
Abstract
Common complications of chest tube insertion are lung laceration, chest wall bleeding, improper tube positioning, and subcutaneous emphysema. However, a penetrating injury of the upper abdominal organs due to chest tube malposition is rare. A 33-year-old suffered multiple injuries in a road traffic accident. Due to the respiratory distress caused by right-sided hemothorax, an intercostal chest drain (ICD) was inserted, which drained 500 ml of venous blood, followed by hemodynamic instability. The post-procedural chest radiograph revealed a lower chest tube position within the liver shadow. As the patient was hemodynamically stable, it was decided to delay the removal of the ectopic ICD, and the patient was kept under close monitoring. After 7 days, ICD removal was done under ultrasound guidance, and a post-procedural serial-focused assessment with sonography for trauma (FAST) was done. Hepatic injury secondary to chest tube insertion is rare, and its management is not standardised. Point-of-care ultrasound has not been used before for the removal of an ectopic ICD. We managed the case conservatively because of the stable hemodynamic situation of the patient and to avoid invasive surgery as possible. Point-of-care ultrasound can be a valuable tool in these conditions where other imaging modalities such as CT are not available and help avoid surgery.
Keywords
Introduction
Intercostal chest drainage is indicated in various clinical scenarios, including managing symptomatic pleural effusion, pleural infection, and pneumothorax. Common complications of chest tube insertion are lung laceration, chest wall bleeding, improper tube positioning, and subcutaneous emphysema. 1 However, a penetrating injury of the upper abdominal organs due to chest tube malposition is rare. We describe a case of chest tube malposition in the liver and its management by the use of point-of-care ultrasound.
Case report
A 33-year-old male who had been involved in a road traffic accident presented to the emergency department with chest, back, and upper and lower limb injuries. The patient was conscious, oriented, and hemodynamically stable although tachycardic and tachypneic. Radiological investigations (x-ray chest/abdomen and high-resolution computed tomography (HRCT) thorax) were performed along with routine blood investigations. Investigations revealed a fracture of the right femur, sixth thoracic vertebra, and sixth rib with right-sided hemothorax. The resident doctor inserted an intercostal chest drain (ICD) to relieve the respiratory distress caused by right-sided hemothorax. Within 10 minutes, 500 ml of venous blood was drained through the ICD, followed by hemodynamic instability. The chest tube was immediately clamped, and the patient was resuscitated with intravenous fluid. The post-procedural chest radiograph revealed a low chest tube position within the liver shadow. HRCT thorax confirmed the diagnosis, and the ICD crossed the complete right lobe of the liver parenchyma and reached up to the right renal hilum (Figure 1A). HRCT was preferred over contrast-enhanced CT because the patient was unstable and at risk of acute kidney injury.
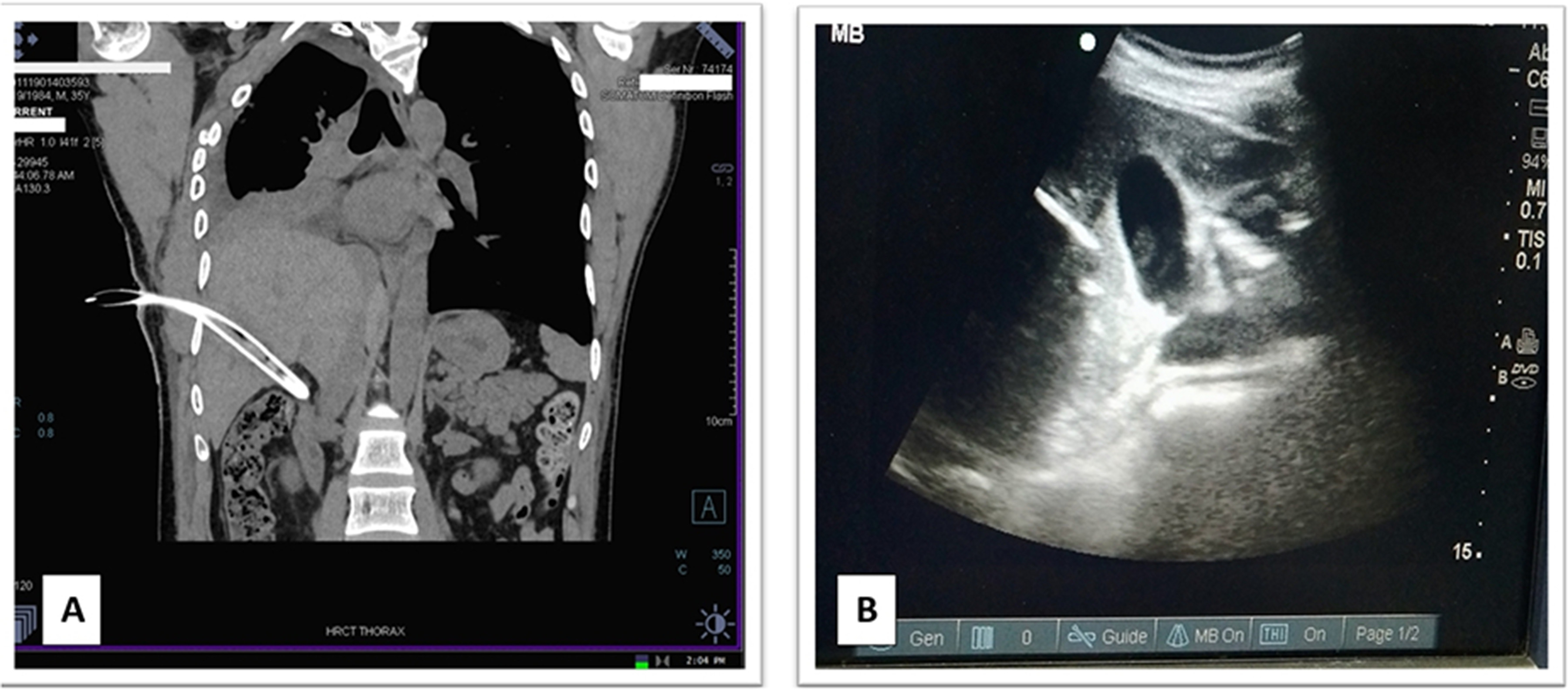
(A) HRCT thorax showing ICD in the liver. (B) Use of point-of-care USG for the removal of ICD.
Another chest tube was then inserted through the fifth intercostal space to drain the hemothorax. As the patient was conscious, oriented and hemodynamically stable, it was decided to delay the removal of ectopic ICD, and the patient was kept under close monitoring. The drain was left in place for 7 days for parenchymal hemostasis. During the stay, the patient was assessed clinically for signs of bleeding along with routine investigations.
After 7 days, the patient was planned for ICD removal under ultrasound guidance in the operating room with adequate preparation for emergency laparotomy if needed. The chest tube was slowly withdrawn by 2 cm under ultrasonic guidance, and then monitored for 5 minutes for signs of active haemorrhage (Figure 1B). The withdrawal was performed for real-time visualisation and early detection of any active bleeding. Interventional radiologists were available to embolise the tract, hepatic artery, or portal vein post-removal in case of bleeding.
After approximately 45 minutes, the ICD had been completely removed without complications. Serial focused assessment with sonography for trauma (FAST) was then performed every 15 minutes for 1 hour and then hourly for 6 hours to assess any post-procedural intra-abdominal haemorrhage. Clinical examinations like palpation and percussion were done in conjunction with serial FAST.
The rest of the patient's course was uneventful, and he was discharged after 1 week. Post-removal CT thorax was performed, which showed a linear hypodensity tract in the liver without any sign of bleeding.
Discussion
Malposition of drains can be associated with severe morbidity and mortality and has been identified as a serious issue by the National Patient Safety Agency. 2 The use of bedside ultrasound for ICD placement, equipment incorporating safety features, and protocols and training help minimise the risks. The British Thoracic Society pleural disease guideline recommends ultrasound guidance for pleural fluid drainage procedures and the usage of small-bore catheters. However, thoracic ultrasound is of limited utility in guiding the insertion of a chest drain in the presence of pneumothorax because of the difficulty in obtaining useful images due to the poor transmission of sound waves through the air. 3 The best way to avoid hepatic trauma is to ensure fifth intercostal space is used, blunt dissection and the feeling of a smooth pleural surface.
Hepatic injury secondary to chest tube insertion is rare, and its management is not standardised. On reviewing the literature, only five cases have been described in the literature. 4 They have been managed conservatively, by surgery or by embolisation. 4 Liver tract embolisation, with or without coiling, has an established role in removing a chest tube in the liver. 4
Numerous studies have demonstrated the utility of FAST in trauma. It has sensitivities between 85% and 96% and specificities exceeding 98% in detecting hemoperitoneum. In the subset of hypotensive trauma patients, the sensitivity of the FAST exam approaches 100%. 5 The risk of developing hepatic pseudoaneurysm in patients with liver trauma is 1–6%. It might be ‘silent’ until enlargement and rupture; the diagnosis is difficult when no default follow-up CT scan is performed. However, the evidence for follow-up radiology after non-operatively managed liver trauma to identify HPA remains debatable. 6
Point-of-care ultrasound has not been used before to aid the removal of an ectopic ICD. We managed the case conservatively because of the stable hemodynamic situation of the patient and to avoid invasive surgery as possible. The chest tube was pulled slowly under ultrasound guidance, and serial FAST was used to detect any active bleeding. Point-of-care ultrasound in these circumstances can be a useful tool in resource-limited settings and military field hospitals where there is no access to CT scans and difficulty in the transfer of patients to a higher level of care, where a risk mitigation strategy is needed beyond serial abdominal examination to avoid a laparotomy ± massive transfusion.
Conclusion
We report the first use of serial point-of-care ultrasound to aid the removal of a chest drain inadvertently inserted into the liver. It allowed safe removal and provided reassurance that there was no ongoing bleeding.
Footnotes
Contributorship
Abhyuday Kumar and Arunima Pattanayak researched literature and conceived the article. Arunima Pattanayak wrote the first draft of the manuscript. Abhyuday Kumar, Neeraj Kumar and Sanjeev Kumar were involved in the management of the case. Neeraj Kumar and Sanjeev Kumar reviewed the article. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from legally authorised representatives before the study.