
Abstract
Background:
Diagnostic laparoscopy is the ultimate tool to evaluate the appendix. However, the intraoperative evaluation of the appendix is difficult, as the negative appendectomy rate remains 12%–18%. The aim of this study is to analyze the intraoperative motive for performing a laparoscopic appendectomy of an appendix that was proven to be noninflamed after histological examination.
Methods:
In 2008 and 2009, in five hospitals, operation reports of all negative laparoscopic appendectomies were retrospectively analyzed in order to assess the intraoperative motive for removing the appendix.
Results:
A total of 1,465 appendectomies were analyzed with an overall negative appendectomy rate of 9% (132/1,465). In 57% (841/1,465), a laparoscopic appendectomy was performed, with 9% (n = 75) negative appendectomies. In 51% of the negative appendectomies, the visual assessment of the appendix was decisive in performing the appendectomy. In 33%, the surgeon was in doubt whether the appendix was inflamed or normal. In 4%, the surgeon was aware he removed a healthy appendix, and in 9%, an appendectomy was performed for different reasons.
Conclusion:
In more than half of the microscopic healthy appendices, the surgeon was convinced of the diagnosis appendicitis during surgery. Intraoperative laparoscopic assessment of the appendix can be difficult.
Introduction
Appendicitis is the most common acute surgical diagnosis worldwide, with a lifetime risk of 9% in women and 7% in men (1). In literature, the percentage of negative appendectomies varies from 6% to 40% (2, 3). When a muscle-splitting incision by McBurney was performed, the (normal) appendix used to be removed routinely. As the typical scare in the right lower abdomen was synonymous with an appendectomy in the past, this high negative appendectomy rate was justified for a long time (4). Since the introduction of laparoscopy for suspected appendicitis, a normal-looking appendix could be left in place and the negative appendectomy rate decreased (5, 6).
In the Netherlands, annually 16,000 appendectomies are performed, of which approximately 7,000 are laparoscopic appendectomies. Recent data show a 16% negative appendectomy rate (http://www.prismant.nl) despite increase in the use of preoperative imaging and laparoscopic surgery (7, 8). So, annually about 2,500 patients undergo a negative appendectomy. The morbidity rate after a negative appendectomy is approximately 6%, and this includes reoperations and an extended hospital length of stay (7, 9). Additionally, it is associated with higher hospital costs (9).
The guideline of the Dutch Society of Surgeons states that a normal-looking appendix at laparoscopy should not be removed (7). However, in the Netherlands, the negative appendectomy rate seems to be constant over the past decades (prismant). Evidence-based criteria for diagnosing appendicitis are not yet defined. In particular, normal appendices are more difficult to diagnose (10), as well as during open appendectomy as during laparoscopy.
Therefore, it is worthwhile to analyze the intraoperative motive to perform a laparoscopic appendectomy on an appendix that is eventually proven to be not inflamed after histological examination, as understanding this motive could be valuable in lowering the total number of negative appendectomies, and more important, the related morbidity and costs.
The aim of this study is to retrospectively analyze the intraoperative motive to perform a laparoscopic appendectomy on a subsequently histologically proven normal appendix.
Methods
A retrospective study was performed in five hospitals in the northern part of the Netherlands. Participating hospitals were requested to provide patient data and pathology reports on performed laparoscopic appendectomies during 2008 and 2009, using operation identification codes. We included patients who were operated for suspicion of acute appendicitis. Only data from 2008 and 2009 were used, as surgeons even in peripheral hospitals could be aware of the so-called Laparoscopic APPendicitis (LAPP) score. From 2010 till 2012, we conducted a pilot study in our hospital regarding laparoscopic assessment of the appendix. The main aim of this pilot study was to define clear and reliable criteria for appendicitis during diagnostic laparoscopy, the LAPP score. This score should safely reduce the negative appendectomy rate (11).
The operating reports on the negative appendectomies were analyzed. We divided the intraoperative motive for performing an appendectomy into four categories (Table 1):
Appendicitis. The appendix showed signs of inflammation.
Doubtful. Uncertainty existed on the degree of inflammation of the appendix. Appendectomy was performed to be sure.
Appendix sana. The appendix appears to be healthy.
Miscellaneous. Other reasons for performing an appendectomy.
Intraoperative assessment of the appendix.
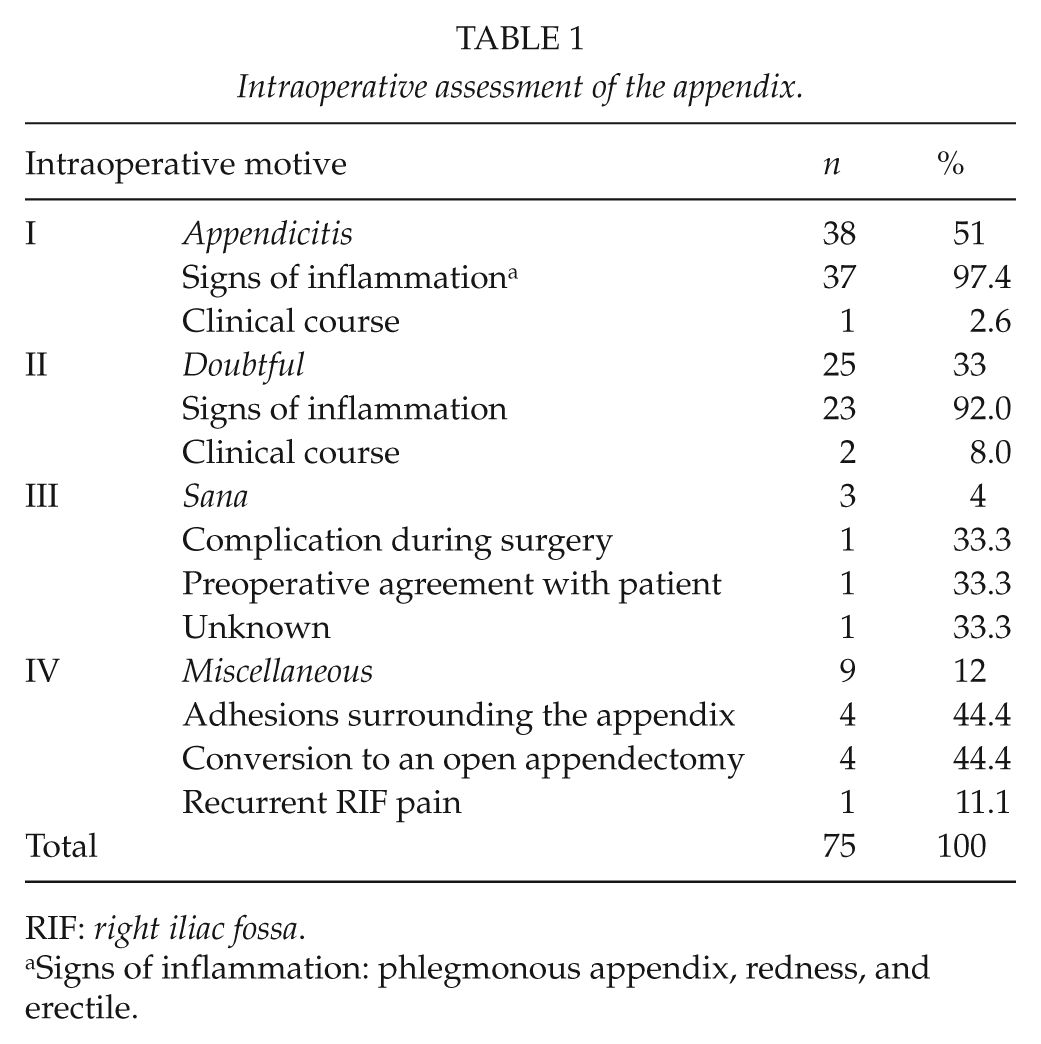
RIF: right iliac fossa.
Signs of inflammation: phlegmonous appendix, redness, and erectile.
Data were analyzed using the SPSS statistical software package, version 19.0. Descriptive statistics were utilized for representation of interhospital differences on quantities of appendectomies performed on healthy appendices.
Results
Throughout 2008 and 2009, the five participating hospitals performed a total of 1,465 appendectomies (Fig. 1). In 565 cases (39%), the appendectomy was performed using McBurney’s incision, and in 841 cases (57%), a laparoscopic appendectomy was performed. In 59 cases (4.0%), the appendectomy was performed as an additional part to another surgical procedure (e.g. urological procedures) or an interval appendectomy was performed (appendectomy à froid).
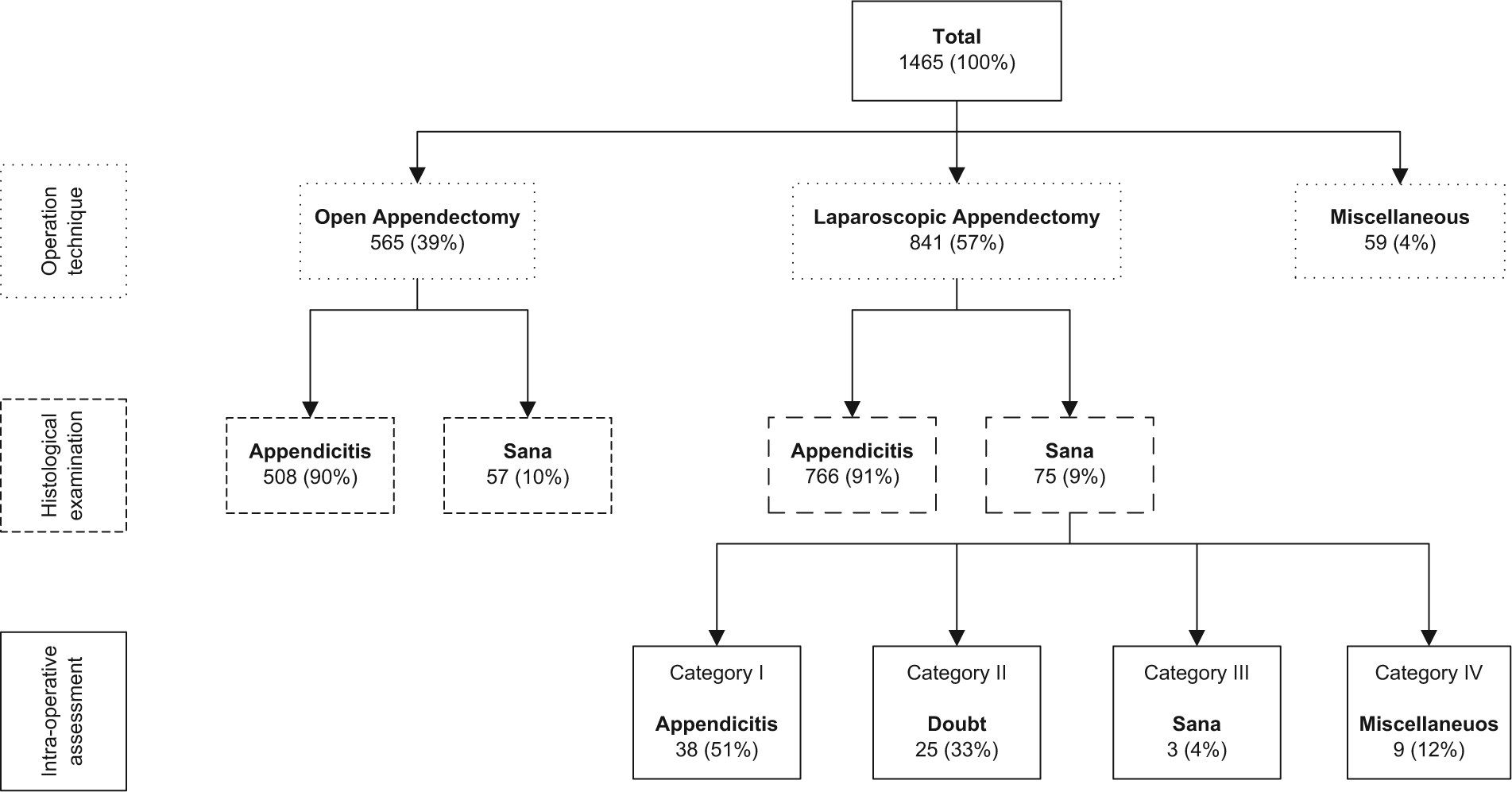
Flowchart inclusion.
No statistically significant difference was found in the percentage microscopic noninflamed appendices removed between patients operated using McBurney’s incision and laparoscopy, 57 (10%) and 75 cases (9%), respectively, (p = 0.461). Interhospital differences in negative appendectomies were observed, varying from 7% to 20% of cases. Mean age of patients where an appendix sana was removed was 29 years (range = 5–77 years), and 71% of these patients were female.
The operating reports of all 75 laparoscopic appendectomies of histologically proven normal appendices were analyzed (Table 1). In 38 cases (51%), the surgeon was convinced of the diagnosis of appendicitis (category I). In 25 cases (33%), the operating surgeon was in doubt about the presence of inflammation (category II). In 3 patients (4%), the surgeon was aware that he or she removed a noninflamed appendix (category III). In the remaining 9 cases (12%), the appendix was removed for different reasons (category IV).
In categories I and II, the decision to perform an appendectomy was in almost all cases mainly based on visual inspection of the appendix (97% and 92% respectively). In a minority, clinical course was mentioned as being decisive in performing the appendectomy. Visual inspection of clinical signs of inflammation seems to be the most crucial factor in the decision making whether to perform an appendectomy or perform a diagnostic laparoscopy alone.
Three patients underwent a negative appendectomy while the surgeon knew he or she removed a normal appendix (category III, 4%). The reason in these three cases were as follows: apparent injury to the appendix in one patient, preoperative agreement with the patient on performing an appendectomy anyway, and in one more patient, there was no reason provided in the operating report.
Discussion
This study presents a retrospective analysis of the surgeon’s rationale to perform a laparoscopic appendectomy on a postoperative histologically proven normal appendix. We found a negative appendectomy rate of 9% in the laparoscopically operated patients, which is in line with the literature (6). After analysis, 51% of the surgeons were sure of the diagnosis of appendicitis and 33% were in doubt and therefore choose to perform an appendectomy. So, in the vast majority of cases (n = 63, 84%), the surgeons who performed a laparoscopic appendectomy on a histologically proven normal appendix assessed the appendix as inflamed.
In our view, there are several explanations for our finding that in the majority of negative appendectomies, the operating surgeon was convinced of the diagnosis appendicitis. First, the surgeon could be influenced by the presentation of the patient and thereby with the preoperative provisional diagnosis of acute appendicitis. In case of strong clinical indications for the diagnosis appendicitis, it requires more courage for the surgeon to assess the appendix objectively and leave a normal-looking appendix in place. Unfortunately, preoperative data such as medical history, physical examination, and diagnostic imaging are unknown.
Preoperative imaging is more commonly performed during the last years, in order to decrease the total number of unnecessary operations/appendectomies. This has led to a significant decrease in negative appendectomies in prospective trials (12). However, these results might be difficult to reproduce, as ultrasonography of the appendix is operator dependent and not all hospitals have experienced and dedicated abdominal radiologists.
Some surgeons perform an appendectomy to prevent future appendicitis. However, van den Broek et al. (5) described the safety of leaving a normal appendix in situ. In addition, the chance to undergo an appendectomy in the future is very low. Some authors suggest the presence of microscopic inflammation in a macroscopically normal appendix, and therefore recommend routine appendectomy (13). However, the natural course of these macroscopically normal appendices is not known. We do know that in our pilot study with a follow-up of 3 years, 18/22 patients where a macroscopically normal-looking appendix was left in place did not develop appendicitis afterward. Two patients were lost to follow-up, and two patients died from another cause (data not published). More research is needed to convince the surgeons who are reluctant to leave a normal-looking appendix in place that it is safe.
In order to improve the laparoscopic assessment of the appendix on signs of inflammation and thereby reduce the number of false-positive findings, a laparoscopic grading system should be designed. This system should not lead to an increased number of false-negative assessments of the appendix. In our center, we designed the LAPP score (11). This score needs to be validated in a prospective multicenter study.
This study has some limitations. The intraoperative interpretation of the surgeon is not necessarily well presented in the operation reports. A well-known phenomenon is the self-affirming aspect of people (14). Hence, it is likely that the operative report of a removed appendix will be written in line of the appendectomy, rather than describe a fully healthy appendix. Unfortunately, we cannot prove this assumption, as there is no intraoperative image of the appendix available. Also, the use of templates for writing an operation report could make it more difficult to describe certain nuances. On the other hand, an advantage of templates is the structure. Another limitation of this study is that the operation reports of appendices that were proven to be inflamed at histological examination were not analyzed and operation reports of diagnostic laparoscopies alone were not included in this study. Possibly, some appendices that were intraoperatively assessed to be not inflamed were postoperatively proven to be inflamed by histology.
In conclusion, this retrospective analysis of operating reports on patients where a histologically proven normal appendix was removed shows that 51% of the surgeons intraoperatively assessed the appendix as inflamed. In a third of the cases, there was doubt about the presence of appendicitis.
So, the most common cause of the negative appendectomy seems to be the false-positive intraoperative assessment of the appendix. There seems to be a need for standardized criteria for a laparoscopic assessment of the appendix. This can possibly lead to a decrease in the negative appendectomy rate and related morbidity and costs.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.