
Abstract
Introduction:
New transoral and minimally invasive techniques for the treatment of gastroesophageal reflux disease (GERD) have emerged, warranting evaluation of their clinical efficacy and safety.
Methods:
A literature review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines. Based on the available amount of information about clinical efficacy, the review was restricted to Stretta, Esophyx/TIF, MUSE (Medigus ultrasonic surgical endostapler), LINX, and RefluxStop procedures.
Results:
In total, 86 original studies evaluating the efficacy and safety of second-generation antireflux techniques were identified. The study populations are well described in which GERD is objectively verified. For Stretta, data were available from four double-blind, sham-controlled, randomized studies (RCT) albeit with a short follow-up time. Cohort-based data on 24-h pH monitoring, proton pump inhibitor (PPI) consumption, and QoL demonstrated a clinically significant long-term effect. For the Esophyx technique, two double-blind, sham-controlled randomized studies with 12 months of follow-up are available, which together with prospective cohort studies with longer follow-up demonstrate a sustained effect. The corresponding long-term effects of MUSE transoral technique need to be defined. The scientific documentation behind the LINX technique is incomplete, but data show the same level of efficacy in terms of objective assessments as for Esophyx. The scientific evidence for RefluxStop is still meager but promising.
Conclusions:
Both Esophyx and LINX seem to provide long-lasting symptom control with normalization of QoL in patients with chronic GERD. This seems to be true for patients with small hiatal hernia who responded well to treatment with PPI. MUSE and RefluxStop™ need better documentation to define their future role in clinical practice.
Keywords
Context and relevance
The use of novel transoral or minimally invasive antireflux technologies to manage chronic gastroesophageal reflux disease (GERD) has disseminated rapidly worldwide, despite incomplete scientific evaluation.
Introduction
Gastroesophageal reflux disease (GERD) is one of the most common gastrointestinal (GI) disorders worldwide. 1 The underlying mechanism of GERD can be viewed as a spectrum from a single anatomic aberration (e.g. incompetent lower esophageal sphincter (LES)) to a combination of multiple anatomic-functional changes, such as hiatal hernia, inadequate esophageal clearance, impaired function of the gastroesophageal flap valve, and decreased resistance of the esophageal mucosa to the noxious impact of the refluxate.2–4 The degree and extent of these alterations seem to correlate with the severity and complications of GERD. 5
Proton pump inhibitors (PPIs) are the first line of treatment for GERD, to which most patients respond well. 6 However, it is important to keep in mind that 20%–25% of patients with GERD do not respond satisfactorily to standard PPI therapy7,8 and therefore look for a more effective and sustainable treatment alternative. In addition, there is a growing concern about long-term serious side effects of PPI treatment. 6 There is also a widespread opinion that effective treatment of GERD requires the control of other components of the refluxate than simply inhibiting acid, not the least to prevent the onset and development of Barrett’s esophagus and the ensuing risk of esophageal adenocarcinoma.9–11 Finally, critical arguments have been raised against the traditional laparoscopic antireflux surgery (LARS), 12 which has since long been proved its clinical efficacy and been scientifically robustly evaluated. For instance, it has been claimed that LARS offers the patients with chronic GERD an overly invasive and risky long-term therapeutic option which burdens the patients with an unacceptable risk of mechanical-functional side effects. Parallel to these concerns, there has been a rapid technological development and marketing of innovative transoral endoscopic and other minimally invasive reconstructive techniques.
The objective of the current review is to assess the level and quality of evidence regarding the clinical efficacy of transoral endoscopic, minimal invasive antireflux procedures.
First generation of transoral endoscopic and minimally invasive techniques for GERD treatment
These “first-generation” techniques, introduced several decades ago, aimed to achieve a reflux-protecting valvular function (pressure barrier) at the gastroesophageal junction (GEJ) and involved either deposition of foreign material submucosally, alternatively to perform so-called suture plications, or to use radiofrequency ablation locally in multiple spots in the GEJ area (Stretta)13–15 (Fig. 1). The Stretta technique seems to create controlled scarring which elicits its effects not only through a pressure gradient between the stomach and the intrathoracic esophagus but also on the tone and relaxation ability of the LES. In addition, an effect on the sensitivity of the esophageal mucosa to harmful agents such as acid has been suggested. 16

As a consequence of negative results from controlled, randomized, not infrequently sham-controlled studies, 16 most of these techniques fell into disrepute.
Continued development of novel antireflux techniques
The ambition behind the “second generation” of techniques has been to mimic the results achieved with a traditional LARS, i.e. to restore the physiological function (and partly also the anatomy) of the GEJ. These devices have not only attracted upper GI surgeons but also specialized gastroenterologists-endoscopists. Likewise, many of these new techniques can be carried out as day care surgery and has relatively quickly been approved by the US Food and Drug Administration (FDA) for clinical use.
Esophyx (transoral incisionless fundoplication (TIF)) is performed by introducing a specially-designed disposable upper esophageal tube through which the gastroscope is introduced into the esophagus and stomach. Since its inception in 2006, minor changes in instrument design and procedure technique have emerged, and currently, the 2.0 version is marketed. A suction function of the endoscope is applied to the distal esophagus, allowing it to be transferred in an aboral direction and thereby repairing or stretching out smaller hiatus herniations. Then, a screw retractor is attached to the musculo-mucosal fold (flap) and via the retroflexed distal part of the instrument, transmural, fixing tacks (polypropylene) are applied, which reconstruct the flap valve function17–22 (Fig. 2A).

(A–D). A schematic illustration of “the second generation” of transoral endoscopic and minimal invasive antireflux procedures. (A) illustrates the various steps in carrying out an Esophyx 2.0 procedure, (B) illustrates the details of performing a MUSE procedure. (C) and (D) illustrate the LINX and RefluxStop interventions, respectively. Modified after previous works.21,25,40,42
The MUSE (Medigus ultrasonic surgical endostapler) technology uses a similar single-use endoscopic solution, but staples are applied transmurally between the downward and retroflected parts of the endoscope. In order not to include the diaphragmatic crus, or adjacent parts of the diaphragm, the position is checked using an ultrasound probe that is connected to the most distal part of the endoscope23–25 (Fig. 2B).
In the LINX technique (Ethicon, Johnson&Johnson), a magnetic ring is applied around the distal part of the esophagus with the traditional laparoscopic technique (also feasible with the single-port technique). This magnetic ring then expands (opens up) as soon as a bolus approaches the GEJ and then closes after the passage of the bolus26–39 (Fig. 2C).
RefluxStop (Implantica, Switzerland) is a recently launched implantable single-use sterile device alleged to ensure maintenance of the GEJ in an intra-abdominal position, allowing normal function of the LES, thereby reducing or eliminating gastric reflux. The device is inserted by use of conventional laparoscopic techniques and consists of an assembly of five sterile components that engage to form a rounded silicone cuboid, with a resorbable suture holding the pieces together. The RefluxStop device is alleged to act as a mechanical stop, preventing the LES from translocating into the thorax and is intended to counteract acid reflux without affecting food transport.40,41 The device is placed above the LES by using an implantation applicator inserted through the abdominal wall (Fig. 2D).
Methods
Search strategy
A literature review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines. 43 The literature search included PubMed, Scopus, and EMBASE electronic databases (from inception to 1 July 2024) to identify studies investigating outcomes after endoscopic, minimal invasive procedures as outlined above. Electronic searches were supplemented by manual searches of reference lists in included studies and review articles. The search was restricted to the English language. Specific search equations were formulated for each database using the following Medical Subject Headings (MeSH) terms: radiofrequency ablation, stretta procedure, PPI use, endoscopic plication, endoscopic fundoplication, endoscopic gastroplication, endoscopic full-thickness fundoplication, Esophyx, transoral incisionless fundoplication, ultrasonic surgical endostapler, endoscopic anterior fundoplication, LINX device, magnetic sphincter augmentation, LARS, laparoscopy, RefluxStop, GERD, efficacy, quality of life, and safety.
Data extraction
One author (L.L.) reviewed the literature and extracted data from eligible studies onto a standardized sheet (Fig. 3). The following data were extracted: author, year of publication, study centers, study design, sample size, and patient demographics (age, sex, disease duration, previous treatment, wash out period of any PPI treatment before enrolment), Procedure characteristics (procedure time), adverse events, length of hospital stay, follow-up time, efficacy (including PPI use) at the specified follow-up points, and postoperative quality-of-life scores were also registered.
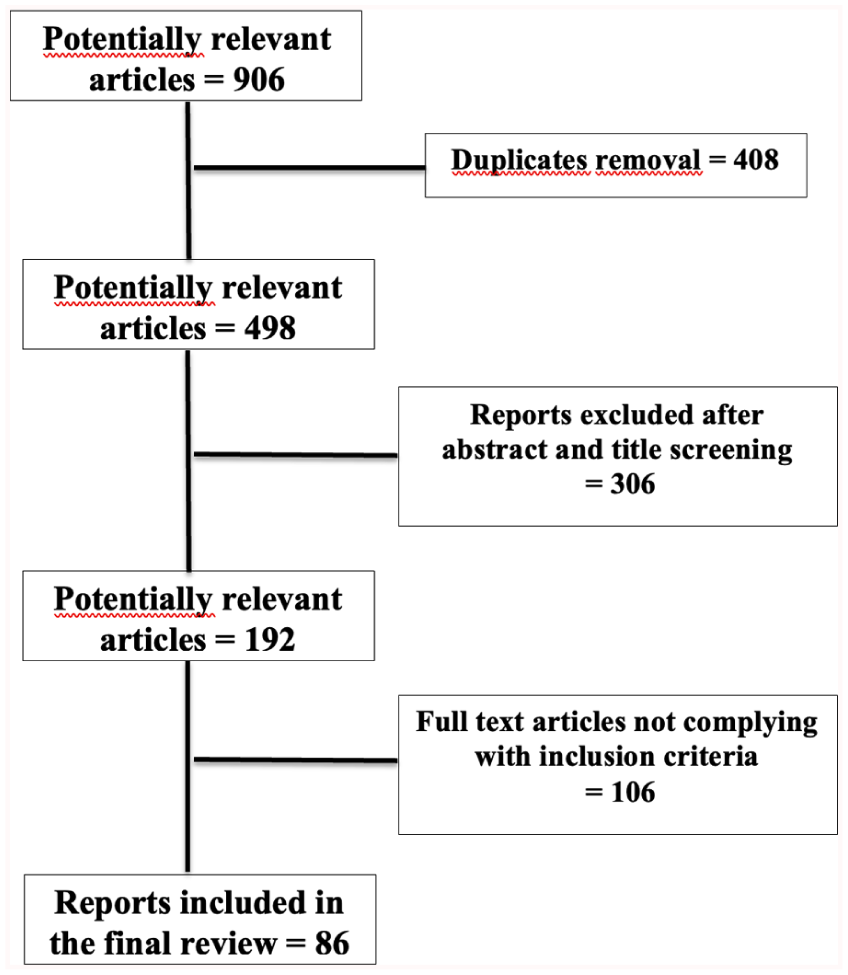
PRISMA flow diagram of study selection process.
Methodological aspects of the selection of patients with GERD and assessment of outcomes?
The relevance of PPI use
Since as many as 60% to 75% of patients with alleged chronic GERD requiring long-term PPI are found not to have GERD after a thorough investigation, it is mandatory to adopt the study design and recruitment of patients accordingly.7,44,45 Consequently, it is vital to verify that each chronic patient with GERD actually needs a PPI to control GERD-induced symptoms. The majority of studies in the current review have enrolled patients with GERD who are on chronic PPI use. In order to ensure that the enrolled patients ultimately need PPI to control symptoms, the recruitment process has to include a so-called “wash out” period during which the patient should document any return of the GERD-related symptoms (+/- endoscopic findings documenting GERD such as esophagitis LA grade B, C, or D or Barrett’s esophagus). If such methodological requirements are not met, it is clear that the frequently used therapeutic outcome variable “need for continued PPI treatment” can be seriously questioned.
PPI refractoriness
Another concept which is frequently used to define the respective study populations, in the literature under survey, is “PPI refractoriness.” Being refractory to PPI is a well-established and described condition in the relevant GERD literature. Hence, to be classified as PPI refractory, a number of specific criteria have to be fulfilled.7,44,45 In the current literature under review, corresponding criteria have only been documented exceptionally despite the frequent use of the term PPI refractoriness as an indication for respective intervention.
Placebo effect
Another important methodological aspect is the placebo effect. Placebo effects in the range of 40–50% have frequently been noted in randomized, double-blind trials including patients with GERD. An effective way to avoid this bias is to include a “sham procedure” (i.e. that in the control/placebo group the entire procedure is carried out with all steps except for the specific antireflux procedure). In addition, a so-called single- or double-blind technique study design should be used. This means that neither the patient nor the clinical assessor are informed regarding which treatment arm patients are allocated to.
Assessment of outcomes in studies evaluating the current techniques
In general terms, the current study populations are well characterized with regard to the proportion of patients with or without endoscopy-verified GERD. 2 The vast majority of reviewed studies enrolled patients with abnormal 24-h esophageal pH monitoring off PPI before enrolment. All studies recruited GERD patients with a disease duration of ⩾6 months. More than 75% of the reports (irrespective of the device evaluated) imply that enrolled patients were PPI refractory, but none of these have a true “PPI refractoriness” been documented.7,8,45
Regarding the Stretta technique, there are data available from four double-blind, sham-controlled, randomized studies (RCT), albeit with a relatively short follow-up time.46–49 There are no independent registry studies with adequate follow-up, but a large number of prospective cohort studies with several years (>3 years) of follow-up.50–54 “PPI refractoriness” was not part of the inclusion criteria. Posttreatment objective assessments were completed in terms of 24-h pH monitoring, PPI consumption, and QoL (Table 1).
Compilation of data forming the clinical documentation behind the “second-generation” transoral endoscopic and surgical minimal invasive techniques for the treatment of GERD. HRQoL stands for health-related quality-of-life assessments (scores < 15–20 being within the normal range) at the time of follow-up.
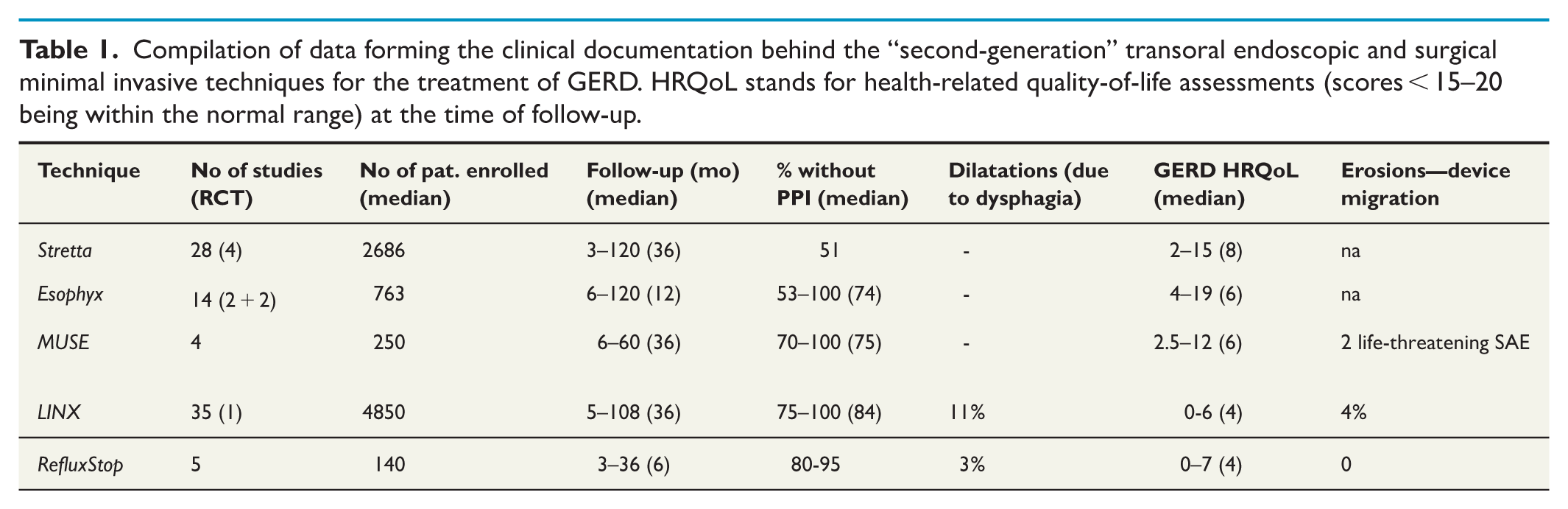
The documentation of the efficacy of the Esophyx technique includes only two double-blind, sham-controlled randomized studies, with a maximum of 12 months of follow-up.18,19 Long-term follow-up of these patients is currently ongoing. Both of these studies included a “washout” period before inclusion. Two additional randomized trials with less stringent study designs have been published, where one includes a short follow-up, whereas one harbors a 5-year follow-up period.21,22 There are several prospective uncontrolled cohort studies published with a follow-up period of ⩾5 years.17,20 “PPI refractoriness” was usually part of the inclusion criteria without giving any documentation behind this specific indication. Posttreatment objective assessments were completed in terms of 24-h pH monitoring, PPI consumption, and QoL (Table 1).
The MUSE technique is a recently introduced device, and the underlying documentation is based solely on prospective experiences of individual institutions and data from an industry-sponsored registry.20,23–25 Again, sparsely documented “PPI refractoriness” was most often part of the inclusion criteria. In none of the studies, the accuracy of the underlying GERD diagnosis was documented in cases with PPI-dependent GERD. Short-term posttreatment objective assessments were completed in terms of 24-h pH monitoring, PPI consumption, and QoL
The LINX technique lacks high-quality scientific documentation in the form of double-blind, sham-controlled, and randomized studies. However, there is one RCT in patients with GERD being “PPI refractory” regarding volume reflux complaints, comparing insertion of LINX versus continued PPI therapy (double dose), showing significant advantage in favor of the former, both in the short- 26 as well as the long-term perspective. 28 In addition, data from individual institutions as well as multicenter prospective protocols are now available with a follow-up >3 years.30,31,37,42 Data from a number of cohort studies comparing the device with traditional LARS are available.34–36,38,39,55 Posttreatment objective assessments have been completed in terms of 24-h pH monitoring, PPI consumption, and QoL.
Data from any randomized, controlled study comparing the LINX technique with an established LARS technique are not yet available.
Given some of the limitations in the documentation, it can be summarized that the use of both the Esophyx and LINX procedures provides lasting symptom-control with normalization of QoL in patients with chronic GERD. Based on the selection criteria in most of the studies, this seems to be true for those patients with GERD who have previously responded well to treatment with PPIs and have only a small (<2 cm) or no hiatal hernia. Furthermore, it seems as if the majority of patients can be off PPIs during the follow-up period after the intervention. Since it is known that it is notoriously risky to implant foreign material around the distal esophagus, it has been particularly important to monitor the risk of erosion(s) or penetration caused by the magnetic ring. So far, this risk has been low but is constantly increasing over time.28,32,56 Nevertheless, the safety profile of these procures seems reassuring. The only exception is MUSE, where some severe life-threatening complications have been reported (Table 1).
Overall, the Stretta seems to be followed by a lower number of patients who can cease PPI intake than the comparators. The device has hitherto not been compared to alternative therapeutic procedures.
Regarding RefluxStop, the short- and long-term documentation is still too limited to allow any firm conclusions regarding its efficacy (Table 1).
Finally, special techniques like endoscopic mucosectomy in the GEJ are still under investigation, and the scientific evidence behind its clinical relevance remains to be established. 57
Discussion
The current review evaluates the efficacy and the quality of evidence concerning novel transoral or minimal invasive antireflux technologies. Despite rapid worldwide dissemination many of these technologies still lack robust scientific evidence. There are a number of factors that have to be carefully assessed when elucidating the scientific background behind current therapeutic alternatives for chronic GERD. The heterogeneity in the phenotype of the various patient groups with GERD is one such factor. For example, the presence and/or size of any hiatal hernia (notifying that a hernia ⩽2 cm should be regarded as being within the normal, physiological ranges) may affect the generalizability of the results obtained, as can the presence and severity of esophagitis (LA grade A B, C or D) or Barrett’s esophagus.2,4,58 Moreover, the size of the hiatal hernia has immediate impacts on the effectiveness of most, if not all therapeutic alternatives. 59 Similarly, patients with GERD who respond to PPIs should be distinguished from those with partial or no PPI response, that is, PPI refractoriness.7,8,44 PPI refractory patients represent a GERD phenotype that is more resistant to traditional therapeutic interventions-procedures, why this term has to be used with great caution.
During recent years, international panels of experts have taken positions on the state of evidence for the respective groups of patients with GERD and proposed suitable transoral endoscopic-minimally invasive treatment options for patients with documented GERD, who have either achieved symptom control with PPIs or have persistent symptoms despite adequate treatment with PPI.60–63 They conclude that for the group of patients with PPI refractoriness, invasive (LARS or endoscopic treatment (SIC!)) should only be offered to those with documented pathological 24-h pH metry and/or esophagitis. The same treatment recommendations are given to those with positive symptom association probability (SAP) during ambulatory 24-h esophageal pH monitoring and to those with documented reflux episodes and significant hiatal hernia (>4 cm). LINX has also been proposed as an appropriate treatment strategy for these groups of patients.61–63 It should be noted that for this rather complex group of patients with GERD, there is currently no or only weak scientific basis for recommending any endoscopic techniques at all. Nevertheless, the LINX and Esophyx procedures are widely disseminated and seem to have surpassed traditional LARS in terms of annual number of procedures in the United States. In the expert surveys, there seems to be a lack of agreement between surgeons and gastroenterologists-endoscopists regarding the superiority-preferences of LARS, LINX, and Esophyx, respectively, in the management of patients with “PPI refractory” GERD.60–63 This disagreement is problematic and leaves open to various interpretations and management strategies depending on the type of specialist that each individual patient with GERD consults.
One of the expert groups 60 expressed an increasing confidence in the role of Esophyx, and by extension also MUSE, which was recommended for patients with GERD but without, or with a small, hiatal hernia, who respond fully or partially to PPIs. All endoscopic transoral methods were considered to be suitable for patients with GERD who respond to PPIs, not the least if results from impedance pH testing, during ongoing PPI therapy, showed low but significant acid exposure in the distal esophagus. Surprisingly, the US experts recommend Esophyx combined with crural repair in GERD patients with a hiatal hernia larger than 2 cm, even given the fact that evidence is lacking. 60 Despite the comparatively solid evidence behind its efficacy in PPI-dependent chronic GERD patients, Stretta is not recommended even for this patient category. 64 Until now, no well-designed comparative trials have been completed between Stretta and alternative transoral or minimal invasive techniques.
The majority of the studies, which allow us to assess the effect of, for example, Esophyx and MUSE, are based on studies of patients who are on PPIs and who respond well to this treatment. In addition, the inclusion criteria in most studies state that the patient must not have a hiatal hernia larger than 2 cm (i.e. no hiatal hernia). In the group showing partial or failing PPI response, there is only one study, of acceptable scientific quality, in which well-investigated patients with GERD were randomized to LINX or to double-dose PPI.26,27 Patients should have persistent complaints of regurgitation, in clinical practice called volume reflux, to be included. As expected, the LINX intervention was superior to the PPI strategy. This is not surprising since it is well known that volume reflux is very difficult to treat with PPIs alone. 4 There is an ongoing RCT in the United Kingdom comparing traditional LARS, with the LINX technique. 66 The results from this study would have the potential to generate important information impacting the long-term clinical decision-making process. Regarding the management of patients with GERD who do not obtain full symptomatic relief from PPIs, this topic has recently been addressed in more detail.4,8,45 For now, LARS performed at centers with high volumes, represents a well-documented long-term therapeutic option for these patients. In addition, with accurate patient selection, the operation can even be performed as a day care surgery procedure. 66 In order to further develop the long-term treatment strategies for patients with GERD, controlled randomized studies must be carried out, comparing these new techniques with the established ones, considering the methodological aspects discussed above. In particular, study designs must consider and circumvent the many pitfalls that exist when recruiting “PPI-dependent” patients with GERD to the active intervention and control arms. The issue of “sham control” design may be perceived by some as ethically problematic. However, much of this problem can be circumvented by focusing on the slightly larger group of patients with chronic GERD, who also have a hiatal hernia exceeding 2 cm in axial length. In recent years, reports are accumulating to show the feasibility and safety of simultaneous laparoscopic cruraplasty and transoral fundoplication or implantation of a magnetic ring insertion.67,68 Thus, laparoscopic cruraplasty can be offered to all eligible for inclusion and intraoperatively randomize the patient to either fundoplication or the experimental antireflux intervention. Preferably, a double-blinded study design should be adhered to as well. When the outcomes of such studies will be reported, robust basis for guiding future patients with chronic GERD across the different therapeutic choices can be offered.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251385759 – Supplemental material for Novel minimal invasive antireflux techniques: A systematic review
Supplemental material, sj-docx-1-sjs-10.1177_14574969251385759 for Novel minimal invasive antireflux techniques: A systematic review by Marcus Reuterwall Hansson, Alexandros Tsoposidis, Apostolos Analatos, Lars Lundell, Srdjan Kostic, Anders Thorell and Bengt Håkanson in Scandinavian Journal of Surgery
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bengt Ihres Foundation, ALF-grant from the region Stockholm, Erling-Persson Foundation, The Swedish Medical Society.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.