
Abstract
Background and objective:
Split-thickness skin grafting is a common procedure for the treatment of complicated wounds. Predictors of skin graft failure are not fully understood. The study aimed to identify baseline predictors of skin graft failure and delayed healing.
Methods:
Consecutive adult patients with wounds treated using split-thickness skin grafting between 2009 and 2019 were included in a retrospective single-center study. Failures referred to total graft loss or the need of a new operation.
Results:
In total, 1484 wounds in 1011 patients were analyzed. Graft failure occurred in 384 (25.9%) cases and reoperation was required in 297 (20.0%) cases. At 1 year, the wound was healed in 91.5% of the cases. Logistic regression analysis showed that peripheral arterial disease, diabetes, use of immunosuppressive medication, and wounds located in the foot significantly increased the risk of graft failure, while wounds located in the chest and those secondary to trauma, burn, or cancer excision had significantly lower graft failure risk. Cox proportional hazards analysis showed that wounds of the hand, forearm, and thigh as well as those secondary to trauma and burns were associated with higher rates of wound healing at 1 year. Wounds in feet, wound duration, lower limb edema, peripheral arterial disease, use of antipsychotic medication as well as wounds secondary to surgical complications, venous insufficiency, diabetes, and other comorbidities were associated with lower wound healing at 1 year.
Conclusions:
The present study identified several risk factors associated with poor outcome after skin grafting. These findings highlight the importance of recognizing patient comorbidities and wound etiology in preoperative planning.
Context and Relevance
Split-thickness skin grafting is a widely used method for treating complex wounds, yet predictors of graft failure remain poorly understood. Prior studies have focused on lower limb wounds with limited sample sizes. This large retrospective study analyzed 1484 wounds across all anatomical sites and identified key baseline risk factors for graft failure and delayed healing. Peripheral arterial disease, diabetes, immunosuppressive medication, and wounds in the foot increased failure risk, while trauma-, burn-, and cancer-related wounds have better outcomes. These findings support individualized preoperative risk assessment and highlight the importance of managing comorbidities to improve graft success. The study provides novel insights that may guide clinical decision-making and reduce the need for reoperations.
Introduction
Acute and chronic wounds are common conditions, and their treatment is a major clinical challenge associated with significant financial burden.1,2 Notably, patients with chronic wounds often suffer from physical, mental, and social disadvantages. 2 Autologous split-thickness skin grafting is one treatment method used to cover large skin defects. 3 This approach has been shown to improve the quality of life and self-esteem in patients with venous leg ulcers. 4 However, skin grafts can fail, potentially leading to multiple skin grafting procedures or chronic soft tissue defects.
Some postoperative conditions have been proposed to deteriorate skin graft take.3,5–7 Preoperative factors, however, also play a significant role. A few studies have investigated the impact of baseline risk factors on split-thickness skin graft healing, primarily in the lower limb.8–11 These studies are limited by small sample sizes, and data on the impact of patient comorbidities on skin graft healing remain scarce.
The present study aimed to investigate split-thickness skin graft failure rates, reoperation rates, and time to wound healing after skin grafting across various anatomical sites in a large patient population. In addition, we sought to identify independent baseline predictors of skin graft failure.
Methods
Study design
This is a retrospective study including all consecutive adult patients who underwent split-thickness skin grafting at any anatomical site at a secondary referral hospital (Department of Plastic Surgery, Hospital Nova, Wellbeing Services County of Central Finland, Jyväskylä, Finland) between March 2009 and November 2019. A few patients underwent skin grafting at multiple anatomical sites and the outcome of each wound was addressed individually. Major burns were not treated at the study hospital and thus not included.
The study was conducted in accordance with the principles of the Declaration of Helsinki 12 and the protocol was approved by the Hospital Nova Review Board on 11 March 2020. The need for ethical approval was waived due to the retrospective design of the study. The need for informed consent from individual participants was also waived as the study was based on retrospective registry data.
The primary outcome of this study was skin graft failure, which refers to total loss of the graft or the need for a new surgical procedure on the same wound. Hence, a partial graft loss was not considered a clinically relevant failure unless it necessitated reoperation. Secondary outcomes included the number and type of reoperations, the duration of wound healing, and graft success at 1 year. If the graft failed and no new skin grafting was performed, the outcome was considered unsuccessful, regardless of other possible methods used for wound closure. Skin grafting was considered successful if a failed graft was replaced and the new graft healed, or if the initial skin grafting partially took and the remaining wound healed through conservative management.
Operative techniques and postoperative care
Skin graft procedures were performed by plastic surgeons or surgical residents. Prior to grafting, wounds were carefully prepared through sharp debridement and removal of non-viable tissue. Burns were excised and grafted in a single stage. Split-thickness skin grafts were harvested using either an air or electric dermatome. In most cases, the grafts were meshed, and the grafts were secured with sutures or staples. Fibrin sealants were not used.
A layer of Vaseline gauze (Unilever US, Englewood Cliffs, NJ, USA) was applied over the graft, followed by either moist and dry swab gauzes or a negative-pressure wound therapy dressing. Patients were either admitted to the hospital or discharged shortly after the procedure. Several patients were transferred to a primary health care facility for rehabilitation following treatment.
Mobilization restrictions were applied at the discretion of the operating surgeon. Postoperative antibiotic therapy was administered on a case-by-case basis. Conventional dressings were typically removed 2–3 days after surgery, while negative-pressure wound therapy dressings were removed after 4–7 days. Sutures or staples were removed 5–7 days postoperatively. Follow-up practices varied between patients depending on the duration of hospital stay, the patient’s municipality of residence, and any issues with graft healing.
Data collection
Pre-, peri-, and postoperative variables were collected retrospectively from electronic medical records by five investigators. Data were available from both in-hospital treatment and outpatient clinics. In addition, for most patients, wound-related information was accessible from primary health care and home care records.
The following variables were collected: age, sex, height, weight, smoking, comorbidities, frailty (assessed using the Geriatric Status Scale), 13 drug treatment as well as the levels of hemoglobin, creatinine, albumin, fasting blood glucose, glycated hemoglobin, and prothrombin time international normalized ratio. Wound-related variables included wound dimensions, location, etiology, duration, prior surgical revisions, use of preoperative negative-pressure wound therapy, results of preoperative bacterial cultures, and presence of preoperative clinically evident infection.
Intraoperative variables included prophylactic antibiotic therapy; bacterial culture results; operating surgeon; wound bed characteristics, for example, tissue types, use of dermal substitutes, or flaps; graft thickness; donor site; and meshing. Postoperative variables included the day of dressing or negative-pressure wound therapy device removal, day of suture or staple removal, duration of immobilization, postoperative antibiotic therapy, clinically evident infection, graft failure, date of graft failure diagnosis, suspected cause of graft failure, and the number, type, and timing of reoperations.
The date of the last follow-up visit, whether at the hospital, a primary health care center, or via home care, was also recorded. A wound was considered healed when no further health care visits were required, even if small non-epithelialized areas remained.
Statistical analysis
Continuous variables are reported as means with standard deviations, and categorical variables as counts with percentages. The Mann–Whitney’s test, the chi-square test, and the Fisher’s exact test were used for univariate analysis. Time to wound healing was estimated using the Kaplan–Meier method.
Independent predictors of skin graft failure were identified using logistic regression with a stepwise backward method including only variables with p < 0.05 in univariate analysis into the regression model. The discrimination and calibration of the final regression model was tested using the Hosmer–Lemeshow test and estimating the area under the receiver operating characteristic curve (AUC).
Cox proportional hazards analysis with the stepwise backward method was performed to identify predictors of wound healing at 1 year, including only variables with p < 0.05 in univariate analysis in the regression model. Risk estimates are reported as odds ratios (OR), hazard ratios (HR) and their 95% confidence intervals (CI). All statistical tests were two-sided, and p < 0.05 was set for statistical significance. Statistical analyses were performed using SPSS software, version 29.0 (IBM Corporation, New York, USA).
Results
Overall, 1506 wounds were included in this registry. Twenty-two wounds were excluded due to data collection inconsistencies. The final study population thus included 1484 wounds in 1011 patients. Baseline patient characteristics and wound-related variables are summarized in Table 1.
Baseline characteristics and wound-related data.
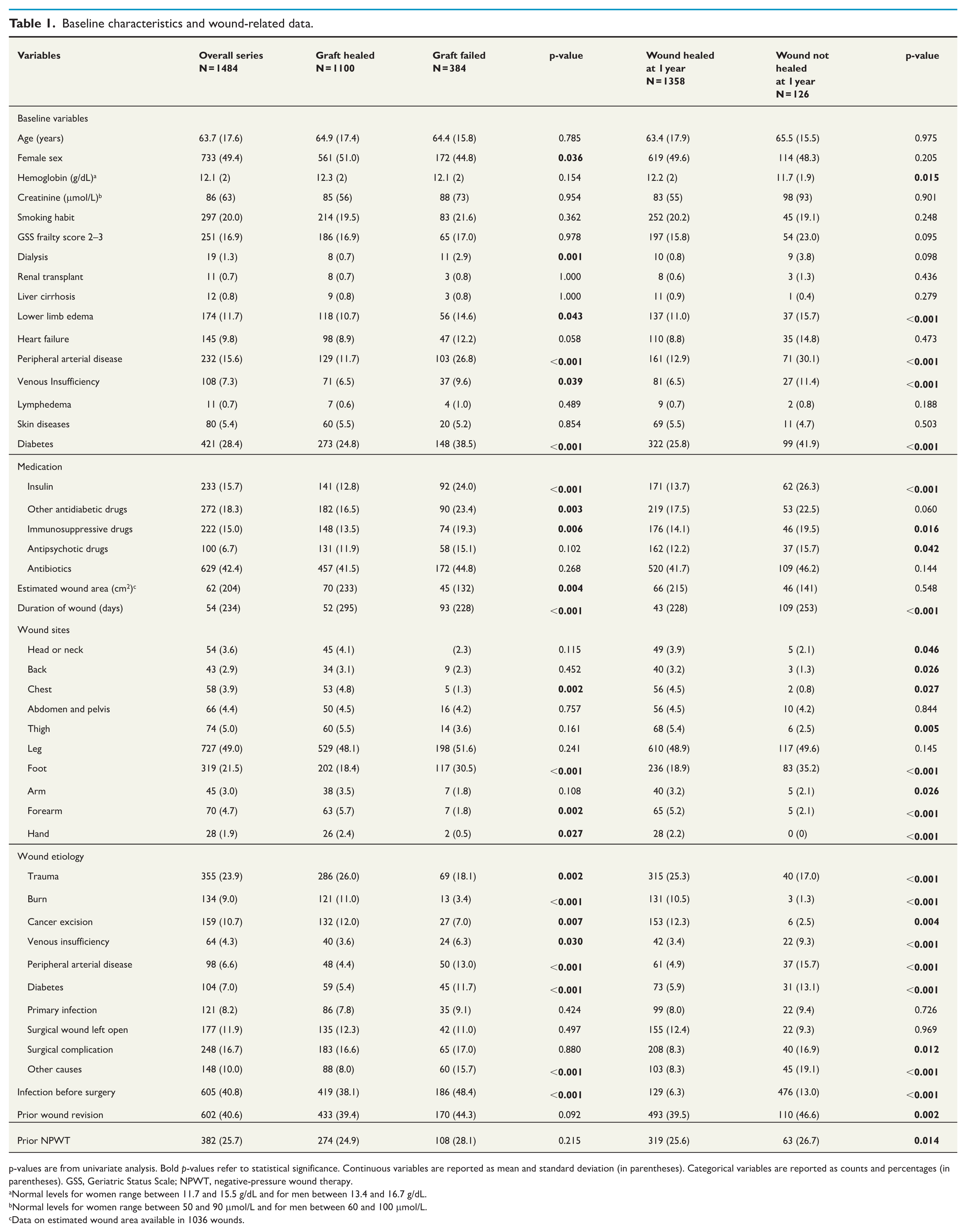
p-values are from univariate analysis. Bold p-values refer to statistical significance. Continuous variables are reported as mean and standard deviation (in parentheses). Categorical variables are reported as counts and percentages (in parentheses). GSS, Geriatric Status Scale; NPWT, negative-pressure wound therapy.
Normal levels for women range between 11.7 and 15.5 g/dL and for men between 13.4 and 16.7 g/dL.
Normal levels for women range between 50 and 90 μmol/L and for men between 60 and 100 μmol/L.
Data on estimated wound area available in 1036 wounds.
Graft failure occurred in 384 (25.9%) wounds, and reoperation for graft failure was required in 297 (20.0%) wounds. The mean number of reoperations per wound was 0.3 ± 0.8. Among wounds requiring reoperation, the mean number of reoperations was 1.6 ± 1.2. A total of 483 reoperations were performed, including 268 skin grafts (55.5%), 129 revisions (26.7%), 50 amputations (10.4%), 21 flaps (4.3%), and 15 other procedures (3.1%). At 1 year, 91.5% of wounds were healed (Fig. 1). In patients who required one or more additional skin grafts, the likelihood of successful graft healing by the end of follow-up declined markedly after the third re-grafting procedure (Fig. 2).
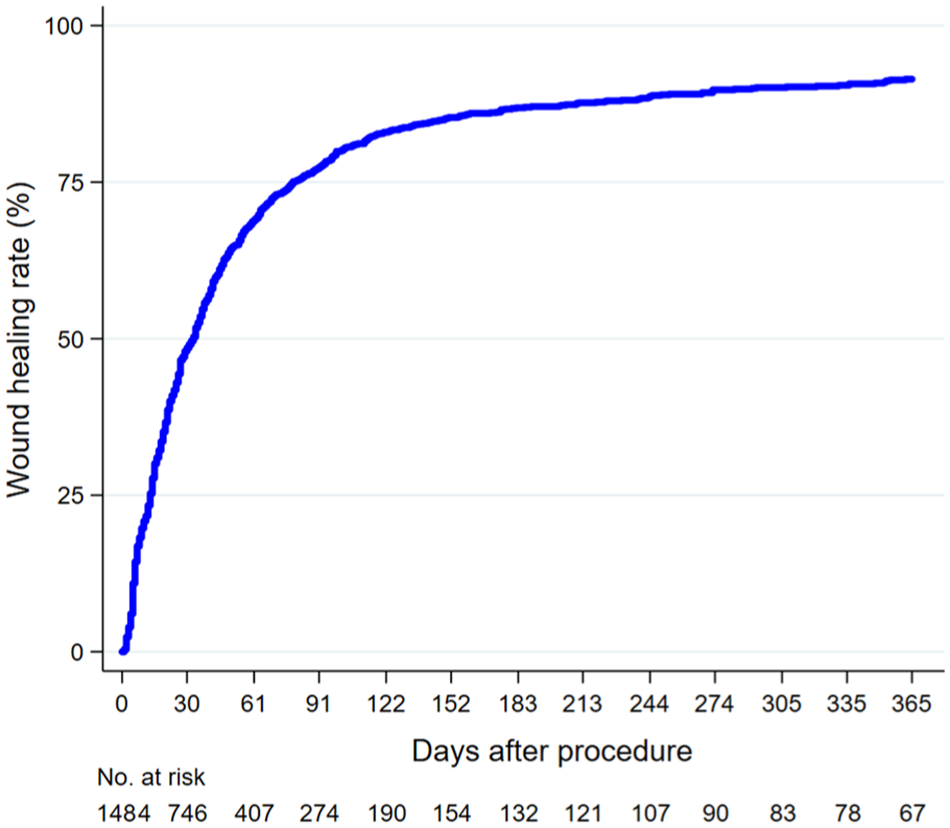
Kaplan–Meier estimates of wound healing after split-thickness skin grafting.
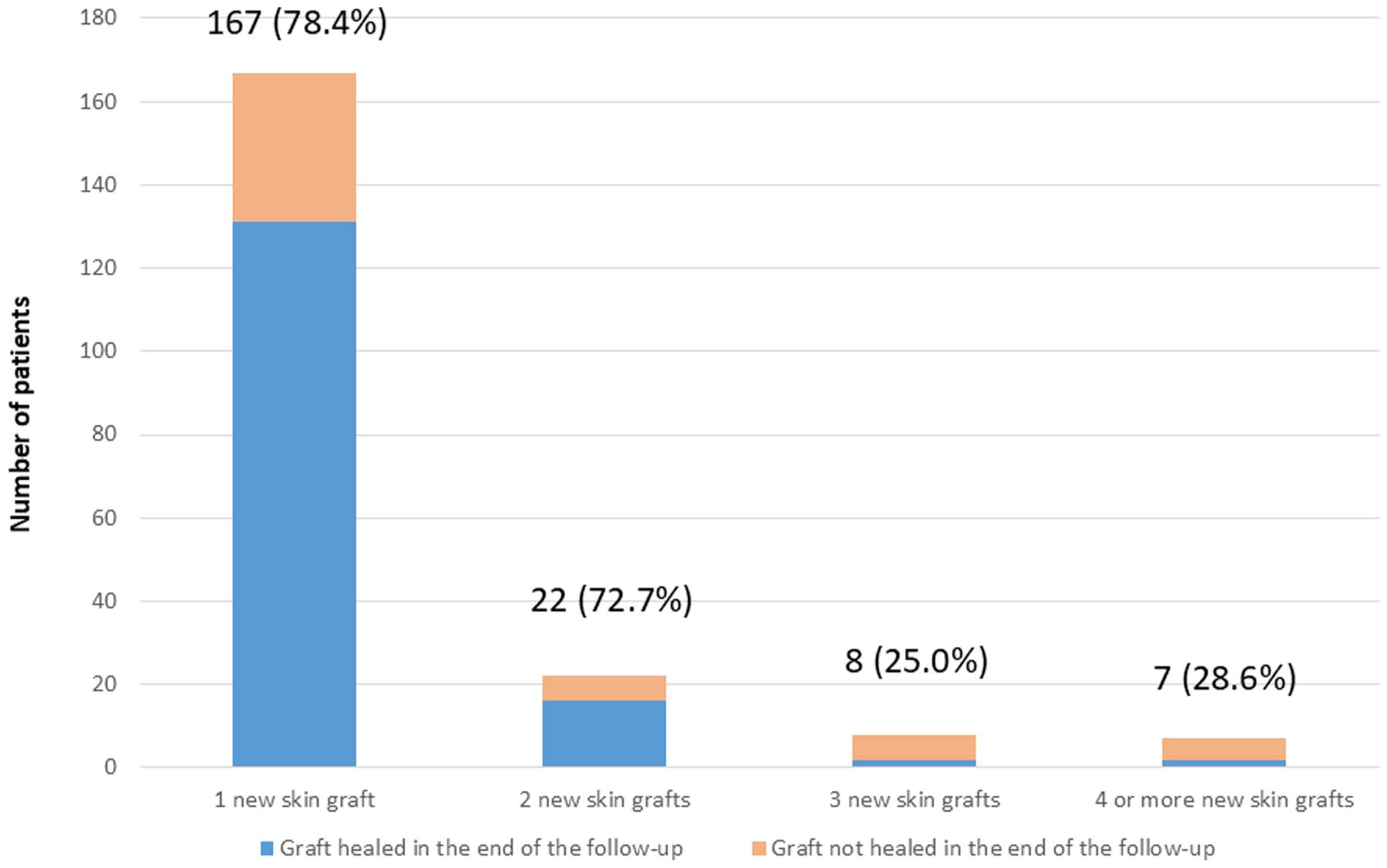
Number of patients requiring one or more new skin grafts after split-thickness skin grafting. Percentages of the grafts healed at the end of the follow-up are presented in parentheses.
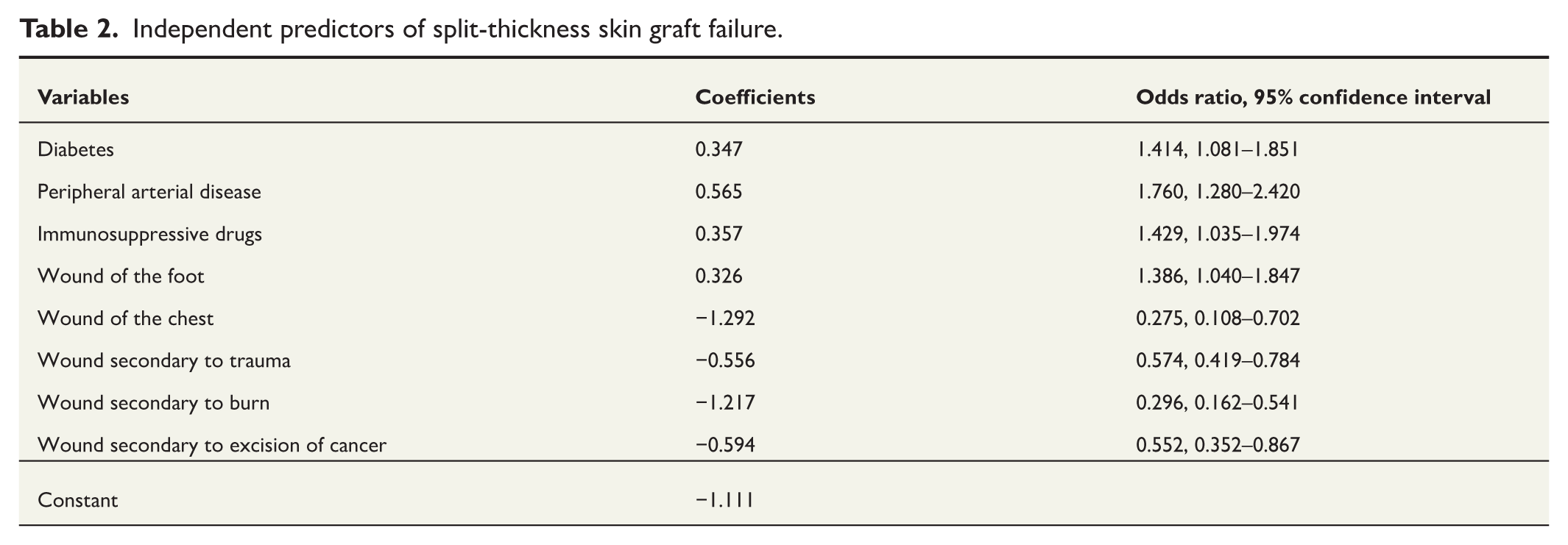
Logistic regression showed that peripheral arterial disease, diabetes, immunosuppressive medication, and wounds located in the foot increased the risk of skin graft failure. In contrast, wounds located on the chest and those secondary to trauma, burn, or cancer excision were associated with a significantly lower risk of graft failure (Hosmer–Lemeshow test, p = 0.795; AUC = 0.678, 95% CI = 0.647–0.709) (Table 2).
Independent predictors of split-thickness skin graft failure.
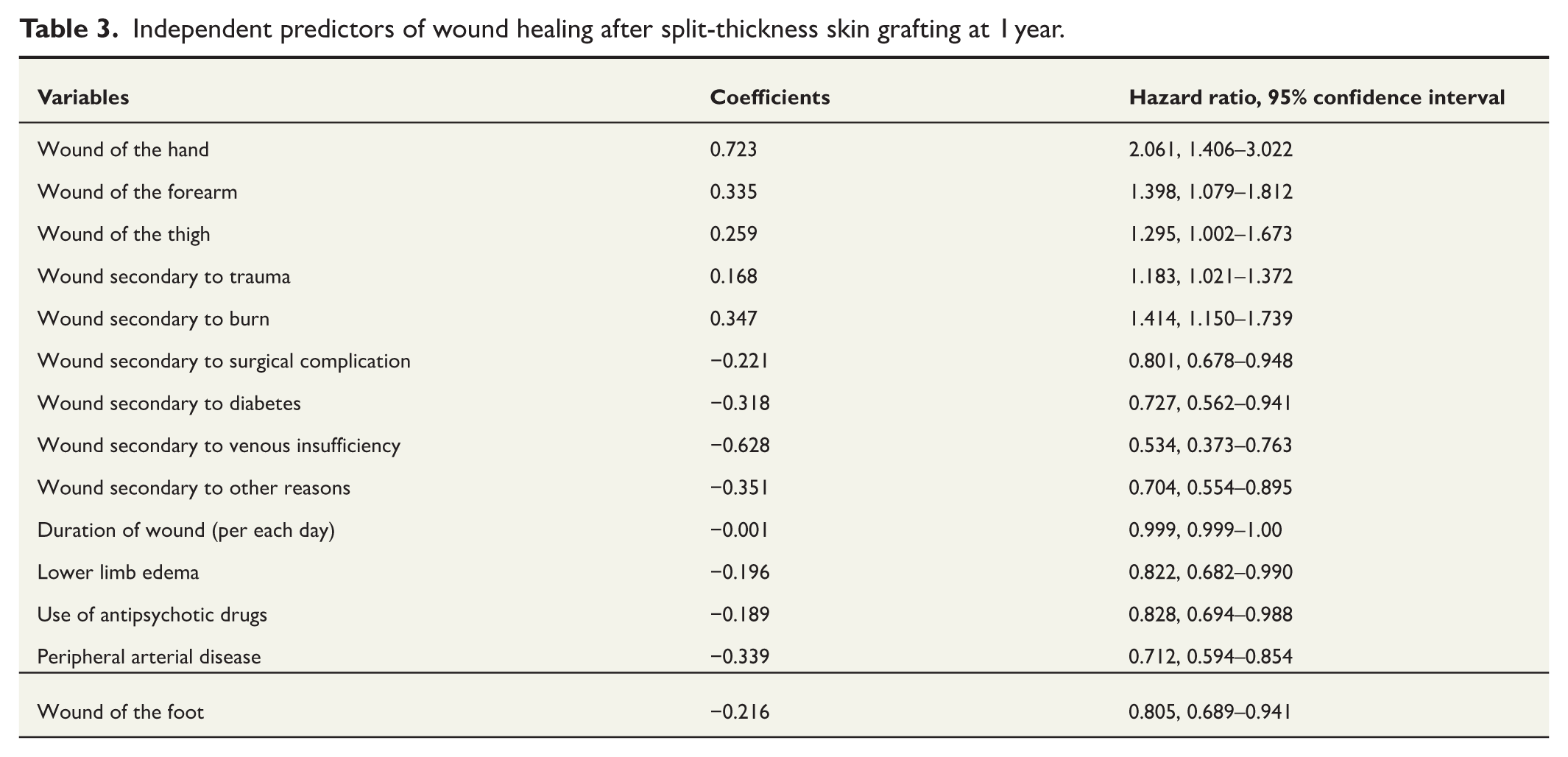
Cox proportional hazards analysis showed that wounds located on the hand, forearm, and thigh, as well as wounds secondary to trauma or burn were associated with higher wound healing rates at 1 year. In contrast, prolonged wound duration, wounds in feet, lower limb edema, peripheral arterial disease, antipsychotic medication as well as wounds secondary to surgical complications, venous insufficiency, diabetes, or other causes were associated with lower wound healing rates at 1 year (Table 3).
Independent predictors of wound healing after split-thickness skin grafting at 1 year.
Discussion
In the present study, skin graft failure occurred in 25.9% of the wounds. Noteworthy, the definition of graft failure varies across previous studies. To the best of our knowledge, no prior study has addressed skin graft outcomes across all anatomical sites, while most have focused specifically on lower limb wounds. In a series of 70 skin grafts applied to lower limb wounds, 91% of which were split-thickness grafts, 33% failed by 6 weeks postoperatively. 9 Similarly, in a series of 94 split-thickness skin grafts for chronic lower limb wounds, 30.9% of the grafts did not experience complete healing and incorporation. 10 Among patients with peripheral arterial disease and wounds on the ankle or foot, 52.5% of wounds remained unhealed 90 days after split-thickness skin grafting. 8 Similar increased skin graft failure rates have been reported in other series focusing on lower limb wounds.11,14 Considering the differences in patient populations, our findings are in line with those of prior studies. In the present cohort, 75.5% of wounds were located on the lower limb, which may explain the slightly lower percentage of graft failures.
One-fifth of patients in the present study underwent reoperation following skin graft failure. On average, patients requiring reoperation underwent more than one reoperation. This reoperation rate is somewhat higher than the 12.2% pooled rate reported in a meta-analysis of 303 patients who received split-thickness skin grafts. 6 Similarly, in a meta-analysis involving 759 skin grafts for foot and leg ulcers in diabetic patients, 12.1% of the patients required a new skin graft. 15 In contrast, in a study by Reddy et al., 9 none of the patients underwent a reoperation, but the grafted wounds were of small size and healed by secondary intention. In another series of 94 patients with lower limb skin grafts, 18 (19.1%) patients required revision, of whom five (5.3%) subsequently required major limb amputation. 10 Indeed, these variations underscore the major challenges in comparing outcomes across studies due to differences in patient populations, wound characteristics, and definitions of key endpoints. Nonetheless, based on our institutional registry, the risk of reoperation is high after skin grafting. Interestingly, 59.8% of reoperations in the present study involved new reconstructive procedures, and 10.4% resulted in amputations.
Diabetes, peripheral arterial disease, immunosuppressive medication, and wounds located on the foot were identified as independent risk factors for split-thickness skin graft failure in this study. These factors are known to impair wound healing by various mechanisms affecting different phases of wound healing.16–19 Only a limited number of studies have, however, investigated risk factors for split-thickness skin graft failure.9–11 In a series of 70 lower limb skin grafts, peripheral vascular disease, immunosuppressive medication, and increased body mass index were associated with graft failure. 9 These findings were based solely on univariate analysis. In addition, the study population including predominantly very small wounds caused by cancer excision is not comparable with the present study. In contrast to our results, also Rose et al. 10 failed to find any association between diabetes and split-thickness skin graft healing in a cohort of 94 chronic lower limb wounds. In their multivariable analysis, only wound size greater than 80 cm2 was identified as an independent predictor of graft failure, 10 but several relevant comorbidities were not included in the model. 10 In our analyses, which accounted for multiple preoperative variables and baseline comorbidities, the estimated wound area was not significantly associated with graft failure rate. This suggests that patient-related factors may play a more prominent role in graft outcome than wound size alone.
In addition to diabetes, peripheral arterial disease, and wound location on the foot, we found that prolonged wound duration, lower limb edema, antipsychotic medication, and wounds resulting from surgical complications, venous insufficiency, or other causes, including pressure ulcers, were associated with lower wound healing rates at 1 year. Several of these variables were chronic conditions known to impact wound healing.17–21 We observed the detrimental effect of antipsychotic medication on wound healing, and this could reflect poorer compliance to postoperative care as well as higher smoking rate in this patient group.22,23
In the present study, wounds located on the chest and those resulting from trauma, burns, or cancer excision were associated with a significantly lower risk of skin graft failure. We hypothesize that traumatic wounds and burns may occur in younger, healthier individuals, and this may contribute to improved graft outcomes. It should be noted that no major burns were included in this study. Previous research has demonstrated that major burns are associated with a higher risk of wound infection and systemic immune dysfunction compared with minor burns,24,25 which may explain the relatively favorable outcomes for burns observed in our cohort. Wounds resulting from skin cancer excision are typically rather small and grafted immediately after excision, potentially reducing infection risk compared with chronic wounds. This may account for the lower incidence of graft failure in this subgroup. In addition, wounds located outside the foot and those caused by trauma or burns were also associated with higher wound healing rates at 1 year, which is in line with our previous findings.
Healing of split-thickness skin grafts can be prolonged. In the study by Rose et al. 10 that included 94 split-thickness skin grafts applied to lower limb wounds, the mean follow-up duration was 12.06 ± 12.9 months (median 6.5 months), and the mean time to successful graft healing was 7.7 ± 5.4 weeks (median 5.0 weeks). By the end of the study, including reoperations, grafts had successfully healed in 70 (74.5%) patients, while 19 (20.2%) patients experienced graft failure. Five (5.3%) patients ultimately required major limb amputation. 10 In another study of patients with peripheral arterial disease and split-thickness skin grafts of the foot or ankle, after excluding nine wounds lost to follow-up, 18 of 38 (47.37%) wounds had healed and 20 (52.63%) remained open at 90-day follow-up. 8 Finally, 36 of 47 (76.60%) wounds healed and six major amputations in six patients were required at a mean 502 ± 342 days of follow-up. 8 In our study, which included also wounds located in other anatomical sites, healing times were somewhat shorter than previously reported. We observed that approximately half of the wounds healed within 1 month, and 91.5% had healed at 1 year.
In this series, the skin graft failure and reoperation rates were somewhat high. Meticulous surgical debridement, antimicrobial dressings, negative-pressure wound therapy, appropriate antibiotics, and vascular interventions are key issues to achieve success after split-thickness skin grafting. These interventions were routinely performed at our unit according to the etiology and local wound conditions. The present results are affected by the relatively high prevalence of diabetes, peripheral arterial disease, and use of immunosuppressive medication, which are recognized as risk factors for wound development and impaired healing. These findings should also be viewed considering the heterogeneity of causes underlying the development of wounds, their site, and significant prevalence of comorbidities and other unmeasured confounders. The number of variables considered in this analysis per se can introduce bias related to overfitting of regression models.
There are some additional limitations that need to be considered. This is a retrospective study and thus subject to data incompleteness. The follow-up data were limited for a subset of patients, with data being unavailable from primary health care institutions in a few municipalities due to variations in institutional data systems. Importantly, data regarding skin graft failures and reoperations are reliable as all major complications were managed at our unit. Moreover, although multiple peri- and postoperative variables were collected, their association with graft healing was not analyzed. It is methodologically challenging to isolate the independent effects of such factors, such as postoperative wound infection, on postoperative complications. Instead, we decided to assess the effect of baseline variables as they are potentially manageable and important in preoperative risk assessment and clinical decision-making. Finally, unmeasured confounding factors may have influenced the outcomes but were not accounted for in the analyses.
The validity of the present findings is strengthened by the large sample size, comprehensive evaluation of baseline variables, and use of multivariate analyses. In addition, based on the available literature, this is the first study to address skin graft outcomes across all anatomical sites. The results are from consecutive patients treated at a secondary referral hospital and this may make the findings generalizable to hospitals providing community-based health care. The need for optimal surgical and medical treatment and wound dressings to achieve a well-vascularized wound environment with minimal exudate, free of non-viable tissue or infection before split-thickness skin grafting should, however, be emphasized in wound care at all health care settings.
Footnotes
Acknowledgements
None.
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support forthe research, authorship, and/or publication of this article: Open Access funding was provided by University of Helsinki. Eve Kinnunen received departmental funding from Helsinki University Hospital for the preparation of this article.
Clinical trial registration
N/A.