
Abstract
Introduction
Requirement for blood transfusion in the injured paediatric civilian population is rare. Therefore, a substantial evidence base underpinning damage control resuscitation (DCR) in paediatric patients is lacking. Published outcome data originating from Iraq and Afghanistan offer a unique opportunity to study large cohorts of children who received DCR. It is hoped that by collating the data, this review will inform pre-deployment medical training and support the development of paediatric specific DCR guidelines, which can be used in all trauma environments.
Methodology
A comprehensive search of the literature was conducted using online databases, grey literature searching and screening of reference lists. Papers discussing blood product, crystalloid or tranexamic acid (TXA) administration in paediatric patients injured in Iraq and Afghanistan from 2001to present were included.
Results
Eighteen papers were included – all were retrospective studies of data from military trauma databases. Most children that received massive transfusion were male (73.4%), injured in Afghanistan (69.9%) by explosives (60.4%) with a median age of 9 years. A definition of paediatric massive transfusion of 40 ml/kg of all blood products within 24 h was developed. Massive transfusion rates were high (15.7% of children). Whole blood administration occurred in 4% of patients requiring blood transfusions. Low crystalloid volumes in combination with balanced blood product ratios were associated with improved survival, along with the use of whole blood and TXA.
Conclusion
The review offers insight into the paediatric population likely to require DCR and the optimal DCR strategies to be used in their management.
Introduction
Damage control resuscitation (DCR) is a strategy that aims to restore haemostasis and maintain tissue oxygenation through various methods including permissive hypotension, balanced blood product transfusion, tranexamic acid (TXA) administration and prevention of hypothermia. 1 Damage control surgery, which can be defined as “abbreviated surgery to control blood loss and contamination, … simultaneous resuscitation of physiology, and definitive surgical management at a later stage after restoration of the physiology” is often carried out as part of DCR. 2 DCR is a concept developed by the military and became common practice in 2004 when a Clinical Practice Guideline was introduced that advocated the principles of DCR. 3 One systematic review 4 demonstrated that the use of a DCR protocol reduced mortality in haemorrhaging adult patients compared with those treated without a DCR protocol. There is, however, limited evidence on the use of these techniques in children.
Children formed a significant portion of the trauma patients admitted to US and British military facilities during the Iraq and Afghanistan conflicts: the Department of Defense Trauma Registry (DoDTR) documented care of 3,439 paediatric patients over nine years which equated to 8% of all casualties, 5 whilst Spinella et al. 6 reported that children made up 11% of trauma admissions that required a blood transfusion.
Blood transfusion, particularly massive transfusion, is uncommon in paediatric civilian populations hence the topic lacks substantial evidence. 7 The European Resuscitation Council (ERC) provides a brief summary of haemorrhagic shock management to be used in civilian paediatric trauma. 8 Resuscitation should focus on improving coagulation with a balanced ratio of fresh frozen plasma (FFP) to packed red blood cells (PRBC); crystalloid boluses should be limited and a dose of 15–20 mg/kg of TXA should be administered within three hours of injury. These guidelines are mainly based on paediatric observational studies 9 and with specific injury patterns such as head, 10 spleen or liver injury. 11 Hence, research on the benefit of these techniques in children is not as comprehensive as the adult population.
The Iraq and Afghanistan conflicts, during which high rates of massive transfusion occurred, 12 therefore, offer a unique opportunity to investigate this issue further: the DoDTR has one of the largest sets of data on paediatric blood transfusion that has ever existed. 13 Conclusions from these data could support the development of both military and civilian paediatric DCR guidelines, ultimately helping to save the lives of severely injured children.
Components of DCR
A key element of DCR is haemostatic transfusion, that is, the use of balanced blood products that mimic the composition of whole blood using a 1:1:1 ratio of FFP: Platelets (PLT): PRBC. 1 In adult studies, such as the Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) trial, 14 it remains unconfirmed whether an FFP:PLT:PRBC ratio of 1:1:2 or 1:1:1 is more beneficial for survival. The optimum ratio of blood products in children is even less certain. 15
An alternative to balanced blood product resuscitation is warm fresh whole blood (WFWB), which tends to be used in rare emergency military situations when blood components are not available. 16 Analysis of combat-related trauma in the adult population has shown survival benefits in patients receiving whole blood 17 although the use of whole blood in civilian populations remains controversial for many reasons; one being the increased risk of infection transmission. 18 The effect of whole blood on survival in children is yet to be determined.
Another element of DCR is limiting the use of crystalloids. Aggressive use of crystalloids has been shown to worsen coagulopathy in trauma patients 19 through haemodilution of platelets and coagulation factors. 20 Similar findings have been identified in civilian paediatric patients 21 ; however, data on children injured through conflict is limited.
TXA is an anti-fibrinolytic that inhibits the conversion of plasminogen to plasmin, blocking fibrinolysis. 22 The Clinical Randomization of an Antifibrinolytic in Significant Hemorrhage-2 (CRASH-2) trial 23 of civilian patients found that administration of TXA reduces all-cause mortality in bleeding adults. In the paediatric population, evidence of benefit with a reduction in blood loss is limited to elective surgery in a civilian setting.24–26
Differences between adults and children
The use of adult DCR strategies not yet validated in the paediatric population is common, despite differences in adult and paediatric physiology. 27 Children demonstrate a higher physiological reserve than adults and thus can maintain normal blood pressure for longer despite substantial blood loss. 28 Use of vital signs as the sole criteria for activating massive transfusion protocol in children is likely to be unreliable. 29 Establishing standardised criteria for the activation of massive transfusion protocol in children is paramount. Many hospital systems have paediatric massive transfusion protocols in place but protocol activation is often governed by physician discretion with significant variability. 30
Paediatric DCR presents additional challenges regarding equipment sizing and dose calculations. Volumes of blood products and crystalloids as well as medication dosages must be accurately calculated based on a child's weight and administered through smaller angiocatheters. 31 The ability of medical teams to adapt to paediatric patients is dependent on their confidence and competence in the equipment, procedures and calculations required and thus familiarisation with these skills is essential in pre-deployment training.
Aims and objectives
The primary aim of the review is to analyse the data on paediatric patients from the Iraq and Afghanistan conflicts to identify the DCR strategies used and their effect on outcomes to inform best practice for the management of paediatric casualties in both future conflict and non-conflict situations.
In order to achieve this, the following objectives are addressed:
Collection of data on the demographics of the paediatric patient population receiving DCR during the conflicts. Quantification of the frequency of application of DCR strategies – including blood product, whole blood, crystalloid and TXA administration. Analysis of whether the principles of DCR used in adults also showed a survival benefit in the paediatric population.
Methodology
A review of the literature was performed using the databases Scopus (Embase), PubMed and Cochrane Library. Figure 1 details the search strategy used. In PubMed, both the full term (paediatric) and the truncated term (paed*) were used when searching to include all MESH terms for the word as well as all alternative endings. The search was limited to literature in English that had been published from 2001 to present. This time frame was chosen because the wars in Iraq and Afghanistan started in 2003 and 2001, respectively. The search was carried out in January 2022. The Google Search Engine was also used to identify additional grey literature relevant to the review.

Combination of terms forming the search strategy.
Following the completion of the search, all duplicates were removed. The remaining results were screened based on their titles and abstracts. Full-text articles were then reviewed, applying the eligibility criteria detailed in Figure 2. Papers that met all of the inclusion criteria, and none of the exclusion criteria were included. The reference lists of included articles were screened but none were deemed applicable for this review.
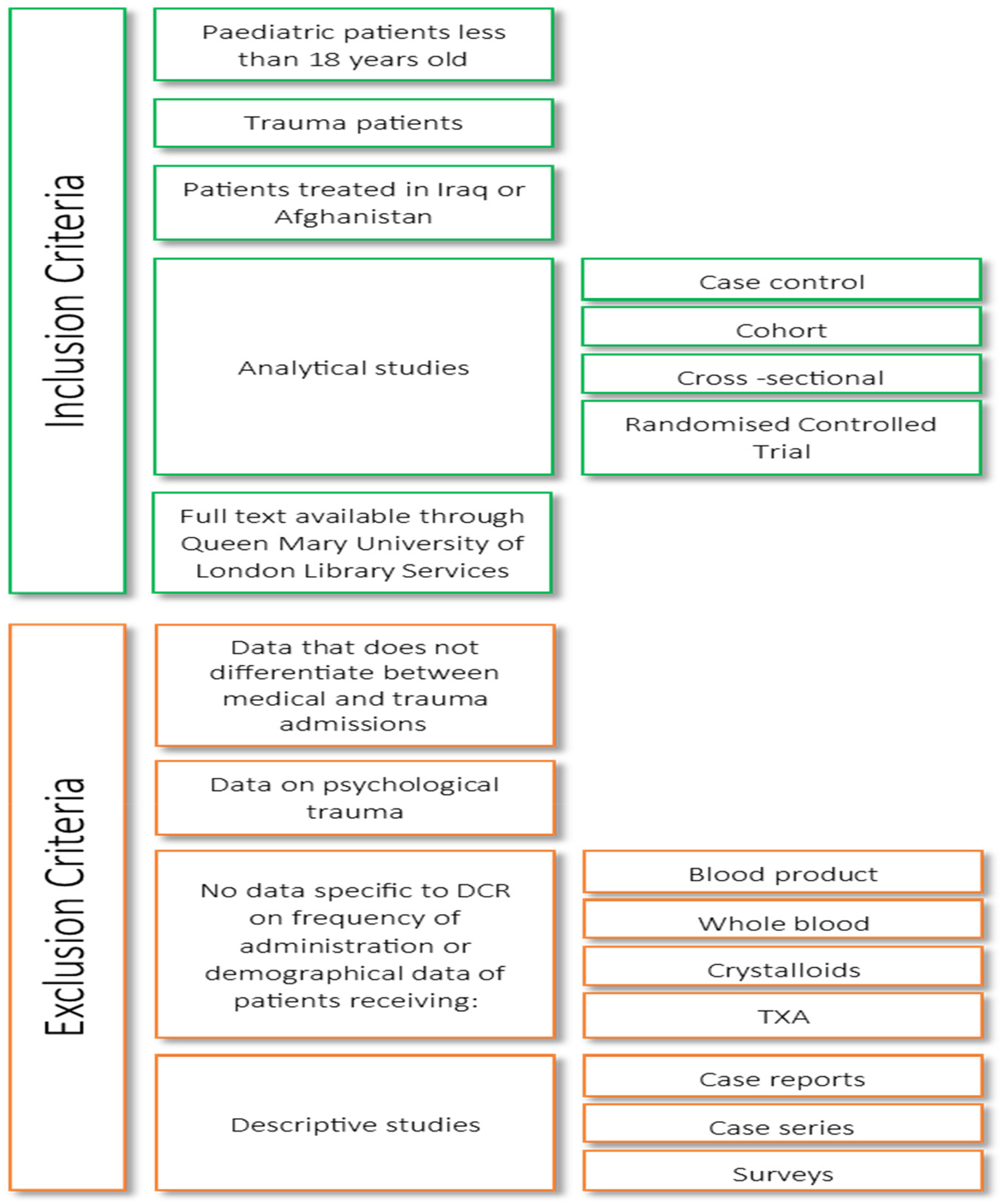
Inclusion and exclusion criteria.
Studies had to provide data on one or more of the following outcomes of interest:
Demographics of paediatric trauma patients (age, sex, mechanism of injury, location) DCR in the prehospital setting, ED or ITU Blood component administration and/or massive transfusion Effect of blood product ratios on survival Use of whole blood Crystalloid administration TXA administration
Results
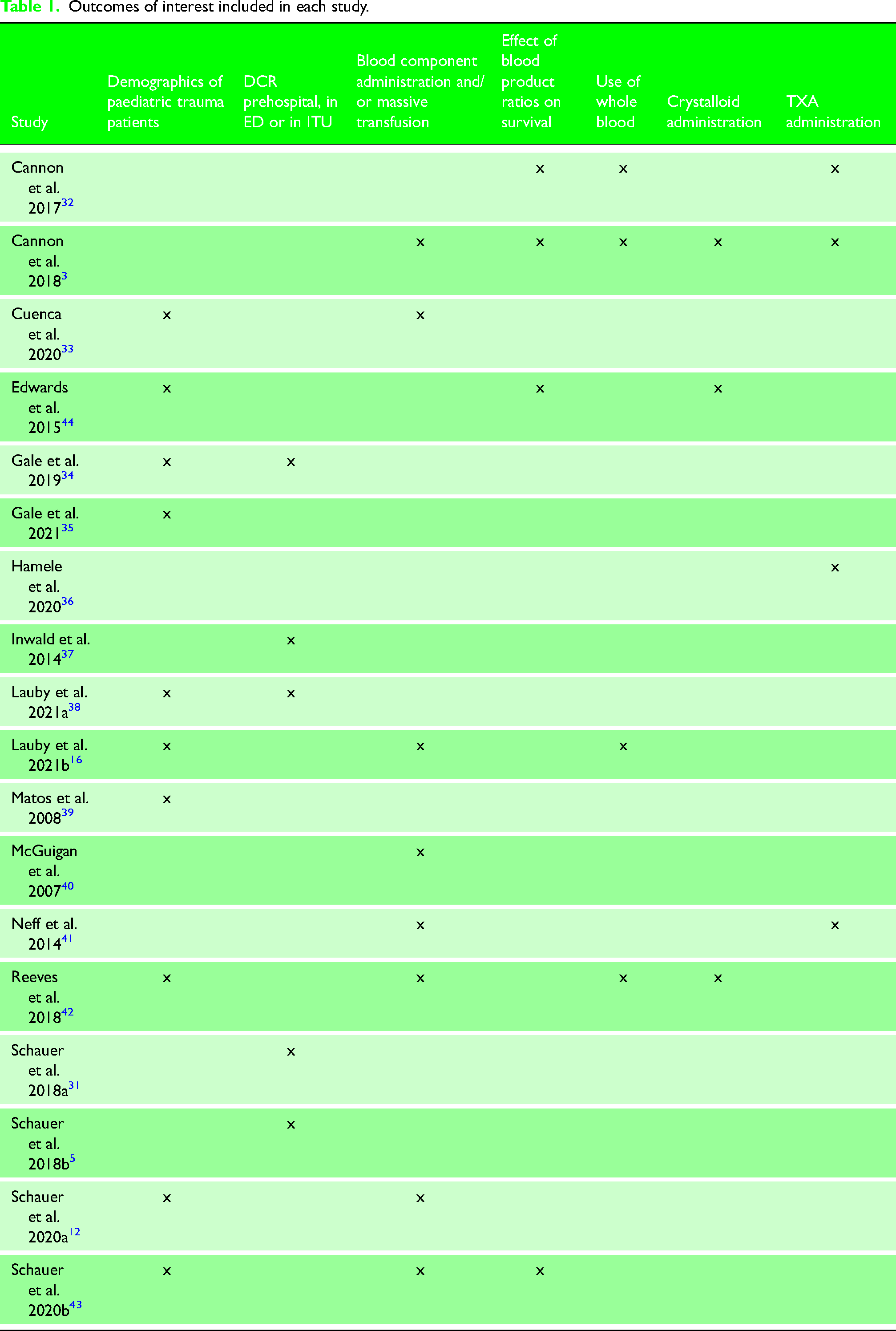
The database searches and search of grey literature yielded 1,407 non-duplicate results. Titles and abstracts were screened leaving 145 records. Exclusion criteria were then applied to the remaining papers by reading the full text to identify 18 articles3,5,12,16,31–44 to be used in the review. This process is described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart below (Figure 3). 45 Table I (Supplementary Online Material) describes the characteristics of the studies identified, and Table 1 outlines the outcomes of interest included in each study.
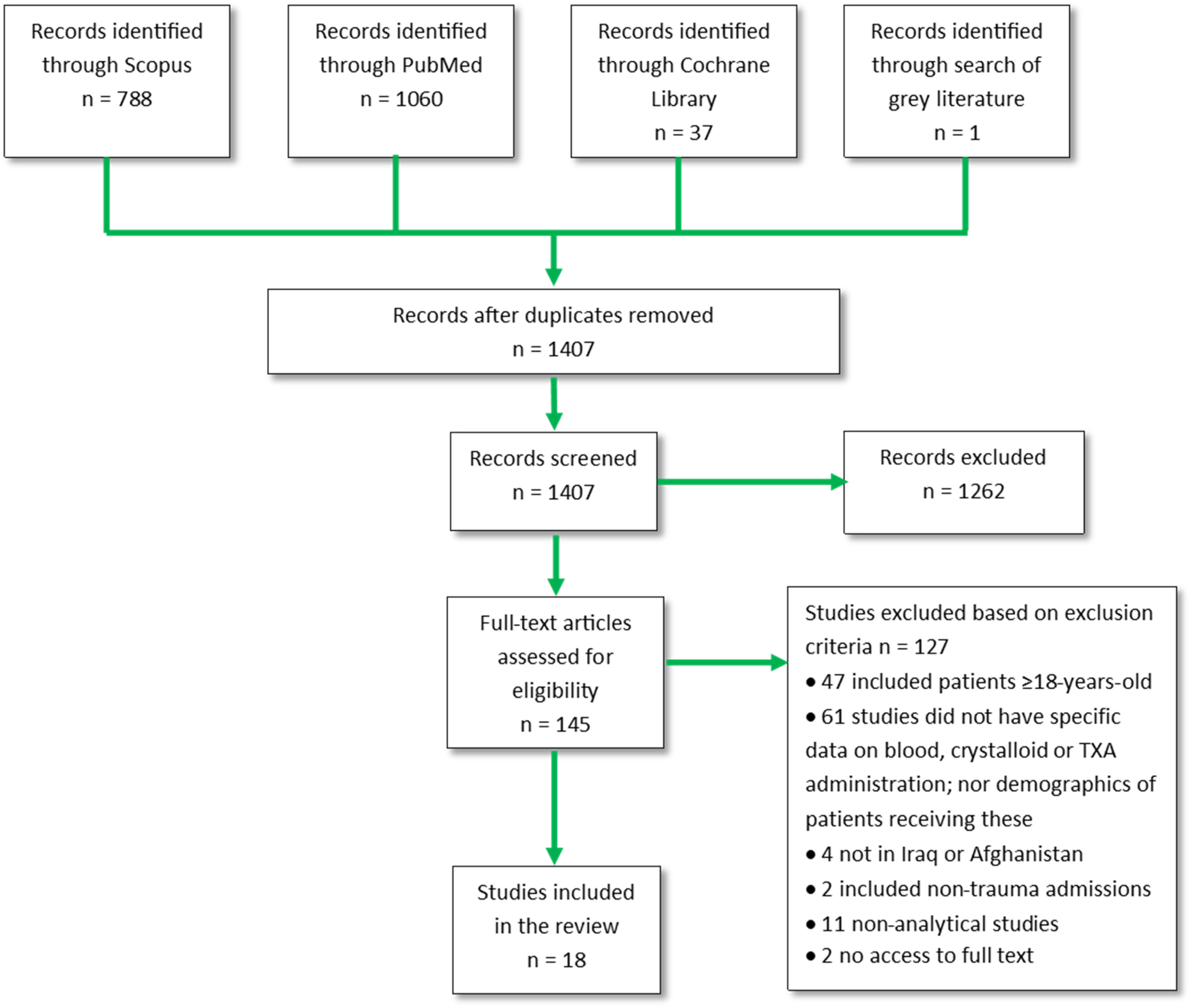
PRISMA flow chart outlining the search and screening process.
Outcomes of interest included in each study.
Eighteen papers were included, with data spanning 15 years from 2001 to 2016. All were retrospective observational studies. Fourteen studies used the DoDTR; the remaining used either a database specific to the hospital being studied or the UK Specific Joint Theatre Trauma Registry. 46 There is a significant risk of patient overlap in the selected papers and for this reason, it was not possible to use meta-analytical techniques in this review. However, the outcomes of interest studied within these papers are different from one another despite overlapping patient cohorts being used.
Discussion
Demographics of paediatric trauma patients
The largest analysis of 543 children that underwent massive transfusion in Iraq and Afghanistan by Schauer et al. 12 reported that the majority were male (73.4%), injured in Afghanistan (69.9%) by explosions (60.4%) and the median age was nine. These findings were similar in two other papers,33,43 which used the same cohort of patients with slightly different exclusion criteria. Older children may have been more frequently injured because they were given more independence and thus were at increased risk of encountering improvised explosive devices (IEDs) and unexploded ordnance (UXO). Half of blast injury in children admitted to Camp Bastion was caused by IEDs and 12% by UXO. 47
Several studies in the review identified males as the predominant casualties receiving in-hospital 34 and prehospital 38 blood products and whole blood. 16 More males were injured in the conflicts but Gale et al. 35 showed that females had a lower survival rate (OR 0.70, 95% CI 0.54–0.90) in their analysis of 3,439 children over 9 years. This is not consistent with civilian literature showing severely injured male children have increased mortality compared to females.48,49 Whilst there is no conclusive evidence to explain this finding, one suggestion is that due to cultural norms in Iraq and Afghanistan in which females should only receive medical care in the presence of a male family member, life-saving treatment of severely injured females may be delayed. 35
Some studies report that older children were more severely injured and were more likely to receive blood products. Reeves et al. 42 found that in Afghanistan the >8 years age group had the largest proportion of patients that received PRBCs (22%) as well as crystalloids (75%). Gale et al. 34 demonstrated that the use of each blood component within ITU increased with age, with all blood products most frequently used in the 10–14 age group. The 10–14 age group also had the highest median ISS of 16. Contradictory to this, Matos et al. 39 claimed that children aged ≤8 years were more severely injured (Injury Severity Score [ISS] ≥ 15 39% vs 20%, p = 0.007) and were more likely to require PRBCs in their small series of 38 patients aged ≤8 years in Iraq. Gale et al. 34 and Reeves et al. 42 studied larger patient populations (1,955 and 1,318, respectively) over several years (9 and 6 years, respectively). The study by Reeves et al. 42 did have limitations: the database used did not document patient weights thus they could not be used to calculate missing ages which limited the analysis of the study. From these studies, it cannot be determined which age group was most severely injured and required the largest volume of blood products.
DCR prehospital, in ED or in ITU
Two studies considered prehospital fluid and blood product administration. In their analysis of prehospital interventions in 3,439 children, Schauer et al. 5 described intravenous fluid administration as one of the most frequent interventions, affecting 13.3% of studied patients. They found that 0.5% of children received prehospital blood products – a similar figure was reported by Lauby et al. 38 likely reporting the same group of patients. Possible reasons for reported low levels of prehospital transfusion included inadequate availability of forward blood products, an absence of paediatric specific prehospital blood administration guidelines (if guidelines are available they are based on adult transfusion protocols) 38 and a lack of confidence among staff in their ability to administer prehospital blood products.
The frequency of blood product administration was far higher in ED than in the prehospital setting. By studying resuscitation in 3,388 children in ED, Schauer et al. 31 found that 33.8% of children received PRBCs, 24% received FFP and only 6.3% received PLT. Multiple studies highlight the unavailability of platelets in the combat setting. Cannon et al. 3 report that 93% of massive transfusion patients received FFP yet only 37.5% received PLT. Additionally, Edwards et al. 44 were unable to include platelets in their analysis of blood product ratios because only 11% of patients received PLT. A civilian paediatric trauma study conducted by Nosanov et al., 50 where blood components were likely to be more accessible, found that 54.3% of massive transfusion patients received PLT. This demonstrates that platelets are used less frequently in the combat setting; this is likely due to an inadequate supply of apheresis platelets in the military field hospitals given their short shelf life. 44
Two studies went on to consider blood products administered in ITU. Inwald et al. 37 found that of the 112 paediatric patients admitted to the Camp Bastion ITU over one year, there was a significant requirement for blood transfusion with seven patients receiving more than 10 units of blood products. Expanding on this study, Gale et al. 34 collected data on all 1,955 paediatric admissions to Role 3 ITUs and documented that 54.5% of patients received PRBCs. Rates of blood transfusion in ITU are even higher than ED: only one-third of paediatric patients received PRBCs in ED 31 compared to half of patients in ITU. 34 This is possibly due to patients in ITU being more severely injured: the median composite ISS for ITU patients was 14 compared to nine in ED.31,34 The volumes of FFP and PLT administered in ITU are relatively similar compared to the low administration rates of platelets in the ED setting. 34 This may be due to the increased availability of platelets in ITU.
Blood component administration and massive transfusion
The largest analysis of 1,244 paediatric patients over nine years in Iraq and Afghanistan by Lauby et al. 16 demonstrated that 36.2% of children received at least one blood component within 24 h of admission; other studies27,40,41 have shown similar results. This shows that blood product administration is a significant requirement in this paediatric cohort, reflecting a high injury burden, with explosive injuries predominating where there is a high likelihood of significant blood loss. 51
Neff et al. 41 studied data on 1,113 children in Iraq and Afghanistan over 12 years in an attempt to develop an evidence-based definition of paediatric massive transfusion which would be advantageous in identifying patients at risk of shock, coagulopathy and death. They defined a threshold of 40 ml/kg of all blood products administered within the first 24 h, as beyond this cut-off there was a demonstrable increase in mortality. This definition was consistent when patient groups above (MT+) and below (MT−) the Massive Transfusion (MT) threshold were compared. Relative to the MT− group, the MT + group showed a significantly higher frequency of coagulopathy (45% vs.29.6%, p < 0.001) and shock (68.1% vs. 47%, p < 0.001) as well as in-hospital mortality (14.7% vs. 6.1%, p < 0.001). Using this definition of massive transfusion, Schauer et al. 12 showed that children that received massive transfusion in Iraq and Afghanistan had lower survival to discharge (82.6% vs. 91.6%, p < 0.001) and were more severely injured with a higher median ISS (17 vs. 9). In the analysis of 907 children over 10 years, Edwards et al. 44 reported a mortality of 11% in all paediatric casualties and 19% mortality in children that received ≥40 ml/kg of blood.
Based on the largest set of data available, it can be concluded that half of the children that received blood products went on to receive massive transfusions. 12 This rate of paediatric massive transfusion is much higher than that of civilian paediatric trauma: analysis of the US National Trauma Databank 7 revealed that only 0.4% of paediatric trauma patients in the civilian population received a massive transfusion – this study uses the same definition of massive transfusion as Schauer et al. 12 Military data, therefore, offer a unique opportunity to guide massive transfusion practice in children.
The early activation of resources prior to the arrival of paediatric patients has shown survival benefit by preventing delay in access to interventions 52 however this requires a paediatric massive transfusion protocol with validated activation criteria. Neff et al. 41 facilitated the development of this by generating a validated definition of massive transfusion which will provide consistency when reporting data. However, the use of vital signs in the activation criteria is not thought to be as reliable in children as it is in adults. 29 Schauer et al. 12 showed that although children that received massive transfusion had higher rates of tachycardia (based on a heart rate greater than the 90th centile for their age), 70.9% of children that did not receive massive transfusion were also tachycardic. Furthermore, only 31.2% of massive transfusion patients demonstrated systolic hypotension.
Effect of blood product ratios on survival
Edwards et al. 44 attempted to determine whether balanced blood product ratios were associated with improved paediatric survival in Iraq and Afghanistan. In the massive transfusion group, balanced blood product ratios were not associated with better outcomes. In fact, when all transfused patients were considered, mortality was greater in patients that received an FFP:PRBC ratio >0.8 (18% vs. 8%, p < 0.0001). These findings, which oppose current DCR practice, may be explained by the limitations of the study which did not control for factors such as acidosis or coagulopathy, excluded 30% of the patient population due to an absence of recorded weights in the registry and did not include platelets in the blood ratio analysis.
Based on definitions from the Trauma Quality Improvement Program, 53 Cannon et al. 32 divided 364 children who received massive transfusion in Iraq and Afghanistan into low plasma:PRBC ratio (<1:2) and high plasma:PRBC ratio (≥1:2) groups. They found no independent association between PLAS:PRBC ratio and mortality. However, the retrospective nature of the study meant there was a high likelihood of confounding variables between study groups.
Cannon et al. 3 investigated the effect of blood product ratios on mortality in 1,377 children that received blood transfusion in Iraq and Afghanistan over 13 years. They divided patients into four groups: LO:LO (low FFP: low PLT), HI:LO (high FFP:low PLT), LO:HI (low FFP:high PLT) and HI:HI (high FFP:high PLT). Regression analysis did not show an improvement in survival in any of the HI groups compared to the LO:LO group and thus did not offer any additional evidence as to an optimum blood product ratio. All three studies3,32,44 analysing blood product ratios showed similar findings; however, there is likely overlap of datasets as all originate from a single operational database.
Paediatric studies in Iraq and Afghanistan have been unable to show that high blood product ratios have similar survival benefits to those seen in the adult population. This may be because the studies do not analyse the use of high blood product ratios in combination with limited crystalloids. Schauer et al. 43 identified this potential limitation and hypothesised that the reason for the lack of benefit in haemostatic resuscitation is due to high volume crystalloid infusion. They demonstrated that children receiving low volumes of crystalloids in combination with a high FFP:PRBC ratio showed improved survival compared to those receiving a lower ratio (OR 3.42, CI 1.04–11.24). This suggests that the DCR principles of higher blood product ratios in combination with limited volumes of crystalloids have a survival benefit in the paediatric population. The reliability of this study is limited by incomplete data held within the DoDTR. 54
Use of whole blood
Whole blood administration occurred infrequently in paediatric trauma treatment in Iraq and Afghanistan. The largest analysis of whole blood in paediatric casualties during the conflicts by Lauby et al. 16 identified that 4% of patients that underwent blood transfusion received WFWB. Other studies3,32 using the same database over a different timeframe documented similar results. After adjusting for confounders and excluding patients with a severe head injury, they found there was a significant improvement in survival of the WFWB group compared to the blood component therapy group (OR 58.63, 95% CI 2.70–1272.67). 16
This study had a small cohort of patients and was retrospective. However, the correlation found should not be dismissed. Whole blood provides an opportunity for DCR in which balanced blood components are not required; this may offer survival benefits. The practicalities of providing whole blood can also be a limitation. 55
Crystalloid administration
Cannon et al. 3 demonstrated an overall decrease in the use of crystalloids in children over the period of conflict. This is likely due to increasing evidence that excessive use of crystalloids can increase mortality through haemodilution. 20
In a study of 907 children in Iraq and Afghanistan, Edwards et al. 44 identified an association between high-volume crystalloids and poorer outcomes including time spent in ITU and in hospital after adjusting for age and ISS. They identified that mortality increased from 10% for patients that received ≤150 ml/kg of crystalloids to 18% for those that received >150 ml/kg (p = 0.011). However, as the data are retrospective it cannot be concluded that the high volumes of crystalloids independently caused increased mortality in these patients.
Two studies3,44 identified an association between very low crystalloid administration and increased mortality which contradicts current DCR strategies. This may be a result of survival bias; it is likely that these patients died before the opportunity to receive additional crystalloid fluids or blood products.
TXA administration
The largest analysis of TXA in 507 paediatric patients injured in Iraq and Afghanistan from 2006 to 2013 by Hamele et al. 36 demonstrated that 11.6% of massive transfusion patients received TXA. After logistic regression analysis, TXA was independently associated with lower mortality (OR 0.35, 95% CI 0.123–0.995, p = 0.0488). Patients that received TXA were also more likely to receive a high FFP:PRBC ratio (OR 1.26, p = 0.33). This suggests a trend towards more balanced blood product resuscitation in combination with TXA as part of DCR. These additional variables may have contributed to the improved survival in the TXA group however TXA administration was still associated with improved survival after regression analysis. They were not able to interpret the safety of TXA in children because the registry used did not include data on complications. 36
The ERC 8 recommends a loading dose of 15–20 mg/kg of TXA in children requiring a transfusion after severe trauma, however, it is not clear whether this was the dosing regimen identified by Hamele et al. 36 in their cohort. The DoDTR fails to document the timing and quantity of the first TXA dose and if/when a second dose was administered. 36 The absence of this information limits the conclusions which can be drawn from the study although it does offer promising evidence as to the benefit of TXA in paediatric trauma patients.
Key findings
DCR strategies of balanced blood transfusion, limited administration of crystalloids and the use of TXA have been increasingly used to treat paediatric trauma patients over the period of war in Iraq and Afghanistan and were associated with improved survival. However, due to the retrospective nature of nearly all the studies, the effect of these techniques on mortality in children cannot be validated.
Massive transfusions in paediatric patients occur more frequently in the combat setting than in civilian populations. The large amount of data on paediatric massive transfusion has enabled the development of a universal definition of massive transfusion in the paediatric population of 40 ml/kg total blood products within 24 h. The development of this definition is useful for clinicians in identifying children at increased risk of mortality and provides consistency in massive transfusion definitions in the literature. Most children who received massive transfusions were male, aged 9–10 years, and injured in Afghanistan by explosives. This information on demographics and interventions is crucial in informing military medical providers on what to expect on deployment and ensuring they are prepared to treat severely injured children.
It is essential that staff receive paediatric-specific training on DCR before deployment, given its relatively high frequency in the combat setting. From the evidence in this review, it is suggested that paediatric DCR training should include identification of children likely to require massive transfusion; weight calculations based on age; the use of blood products, limited crystalloids, TXA and whole blood in children if appropriate.
Differences in paediatric cohorts may limit the applicability of these data to the civilian population. It is documented that children in Afghanistan have very poor nutritional status 56 – this is reinforced by MTFs reporting that wounds in children normally expected to heal within one week were taking up to 2–3 weeks. 6 There is also a discrepancy in mechanism and type of injury: a large proportion of children suffered blast injuries in the conflicts which combine blunt and penetrating injury. 51 Unlike the civilian population in which the most prevalent mechanism of trauma in children is blunt force alone. 57 Consequently, military DCR strategies may not be directly applicable to civilian paediatric trauma patients. Nevertheless, devastating events have seen children injured by explosives in civilian terrorist attacks such as the Manchester Bombing. 58 It is possible that the lessons learnt from Iraq and Afghanistan will prove valuable even in civilian populations in addition to current conflicts such as recent events in Ukraine. 59
Limitations
All studies included within this review use data from military trauma databases which have their own limitations. Firstly, a combat medical environment can be high-pressured and understaffed hence documenting information can be difficult and multiple studies3,32,42 highlight the issue of missing values in the data. Secondly, the DoDTR, used by most studies, does not document the extent to which blood product resuscitation was guided by test results. 46 Thirdly, the DoDTR only documents patients who arrive at MTFs with signs of life or ongoing interventions – it does not provide data on patients that died prehospital and who may have benefitted from DCR. 46 Finally, the long-term effects of DCR strategies could not be measured because data were limited to outcomes within the MTF.
All studies included in the review are retrospective studies. This creates limitations in that causation cannot be established, and all conclusions are established on correlation alone. The studies are also vulnerable to survival bias in which patients that survive are also more likely to receive interventions as they have survived for longer. Additionally, analysis of paediatric data from military hospitals is vulnerable to selection bias. MTF protocol only permits the admission of children that have been injured through conflict or those with an immediate threat to life, limb or eyesight 44 so more severely injured children are more likely to be included.
As previously discussed, there is a significant overlap in patient cohorts between the studies. Data may appear to be derived from multiple sources when actually the results complement each other because many of the patients are the same.
Most studies define paediatric as <18 years; however, some studies32,37,44 used a younger group of patients in an attempt to generate cohorts with entirely paediatric physiology. This inconsistency limits the conclusions that can be drawn from the combined results of multiple studies.
Conclusion
Children continue to be injured in war to this day as demonstrated by recent events in Ukraine. Without larger prospective studies, medical providers will continue to use the evidence from military databases to inform their practice. Larger prospective trials in paediatric trauma are both ethically and logistically challenging, even more so in the combat setting, and therefore, the conclusions reached in this review are likely to be the most reliable in informing current DCR strategies for paediatric trauma. Positive associations have been identified between survival and balanced blood product ratios in combination with limited crystalloids, whole blood and TXA suggesting that the use of these principles may be beneficial in many paediatric trauma environments.
Overall, retrospective analysis of the children treated in Iraq and Afghanistan has provided insight into the optimal DCR strategies to be used in the management of children injured through conflict. Educating DCR providers on these strategies will ultimately help to save the lives of many severely injured children.
Declarations
Supplemental Material
sj-docx-1-tra-10.1177_14604086231152661 - Supplemental material for A narrative review of damage control resuscitation for paediatric trauma patients in Iraq and Afghanistan from 2001 to 2016
Supplemental material, sj-docx-1-tra-10.1177_14604086231152661 for A narrative review of damage control resuscitation for paediatric trauma patients in Iraq and Afghanistan from 2001 to 2016 by Annie Mae Wright, Lisa Ramage, Jon Barratt, Gareth Grier and Amy Hughes in Trauma
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Trial registration
Not applicable.
Contributorship
AMW conceived the study, researched the literature and wrote the first draft of the manuscript. LS reviewed, edited and approved the manuscript for submission. JB provided conceptual guidance and reviewed the manuscript for submission. GG identified the area of research and reviewed the manuscript for submission. AH helped to conceive the study and provided guidance in the literature review.
Acknowledgements
The authors would like to thank Professor Danë Goodsman for her support while writing this review and throughout my time on the Prehospital Medicine iBSc.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.