
Abstract
Objective
To assess the accuracy of a five-step prehospital trauma triage protocol (Échelle québécoise de triage préhospitalier en traumatologie (EQTPT)) to identify patients requiring urgent and specialized in-hospital trauma care in the Capitale-Nationale region – Québec.
Methods
The medical records of trauma patients transported by ambulance to one of the five participating emergency departments (EDs) between November 2016 and March 2017 were reviewed. Our primary outcome was the need for one of the following urgent and specialized trauma care: endotracheal intubation in the ED, administration of ≥ 2 blood products in the ED, angioembolization or surgery (excluding single limb surgery) < 24 h and admission to the intensive care unit (ICU) or in-hospital trauma-related death.
Results
A total of 902 patients were included. The median age was 63 (interquartile range (IQR) 51) and 494 (54.8%) were female. The main trauma mechanism was falls (n = 592), followed by motor vehicle accidents (n = 201). Eighty-two (9.1%) patients required at least one urgent and specialized trauma care. Of those, 44 (53.6%) were identified as requiring transport to a level one trauma centre (steps 1–3), 16 were identified as requiring transport to a centre with a lower level of trauma designation (steps 4–5) while 22 (26.8%) did not meet any of the EQTPT criteria. For steps 1 to 3, the sensitivity was 53.7% (95% confidence interval (CI) 42.9–64.4) and the specificity was 81.7% (95% CI 79.1–84.4) in identifying patients requiring specialized trauma care.
Conclusion
The EQTPT lacked sensitivity and was poorly specific to identify trauma patients who need specialized in-hospital trauma care.
Background
Trauma is a leading cause of morbidity and mortality worldwide. In the past decades, trauma systems integrating a continuum of prehospital and in-hospital care have improved outcomes for severely injured patients.1–6 Hence, trauma-related in-hospital mortality has decreased significantly. However, the proportion of deaths occurring in the prehospital setting is increasing and now represents close to 75% of all trauma-related deaths. 7 Studies focusing on the early prehospital and emergency department (ED) care of trauma patients are therefore essential to improve patient outcomes.4,8,9
Prehospital trauma triage protocols aiming to identify severely injured patients who require urgent and specialized trauma care are a cornerstone of initial trauma management. 10 Field triage of injured patients significantly impacts patient and system-related outcomes. For severely injured patients, prompt access to specialized trauma care reduces mortality, whereas underestimating the severity of a patient's injuries and needs is a major contributor to avoidable mortality.1,10,11 On the other hand, as a high proportion of trauma patients sustain only minor injuries, a systematic overestimation of the severity of their injuries could contribute to major trauma centre overcrowding and increased healthcare expenditures. 12 Unfortunately, current prehospital trauma triage protocols lack sensitivity and specificity in identifying severely injured patients and their acute trauma care needs.13–15 The American College of Surgeons Committee on Trauma (ACSCOT) guidelines for field triage recommend a maximum undertriage proportion of 5% and a 35% proportion of overtriage. 16 However, a recent systematic review has shown that currently available prehospital trauma triage protocols do not meet these benchmarks. 17
In 2016, the Échelle québécoise de triage préhospitalier en traumatologie (EQTPT), a prehospital trauma triage protocol identifying patients who require direct transportation to a trauma centre, was implemented in the province of Quebec, Canada. This five-step protocol was adapted from the Centers for Disease Control and Prevention (CDC) - ACSCOT protocol. 16 In the Capitale-Nationale region – Québec (approximately 730,000 inhabitants), trauma care is regionalized with a prehospital bypass system allowing the transportation of trauma patients from the field directly to a level one trauma centre. Therefore, a patient presenting with at least one criterion from steps 1, 2 or 3 of the triage protocol (Supplemental Figure 1) should be transported to a level one trauma centre if transport time is expected to be < 60 min. If a patient has at least one criterion from steps 4 or 5, they can be transported to any ED (except for the Heart and Lung Institute). Prehospital care is almost exclusively provided by paramedics with basic life support skills. For trauma patients, prehospital interventions are protocol-driven and are limited to supraglottic device insertion, 18 application of spinal restriction of motion devices and limb immobilization for suspected fractures.
The accuracy of our provincial triage protocol in identifying patients who require urgent and specialized trauma care has yet to be evaluated in the general trauma population. Therefore, this study aims to assess the EQTPT's accuracy in identifying patients who require urgent and specialized in-hospital trauma care in the Capitale-Nationale region – Québec. The secondary objectives were to assess the proportions of overtriage and undertriage associated with this protocol.
Methods
We conducted a retrospective audit of prehospital and in-hospital medical charts. Patients were identified using regional administrative prehospital databases. Prehospital and in-hospital data from the CHU de Québec (which includes five of the six major EDs within our region and receives approximately 80% of all ED consultations in Quebec City) were combined.
Ethics
This project was approved by the CHU de Québec – Université Laval Research Ethics Board. Our results are reported as per the EQUATOR Network STROBE reporting guidelines. 19
Study population
Patients were included if they were transported by ambulance to one of the CHU de Québec EDs between November 2016 and March 2017 after having sustained a trauma for which an emergency medical services (EMS) intervention was required.
Patients with a documented terminal disease (prognosis < 6 months) and those who were misclassified (no history of trauma) were excluded after reviewing the patient’s medical record.
Outcome measures
Following a literature review, the study's steering committee, which included local trauma experts, agreed upon a list of six urgent and specialized trauma interventions (primary outcomes): (1) endotracheal intubation in the ED, (2) administration of ≥ 2 blood products in the ED, (3) angioembolization for a pelvic, spleen, hepatic and/or renal injury within 24 h of ED arrival, (4) urgent surgery within 24 h of ED arrival (excluding an orthopaedic surgery for one limb only), (5) initial admission to the intensive care unit (ICU) or intermediate care unit (IMCU) and (6) trauma-related deaths (in the ED or during the hospitalization). It was considered that patients requiring these interventions should be transported directly to a level one trauma centre and therefore, should be identified by the EQTPT protocol.
Our secondary outcomes were the proportion of over and undertriage. Overtriage was defined as a patient identified by one of the five steps of the EQTPT who did not receive any urgent and specialized trauma care. Undertriage was defined as a patient who required urgent and specialized trauma care but did not meet any of the EQTPT criteria. Furthermore, we measured over and undertriage proportions specifically for steps 1, 2 and 3, as those steps determined whether the patient was transferred to the level one trauma centre. Overtriage was thus defined as a patient who fulfilled at least one of the EQTPT's steps 1, 2 or 3 criteria, but did not require any specialized trauma care, while undertriage corresponded to a patient without any criteria in the first three steps but who ultimately required specialized trauma care.
Data extraction
Trained research assistants and medical students collected data using a standardized form. Sociodemographic data, trauma mechanism and the EQTPT criteria used to determine the patient's destination hospital were extracted from the prehospital record. In-hospital interventions, orientation, final diagnosis, ED and in-hospital length-of-stay (LOS) were extracted from the hospital record. All data pertaining to patients who underwent at least one specialized trauma intervention were reviewed by an experienced emergency physician and trauma team leader (EM).
Statistical analysis
We conducted a series of descriptive statistics (median, interquartile range (IQR)), frequencies and proportions). The sensitivity and specificity were computed with their 95% confidence intervals (CIs). All analyses were performed using Excel™ and Statistical Analysis System software (SAS Institute, Cary, North Carolina, USA, v. 9.4).
Results
A total of 902 patients were included in our analyses. The median age was 63 (IQR 51) years, and 54.8% were female (Table 1). The main trauma mechanism was falls (65.6%), followed by motor vehicle accidents (22.5%); those transported directly to a level one trauma centre accounted for 40.7% of our patients. Most patients (71.9%) were discharged home from the ED, while 23.9% were admitted to the hospital (Table 2). There were 13 trauma-related deaths in our cohort, of which 10 were due to a fall from a standing position.
Prehospital characteristics of the 902 patients included in the study.
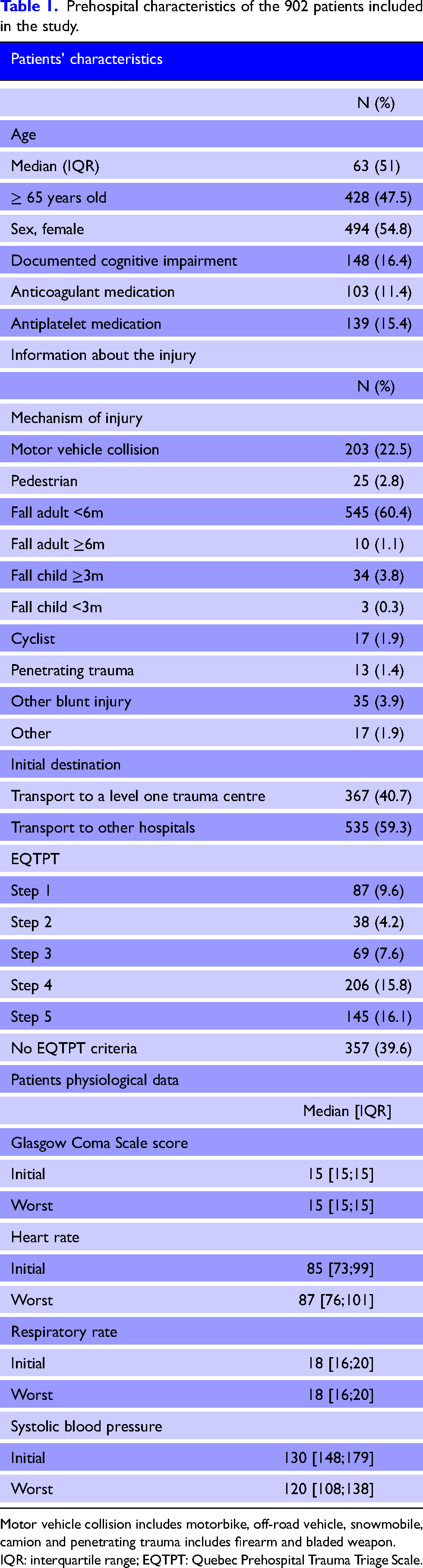
Motor vehicle collision includes motorbike, off-road vehicle, snowmobile, camion and penetrating trauma includes firearm and bladed weapon.
IQR: interquartile range; EQTPT: Quebec Prehospital Trauma Triage Scale.
Hospital characteristics of the 902 patients included in the study.
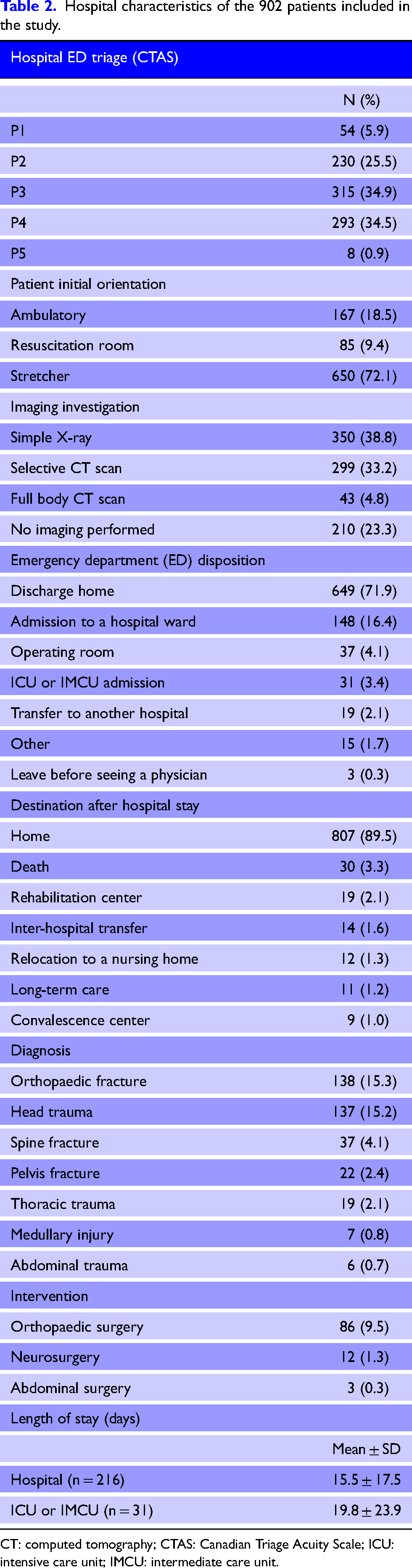
CT: computed tomography; CTAS: Canadian Triage Acuity Scale; ICU: intensive care unit; IMCU: intermediate care unit.
Primary outcome
Of the 902 included patients, 555 (61.5%) met at least one of the trauma triage protocol criteria, and 194 (21.5%) met at least one criterion from the first three steps of the protocol. Step 4 (special considerations) included the most patients with 206 (22.8%) of the whole cohort.
A total of 82 patients (9.1%) required urgent and specialized trauma care. Urgent surgery (58.5%) and admission to ICU or IMCU (57.3%; ICU: 23, IMCU: 24) were the most frequent. Only one massive transfusion protocol was activated among the seven patients who received at least two blood products in the ED. Table 3 shows the interventions and patient outcomes of our population.
Description of urgent and specialized trauma interventions.
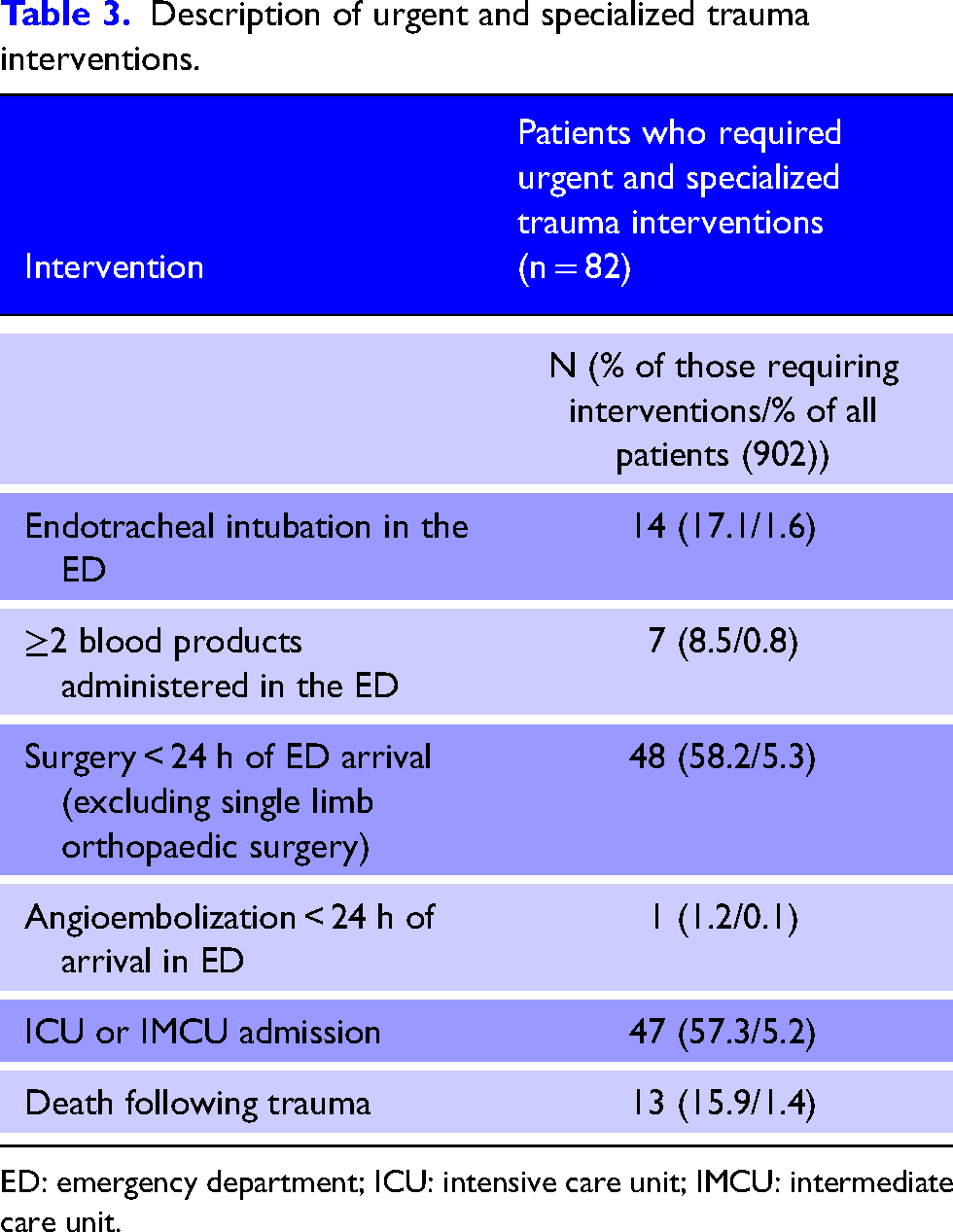
ED: emergency department; ICU: intensive care unit; IMCU: intermediate care unit.
Patient triage according to EQTPT steps.
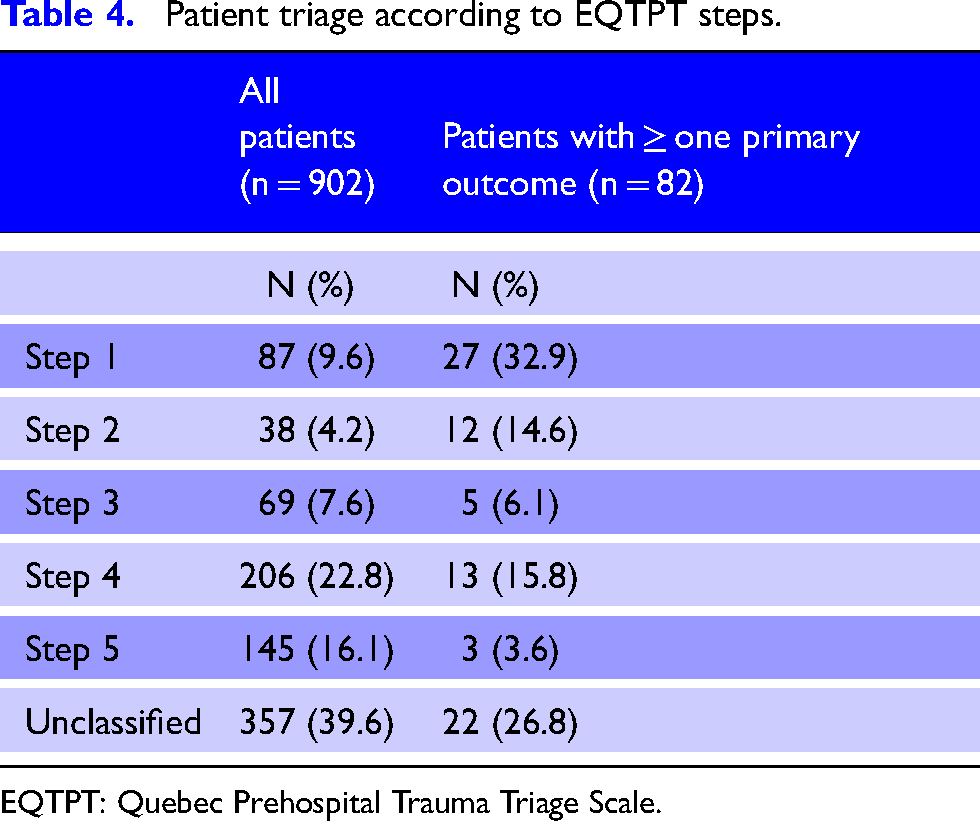
EQTPT: Quebec Prehospital Trauma Triage Scale.
The first EQTPT step identified 32.9% of patients requiring specialized trauma care. When using the first three steps only, the protocol identified 53.7% of patients and 72.9% when using all five steps. Finally, 22 patients (26.8%) who required in-hospital specialized trauma care were not identified by any of the triage protocol's steps (Table 4).
Secondary outcomes
A total of 150 patients met at least one criterion from steps 1 to 3 but ultimately did not require specialized trauma care. For those steps, the sensitivity was 53.7% (95% CI: 42.9–64.4) and the specificity was 81.7% (95% CI: 79.1–84.4). The overtriage proportion was 18.3% while the undertriage was 46.3%.
When using all five steps of the protocol, the overall sensitivity was 73.2% (95% CI: 63.6–82.8), and the specificity was 40.9% (95% CI: 37.5–44.2), with an overtriage proportion of 59.1% and an undertriage of 26.8%.
Discussion
This is the first study investigating the accuracy of our field trauma triage protocol in a general trauma population since its implementation in 2016. Accurate trauma triage is a cornerstone of an efficient trauma system. The overarching objective of a triage protocol is to send the right patient quickly to the appropriate place based on their needs. The EQTPT protocol accurately identified 53.7% of patients needing specialized care in a level one trauma centre.
The EQTPT was based on the CDC-ACSCOT protocol and was adapted to the needs of the Quebec trauma population. Indeed, the CDC-ACSCOT protocol was created and implemented in the United States, where the proportion of penetrating trauma is higher (compared to less than 3.5% in the province of Quebec 20 and only 1.4% in our study). Given the differences in demographics and trauma mechanisms, an American triage protocol might not be suited to our trauma population; hence, the differences between the two protocols include some minor adjustments (units of measure) and the addition of a fifth step. Like other available prehospital trauma triage protocols, 17 the overall EQTPT does not meet the benchmarks set by the CDC-ACSCOT. 21 The consequences of undertriage are well documented and include delayed treatment, missed injuries and poor functional outcome.3,22 The latest version of the CDC-ACSCOT has a reported 77% specificity and a 72% sensitivity. 23
When considering the accuracy of the EQTPT in identifying patients who require specialized trauma care, steps 1 to 3 obtained an 18.3% overtriage proportion and 46.3% undertriage. These three steps performed fairly well with regard to the recommended CDC-ACSCOT overtriage proportions. However, several patients who would have required acute trauma care were missed, resulting in a proportion of undertriage exceeding the recommended 5%. The first two steps of the CDC-ACSCOT have a reported undertriage of 51% and an overtriage of 22%, 24 which is similar to the results from the first three steps of the EQTPT. Therefore, there is a clear need to improve the current prehospital triage protocols for trauma patients. Modifying a few EQTPT criteria could likely improve its accuracy. Older adults are at higher risk of undertriage 25 than younger patients. In a study limited to older adults, we have previously reported that the EQTPT's sensitivity is low in patients > 65 years old and only 30% to identify patients ≥ 75 years old requiring specialized trauma care. 26 Hence, including senior-friendly modifiers could improve the protocol's sensitivity for this age group. 27 Furthermore, identifying head-injured patients can also be challenging in the prehospital setting, and a recent systematic review reported that prehospital trauma triage protocols lack sensitivity in identifying those patients. 28 The EQTPT includes four criteria pertaining to head injury (step 1: GCS ≤ 13; step 2: skull fracture; step 4: anticoagulation; step 5: traumatic brain injury with vomiting, loss of consciousness or post-traumatic amnesia). Additional criteria, such as external signs of head trauma or antiplatelet medications, have been suggested to improve the sensitivity of triage tools.29,30
Historically, the performance of prehospital trauma triage protocols was solely based on their capacity to distinguish severely injured patients from those who sustained minor injuries. However, the definition of severe trauma varies widely in the literature, and up to 14 indicators have been described. 31 Most prior studies defined severe trauma as an Injury Severity Score (ISS) > 15. 32 Nevertheless, an evaluation based on anatomic severity only (i.e. ISS score) is suboptimal because it poorly relates to the trauma resources needs, especially in acute settings. 33 For this reason, we have decided to use a consensus-based and more restrictive outcome definition to capture patients with higher acute trauma resource needs. Furthermore, studies on prehospital trauma triage protocols are often limited to patients transported to a centre with a higher level of trauma care designation. As most trauma patients only sustain minor injuries, we chose to include all trauma patients within one region to decrease the risk of selection bias.
Limitations
Our study has some limitations. First, data were collected following the EQTPT implementation in 2016 and 2017. Considering the possible lack of familiarity with this new protocol, it is possible that some patients were incorrectly categorized or not sent to the appropriate centre. It is unknown if more recent data would have brought different results. The second limitation is the fact that results are limited to the Capitale-Nationale region – Quebec, which only includes a single-level one trauma care centre. Future similar research should consider more rural regions to provide a more comprehensive assessment of the accuracy of the EQTPT at a provincial level. Furthermore, comparing our results with other studies is difficult, considering the lack of a standardized definition to identify trauma patients who need urgent and specialized care. As previously mentioned, most studies on trauma triage protocols rely on ISS assessments. A resource-based outcome was believed to be more useful to capture patients who would benefit the most from receiving specialized trauma care from a level one trauma centre.
Conclusion
In conclusion, the EQTPT protocol, inspired by the CDC-ACSCOT is insufficiently sensitive and poorly specific to identify patients who require specialized and urgent care in a level one trauma centre. Future research should aim at improving current protocols or developing new and more performant triage tools.
Declaration
Supplemental Material
sj-docx-1-tra-10.1177_14604086231156263 - Supplemental material for Performance of a provincial prehospital trauma triage protocol: A retrospective audit
Supplemental material, sj-docx-1-tra-10.1177_14604086231156263 for Performance of a provincial prehospital trauma triage protocol: A retrospective audit by Roxane Beaumont-Boileau, Alexandra Nadeau and Pier-Alexandre Tardif, Christian Malo, Marcel Emond, Lynne Moore, Julien Clément, Eric Mercier in Trauma
Footnotes
Conflicting of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Département de médecine familiale et médecine d’urgence de la Faculté de médecine de l’Université Laval.
Ethical approval
This project was approved by the CHU de Québec Research Ethics Board. Our results are reported as per the EQUATOR Network STROBE reporting guidelines.
Informed consent
Informed consent was not needed for the present study as it was a retrospective study with little risk for the patient.
Contributorship
EM and RBB conceived the study and wrote the study protocol with inputs from all other authors. EM, AN and RBB developed the data extraction sheet. RBB was in charge of the data extraction with oversight by EM, ME, JC and CM. PAT performed the statistical analysis with inputs from all other authors. RBB, AN and EM drafted the manuscript, and all authors contributed substantially to its revision. EM takes responsibility for the paper as a whole.
Acknowledgements
We would like to acknowledge the contribution of Maxime Arbour, Isabella Mercier, Florence Cantin, Marion Fournier, Marie-Philippe Gauvin, Kahina Ait Zaid, Marie-Laurence Ouellet-Pelletier, Philippe Pelletier, Cristina Nebunescu and Madeleine Picard-Moreau in extracting the data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.