
Abstract
Background and Aims:
Gender balance in surgical specialization has received increased focus, as women have traditionally made up a minority in surgical specialties. Little is known about how surgical disciplines are approaching gender equity and balance in general and subspecialty surgery in Norway. The aim of this study was to explore gender distributions across surgical disciplines to investigate gender balance and changes over time.
Material and Methods:
An observational, cross-national study derived from specialists statistics on board certification in Norway. We investigated gender balance for surgical disciplines for the time period 2008 to 2024. Temporal time trends were investigated for fiscal years 2010, 2015, 2020, and 2024. Statistical analyses were done by the Poisson regression for temporal trends and gender distribution.
Results:
For the 10 surgical disciplines investigated, the total number (n) of surgical specialists increased by 33.3% during the period. Numerically, general surgery, gynecology, and orthopedics made up 72% of all surgeon specialists in 2024. The female rate increased from 20.2% to 36.2% across all surgical disciplines. The observed female rate in 2024 was the highest in gynecology (75% women) and the lowest in thoracic surgery (<10% women). Despite a significant increase (with P < 0.001) in the female rate in all specialties, only gynecology and breast-endocrine surgery achieved >50% female rate among specialist surgeons.
Conclusion:
Considerable variation in the rate and speed of obtaining gender equity exists across surgical specialties, concerningly in some of the larger surgical specialties. Further investigations should focus on identifying and addressing factors influencing the recruitment and retention of women in surgical specializations.
Keywords
Introduction
Globally, the proportion of women is increasing in the medical workforce across several countries, although at variable rates.1–5 Despite the attention received and the fact that the majority of medical students for the past two decades are female, surgical disciplines still face a significant and persistent gender gap dominated by the male gender.6–8 In Scandinavia, the shift toward a higher rate of women in medical school occurred around the turn of the millennium, with women making up a majority of admitted students by that time.7,9 In the United States, the female majority in medical school was reached in 2004. 10 However, the corresponding shift in gender representation across medical specialties has been slow,8,11 and concerns regarding recruitment of women into surgical training in particular have been debated fiercely.4,6,12–15 The decision to pursue a surgical career, or even avoid it altogether, is likely a multifactorial choice.4,10,16 Even among those who decide to enter surgery as a profession, there does not seem to be just one “surgical stereotype,” and personality traits seem to differ across sexes. 17 Another factor is that the surgical profession itself has changed as a discipline, with issues related to working-time restrictions, training opportunities, increasing subspecializing within surgery, and issues with work–life balance.18,19 Past investigations among medical students of both genders in Norway found diverse attitudes toward career choice, with influences on career decision ranging from perceived prestige and ambitions to the potential for an impact, positive or negative, on work–life balance related to different disciplines. 20 Issues related to family life and parental leave demonstrate considerable diversities globally, 21 and pressures regarding work–life balance seem to be a universal issue, 4 with an impact on recruitment of women to surgery. 22
Despite the pressing issues of gender gaps and surgical (sub-)specialization, remarkably little is known about how surgical disciplines in the Nordic countries are addressing gender equity and balance, let alone the rate of women in the surgical disciplines, both in general surgery and surgical specialties. The aim of this study was to investigate gender balance and changes over time in Norway for 10 selected surgical specialties.
Methods
Study ethics
No formal ethical approval was needed, as the data are anonymized and based on public repositories.
Study design and data accrual
Observational cohort of all-time registered specialists with board certification through the Norwegian Medical Association (later Norwegian Directory of Health) and as documented through Statistics Norway (www.ssb.no) and doctor-statistics in Norwegian Medical Association (Den norske legeforening). 23 Complementary data were kindly provided by chief statistician Anders Taraldset, Legeforeningen (Norwegian Medical Association).
For the current study, data were retrieved from 10 surgical specialties for comparison, including general surgery, gastrointestinal surgery, vascular surgery, breast & endocrine surgery, pediatric surgery, cardiothoracic surgery, plastic surgery, urology, orthopedics, and gynecology.
Study period
Data were obtained as available from the period of the first quarter of 2008 and up to the last quarter of 2024. Only specialists <75 years of age are reported for any year in the study period, and the last data obtained were per 14th November 2024.
In order to investigate changes for time periods, data were investigated for arbitrarily selected 5-year intervals from 2010, 2015, 2020, and up to 2024.
Surgical specialization and subspecializing in Norway
In Norway, training in surgery has historically followed through initial certification in general surgery. The Norwegian Surgical Association was established in 1911, but certification as a surgeon followed through several changes until a formal designation of specialty training in the late 1970s through the Norwegian Medical Association was agreed on. The historical evolution of surgical specialty training is beyond the scope of this article, but for context, some brief notes are presented for the designations to surgery in Norway. For one, general surgery was designated as the main specialty in 1977, 24 with further subspecialty training possible in pediatric surgery, gastrointestinal surgery, urology, thoracic surgery, and orthopedic surgery. Vascular surgery became a subspecialty in 1986 and breast/endocrine in 2006. Orthopedic surgery was separated from mandatory full training in general surgery as requirements in 1997 and became an independent specialty, even if a mandatory period (some 2 years) of general surgery rotation was maintained until 2009 but is no longer required. Breast/endocrine surgery became a recognized branch of surgery (not simply included in general surgery) in 2008. The combined specialty of obstetrics and gynecology was established in 1947 (and had existed as separate specialties as “obstetrics” and “womens’ disease” prior to that). Both gynecological surgery and plastic surgery still require a mandatory period of general surgery rotation during training. However, with increasing subspecialty focus, several previous “sub-branches” of surgery have become independent surgical specialties, with all past “branch” disciplines becoming independent surgical specialties since 2019.
Included surgical disciplines in the current study
For the current study, we chose to include the “surgical specialties” in the broadest sense, including general surgery, orthopedic surgery, and gynecology and obstetrics as numerically large medical specialties and for which surgery is a main or considerable part of the treatment armamentarium. Also, all surgical specialties previously derived from “general surgery” were included. Hence, 10 disciplines were overall included (general surgery; gastrointestinal surgery; vascular surgery; breast-endocrine surgery; urology; plastic surgery; pediatric surgery; cardiothoracic surgery; orthopedics; and gynecology). Notably, smaller, independent tracks to surgical specialties such as neurosurgery, ear-nose-throat surgery, and ophthalmology were not included in the current study.
Statistics
Analyses were done using IBM SPSS statistics (v. 29.0.2.0 for Mac) and R version 4.3.3. 25
The chi-square test for trends is used to test for differences in gender proportions across fiscal years and per subspecialty. For modeling time trends in gender rates, a Poisson regression model with a log-linear time trend was used. The estimated regression lines are plotted together with the observed data for each specialty. A block-permutation approach was used for estimating the P-value of the time trend parameter, due to the temporal dependency in the data. All tests were two-tailed, and P-values < 0.050 were considered statistically significant.
Results
For the 10 surgical disciplines investigated, the total number of surgical specialists increased by 33.3% during the time period (from n = 3120 in year 2010 to n = 4159 in year 2024). The overall rate of women increased from 20.2% to 36.2% (Fig. 1A). The total increase in the number of surgical specialists is unevenly distributed across disciplines (Fig. 1B), with the three disciplines of general surgery, gynecology, and orthopedics making up a large majority of all surgeons (for fiscal year 2024: n = 2988; 71.8%).
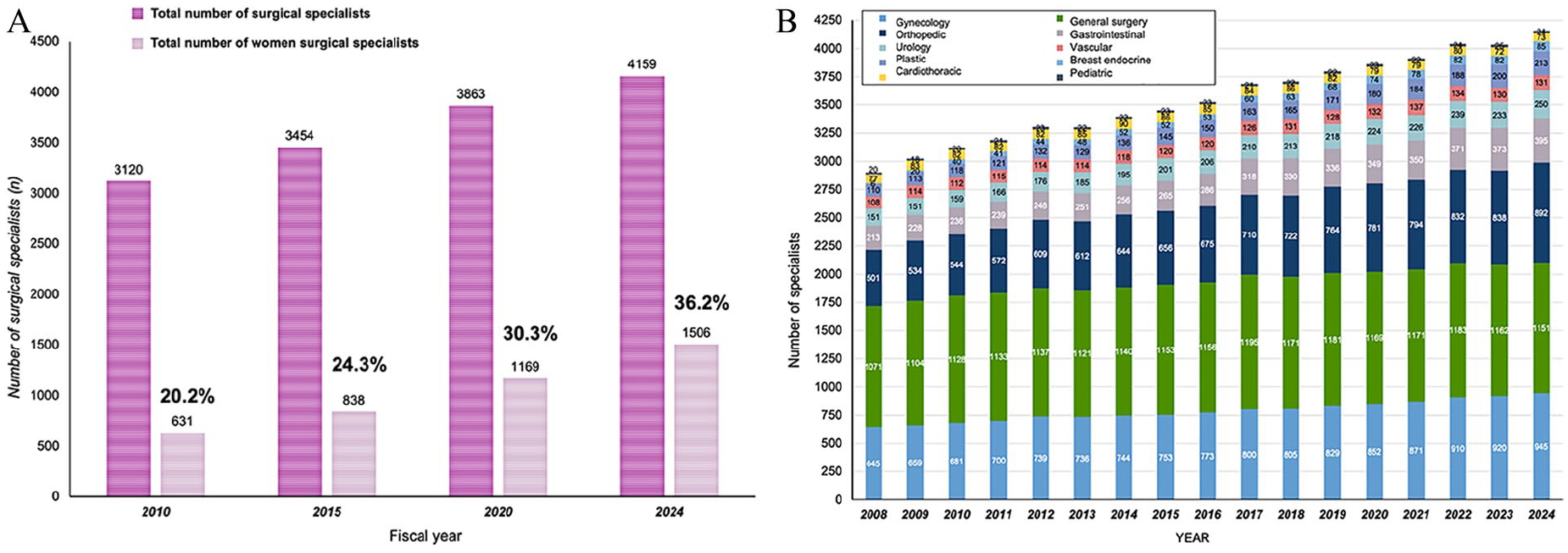
Absolute number of registered surgical specialists over time in Norway. (A) Total number and increase of surgical specialists for fiscal years in Norway, with corresponding number of women specialists (n, %). (B) Absolute number of surgeon specialists over time and by contribution for each of the 10 specialties.
The numerical change over time in surgical specialists is also unevenly distributed across surgical disciplines, as demonstrated in Fig. 2. General surgery seems to have stabilized (even with a slight decrease), with the strongest numerical increase in specialists seen in gynecology, orthopedics, gastrointestinal surgery, urology, and plastic surgery (Fig. 2).
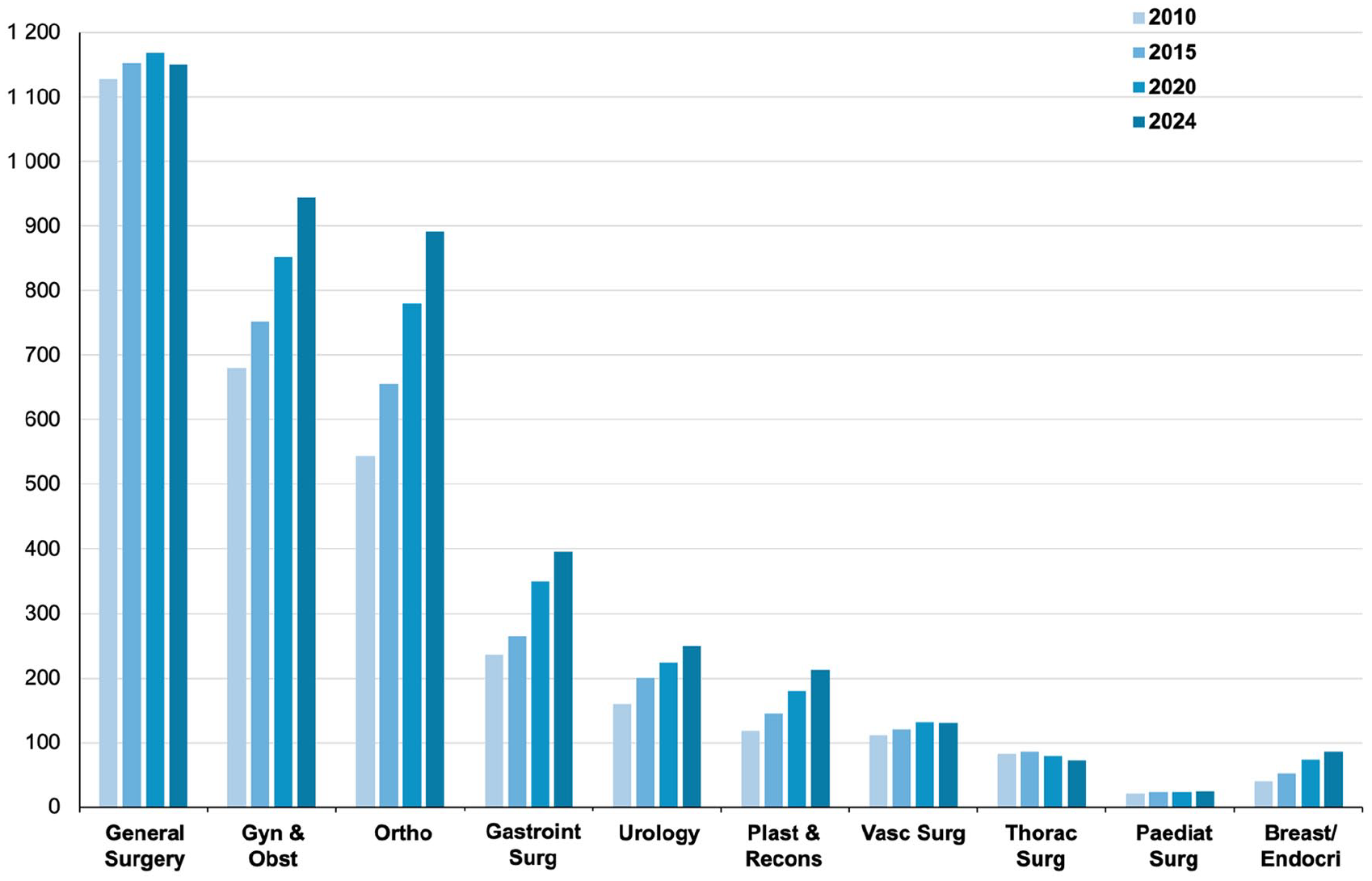
Absolute number of surgeon specialists over time. Legend: For the selected 4 fiscal years (2010, 2015, 2020, 2024), demonstrating change in absolute numbers (number of surgeons within a surgical specialty) as well as contribution in share number (the number within a surgical specialty related to any other surgical specialty; that is, the share difference in number of general surgeons compared to the number of plastic surgeons) for each specialty across the 10 selected surgical disciplines.
A statistically significant increase in gender distribution over time was found across all surgical specialties (Fig. 3). The temporal trend Poisson regression for specialties in Fig. 3A was highly significant (P < 0.001), with P = 0024 for thoracic surgery. For specialties in Fig. 3B, a similar strong trend was found for four of the specialties (P < 0.001) and for pediatric surgery (P = 0.005).
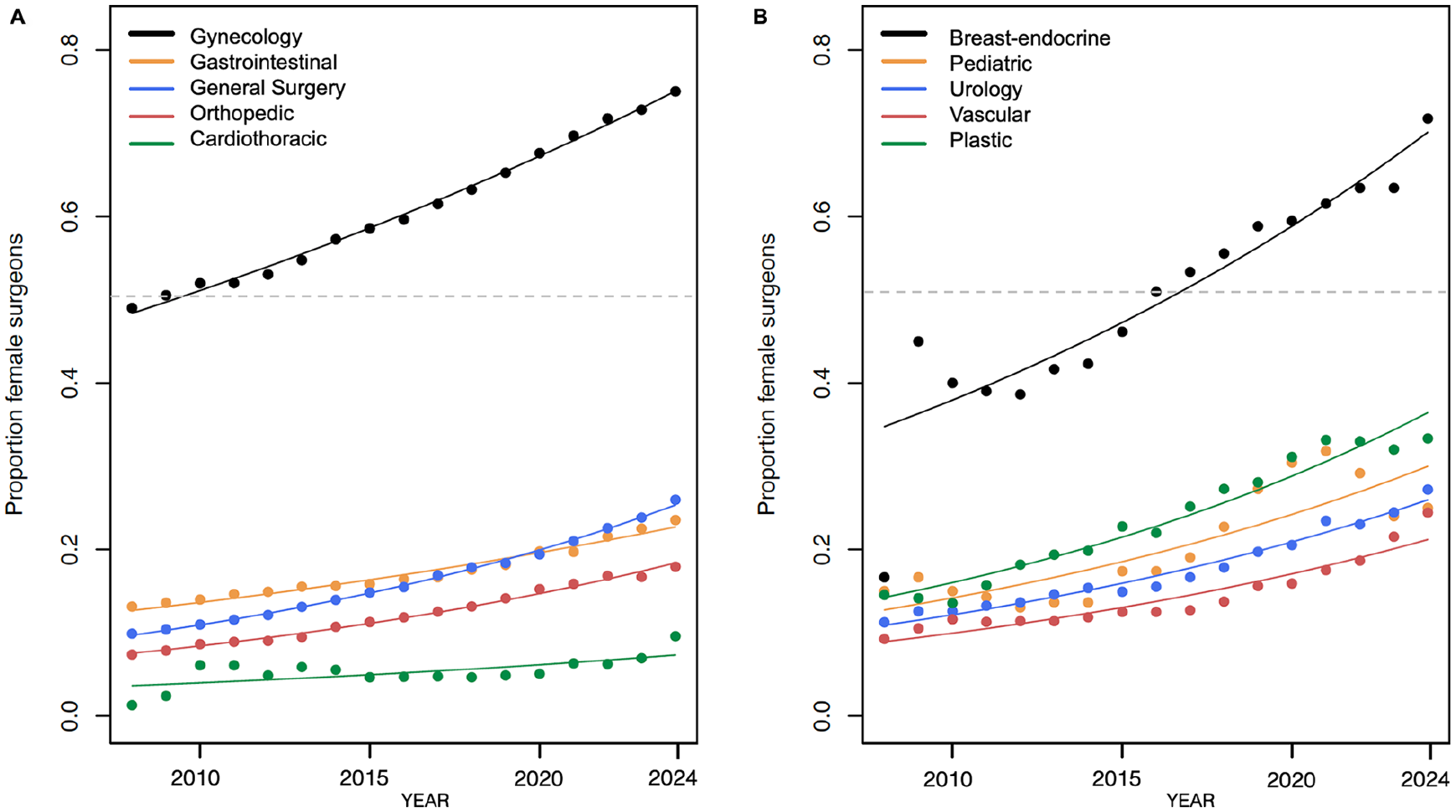
Poisson time-trend regression analysis of female rate of surgeons according to surgical specialty. (A) The time trend in change of female rates in gynecology, gastrointestinal surgery, general surgery, and orthopedics was statistically significant (P < 0.001) for all surgical specialties, except for cardiothoracic surgery with a P-value of 0.024. (B) The time trend in change of female rates in breast-endocrine, urology, vascular, and plastic surgery was statistically significant at P < 0.001, except for pediatric surgery with P = 0.005. The full line represents the Poisson regression line for female rates in each surgical specialty over time. Dotted gray line represents the cut-off for a 50% gender rate. Datapoints represent the female rate for each year and each specialty.
Among the surgical disciplines, it is only gynecology and breast-endocrine surgery that have a women proportion surpassing 50% (gynecology had a >50% in 2009 and breast-endocrine surgery in 2016). However, even if a high female rate is found (75% and 72%, respectively, for gynecology and breast-endocrine in 2024), the numerical contribution is considerable with some 945 gynecological specialists in 2024 compared to 85 in breast-endocrine surgery.
Of note, the two other large surgical specialization, general surgery and orthopedics, have 26.0% and 17.9% women specialists, respectively. Only cardiothoracic surgery remains below 10% women specialists.
Discussion
This study found a statistically significant increase in the female rate over time and across 10 surgical specialties. However, only two surgical specialties have more than 50% women rate in Norway in 2024 (gynecology and breast-endocrine surgery), and large numerical differences in numbers of specialists exists, from several hundreds to a mere handful of specialists in a specialty (Fig. 2). A numerical increase as well as strong rate increase in the female rate for plastic surgery was seen. Both general surgery and orthopedic—both being two large surgical disciplines—are recruiting women at a relatively slow pace, and currently, only have 1 in 4 and 1 in 5 of every surgeons being female, respectively. For both general surgery and orthopedics, a statistically significant increase in women rates was found year-on-year. A stable and rather unchanged absolute number for general surgery specialists as the largest surgical discipline was matched with an increase in the female rate. The latter may be due to more elderly generation of elderly surgeons reaching retirement age, rather than only a contribution of more women to general surgery. Notably, as most previous “branch” specialties have become independent surgical disciplines with no prior requirement of general surgery, the number of general surgeons may stagnate and even decrease.
Some have argued that women avoid surgical disciplines due to work–life balances and working conditions. This may only partly be true, as the life–work balance with consistent and lifelong on-calls in gynecology does not seem to have discouraged women from choosing and even preferring this discipline in medicine. Indeed, one may envision that other factors and experience during medical school that relates to cultural barriers, bias-mindsets, and microaggression may be more likely determinants of choice of a surgical or non-surgical career.13,26,27 Although gynecology does imply lifelong on-call demands when working in hospitals, it also offers the opportunity for entering private practice and avoiding the on-calls altogether. This may be one of the reasons why this specialty has seen an unprecedented rate of women recruited compared to other specialties. The one specialty of breast-endocrine also achieving a high rate of female surgeons is a specialty favoring a predominantly elective practice, little or no on-calls (as currently practiced in most centers in Norway), and a focused area of surgery, hence attracting a high female rate. However, the share numbers are small, and the contribution from breast-endocrine surgery as such is thus not a driver to attract women into surgery. There are more women in total in other surgical fields (i.e. general surgery, gastrointestinal, orthopedic, and gynecological surgery), and these specialties are likely more important for increasing the total number of female surgeons for the future. Also, the surge in females in breast-endocrine surgery came after the formal start of this specialization in 2008, with a steady increase since 2009 and onwards. Women recruitment to surgery may be a global issue with generic challenges recognized across different countries and continents,27–33 or some more particularly specialties prone to gender biases, such as reported in cardiothoracic surgery. 34 The solutions to these issues may be in part generic across specialties (i.e. work–life balance) or specialty specific (i.e. lack of role models), and several approaches to recruitment of new trainees may be warranted to attract medical students into a surgical career.
A previous study from North America found a relative flattening of the curve in terms of recruitment of women to surgical disciplines. 1 The slow rate of accrual is of concern for several reasons. One is the lack of recruitment of new specialists, as the male-dominated specialist will see a proportionate share of retired specialists in the year to come. The other is the reason behind the slow recruitment, whether the slow recruitment simply represents a lag time of training duration to board-certified specialist in surgery or if it reflects that women are simply avoiding surgical disciplines for other reasons.
Some limitations need to be mentioned. One is the lack of information of whether the certified surgical specialists actually work in his or her discipline or rather work in another medical field. Retention of specialists may also be an issue, that is, some surgeons shift to general practice after completing training due to life or family issues. Others may seek private specialty practice (i.e. in gynecology), although this opportunity is limited within the Norwegian public health care system. However, increased private health care insurance makes some specialties increasingly attractive for private practice, including general gynecology, outpatient type of orthopedic surgery, and an increasing rate of plastic surgery. The latter also with a heavy influence of cosmetic and aesthetic procedures being offered in the private sector. Furthermore, quite a few surgeons still hold “double specialties” (e.g. general surgery as primary specialization and then gastrointestinal or vascular surgery as a subspecialty), meaning the number of active surgeons may be lower than the number of specialists registered. However, this has declined over the years as the previous branch specialties have become main surgical specialties (i.e. breast-endocrine surgery and urology). In addition, a proportion of specialist-registered surgeons may be approaching or beyond retirement age, resulting in a lower number of actively working specialists (particularly those aged 67 and above) compared to the number of registered specialists in any field.
In Norway, no formal person-registry exists for each time period and for each individual specializations, and certain assumptions must be considered when interpreting the data set. For each time period, a specialist is registered when he or she has applied for board certification and this application has been approved (central process held by the Norwegian Medical Association; later by the Directory of Health). It does not imply that the same person works in that specialization and further certified specializations may also be applied for based on the given accreditation process at any given time period. For example, prior to 2019, a certified general surgeon also further subspecialized in vascular surgery may only work as a vascular surgeon and not as a general surgeon per se. This “double specialization” registration ceased after 2019, and it may take some time to have an effect on the actual numbers as well as female rates, as the formal number of general surgery specialists may decrease. Hence, future investigations and statistical analyses for comparison will need to take this into consideration. Also of note is that, for the current data, any registration as a specialist in Norway implies that the person resides in Norway; hence, certified specialists in Norway working abroad are not counted in these statistics.
Some strengths to this study are warranted to mention. Overall, despite some limitations, the data should reflect relatively well the change in surgical specialists over time and for the nationwide depiction of trends in Norway. We are not aware of any comparable or previous comprehensive analyses to investigate this and believe these data represent a novel contribution to the gender evolution analysis in surgical disciplines in Norway. We would be eager to see comparable data from the other Nordic countries and to compare it to other European countries. More importantly, the data should be used as a baseline for discussing future workforce and recruitment to surgical disciplines, involving various stakeholders, including the medical associations, the governmental agencies and even politicians for awareness and future planning.
Conclusion
In this study, we found a significant increase over time in the rate of female surgeon specialists across 10 selected surgical specialties. However, there are large differences in the rate of women accrual and actual female rates for each specialty and in the share number of specialists for any given surgical discipline. Only two specialties had a female rate over 50%. An emphasis on recruitment of women to surgical disciplines may be warranted, given the need to strengthen and keep up the number of surgeon specialists for the future.
Footnotes
Acknowledgements
The authors thank senior statistician Anders Taraldset for providing updated data on surgical specialists from the Norwegian Medical Association statistics.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CFT reports having received personal fees from AstraZeneca, Pfizer, and GlaxoSmithKline, but none with relevance to the current work. None of the other authors declare any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Trial registration
Not applicable.