
Abstract
Introduction
Resuscitative thoracotomy (RT) is an emergent procedure to gain access to the thoracic cavity to control hemorrhage and other life-threatening injuries. Data predicting survival is variable. This review aims to highlight key predictors of survival and mortality following RT.
Methods
The EMBASE database was searched using the following terms: [exp. Thoracotomy] AND [Trauma.mp] AND [exp. Survival OR exp. Mortality]. The search was limited to full-text articles in the English language and publications released up to February 27, 2022. Reference lists of included articles were reviewed to identify other studies meeting inclusion criteria.
Results
Thirty-seven studies were included. Seventy-six outcome predictors were identified. Prehospital outcome predictors included prehospital vital signs, police transport, cardiopulmonary resuscitation, application of a cervical spine collar, and the number of total prehospital procedures performed. In-hospital variables associated with survival included traumatic cardiac arrest (TCA) in the emergency department (ED), initial ED vital signs and cardiac rhythm, Shock Index Pediatric Age-Adjusted score, location of RT, duration of RT, Focused Assessment with Sonography in Trauma findings, amount of blood products, and amount of administered fluids.
Conclusions
Our study highlights the disparity of data regarding prehospital outcome predictors for trauma patients requiring RT. Most studies focus on injury-specific and in-hospital variables and do not explicitly look at the TCA population. Further work is needed to better define specific variables implicated in enhanced survival across different care settings and to inform management guidelines within these clinical areas.
Keywords
Introduction
Traumatic injuries are one of the leading contributors to disease burden worldwide. 1 As trauma systems advance and management in prehospital and in-hospital settings evolve, an increasing number of studies are evaluating factors implicated in survival, with a goal of further optimizing trauma care. Although blunt and penetrating thoracic injuries make up approximately 25–50% of traumas, only 10–15% require resuscitative thoracotomy (RT) as part of the initial resuscitation.2,3 Previous studies have identified overall poor outcomes following RT, particularly in the context of blunt injuries when compared to penetrating trauma.4–8 Additionally, several factors have been linked to lower likelihoods of survival, including the performance of RT more than 30 min after hospital arrival, RT in the context of traumatic cardiac arrest (TCA), the patient's clinical status on emergency department (ED) arrival, RT procedure duration, heart rate (HR) at the end of the procedure, absence of signs of life (SOL) on-scene or in the ED, and cardiopulmonary resuscitation (CPR) duration.9–13 However, to date, data have primarily focused on in-hospital and injury-specific variables and literature that synthesizes what we know about outcome predictors in the trauma population following RT is lacking. Additionally, there is a scarcity of studies that provide a breakdown of data based on different care settings (i.e., prehospital and in-hospital). Therefore, this review aims to highlight key outcome predictors following RT in both care settings that have been identified in existing literature, while concurrently evaluating the breadth of data that exists in this area.
Methods
A literature review was conducted using the EMBASE database, with further review of included papers’ reference lists to extract additional studies that meet inclusion criteria. The following search terms were applied: [exp. Thoracotomy] AND [Trauma.mp] AND [exp. Survival OR exp. Mortality]. The search was limited to full-text articles in the English language and publications released up to February 27, 2022. We included all primary research studies that qualitatively or quantitatively evaluated the predictive value of one or more prehospital, in-hospital, patient or injury-specific characteristics in survival, mortality or return of spontaneous circulation (ROSC) of trauma patients post-RT. The following exclusion criteria were applied: (1) Inability to access the full-text article and (2) systematic reviews, meta-analyses, case reports, animal-based studies, conference proceedings, and letters to editors.
All titles and abstracts were reviewed by two authors (N.R. and R.W.) and included based on the above criteria. Full-text review was subsequently undertaken individually by N.R. and R.W. to extract the following data: publication year, publication country, publication type, whether TCA was an inclusion or exclusion criteria, prehospital variables (prehospital systolic blood pressure [SBP], diastolic blood pressure [DBP], HR, SOL [defined as organized electrical activity, pupillary response, spontaneous respiratory attempts or movement], HR, SBP, or respiratory rate [RR]12,14), in-hospital variables, patient characteristics and injury characteristics. For all identified characteristics, we extracted the following associated statistical values: sensitivity, specificity, odds ratio, relative risk, and area under the receiver operating curve (AUROC) with 95% confidence interval (CI) or p values.
Results
Study selection and demographic characteristics
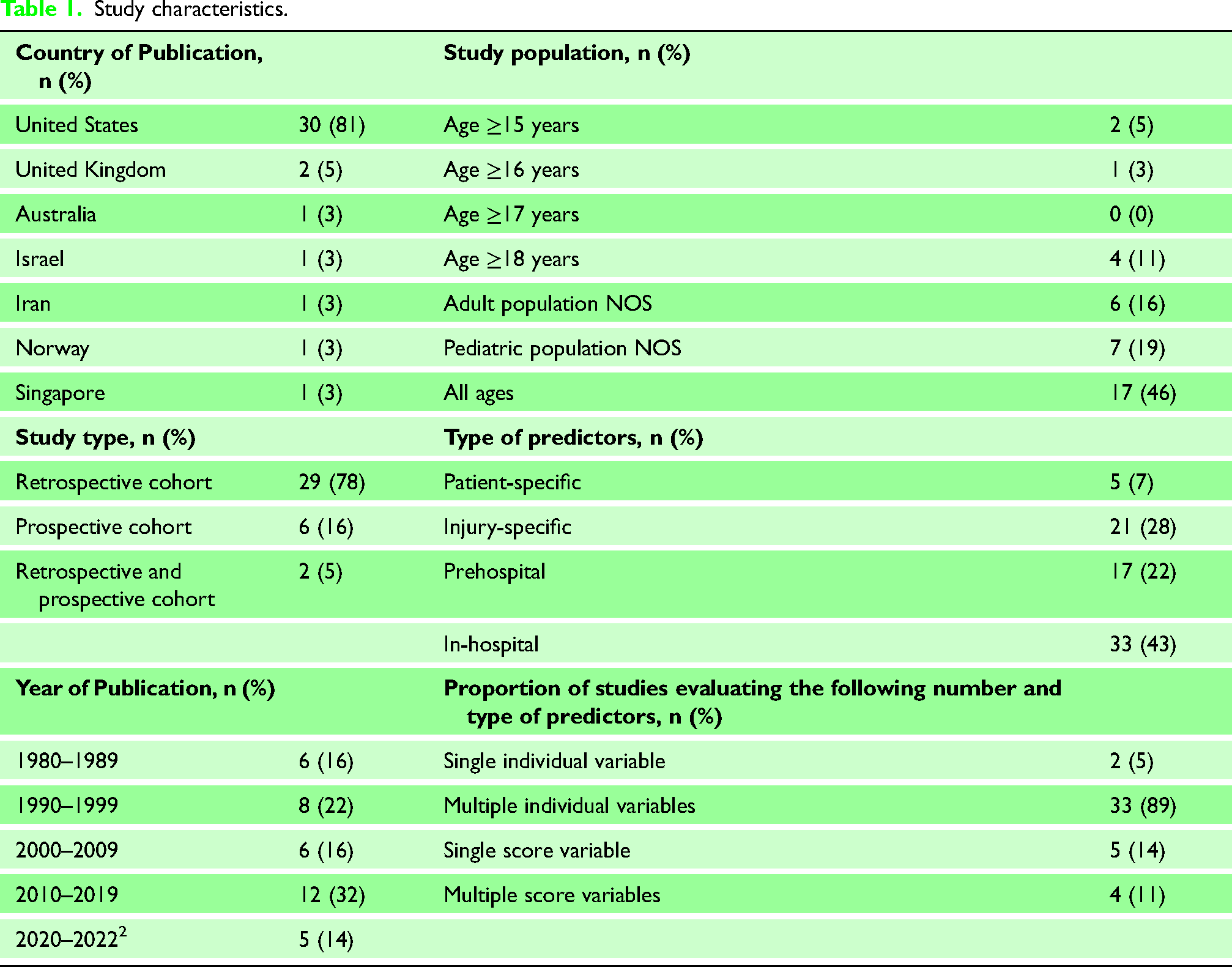
After applying the search strategy and limitations, we retrieved a total of 204 articles (Figure 1). A total of 37 studies were included in this scoping review. A detailed list of study demographics is shown in Table 1.
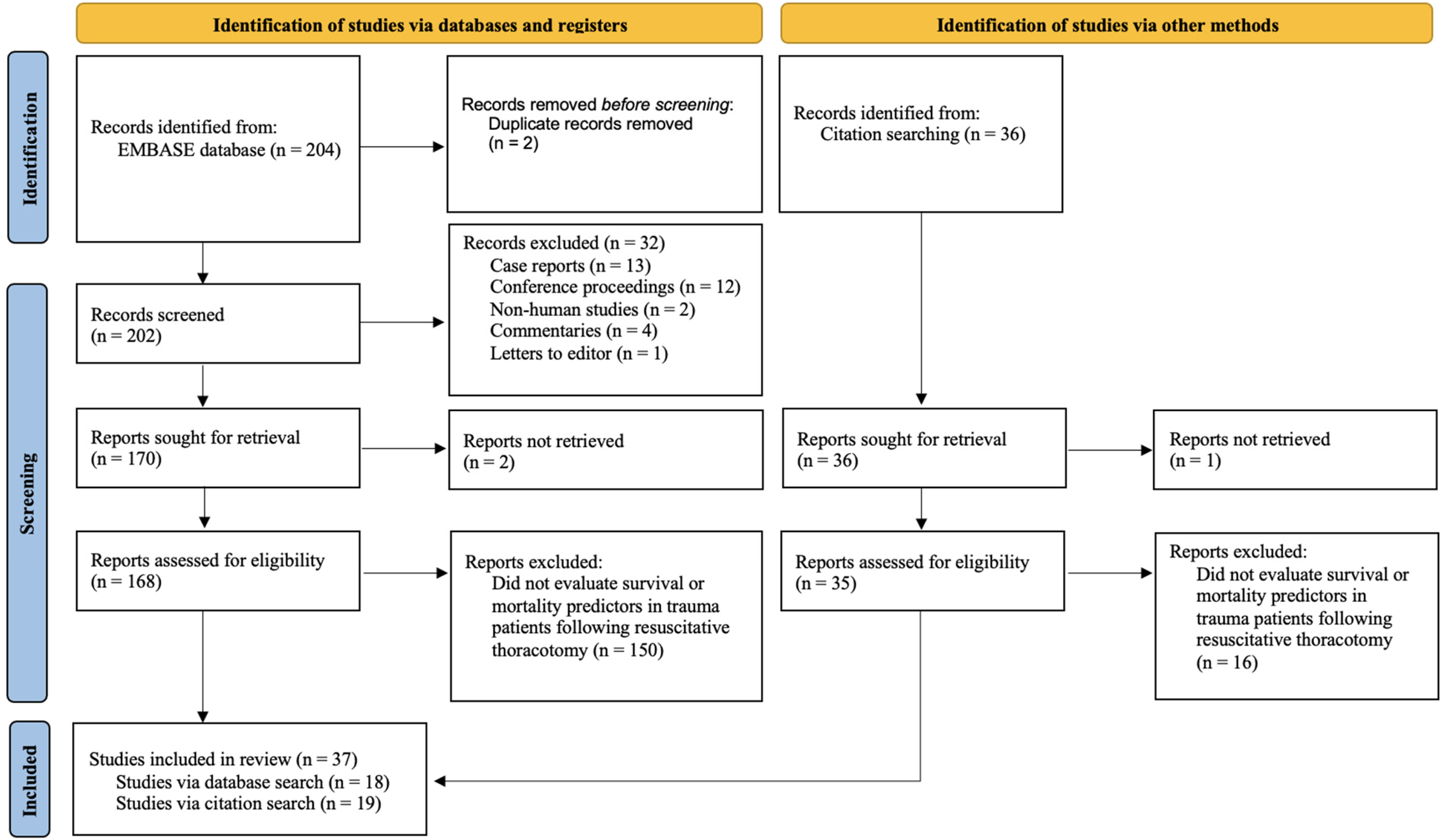
PRISMA flow diagram of study screening and selection. 15
Study characteristics.
All outcome predictors and statistical properties
A total of 76 outcome predictors were identified (86% individual variables and 14% score variables) (Table 1). Age, sex, and mechanism of injury were the most evaluated factors throughout all studies. Over three-quarters of studies relied on methodology that incorporated multiple individual variables into their analysis. We identified considerable heterogeneity in primary outcome measures that were reported. Specifically, 78% of studies looked at survival as the primary outcome measure, with the following breakdown of specific survival parameters: survival to hospital discharge (45%), survival to hospital discharge without neurological deficits (7%), survival to hospital discharge or to organ donation (3%), 30-day survival (3%), survival to intensive care unit admission (7%), and survival not otherwise defined (34%). Conversely, 22% of studies reported on mortality as the primary outcome measure, with the following breakdown of specific mortality parameters: 30-day mortality (25%), in-hospital mortality (25%), and mortality not otherwise defined (50%). We did not identify any studies that evaluated ROSC as the primary outcome measure. Lastly, we identified a proportion of studies (24%) relying on descriptive methodology (i.e., frequency and percentages) to define the predictive ability of various factors. Of the remaining studies that explicitly defined statistical properties of variables, they predominantly reported ORs and RRs, and only a single study evaluated sensitivity and specificity. AUROC was not reported in any study.
Patient and injury outcome predictors
When looking at reported statistical properties of all patient- and injury-specific variables, sex, race, mechanism, extra-thoracic injury, injury severity score (ISS), arrest rhythm, initial cardiac rhythm, ROSC at any time, Revised Trauma Score (RTS), and Cardiovascular Respiratory Score (CVRS) were the most significant outcome predictors (Supplementary Online Material, Tables 2 and 3). Patient sex (Survival to hospital discharge: OR 2.90, 95% CI: 0.53–15.88) 16 and mechanism of injury (Stab wound, survival to hospital discharge: OR 11.11, 95% CI: 3.72–33.20) 17 had the highest documented OR of all patient- and injury-specific variables pertaining to survival, respectively.
Prehospital and in-hospital outcome predictors
Prehospital outcome predictors that were noted to be statistically significant included SBP, HR, vital signs lost on-scene or enroute to hospital, prehospital intubation, SOL, Glasgow Coma Score (GCS), police transport, CPR, the application of a cervical spine collar, and the number of total prehospital procedures performed (Supplementary Online Material, Table 4). Police transport to hospital had the highest documented OR of all prehospital predictors (Survival to hospital discharge without neurological deficit: OR 9.08, 95% CI: 1.07–77.00). 17 Conversely, arrest in the ED, initial ED cardiac rhythm, SBP, HR, SOL, Shock Index Pediatric Age-Adjusted score, location of RT (ED vs. operating room (OR)), duration of RT (as a measure of time), Focused Assessment with Sonography for Trauma exam, amount of blood products, and amount of administered fluids were significant in-hospital variables (Supplementary Online Material, Table 5). HR in the ED had the highest documented OR of all in-hospital predictors (Survival: OR 44.70, 95%CI 13.2–151.4) for post-RT survival. 18 The location of RT had the highest documented RR (Mortality: 3.25, 95% CI: 2.21–4.76), with greater mortality being noted following RT performed in the ED compared to in the OR. 19
Discussion
Our study highlights the disparity of data available when contrasting demographic variables with prehospital and in-hospital outcome predictors, which is even more pronounced in the prehospital setting. Existing data predominantly focus on injury and patient variables, and most studies do not explicitly look at the TCA population.
The use of thoracotomies for resuscitation of trauma patients with penetrating or blunt traumatic injuries continues to be controversial, owing to a high amount of material and personnel resource utilization, low overall survival rates, and potential exposure of staff to bloodborne pathogens.20,21 Despite this, RT can be lifesaving with excellent long-term outcomes, particularly for patients with penetrating mechanisms of injury presenting to the ED with SOL or vital signs. As such, the Western Trauma Association and the Eastern Association for the Surgery of Trauma advocate for the performance of RT when specific—and slightly varying—indications are met. 22 Based on our scoping review of existing literature, we can conclude three major findings in the context of RT: (1) RTs performed in the setting of blunt trauma have a worse prognosis compared to patients undergoing RT for penetrating injuries, (2) procedures that have the potential to delay patient transport to hospital, such as intubation, may significantly increase the risk of mortality (Prehospital intubation, survival to hospital discharge: OR < 0.001, 95% CI: <0.01–0.05 16 ; number of prehospital procedures, survival to hospital discharge: OR 0.38, 95% CI: 0.18–0.79 16 ), and (3) the presence of SOL or hemodynamic stability in the prehospital or in-hospital setting are positive survival predictors in the setting of RT (In-hospital SOL, survival to hospital discharge: OR 13.32, 95% CI: 9.27–19.15) 14 ; prehospital HR < 60 bpm, mortality: OR 3.43, 95% CI: 1.73–6.79 23 ; in-hospital pediatric hypotension (based on SBP), mortality: OR 2.10, 95% CI: 1.10–4.00. 18
The most recently published systematic review on survival predictors following RT that was identified through our literature search was limited to independent patient- and injury-specific factors and did not look at multiple factors in the context of various clinical settings (i.e., whether vital signs or SOL were lost in the field vs. in-hospital, field interventions). 22 Additionally, a major portion of studies that met inclusion criteria in the present review provided only qualitative analyses of factors contributing to the survival or mortality of trauma patients following RT. In combination, the capacity of these studies to inform future clinical guidelines on the use of RT in different settings, including prehospital management for emergency medical services (EMS) personnel, and more precisely defining RT indications for trauma teams, is limited. This scoping review summarizes existing data in the form of quantitative predictive abilities of variables, while concurrently delineating findings based on prehospital, in-hospital, patient-specific, and injury-specific outcome measures.
Limitations
There are several limitations to the present review that should be acknowledged. First, the search strategy used was applied to a single database; therefore, it is expected that our review did not capture all available studies regarding outcome predictors in this trauma population. Additionally, most studies originated from the United States, limiting our ability to account for geographic and regional variations of confounding factors (i.e., different patient demographics and management practices) as well as impacting the overall generalizability of data. Lastly, it is important to note the heterogeneity of outcome measures that were reported in identified literature. Specifically, many studies reported data using different survival definitions (i.e., 30-day survival, survival to hospital discharge, unspecified survival) and mortality (in-hospital mortality, 30-day mortality, unspecified mortality). Therefore, these inconsistencies can create challenges when attempting to compare data between literature and develop meta-analyses in this area.
Future directions
Our study has identified numerous gaps in existing literature pertaining to RT outcomes. Specifically, we have identified an overall scarcity of data pertaining to quantitative evaluation of predictors. Similarly, most studies did not use TCA as an inclusion criterion. Given that a large subset of patients undergoes RT in the setting of TCA, future studies investigating the impact and quantitative predictive value of prehospital factors on survival following RT in TCA would be valuable to delineate potentially beneficial prehospital interventions and metrics. There is current work on defining patient-centered “textbook” outcomes in the setting of trauma. 24 Similar work on creating expert-based patient-centered standardized outcomes related to RT could be helpful in comparing future studies. Furthermore, stratifying the abovementioned data into both adult and pediatric subgroups, and additionally encouraging global work with increased geographic diversity, may facilitate the application of this knowledge to a broader patient population.
Conclusion
In summary, our study has highlighted the limits of current data regarding outcome predictors in the trauma patient requiring RT. We identify many patient-specific, mechanism of injury, and management variables that may impact survival from RT. Further studies defining outcomes or predictors of survival from RT could better inform clinical decision tools and develop prehospital management guidelines to improve overall survival.
Declaration
Supplemental Material
sj-docx-1-tra-10.1177_14604086231156265 - Supplemental material for Predictors of survival in trauma patients requiring resuscitative thoracotomy: A scoping review
Supplemental material, sj-docx-1-tra-10.1177_14604086231156265 for Predictors of survival in trauma patients requiring resuscitative thoracotomy: A scoping review by Nada Radulovic, Richard Wu and Brodie Nolan in Trauma
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Trial registration
Not applicable.
Contributorship
NR, RW and BN conceived and designed the study and obtained research ethics approval. NR and RW performed data collection and analysis. NR and RW drafted the manuscript, and all authors contributed extensively to its revision and final approval.
Acknowledgements
We acknowledge the invaluable support and contributions from Melissa McGowan, our research coordinator.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.