
Abstract
Background
A better understanding of how chronic physical health conditions affect long-term outcomes following injury is essential for quantifying the burden of serious orthopaedic injuries. We aimed to describe the association between the presence of post-injury chronic physical health conditions and (i) the change in health status from before injury to six different follow-up time points after injury; and (ii) survival time.
Methods
A cohort study was conducted using linked data from the REcovery after Serious Trauma: Outcomes, Resource Use, and Patient Experiences study, the Victorian Registry of Births, Deaths and Marriages (BDM) (2009–2017), the victorian admitted episodes dataset (2009–2017) and the victorian emergency minimum dataset (2009–2017). Adults (≥ 18 years old) with serious orthopaedic injuries who survived to discharge from their trauma admission were included. Multivariable linear regression analysis was conducted to evaluate the association between post-injury chronic physical health conditions and the mean change in health status (EuroQol-Visual Analogue Scale) from before injury to six follow-up time points post-injury. Survival analysis was conducted to estimate the probability of survival for people with and without chronic physical health conditions following injury.
Results
Out of 894 participants, 177 (19.8%) had at least one chronic physical health condition recorded up to five years post-injury. People with post-injury conditions reported a greater mean decline in health status than people without post-injury conditions (difference, (95% CI): −6.9 (−9.7, −4.2), p = 0.01). Over the study period, almost six times as many people with chronic physical health conditions post-injury died as people without these conditions (AHR (95% CI): 5.7 (2.9, 11.3), p < 0.01).
Conclusions
Chronic physical conditions after serious orthopaedic injuries were associated with a lower survival probability and a deteriorating health status. Orthopaedic injury survivors may benefit from early detection and treatment of chronic conditions.
Introduction
Serious orthopaedic injury is one of the leading causes of mortality and morbidity.1,2 People with serious orthopaedic injuries have a high prevalence of chronic physical health conditions including cancer, cardiovascular disease (CVD), type 2 diabetes (DM), and hypertension. 3 Chronic conditions may hinder the recovery process,4,5 and may increase mortality risk following injury. 6
Previous studies have demonstrated that chronic conditions are associated with poorer long-term outcomes following injury.7,8 These studies, however, have only looked at pre-existing chronic conditions, rather than conditions that develop after injury.9,10 Furthermore, few have focussed solely on serious orthopaedic injury.11,12 As such, there is a lack of information specific to this population.
Understanding the link between new-onset chronic conditions and long-term health outcomes post-injury will have implications for both clinical practice and future research. Therefore, in people with serious orthopaedic injuries, we aimed to describe: (i) the association between the presence of post-injury chronic physical health conditions and the change in health status from before injury to six follow-up time points (six months, one, two, three, four, and five years) after injury; and (ii) the association between the presence of post-injury chronic physical health conditions and survival time.
Methods
Study design
We conducted a cohort study using linked data from the REcovery after Serious Trauma Outcomes, Resource Use and Patient Experiences (RESTORE) study, the Victorian Registry of Births, Deaths and Marriages (BDM) (2009–2017), the Victorian Admitted Episodes Dataset (VAED) (2009–2017) and the Victorian Emergency Minimum Dataset (VEMD) (2009–2017).
Data sources
The RESTORE study was a population-based longitudinal cohort study using quantitative and qualitative methods to capture outcomes and experiences of seriously injured people from the Victorian State Trauma Registry (VSTR) up to five years post-injury. 13 Victorian State Trauma Registry is a population-based registry that collects information about major trauma patients from all trauma-receiving hospitals in the Australian state of Victoria (population 6.4 million) to monitor and evaluate trauma care.14,15 Patients are included in the VSTR if they meet any one of the following criteria: death after injury; an Injury Severity Score >12; admission to an intensive care unit for >24 h and requiring mechanical ventilation for at least part of their stay; or requiring urgent/emergency surgery.15,16 People with a date of injury between July 2011 and June 2012 were included in the RESTORE study. The RESTORE dataset included participants’ demographics, injury events, diagnosis, treatment, in-hospital outcomes, and patient-reported outcome data from the six-month, one-, two-, three-, four- and five-year follow-up surveys.
The VAED contains de-identified data on hospital admissions for admitted patients in all Victorian public and private hospitals, including rehabilitation centres, extended care facilities and day procedure centres. 17 The VEMD contains de-identified demographic, administrative and clinical details from emergency presentations at all Victorian public hospitals with designated emergency departments (EDs). 18 The Victorian Registry of BDM records births, deaths, marriages and adoptions of all people in Victoria.
Data linkage process
The RESTORE dataset was first linked to data from the Victorian BDM to establish if any patient had died following injury. Dates of death were extracted from the Victorian BDM if not available in the RESTORE study dataset. This combined dataset was provided to the Centre for Victorian Data Linkage (CVDL) at the Department of Health for linkage with data from the VAED and VEMD. 19 Hospital admissions and ED presentations were linked for each RESTORE participant for the two years prior to, and up to five years after their VSTR admission (Figure 1). Data were linked using probabilistic methods based on identifiers such as first name, surname, birth date and sex, using ‘fuzzy matching’ on the name to achieve a higher linkage rate than exact matching. 20 The linkage rate was 97.8%. Ethical approval for the linkage was provided by the Victorian Department of Health and Human Services Human Research Ethics Committee (DHHS HREC) and participating health service ethics committees.
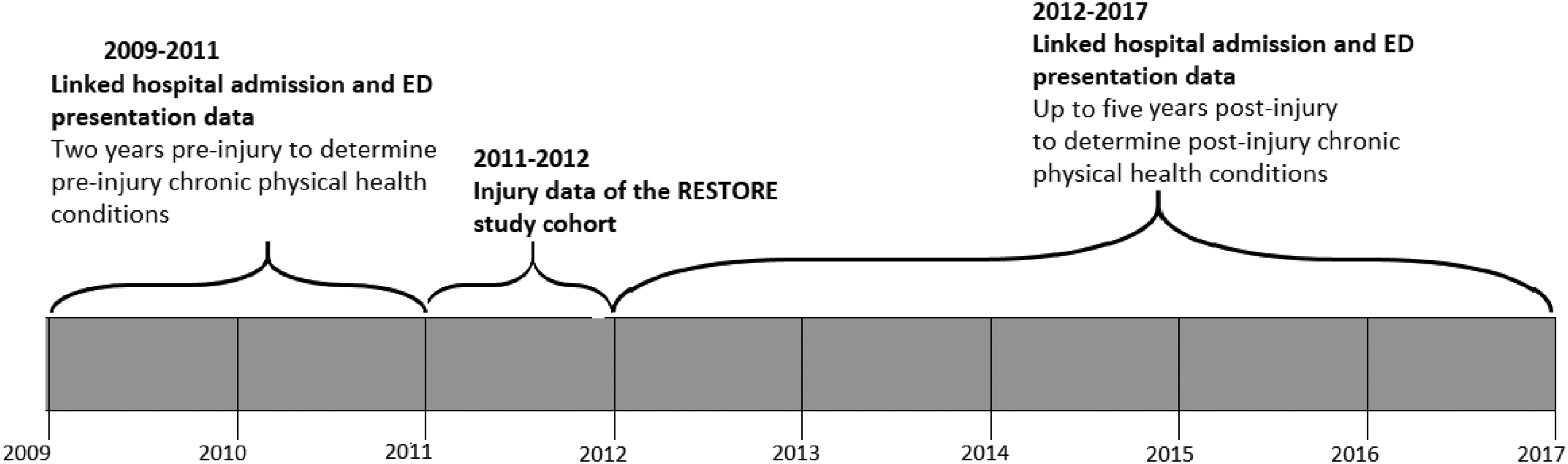
Timeline of the data and time periods required for the analysis of chronic physical health conditions following serious orthopaedic injury.
Study participants
Adults (≥ 18 years old) with serious orthopaedic injuries from RESTORE who survived to discharge from their trauma admission were included in this study. Serious orthopaedic injury was defined as a traumatic injury that resulted in at least one fracture and met the VSTR inclusion criteria.21,22 People with neurotrauma (spinal cord injury or severe traumatic brain injury (AIS score of ≥ 3 in the spine or head region)) or burns were excluded.
Exposure
Chronic physical health conditions are defined as any condition expected to result in the long-term or ongoing deterioration of an individual's physical health. 23 Post-injury conditions were defined as those identified within the VAED or VEMD datasets up to five years after injury that had not been identified in the two years prior to injury (within the VAED or VEMD), nor at the time of injury (within the VSTR). Indicator variables for conditions of interest were mapped from the International Classification of Diseases, 10th Edition, Australian Modification (ICD-10-AM) diagnosis codes and relevant procedure codes from the Australian Classification of Health Interventions (ACHI)-Tenth Edition. Conditions included in the study were arthritis and arthropathies, cancer (all types), cardiovascular disease, chronic kidney disease, chronic pulmonary disease, type 2 diabetes, hypertension, obesity, Alzheimer's disease and vascular dementia. Cardiovascular disease (CVD) includes atherosclerosis, chronic heart failure, ischaemic heart disease, myocardial infarction, peripheral vascular disease or stroke. The methodology for identifying chronic physical health conditions was developed based on research by Tonelli et al. 24 The VAED ICD-10-AM prefix classifies conditions as a principal diagnosis, complication or comorbid diagnosis, while VEMD ICD-10-AM codes indicate primary diagnoses only. This study included principal diagnoses from the VAED and primary diagnoses from the VEMD. The presence of post-injury chronic physical health conditions (yes/no) was determined at six follow-up time points (six months, one, two, three, four and five years) post-injury.
Procedures
Participants’ demographic information (age, sex, level of education, and socioeconomic characteristics), pre-injury health and disability status, injury event details (cause, place, and intent of injury), Injury Severity Score (ISS) 25 and compensation status were obtained from the linked dataset. The ISS was categorised into tertiles for analysis (ISS < 17, ISS = 17–24, ISS > 24). Self-reported pre-injury disability (yes/no) was derived from a five-category global disability rating scale. 26 Indicators for pre-injury mental health conditions, alcohol and drug-related conditions and smoking status were mapped from ICD-10-AM diagnosis codes from pre-injury hospital admissions/ED presentations and trauma admissions. Residential postcodes were mapped to the Accessibility/Remoteness Index of Australia (ARIA), 27 and the Index of Relative Socio-economic Advantage and Disadvantage (IRSAD), which ranks areas in Australia according to relative socio-economic advantage and disadvantage. 28 Deciles of the IRSAD were collapsed into quintiles. Transport and work-related injuries in Victoria are covered by no-fault compensation schemes regulated by the Transport Accident Commission and the Victorian Workcover Authority respectively.29,30
Outcomes
The change between pre- and post-injury health status at six months, one, two, three, four and five years was measured respectively. Pre- and post-injury health status was measured using the EuroQol-Visual Analogue Scale (EQ-VAS). 31 To complete the pre-injury EQ-VAS, study participants were asked the following question: ‘How would you say your health was prior to your injury on a scale of 0–100, with 0 being the worst imaginable health state and 100 being the best imaginable health state?’ To complete the post-injury EQ-VAS, participants were asked the same question, relating to that point in time. Both pre-and post-injury EQ-VAS scores were collected by trained telephone interviewers within the VSTR at six months, one, two, three, four and five years post-injury. The change in health status (EQ-VAS) from pre- to post-injury was calculated by subtracting the pre-injury EQ-VAS from post-injury EQ-VAS for each follow-up period, with a negative value indicating a decline in health status. To address the second aim, we determined survival time by subtracting the date of injury from the date of death, summarised in years.
Data analysis
Descriptive statistics were used to summarise participants’ baseline characteristics. Frequencies and percentages were used to characterise categorical variables. For continuous variables, the mean and standard deviation (SD) were calculated for normally distributed data and median and interquartile range (IQR) for skewed data.
To describe the mean change in health status by post-injury chronic condition status at each time point, we fitted a linear regression model with an interaction between time and outcome. We used a clustered sandwich estimator for the standard errors to account for the repeated EQ-VAS scores reported by each participant. 32 The estimates were then standardised to the sample mean and proportion for the following potential confounders: age, sex, pre-existing health conditions (identified in the two years prior to injury or at the time of injury), pre-injury EQ-VAS score, EQ-VAS score at previous time points (for example, 6months and one year for two-year outcome), pre-injury disability, pre-injury smoking status, pre-injury drug and alcohol-related conditions and mental health conditions. 33 These variables were selected because they have previously been identified as being associated with the health status of people with serious orthopaedic injuries.34,35
To estimate the association between post-injury chronic conditions (yes/no) at each follow-up time point (e.g. up to two years post-injury) and the mean change in health status at that time point, we fitted a multivariable linear regression model. 36 The estimate of the association was adjusted for the potential confounders listed prior. By inspecting variance inflation factors (VIFs), we identified no collinearity between post-injury chronic physical health conditions and other variables (mean VIF = 2). The homogeneity of variance was graphically tested. Because the pre-injury EQ-VAS values were missing in 9.95% of the study participants, we conducted a sensitivity analysis to investigate if the qualitative interpretations of our study findings changed as a result of the missing pre-injury EQ-VAS data. By comparing the association between chronic physical health conditions and post-injury EQ-VAS to the association between chronic physical health conditions and changes in pre- to post-injury EQ-VAS, we determined if the results were influenced by missing data or the pre-injury adjustment.
Survival analysis was conducted to estimate the survival probability of people with and without post-injury chronic conditions. The exposure (chronic physical health conditions) was treated as time-varying because the percentage of people with post-injury chronic physical health conditions changed from the ‘no chronic physical health condition’ group to the ‘yes’ group over the five-year period. 37 Participants were followed from the date of injury up to five years post-injury, and were considered censored if still alive at five years. The association between post-injury chronic physical health conditions and survival following serious orthopaedic injury was described with a proportional hazards ratio, estimated using a multivariable Cox proportional hazards model, adjusted for baseline factors: age, sex, pre-injury physical health conditions, pre-injury mental health conditions, smoking, drug and alcohol-related conditions and IRSAD.37,38 These variables were selected because they have previously been identified as being associated with mortality among people with serious orthopaedic injuries.34,35 The Cox proportional hazards assumption was assessed by inspecting the log-minus-log plots (log-log survival time against the log analysis time).39,40
Results
Overview of study participants
There were 2941 people with major trauma included in the RESTORE project, of whom 894 met the inclusion criteria (Figure 2). Most (70.7%) participants were male, and the median (IQR) age and ISS were 53 (36–66) years and 30 (25–43), respectively (Table 1).
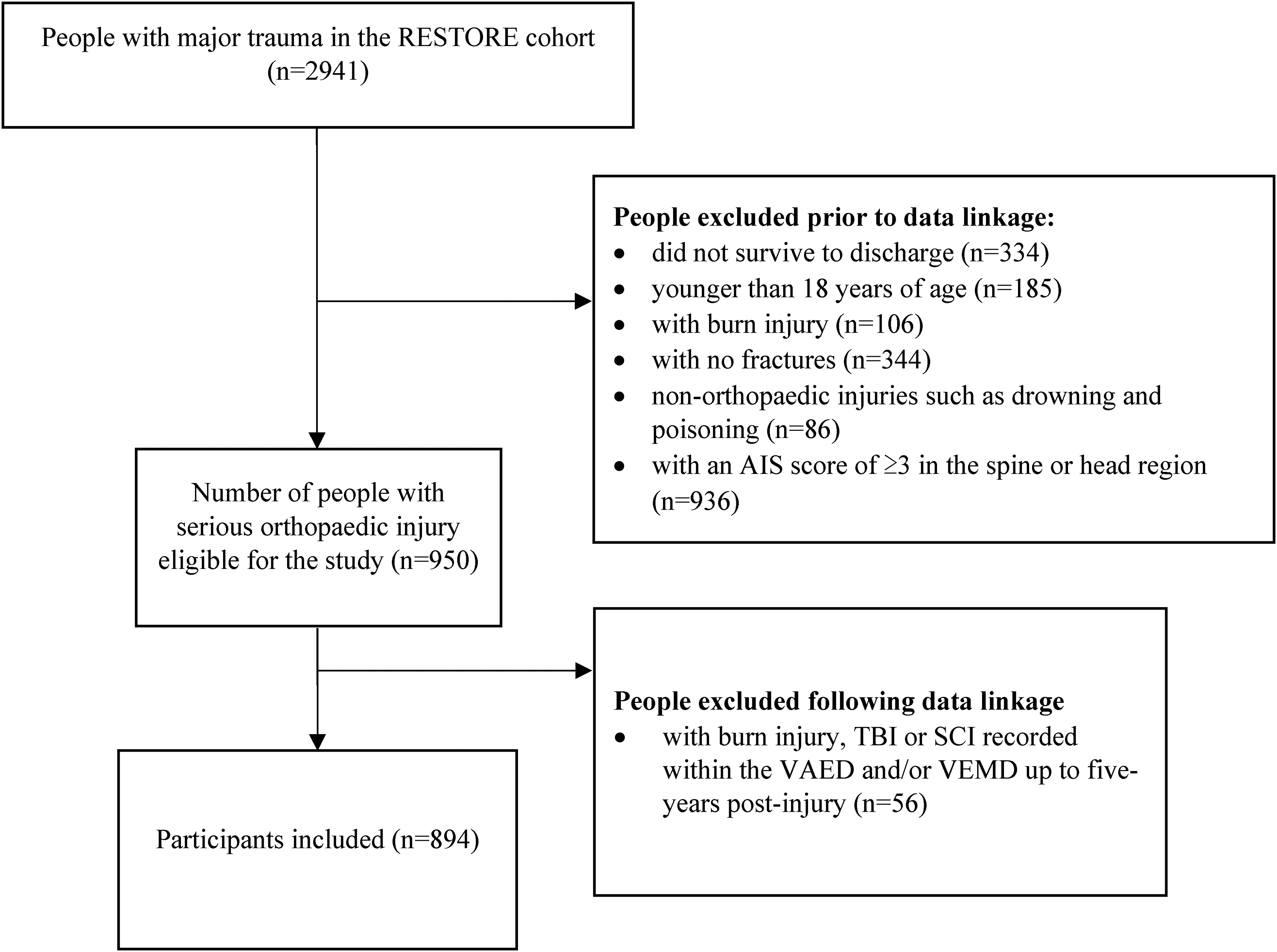
Flow diagram depicting selection of study participants.
Baseline characteristics of study participants (N = 894).
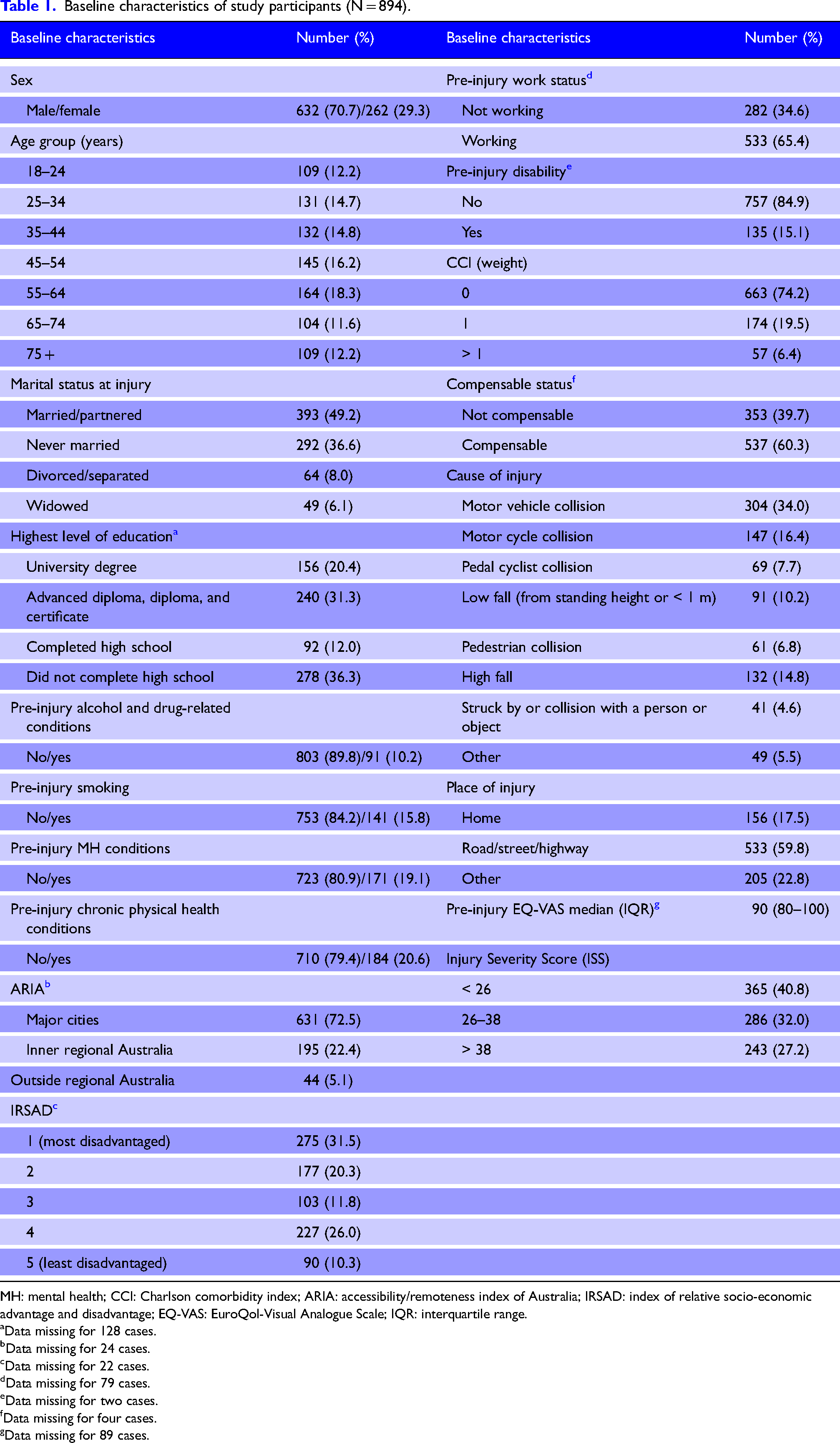
MH: mental health; CCI: Charlson comorbidity index; ARIA: accessibility/remoteness index of Australia; IRSAD: index of relative socio-economic advantage and disadvantage; EQ-VAS: EuroQol-Visual Analogue Scale; IQR: interquartile range.
Data missing for 128 cases.
Data missing for 24 cases.
Data missing for 22 cases.
Data missing for 79 cases.
Data missing for two cases.
Data missing for four cases.
Data missing for 89 cases.
Post-injury chronic physical health conditions in people with serious orthopaedic injury
Figure 3 shows the percentage of people with and without post-injury chronic physical health conditions. There were 177 people (19.8%) with at least one post-injury chronic physical health condition up to five years after injury. The proportion of people with serious orthopaedic injuries admitted to hospital/presented to ED with each type of condition up to five years post-injury is presented in Supplemental Material 1.
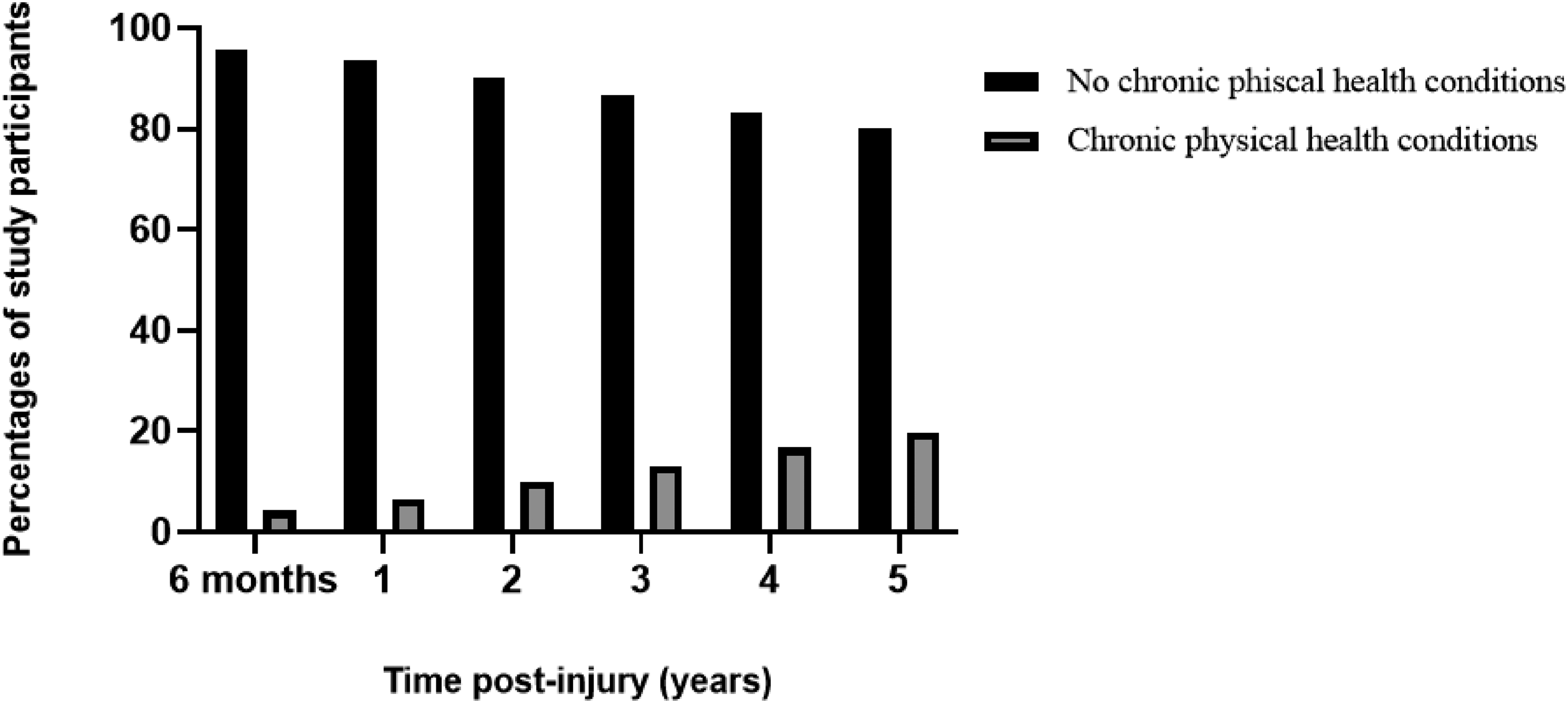
The cumulative distribution of post-injury chronic physical health conditions in people with serious orthopaedic injury up to five years post-injury.
Changes in pre- to post-injury health status
Figure 4 shows the mean change in health status from pre-injury to various time points post-injury up to five years post-injury. The mean (SD) change in health status of people with no post-injury chronic conditions ranged from −14.9 (22.2) at one year post-injury to −17.3 (22.6) at three years post-injury, representing a decline from pre-injury health status at all time points post-injury. The mean (SD) change in health status of people with post-injury chronic conditions ranged from −18.1 (19.1) at two years post-injury to −23.8 (23.3) at five years post-injury, representing a decline from pre-injury health status at all time points post-injury. People with no post-injury conditions reported less health decline at every time point than people with post-injury conditions. There was a significant difference in health status between people with and without post-injury chronic conditions at five years post-injury.
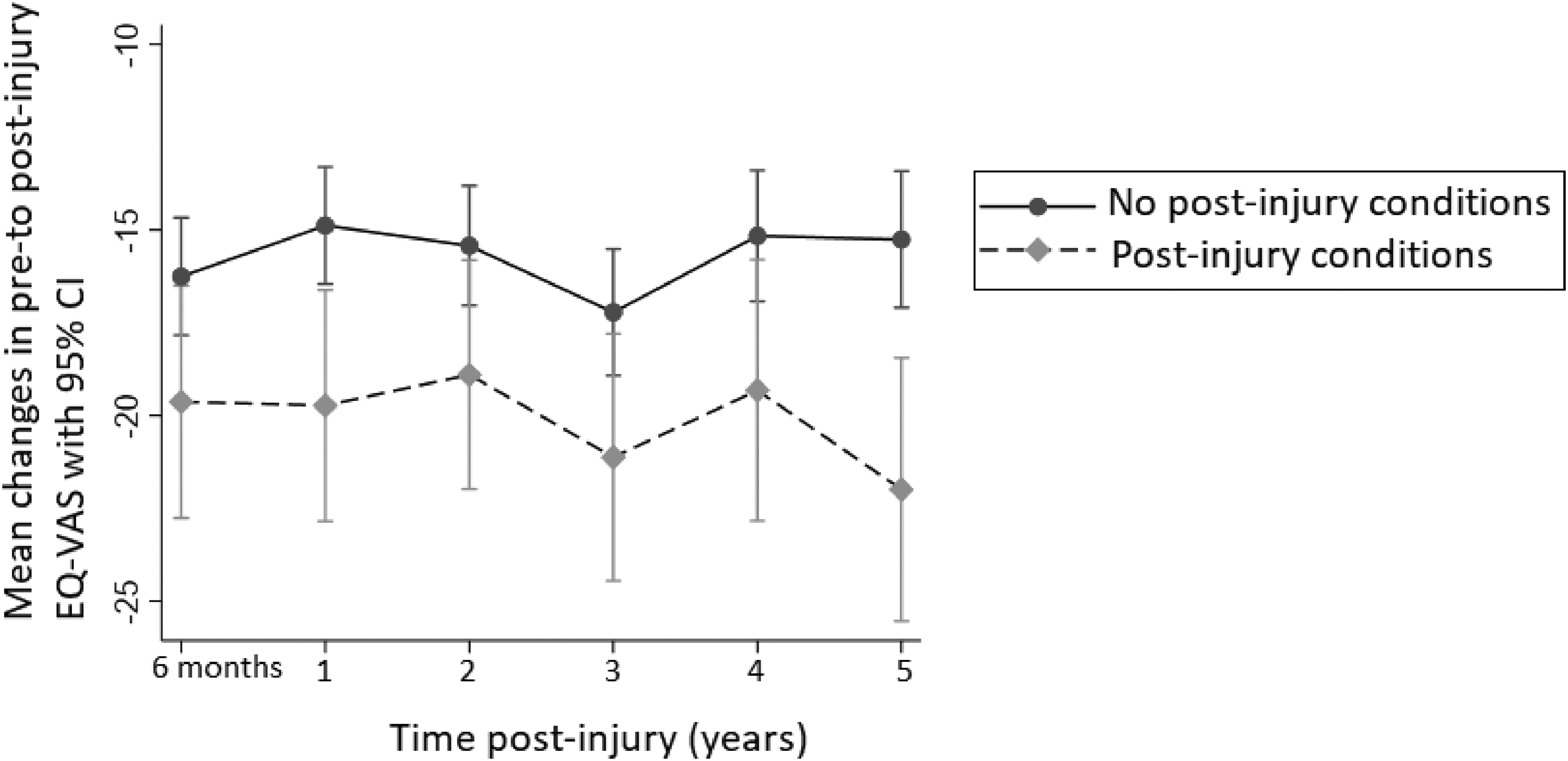
Mean changes in EuroQol-Visual Analogue Scale (EQ-VAS) (health status) from pre-injury to various time points post-injury, up to five years post-injury.
The association between chronic physical health conditions and changes in health status from pre to post-injury
The adjusted association between post-injury chronic physical health conditions (yes/no) and changes in health status is shown in Figure 5. There was no association between post-injury chronic physical health conditions and health status at any time point up to four years after injury. At five years post-injury, the presence of a post-injury chronic physical health condition was significantly associated with a decline in health status. People with post-injury chronic physical health conditions reported a mean decline in health status, 6.9 units greater on the EQ-VAS scale than people without post-injury chronic physical health conditions, after adjusting for confounders (such as age, sex, and socioeconomic status) (difference, (95% CI): −6.9 (−9.7, −4.2), p = 0.01). Supplemental Material 2 provides the adjusted mean difference between post-injury chronic physical health conditions (yes/no) and changes in pre-to post-injury health status). The sensitivity analysis using the alternative outcome resulted in values that were consistent with the main analysis (Supplemental Material 3).
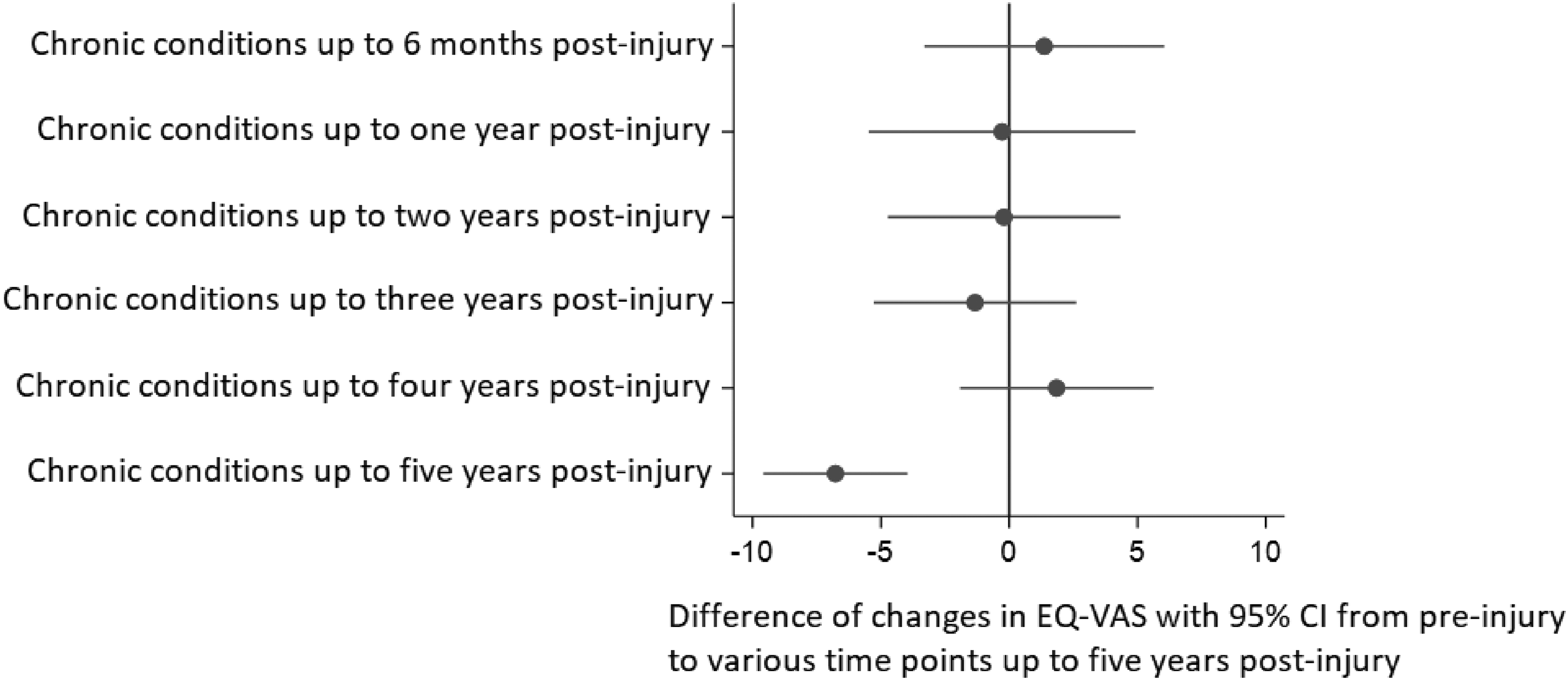
Adjusted association between post-injury chronic physical health conditions (yes/no) and changes in EuroQol-Visual Analogue Scale (EQ-VAS) (health status) from pre-injury to various time points up to five years post-injury: a negative score implies a decrease in post-injury health status.
The association between post-injury chronic physical health conditions and mortality following serious orthopaedic injury
The median (IQR) follow-up period for mortality was 2.6 (1.5–3.5) years. The cumulative mortality up to five years post-injury was 12.4% (95% CI: 10.4%, 14.7%). About 16.9% of people with post-injury chronic physical health conditions, and 11.3% of people without post-injury chronic physical health conditions, had died by five years. The unadjusted Cox proportional hazards regression showed that at any time point during the study period, more than four times as many people with post-injury chronic physical health conditions had died than people without post-injury chronic physical health conditions (AHR (95% CI): 4.2 (2.6, 6.7), p < 0.01). After adjusting for age, sex, pre-injury physical health conditions, pre-injury mental health conditions, smoking, drug and alcohol-related conditions and IRSAD, the Cox proportional hazards regression showed that at any time point during the study period, almost six times as many people with post-injury chronic physical health conditions had died than people without post-injury chronic physical health conditions (AHR (95% CI): 5.7 (2.9, 11.3), p < 0.01).
Discussion
The aim of this study was to describe the association between post-injury chronic physical health conditions and long-term outcomes (health status and mortality) following serious orthopaedic injury. We found that people with post-injury chronic physical health conditions had a poorer long-term health status five years following injury than people without post-injury chronic conditions. A significant association between post-injury chronic conditions and decreased survival probability up to five years post-injury was also observed.
Research indicated that pre-existing conditions are associated with poor long-term health outcomes.7,41 However, until now there was a lack of research on the association between post-injury chronic physical health conditions and long-term outcomes in people with serious orthopaedic injury. There are several possible explanations for the greater health decline observed in people with post-injury chronic conditions.42,43 People with post-injury chronic conditions may have diminished physical and mental resilience to the repercussions of the injury, curtailing their capacity to recover. 43 Negative behaviour changes caused by injury may also lead to the onset of chronic conditions that are linked to a lower health status after an injury. 44 Conditions that may have been present at the time of injury or at the pre-diagnosis level but just not identified, whereby some effects of the condition were present to a minor degree of severity but not yet fully expressed, may also lead to poorer long-term outcomes and recovery following injury. This finding was observed only five years after injury, indicating that chronic physical health conditions develop gradually and need a longer period of time to manifest and have an effect on trauma survivors following injury. As such, long-term follow-up care following a significant orthopaedic injury may be necessary to prevent chronic physical health conditions and to reduce long-term effects.
Another explanation for the link between chronic health conditions and health status following serious orthopaedic injury is that chronic physical health conditions can both contribute to, and be a result of, poor long-term physical and mental health status. 45 For example, people with serious orthopaedic injuries may experience a variety of negative outcomes, including pain, increasing functional impairment, activity limitation, participation restriction and mental illness such as depression, which may be detrimental to their reported health status. Subsequently, not undertaking sufficient physical activity to incur health benefits, such as maintaining appropriate body weight and a healthy musculoskeletal system, could then facilitate the development of chronic conditions.46,47
Our study showed that people with post-injury chronic physical health conditions had a higher mortality rate than people with no post-injury chronic physical health conditions during the follow-up period. Until now, the impact of new post-injury chronic conditions on mortality in people with serious orthopaedic injury was unclear, as previous studies focused only on pre-existing conditions.48,49 For example, a study on the timing and causes of mortality after injury, found that mortality was associated with pre-existing cancer and CVD. 50 Given the evidence of an association between post-injury chronic physical health conditions and mortality after serious orthopaedic injury, it may be necessary to identify people with these conditions and implement treatment strategies to prevent mortality following injury.
The findings of this study have significant implications for understanding how chronic physical health conditions may affect the recovery process of people with serious orthopaedic injuries. Given the prevalence of post-injury chronic conditions and their association with poor long-term outcomes and mortality following injury, people with serious orthopaedic injuries may need to be monitored more frequently and over a greater length of time than people without chronic physical health conditions. Early and regular screening for chronic physical health conditions following serious orthopaedic injury may also be needed to help reduce the risk of mortality and poor long-term health status.
Our findings also have important implications for future research. For example, researchers are recommended to consider post-injury chronic physical health conditions when determining risk for long-term outcomes and mortality. Further research such as prospective studies in which chronic conditions and health status are assessed at a baseline time point and re-assessed over time (up to 10 years) post-injury could help in improving our understanding of the impact of chronic conditions on health status and survival. Further research on which types of chronic physical health conditions have the most influence on long-term outcomes following injury may also be needed to develop targeted interventions to improve outcomes and post-injury recovery.
The primary strength of this study was the long-term (five-year) follow-up of outcomes, enabled by linking the RESTORE dataset with administrative data. Additionally, by using self-reported pre-injury health status data to calculate pre-to-post-injury health status changes, we avoided underestimating the impact of injury upon post-injury health outcomes.
Certain limitations should also be considered. It was not clear from this study whether serious orthopaedic injuries are associated with chronic conditions, long-term health outcomes, or both following injury. However, studies showed that the relationship between chronic health conditions and health status following a serious orthopaedic injury is complex.3,5,51 Serious orthopaedic injuries, such as fractures, can have significant consequences, including persistent pain, functional impairment, limitations in activity, and restrictions on participation. A combination of these complications and chronic health conditions may result in an overall decrease in health status.52,53 This vulnerability arises from the interplay between serious orthopaedic injury and post-injury chronic health conditions. Additionally, the psychological stress associated with serious orthopaedic injuries can affect an individual's mental and emotional well-being, which, when combined with the effects of chronic physical health conditions, can further compromise health status.2,8 This bidirectional nature of the association between chronic health conditions and long-term health outcomes can vary among individuals. This creates a cyclic pattern that underscores the importance of adopting a comprehensive and personalized approach to healthcare. Because we used hospital admission/ED presentations to determine the presence of health conditions, we could not ensure a complete capture of all chronic health conditions (e.g. those diagnosed and treated in the community, or undiagnosed). As a result, the prevalence of chronic physical health conditions is likely to have been underestimated. Using Medicare Benefits Schedule (MBS) and/or Pharmaceutical Benefits Schedule (PBS) data in future Australian studies might reduce this limitation. We limited our analysis to conditions with a principal/primary diagnosis in order to focus on new post-injury conditions. This could also have lowered the prevalence of chronic conditions following serious orthopaedic injury. Furthermore, reported health status may differ systematically between people with chronic conditions that are missed and people with chronic conditions that are captured in hospital admissions/ED presentations. People with chronic physical health conditions managed in the community or people who have better self-management skills for their chronic condition may score higher on the EQ-VAS than those with chronic conditions admitted to the hospital or presenting to the emergency department. Another potential limitation of our study was the potential for ‘survivor bias’. People with serious orthopaedic injuries who died before completing follow-up may have differed from people who survived until completed follow-up. For people who died before the follow-up was complete, post-injury health status was not simply missing, but rather, undefined. People with no chronic conditions who died before completing follow-up may have been healthier overall than people without chronic physical health conditions. The other limitation of this study was that about 10% of pre-injury EQ-VAS data were missing. However, we conducted a sensitivity analysis without using pre-injury EQ-VAS and found no qualitative alteration in the overall interpretation of the outcome. Furthermore, because we only looked at elements that could be extracted from the linked dataset, important confounding factors like physical inactivity, sedentary behaviour, post-traumatic stress disorder and dietary habits were not included in our model because they were not included in any datasets.
Conclusion
Post-injury chronic physical health conditions were associated with a lower long-term health status and a higher mortality rate. Chronic conditions may affect recovery after injury, and this needs to be considered in future research. Assessing risk-adjusted long-term outcomes in orthopaedic injury populations requires adjustment for post-injury chronic physical health conditions. Early screening, prevention, detection, and management of chronic physical health conditions could improve long-term outcomes following injury. People with chronic physical health conditions need to receive more frequent long-term health monitoring than people without chronic physical health conditions following injury.
Supplemental Material
sj-docx-1-tra-10.1177_14604086231216180 - Supplemental material for The association between post-injury chronic physical health conditions, health status, and survival time in people with serious orthopaedic injuries
Supplemental material, sj-docx-1-tra-10.1177_14604086231216180 for The association between post-injury chronic physical health conditions, health status, and survival time in people with serious orthopaedic injuries by Asmare Yitayeh Gelaw, Belinda J Gabbe, Sarah J Arnup, Sandra Reeder, Mark Fitzgerald, Ronan Anthony Lyons, Jennie Louise Ponsford, Alex Collie, Nicola Christie, Andrew Nunn, James E Harrison, Peter Cameron and Christina L Ekegren in Trauma
Supplemental Material
sj-docx-2-tra-10.1177_14604086231216180 - Supplemental material for The association between post-injury chronic physical health conditions, health status, and survival time in people with serious orthopaedic injuries
Supplemental material, sj-docx-2-tra-10.1177_14604086231216180 for The association between post-injury chronic physical health conditions, health status, and survival time in people with serious orthopaedic injuries by Asmare Yitayeh Gelaw, Belinda J Gabbe, Sarah J Arnup, Sandra Reeder, Mark Fitzgerald, Ronan Anthony Lyons, Jennie Louise Ponsford, Alex Collie, Nicola Christie, Andrew Nunn, James E Harrison, Peter Cameron and Christina L Ekegren in Trauma
Supplemental Material
sj-docx-3-tra-10.1177_14604086231216180 - Supplemental material for The association between post-injury chronic physical health conditions, health status, and survival time in people with serious orthopaedic injuries
Supplemental material, sj-docx-3-tra-10.1177_14604086231216180 for The association between post-injury chronic physical health conditions, health status, and survival time in people with serious orthopaedic injuries by Asmare Yitayeh Gelaw, Belinda J Gabbe, Sarah J Arnup, Sandra Reeder, Mark Fitzgerald, Ronan Anthony Lyons, Jennie Louise Ponsford, Alex Collie, Nicola Christie, Andrew Nunn, James E Harrison, Peter Cameron and Christina L Ekegren in Trauma
Footnotes
Acknowledgements
We would like to thank the Victorian State Trauma Outcome Registry and Monitoring group for providing Victorian State Trauma Registry data. We also gratefully acknowledge Monash Secured Research Platform (SeRP). Monash SeRP is a secure environment for sharing research data for collaboration and analysis, within the control and governance of the data custodian. We would like to thank the Centre for Victorian Data Linkage unit for conducting the data linkage. The authors would like to acknowledge the Victorian Department of Health as the source of VAED and VEMD data used for this study. Finally, we would like to thank Pamela Simpson, Leva Sriubaite and Joanna Dipnall for their assistance in the preparation and management of the linked data and for their statistical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for the linkage was provided by the Victorian Department of Health and Human Services Human Research Ethics Committee (DHHS HREC) and participating health service ethics committees
Informed Consent
Not applicable
Trial Registration
Not applicable
Contributorship
AG conceptualized the manuscript. AG was responsible for cleaning and analyzing the data, AG wrote the draft manuscript, and all others contributed by providing feedback, interpreting results, and refining the manuscript. All authors reviewed and edited the manuscript. All authors have read and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.