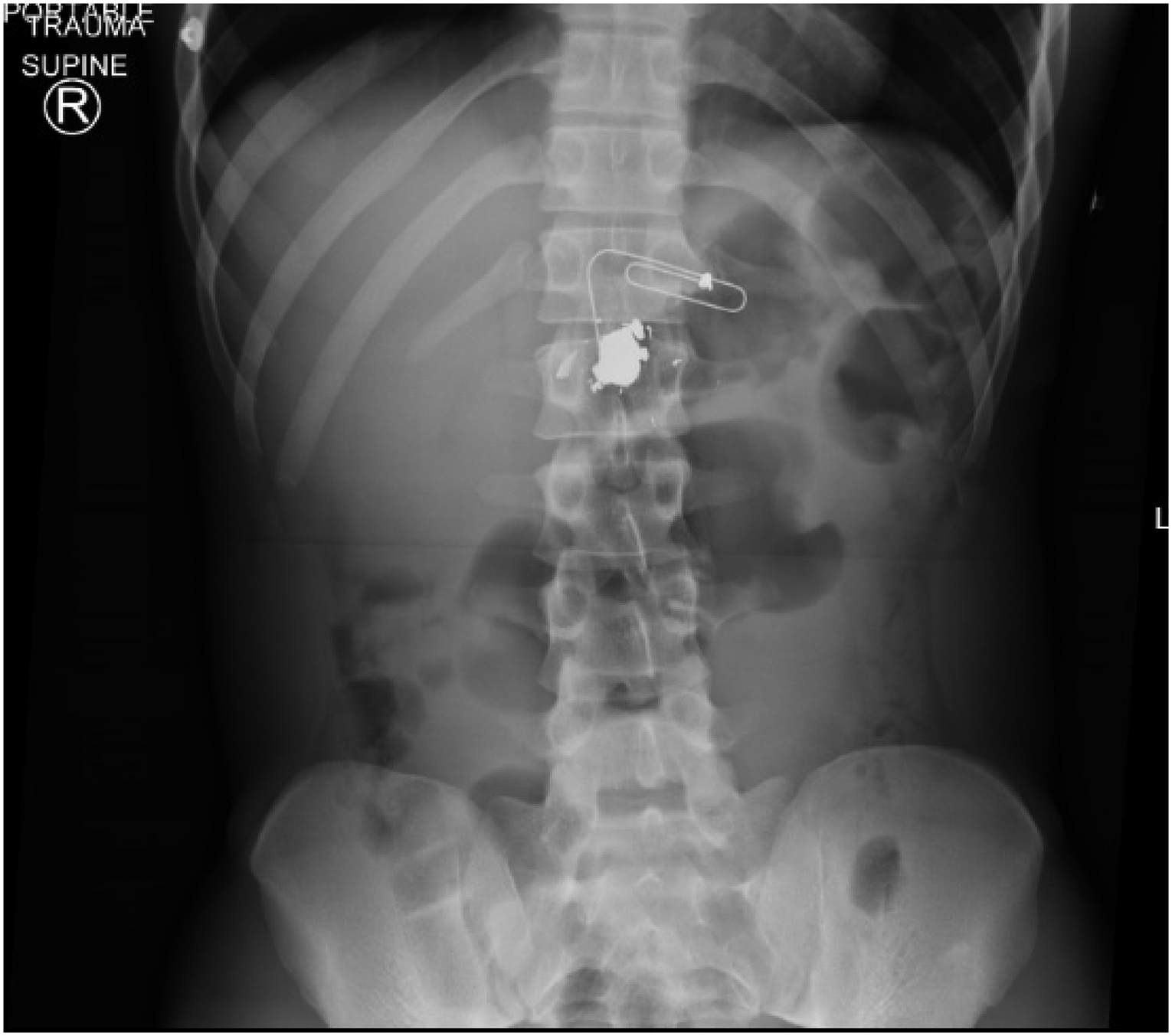
Abdominal radiograph showing AP view of fragmented bullet lodged in L2 vertebral body. The paperclip is placed externally to designate a bullet entry/exit wound during the primary survey.
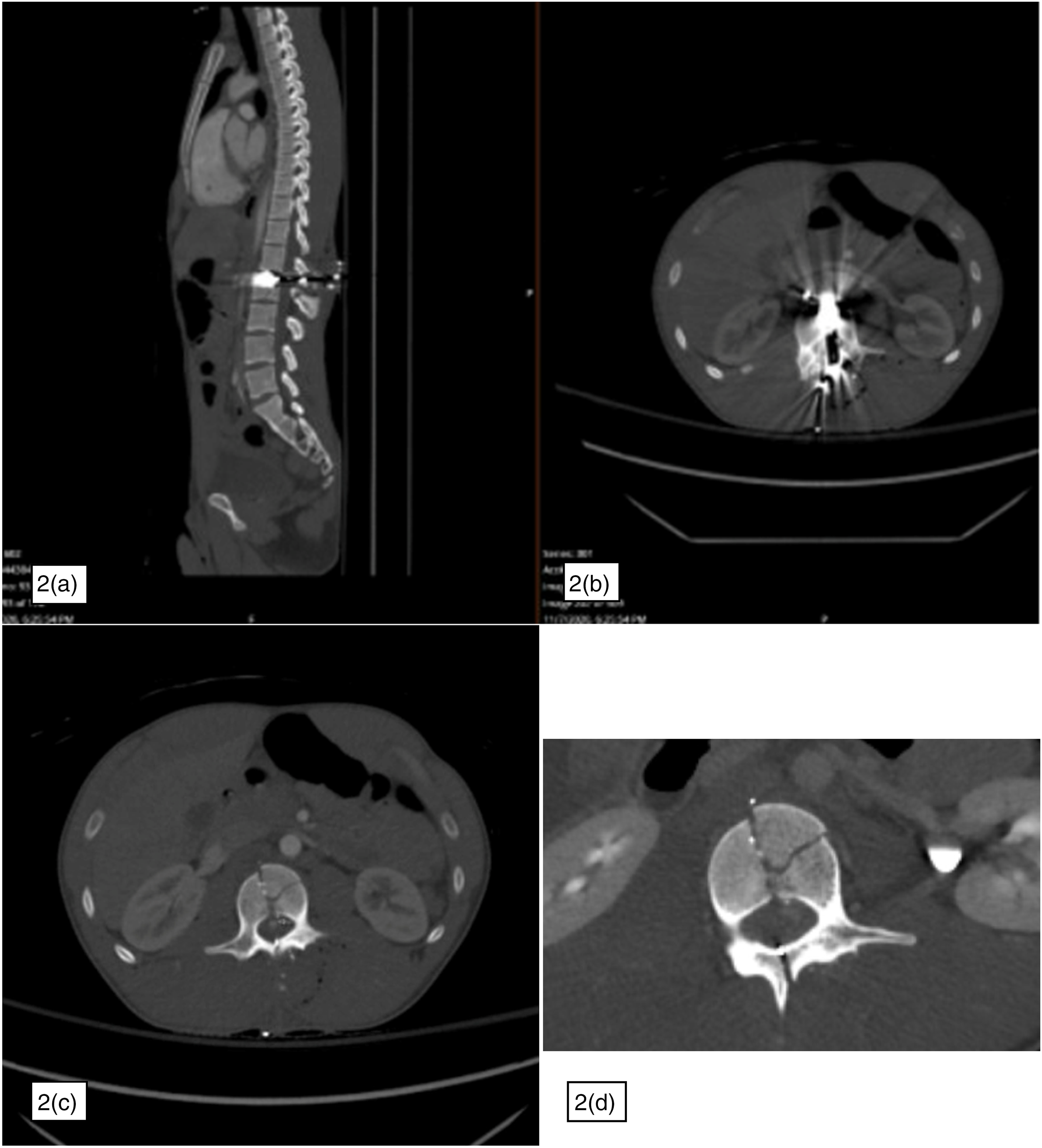
CT A/P with sagittal (a), and axial (b) cuts revealing bullet fragments in the vertebral body of L2, anterior to the L2 vertebrae, in the spinal canal, and in the posterior spinal column and soft tissue of his back. Also seen is a multi-column L2 fracture and comminuted fracture of the L1 spinous process. Contrasted imaging (c) reveals a focus of hyperattenuation posterior to the L2 vertebral body, initially concerning for contrast extravasation versus pseudoaneurysm. Follow-up CT 4 days later (d) reveals enlargement of the pseudoaneurysm.
Repeat CT angiography (CTA) was performed 4 days after presentation to re-evaluate the possible pseudoaneurysm, and revealed that the hyperattenuating focus posterior to the L2 vertebral body appeared larger compared to the prior study, and was visible on both arterial phase and delayed phase imaging, concerning for an enlarging pseudoaneurysm (Figure 2(d)). Given the short interval enlargement, the patient was planned for spinal angiography and embolization.
The following day, a spinal angiogram was performed, revealing a 7 mm pseudoaneurysm at the level of L2 supplied by collateral vessels arising from the left L3 segmental artery, and occlusion of the left L2 segmental artery (Figure 3(a)). The pseudoaneurysm was treated with transcatheter deployment of microcoils in the distal left L3 segmental artery just at its bifurcation, as well as particles injected at the mid-portion of the left L3 segmental artery after an HS1 catheter was guided to the left L3 segmental artery origin, and a construct of an SL-10 microcatheter was navigated over a Synchro-2 microwire into the arterial trunk. Post-embolization angiography showed resolution of the previously seen L2 pseudoaneurysm (Figure 3(b)). Interval CT imaging showed continued resolution of the pseudoaneurysm 5 days post-op. The patient progressed well with pain control and after working with physical therapy, inpatient acute rehabilitation was recommended. The patient was discharged to rehab on post-procedure day 7.
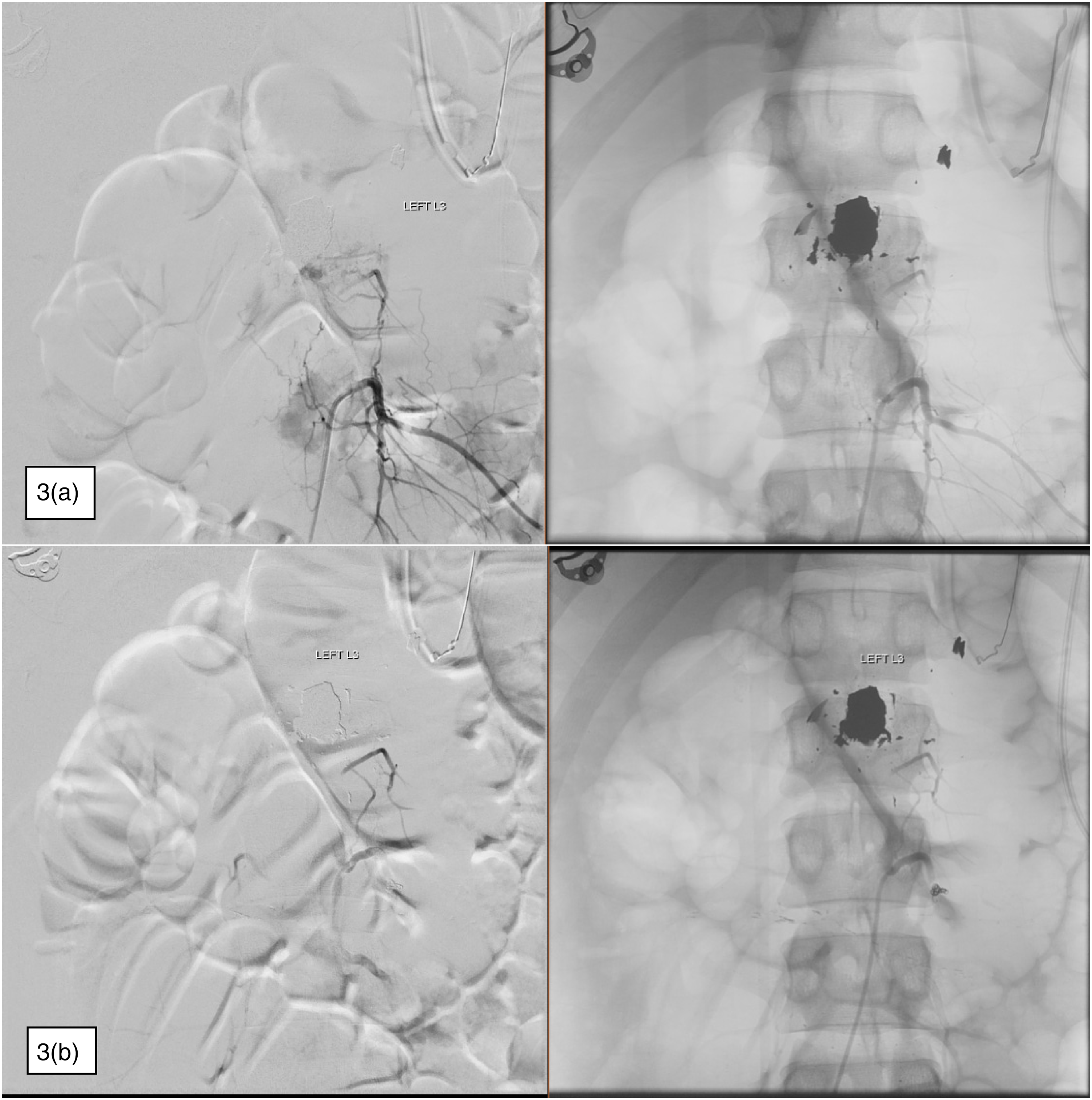
Spinal angiography with selection of spinal segmental arteries. (a) Collateral vessels fed by the left L3 segmental artery (selected in this sequence) that supply a 7 mm pseudoaneurysm at the level of L2. (b) Injection of the left L3 segmental artery after deployment of coils and particles showing no filling of the pseudoaneurysm.
Discussion
Pseudoaneurysms make up less than 1% of aneurysms and are characterized by a disruption of the arterial wall that allows blood to escape into surrounding tissues forming a hematoma that is in continuity with the lumen of the parent vessel. 3 The uninjured portion of the arterial wall prevents the vessel from constricting, resulting in fibrin forming around the swelling that can rupture.3,4 Common treatment options include ligation, resection, and endovascular embolization. 5 Open surgical treatment was traditionally first-line management, but this approach requires exposure and thereby risk to neural elements, and locating both the lesion and its feeding vessels can be challenging.6–9 The preferred treatment has since become transcatheter embolization, as it can diagnose and treat pseudoaneurysms in a safe and minimally invasive manner.1,9–11 Pseudoaneurysms most often occur secondary to blunt trauma, commonly from sports-related injuries, fractures, and accidents. 3 Pseudoaneurysms secondary to penetrating injuries are less common but have been described in the literature.3,12–14
Lumbar artery pseudoaneurysms secondary to penetrating trauma are rare, and most commonly are iatrogenic secondary to lumbar surgery or interventional procedures. 1 Specifically, lumbar artery pseudoaneurysms from penetrating injuries have been observed in patients presenting with GSWs, stab wounds, and fractures.1,6,7,10,11,15,16 To the best of our knowledge, only three other lumbar artery pseudoaneurysm cases secondary to GSWs have been reported.1,17,18 Lumbar artery pseudoaneurysms are important to diagnose and treat early as they can expand or rupture, causing morbidity or mortality from hemorrhage, thrombosis, or embolic complications. 6 Hemorrhages from lumbar segmental arterial bleeds that are left untreated can lead to fatal retroperitoneal hemorrhage. 1
Our patient was diagnosed and treated within five days of presenting to the trauma bay, and suffered no complications secondary to the pseudoaneurysm. Although this case highlights the importance of early detection, lumbar artery pseudoaneurysms are difficult to diagnose because of the rarity of the condition, delayed onset of clinical presentation, and non-specific symptoms such as lower back pain.1,6 In this case, interval imaging was vital to an accurate diagnosis and decision to treat. On initial imaging, the possible pseudoaneurysm was small, and evaluation was limited secondary to streak artifact from the retained bullet; however, the repeat study showed clear growth of the well-circumscribed enhancing segment with maintained visualization and an increase in size from arterial through delayed phase contrasted imaging, consistent with an enlarging pseudoaneurysm.
Clinical presentations of lumbar artery pseudoaneurysms can vary, with some patients remaining asymptomatic; however, the most common symptom is pain, caused by the pseudoaneurysm either rupturing or stretching the surrounding nerves. 10 Patients usually present with non-specific lower back, flank, and/or abdominal pain.1,6,7,10,11,15,16 Chan et al. reported a 24-year-old man with a lumbar spinal cord injury secondary to a GSW who developed a lumbar pseudoaneurysm. The patient developed lower back and flank pain during inpatient rehabilitation, but his symptoms were initially attributed to musculoskeletal injury from the GSW and later an intra-abdominal abscess. 1
Conclusion
Lumbar artery pseudoaneurysms should be treated urgently due to risk of life-threatening complications such as retroperitoneal hemorrhage, with no clear correlation between pseudoaneurysm size and rupture risk. CTA should be obtained initially for detecting lumbar artery pseudoaneurysms and other vascular injuries in these patients. If, as in our patient, there is an identified pseudoaneurysm or if there remains a high clinical index of suspicion, angiography should be pursued, which can provide a definitive diagnosis and prompt method of treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
YK, DR, JG, MS, SA, RB, DK, and JS researched literature and conceived the study. YK, DR, JG, and MS were involved in protocol development and gaining patient consent. YK wrote the first draft of the manuscript. JG and MS wrote subsequent drafts of the manuscript and evaluated patient imaging and clinical findings. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.