
Abstract
Objectives
Ankle fractures have an incidence of around 90,000 per year in the United Kingdom. They affect younger patients following high energy trauma and, in the elderly, following low energy falls. Younger patients with pre-existing comorbidities including raised BMI or poor bone quality are also at risk of these injuries which impact the bony architecture of the joint and the soft tissues leading to a highly unstable fracture pattern, resulting in dislocation. At present, there is no literature exploring what effect ankle fracture-dislocations have on patients’ quality of life and activities of daily living, with only ankle fractures being explored.
Methods
Relevant question formatting was utilised to generate a focused search. This was limited to studies specifically mentioning ankle injuries with a focus on ankle fracture-dislocations. The number of patients, fracture-dislocation type, length of follow up, prognostic factors, complications and outcome measures were recorded.
Results
Nine hundred and thirty-nine fractures were included within the studies. Eight studies looked at previously validated foot and ankle scores, two primarily focused on the American Orthopaedic Foot and Ankle Society score (AOFAS), three on the foot and ankle outcome score (FAOS), and one study on the Olerud–Molander score (OMAS). Patient, injury, and management factors were identified as being associated with poorer clinical outcomes.
Conclusions
Not only are age and BMI a risk factor for posttraumatic osteoarthritis but they were also identified as prognostic indicators for functional outcome in this review. Patients sustaining a concurrent fracture-dislocation were found to have poorer clinical outcomes, and the timing and success of reduction further influenced outcomes. This review found that the quality of reduction was directly related to the patients’ functional outcomes post-follow up, and the risk of developing posttraumatic osteoarthritis, which was more frequent in patients sustaining Bosworth fractures, posterior malleolar fractures, and in patients with increasing age.
Level of evidence
IV.
Keywords
Introduction
Ankle fractures have an incidence of approximately 90,000 per year in the United Kingdom. They have a bimodal distribution, affecting younger patients following high energy trauma and, in the elderly, following low energy falls. Younger patients with pre-existing comorbidities such as raised body mass index (BMI) or poor bone quality are also at risk of these injuries1,2 which not only affect the bony architecture of the joint but also the soft tissues, resulting in a highly unstable fracture pattern associated with dislocation. When the soft tissues fail, this may result in an open fracture and add to the risk profile. 3
Current UK practice advises for all ankle fracture-dislocations to be reduced urgently within the emergency department (ED), minimising the risk of further soft tissue injury and oedema. The British Orthopaedic Association Standards for Trauma and Orthopaedics (BOAST) 12 guidance recommends a pre-reduction radiograph unless this would cause an unacceptable delay. 4 Ankle fracture-dislocations are commonly managed with either primary open reduction and internal fixation (ORIF), or staged management with a period of external fixation prior to definitive surgery, allowing recovery of soft tissues. The definitive use of external fixation is indicated for patients with a poor soft tissue envelope, or those not medically fit for a second procedure.
Previous studies have illustrated an association between ankle fracture-dislocations and post-traumatic osteoarthritis (PTOA) due to imperfections in the articular surface and changing joint biomechanics. This can affect the individual’s ability to return to work and increases the risk of further operative intervention in the form of ankle arthroplasty or fusion. 5 Subsequently, the effect of changing the joint biomechanics increases the potential for further fusions, including those of the talocalcaneal and talonavicular joints. 6
Existing literature reviews have identified prognostic factors associated with outcome progression in patients with non-displaced ankle fractures. These include osteochondral lesions resulting in a lower threshold for recurrent injury 7 and early weight-bearing which improves functionality. 8 This review aims to explore the current evidence for outcomes of ankle fracture-dislocations and the available prognostic evidence.
Methods
Data sources
This systematic review was written in accordance to the PRISMA guidelines (Figure 1). Relevant question formatting was utilised to generate a focused search using PICO: population, intervention, comparison, and outcome. This guided the selection of literature sources and provided a focus for the search. Our population, as well as search limitation, consisted of patients over the age of 16 who sustained ankle fracture-dislocations. Patients receiving operative intervention were compared to those who were managed conservatively to identify factors associated with poorer prognosis. The assessment of functional outcomes was derived using appropriate foot and ankle scoring systems, weight-bearing status, and radiographic evaluation. An extensive search strategy (Figure 1) was employed using Boolean operators. Computerised databases consisted of Wolters Kluwer OvidSP Database (1733 papers), Cochrane Library (4 papers), and EBSCOhost (5 papers).
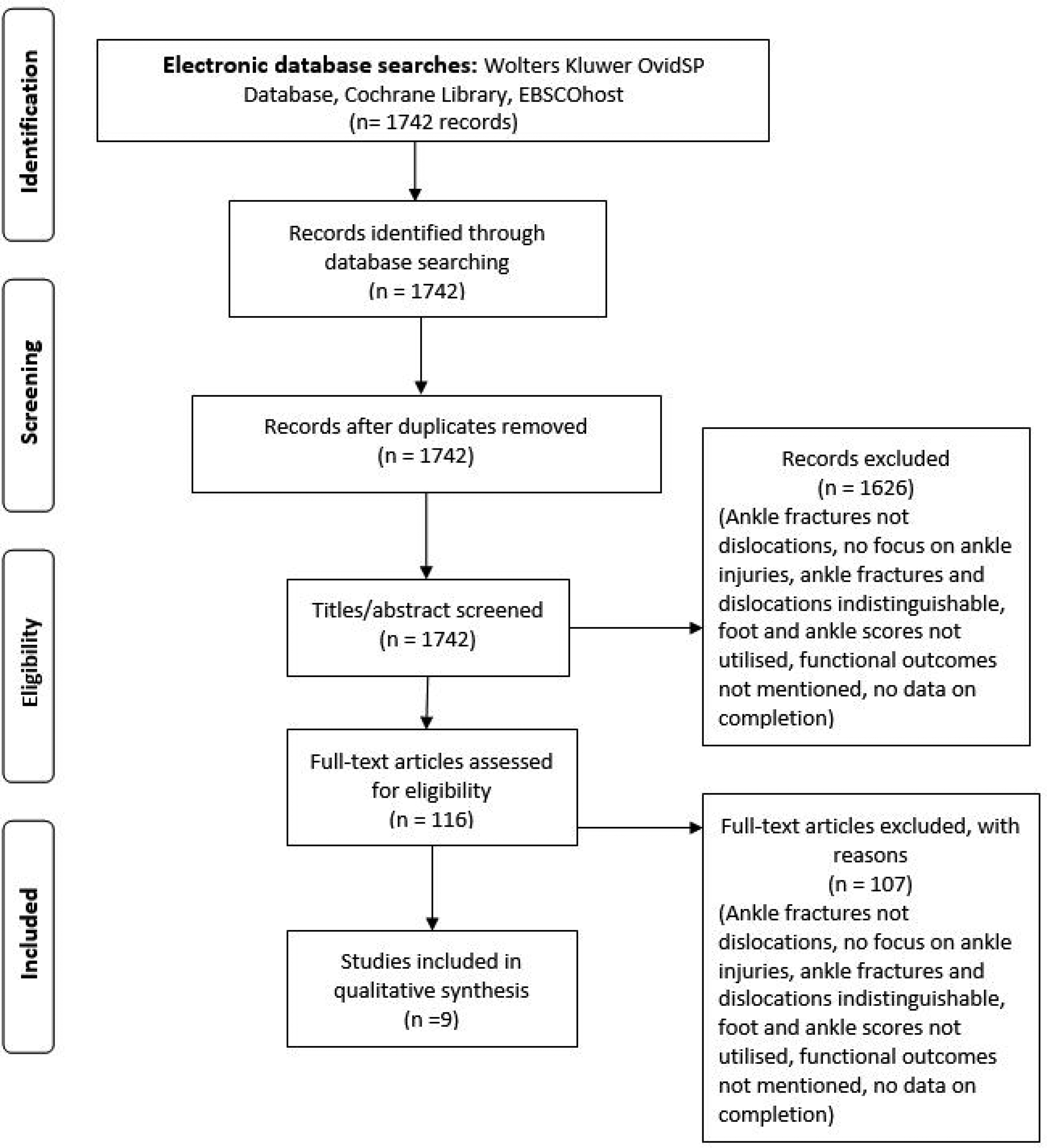
PRISMA flow diagram.
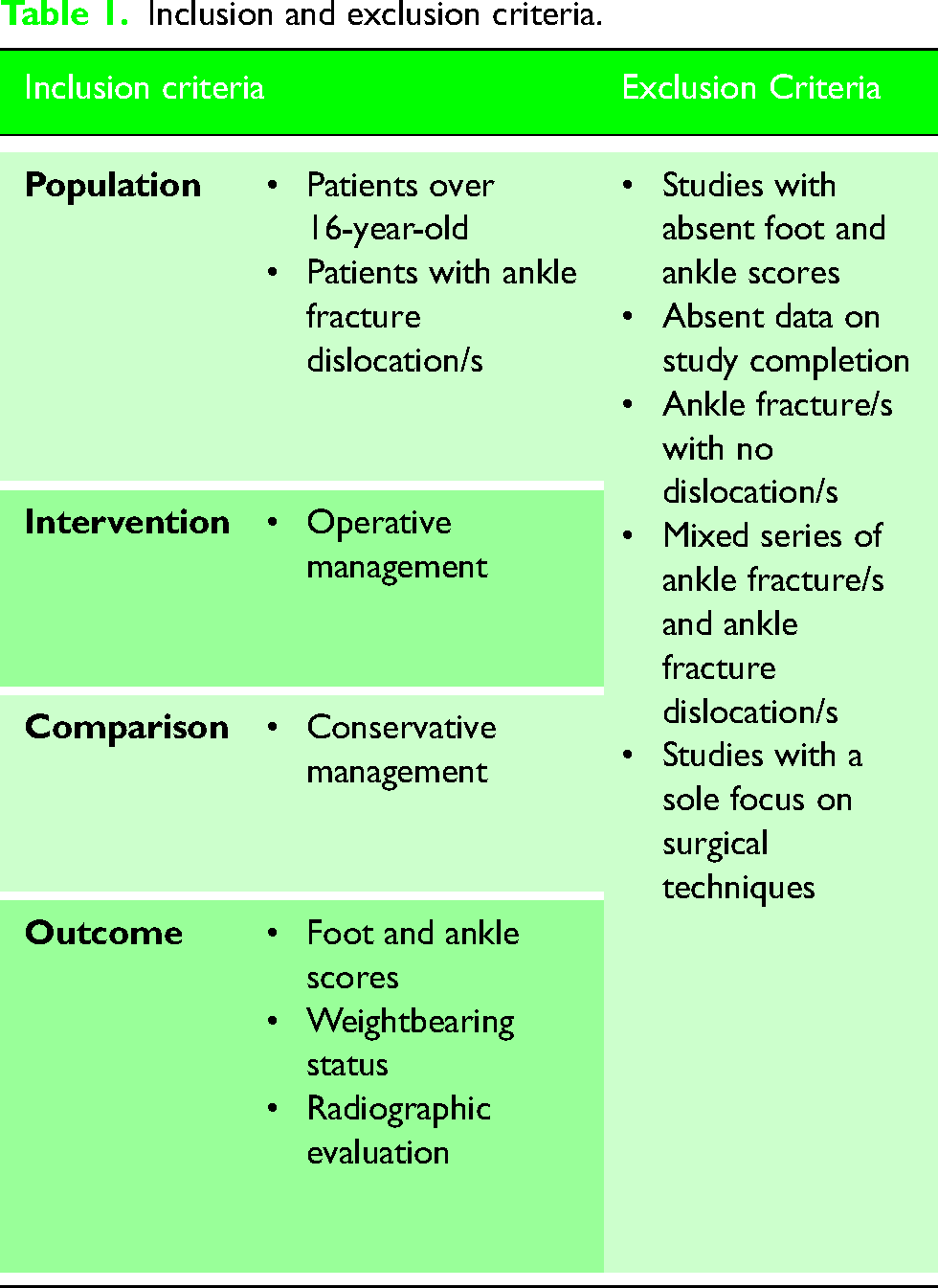
The literature search was limited to studies specifically mentioning ankle injuries with a focus on ankle fracture-dislocations. The exclusion criteria consisted of studies which did not utilise foot and ankle scoring systems to assess functional outcomes, no data on completion, and a focus solely on ankle fractures without dislocation. Articles reporting a mixed series of non-displaced ankle fractures and ankle fracture-dislocations were excluded if the qualitative and quantitative analysis between the two subgroups could not be distinguished. Papers focussing on surgical techniques were also excluded.
Study selection
During the screening stage, the title and abstract of prospective articles were assessed. Studies which either demonstrated the inclusion criteria, or insufficient detail, progressed to the successive stage. Full paper screening of these studies then took place with two authors (AEW and RA) assessing which studies met the inclusion criteria (Table 1). In a situation of disagreement, the final decision followed a discussion between both authors to reach a consensus. Of the initial 1742 papers, 9 met our inclusion criteria. Figure 1 demonstrates the screening process.
Inclusion and exclusion criteria.
Data extraction
The data of the included studies were extracted by one author (RA) and verified by the second author (AEW). Only data from the published articles were included in the analysis with the authors not being contacted for further details. Studies were assigned their level of evidence as defined by the Centre for Evidence-Based Medicine. 9 Relevant information including the population sample, pattern of fracture-dislocation, length of follow up, prognostic factors, complications and outcome measures were recorded.
Risk of bias in individual studies
During the full paper screening, obvious sources of bias were recorded (Figure 2) including funding and affiliations. These are discussed within the limitations section of this review. A specific bias screening tool was not utilised.
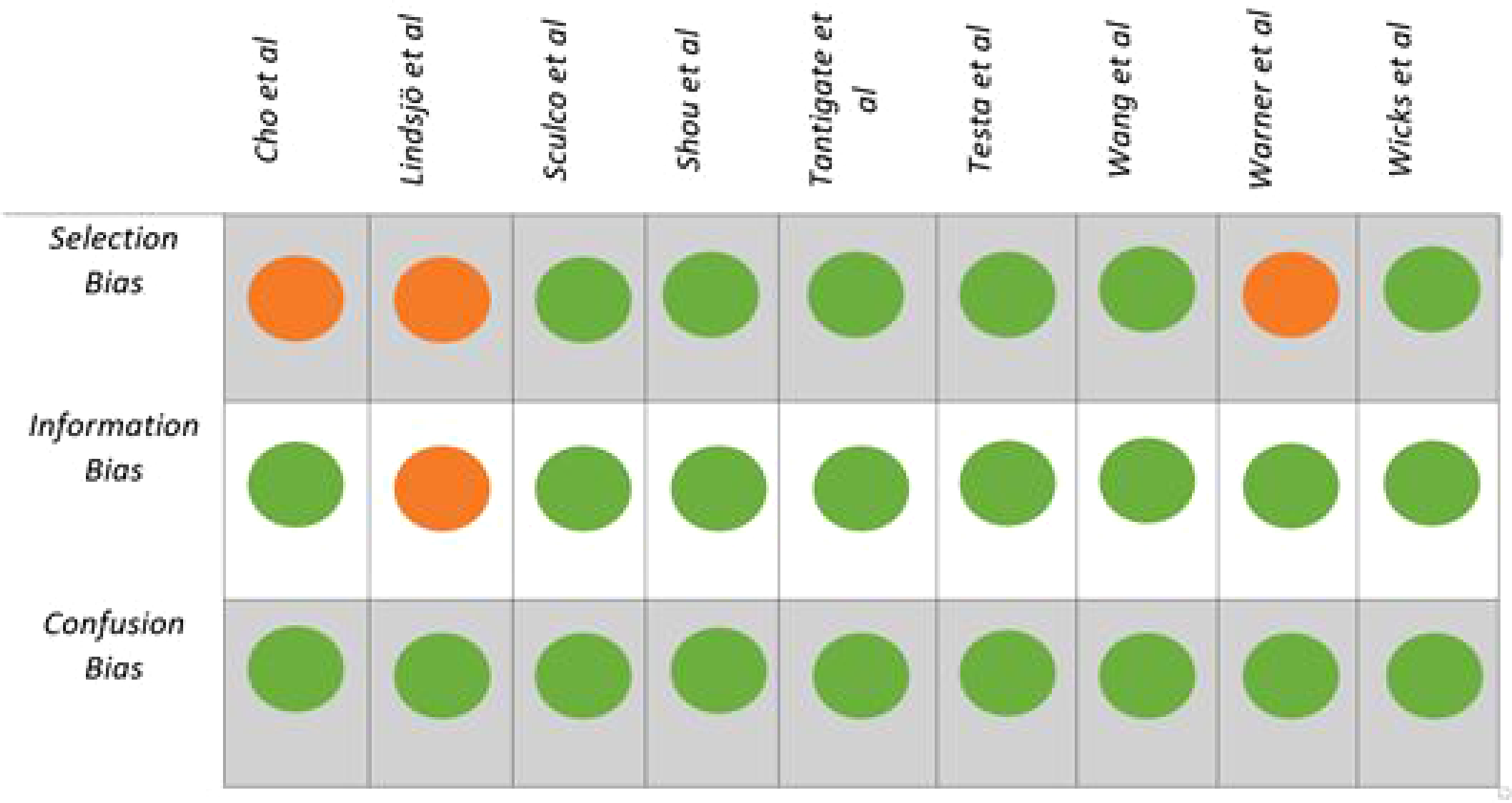
Risk of bias. 10
Data synthesis and statistics
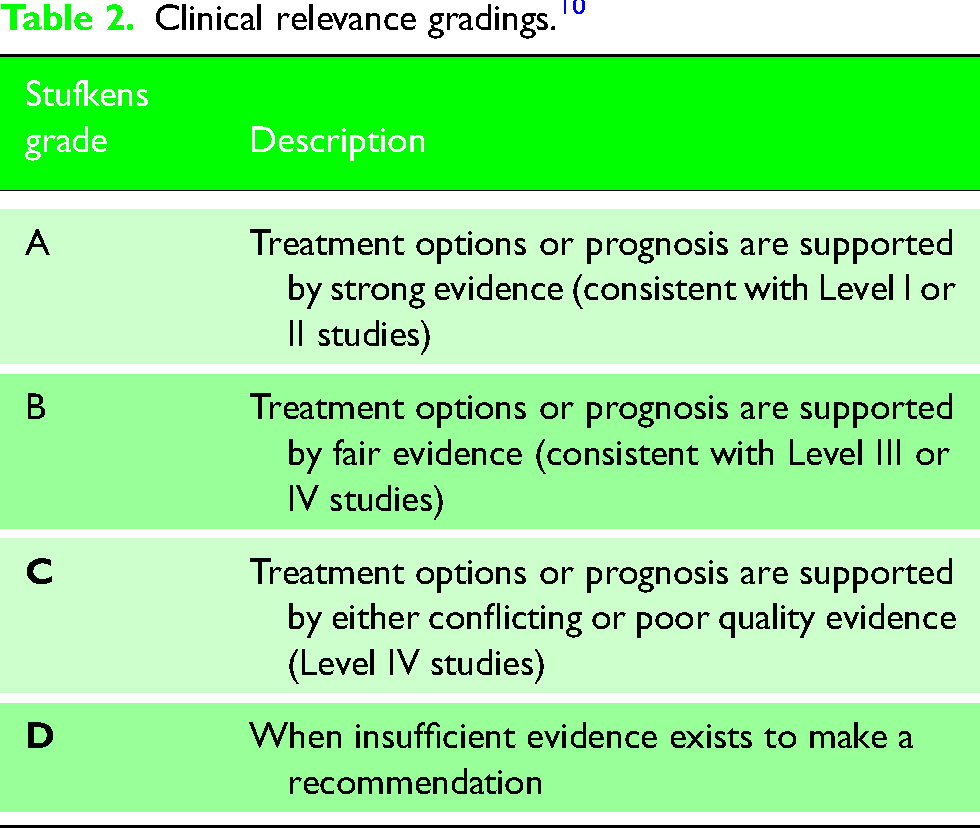
Using methods identified by Stufkens et al., prognostic indicators were assigned a grade A to D which associates their clinical value. 11 These gradings are outlined in Table 2. Papers were compared using the functional outcomes scores, and the most frequently used functional outcome score was used to prevent duplication within a single paper utilising multiple clinical outcome scores.
Clinical relevance gradings. 10
Results
The included nine studies totalled 939 ankle fractures. Amongst these papers, three were Level III12–14 studies and the remainder were Level IV.15–20 (Table 3). Two papers focussed on prognostic factors associated with poorer outcomes in ankle fracture dislocations15,19 and three papers identified risk factors associated with PTOA.16,18,20
Overall outcomes.
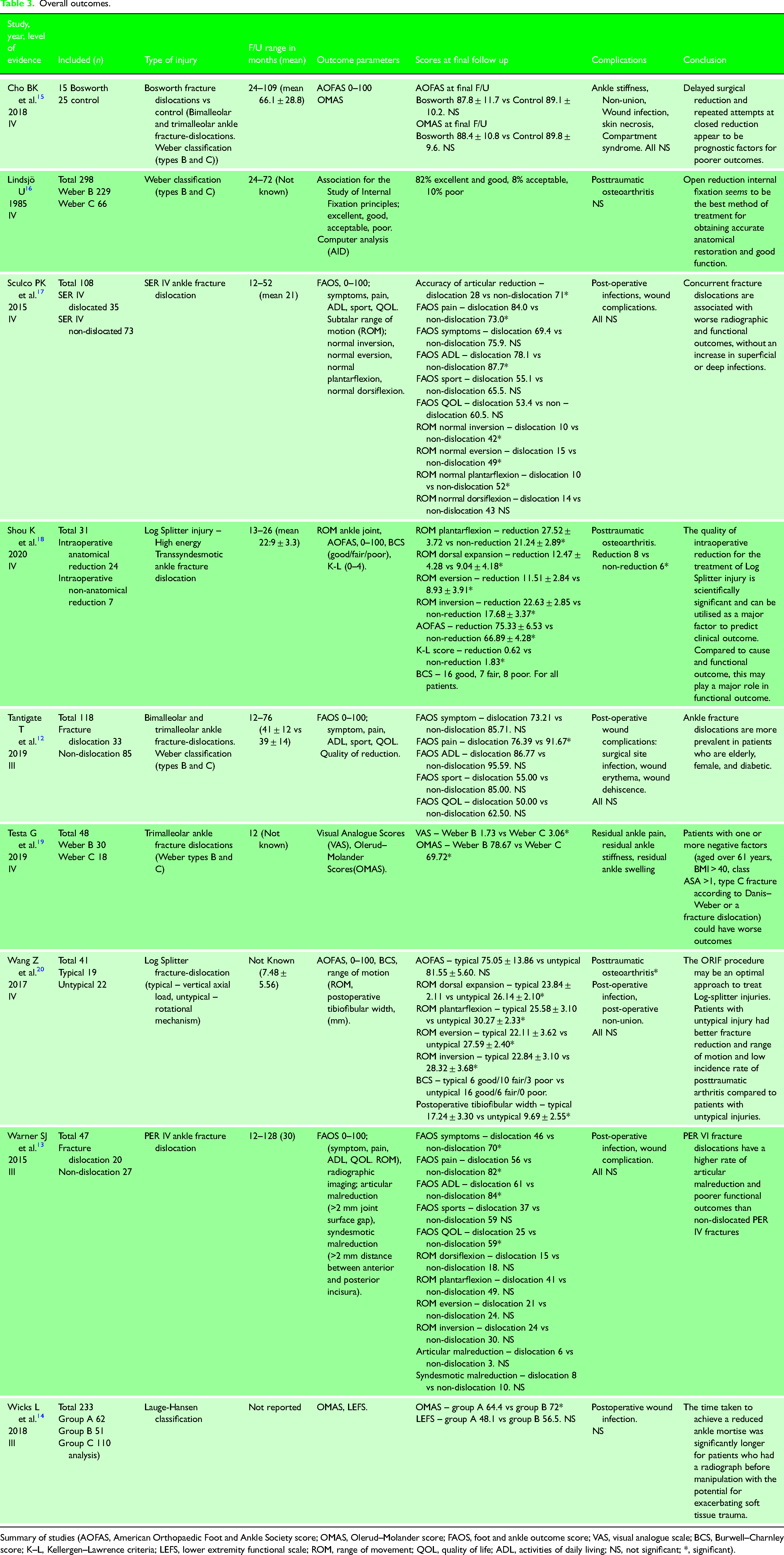
Summary of studies (AOFAS, American Orthopaedic Foot and Ankle Society score; OMAS, Olerud–Molander score; FAOS, foot and ankle outcome score; VAS, visual analogue scale; BCS, Burwell–Charnley score; K–L, Kellergen–Lawrence criteria; LEFS, lower extremity functional scale; ROM, range of movement; QOL, quality of life; ADL, activities of daily living; NS, not significant; *, significant).
Four of the included nine studies did not report the number of patients initially identified.14,15,18,20 Of those patients in the remaining five studies (n = 670), 86.71% (n = 581) completed follow-up.12,13,16,17,19 Six papers reported a follow-up range between 3 and 128 months.12,13,15–18
Functional outcomes
Three studies used the American Orthopaedic Foot and Ankle Society (AOFAS) score to assess the clinical outcomes of different types of fracture-dislocation. The score is out of 100 and consists of nine questions, focussing on three areas: pain (40 points), function (50 points), and alignment (10 points). Scores of more than 90 show an ‘excellent’ result, more than 80 show ‘good’ result, but an acceptable result is debated. 21
Cho et al. 15 further subdivided the injuries as standard Danis–Weber B or C fracture-dislocations and Bosworth fracture-dislocations. These injuries are defined as ‘fracture-dislocation of the ankle with fixed displacement of the proximal fragment of the distal fibular fracture behind the posterior tibial tubercle’ 15 and are commonly caused by severe external rotation with supination and can be irreducible unless opened. 22
Shou et al. 18 and Wang et al. 20 examined the outcomes for the Log-splitter fracture-dislocation. Both assessed the typical pattern of injury caused by a vertical axial load and illustrated that when anatomically reduced intraoperatively, these injuries had a similar ‘acceptable outcome (75.33 ± 6.53 vs 75.05 ± 13.86).
Testa et al. 19 compared the outcomes of ankle-fracture dislocations according to the Danis–Weber classification. 23 Weber B injuries (those at the level of the syndesmosis), and Weber C (those above the syndesmosis), both had a significant improvement at the end of the 12-month follow up (78.67, 45–100 vs 69.72, 35–100, p = 0.03). Patients did suffer with residual ankle pain, stiffness and swelling.
Wicks et al. 14 assessed ankle fracture dislocations using the Lauge–Hansen classification 24 but the functional outcomes were not grouped according to this, but rather whether they underwent manipulation according to clinical groups alone or if they had a radiograph performed prior to reduction. This method was used to assess outcomes according to the BOAST 12 which suggests ‘Reduction and splinting should be performed urgently for clinically deformed ankles. Radiographs should be obtained before reduction unless this will cause an unacceptable delay’. 4 Patients in group B (patients undergoing manipulation in the ED based on clinical grounds alone), had better outcomes than those in group A (patients receiving an X-ray before any attempt at ankle reduction) (72, 25–100 vs 64.4, 20–90, p = 0.039).
Two papers assessed the injuries according to the Lauge–Hansen Classification. 24 The results were significant for the pronation-external rotation (PER) injuries studied by Warner et al. 13 Of the 47 injuries assessed, the 20 fracture-dislocations illustrated significantly worse outcomes than the 27 fractures alone across the symptom, pain, ADL and quality of life (QOL) domains (Symptoms 70 ± 23.3 vs 46 ± 21.7, p = 0.002; Pain 82 ± 20.1 vs 56 ± 20.7, p ≤ 0.001; ADL 84 ± 21.6 vs 61 ± 23.3, p = 0.002; QOL 59 ± 29.4 vs 25 ± 21.3, p ≤ 0.001).
Fracture reduction as a prognostic indicator
Across the nine studies, a range of scores and measurements were used to assess whether the ankle fracture-dislocations were reduced successfully following operative intervention. Lindsjö 16 judged the acceptability of the reduction following operative intervention but did not state what criteria were used; 90% of the fractures were satisfactorily reduced, and this was linked to better clinical outcomes on combined subjective clinical and examination findings (Stufkens Grade C).11,16
Other studies did outline clear measurements the authors had used on postoperative films to identify whether the fracture had been effectively reduced. Warner et al. 13 used the tibiofibular distance to judge how well the syndesmosis had been reduced, as well as judging the articular reduction on postoperative CT scans. Syndesmotic malreduction was common, in not only fracture-dislocations but also in fractures alone (44.4% vs 47.6%, p = 0.95). Articular malreduction was more common in fracture-dislocations (33.3% vs 14.3%, p = 0.15) (Stufkens Grade C).11,13
Two studies used the Burwell–Charnley score to identify fractures that were unsatisfactorily reduced.19,20,25 This scoring system classifies fractures into those with anatomical, fair, and poor reduction based on the degree of postoperative displacement. 6 Both studies found that the quality of intraoperative reduction was not only linked to significantly better short-term outcomes, as measured by the AOFAS, but also to significantly lower rates of early post-traumatic arthritis after completion of the 2-year follow-up period (Stufkens Grade B).11,18,20
Other prognostic factors associated with poorer outcomes
Patient, injury and management factors were identified as being associated with poorer clinical outcomes. Testa et al. found that patients with a BMI of over 40 as well as those above the age of 61 years experienced poorer outcomes (AOFAS) at the end of the 12-month follow-up period. 19 The authors also found that patients with comorbidities which caused them to be assigned an American Society of Anaesthesiologists (ASA) grade of greater than one were more likely to have poorer clinical outcomes (Stufkens Grade C).11,19
As for the fracture personality, unsurprisingly patients who had a concurrent fracture-dislocation were found to have poorer clinical outcomes than those with an ankle fracture alone (Stufkens Grade C).11,17,19 Patients with these injuries had poor reduction on radiographs during follow up (Stufkens Grade B).11,19,26 Patients with Weber C fracture-dislocations were also identified as having poorer clinical function owing to the greater disruption of the syndesmosis (Stufkens Grade C).11,27
Within the ED, the timing and success of reduction were found to be important factors influencing outcomes. Wicks et al. found that patients with ‘frankly displaced ankle fracture-dislocations’ who waited longer for reduction, due to a prolonged waiting time for pre-reduction radiographs, had a significantly worse clinical function at the end of the study period. OMAS and FAOS were used to assess the functional outcome in this study (Stufkens Grade C).11,15 This was also true for patients who required multiple attempts to achieve adequate closed reduction (Stufkens Grade C).11,16 One study did demonstrate how prolonged reduction time for ankle fracture-dislocations leads to poorer functional outcomes. 14
Complications associated with ankle-fracture dislocations
Soft tissue complications were reported across six of the nine studies.12–15,17,20 Primarily, the rates of superficial wound infections were described in five studies, but when compared to patients who suffered fractures without dislocation, there were no significant differences (Stufkens Grade D).11–15,17,20 Oral antibiotics and better surgical site hygiene were described as adequate solutions for the management of these infections. 19
Other soft tissue complications included the impact of managing the patient in casts. Lindsjö et al. reported one patient suffering with a pressure sore and a second having a hypersensitivity reaction to plaster of Paris (Stufkens Grade D).11,16
Thromboembolic events were reported in two studies, although these were rare. Lindsjö 16 described two patients (0.006%) who were treated for deep venous thrombosis (DVTs), both of which were mobile throughout their treatment in a cast. The use of chemical thromboprophylaxis was not discussed. According to Tantigate et al., 12 two patients suffered from thromboembolic events in the non-dislocated cohort (2.4%), in comparison to the dislocated subgroup (p = 0.42) which reported no patients suffering this complication (Stufkens Grade D).11,12
Three studies focussed on factors associated with PTOA.16,18,20 Lindsjö 16 found that the incidence of PTOA was significantly higher in patients over the age of 35 years and in those whose injury included a posterior malleolus fracture. The quality of reduction was also associated with the likelihood of developing PTOA, those with excellent or good reduction being less likely to suffer in the future. 3
Discussion
Patients sustaining severe ankle fractures including PER and Weber C, have worse clinical outcomes when compared to patients sustaining less severe injuries.11,13,27 It is therefore no surprise that fracture dislocations have worse outcomes than fractures alone.15,19
The quality of fracture reduction in the included studies was directly related to the patient's functional outcomes at the end of follow up.13,15,18 This has been previously observed in studies focussing on pilon fractures whereby a better-quality reduction is associated with better functional outcome scores at 2 years following injury.26,27 This systematic review also found that the quality of reduction is directly related to the risk of developing PTOA in the future, and was more frequent amongst patients sustaining Bosworth fractures, those with a posterior malleolar fracture, and those over the age of 35 years.16,19 This adds to the existing literature which demonstrates that the risk factors for PTOA include a high BMI, length of time since surgery, sustaining a Weber C fracture, and associated medial malleolar fracture. 28
Apart from being identified as a risk factor for PTOA, two studies identified increasing patient age11,18 and BMI 18 as significant prognostic indicators for functional outcomes. This result mirrors a Swedish study which assessed the outcomes and QOL in patients over 65 years sustaining ankle fractures alone without dislocation, who underwent operative management. These patients experienced higher rates of difficulties with pain and reduced mobility when compared to younger patients at the end of a 2-year follow-up. 29
An ASA score of more than one was also found to be associated with a poor functional outcome in ankle fracture-dislocations. 19 This trend has previously been observed in studies which illustrate that patients with a higher ASA had poorer functional outcomes at 1 year following ankle fracture injury. 30
At present, there are no qualitative studies exploring what effect ankle fracture-dislocations have on patients QOL and ADLs, with only ankle fractures being explored. One such qualitative study interviewed patients on their individual experiences of ankle fractures and essential factors personal to their recovery, and reported the impact on factors including ADLs, sleep disturbance, and social life. Participants described struggling with personal care resulting in the necessity of adapting to new routines. This was discussed in relation to individuals’ weightbearing status and mobility aids. With regards to QOL, several participants reported negative impacts on social and family life, including psychological effects associated with depression and anxiety. 5
Within this study, an analysis of bias was conducted according to Ramírez-Santana. 10 Three studies had a greater risk of selection bias. The recruitment of the control group in the study by Cho et al. 15 was not discussed at length, leading to potential bias in individual case selection.3,8,26 In the study by Lindsjo, 16 it was not clear how much the patients’ activities were affected by their injury within the follow-up period, having been assigned an outcome rated from poor to excellent by clinicians without a validated questionnaire being employed. The recruitment of the study group was not discussed at length in the study by Warner et al. 12 There was no evidence of confusion bias in any of the included studies. Hence, the effect of information bias in this study remains uncertain. 14
The limitations of this review include the number of eligible studies, small patient cohorts, and the use of different functional outcome scores. These factors make it difficult to directly compare outcomes across the studies and therefore meaningful conclusions cannot be drawn due to low-level evidence. The results derived from this systematic review can be utilised in the development of future randomised control trials or prospective cohort studies with a similar focus.
Conclusion
Ankle fracture-dislocations are severe injuries which can be associated not only with poor clinical outcomes as assessed by validated foot and ankle scores, but also with an increased risk of PTOA. In addition to being identified as a risk factor for PTOA, increasing patient age and BMI were also concluded as prognostic indicators for poorer functional outcome in this systematic review.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Trial registration
Not applicable.