
Abstract
Background and Aims:
All Nordic countries have reported a high female admission rate to medical schools over the past decades. A similar female rate is not observed among surgical specialists. The aim of this study was to report the observed female rate in admission to medical school and compare to the female recruitment rate observed in surgical training.
Material and Methods:
An observational, cross-sectional, nationwide, point-prevalence study (index year 2024) derived from registered medical students (from 2010 to 2025), number of trainees, and certified specialists’ statistics of active specialists (defined <70 years of age) in 10 surgical specialties. The national averages of female rate were compared.
Results:
The female rate of medical students was 70% (n = 3460 females; n = 1491 males) in Norway in 2024 (with stable rate since 2020 and >60% female rate since 2010). In 2024, there were a total of 9601 doctors in training across 46 medical specialties, with a female rate of 62.7% (n = 6022) of trainees. Among all trainees, some 13.6% (n = 1304) were registered in one of 10 surgical specialties, with 62.7% (n = 817) female rate. Gynecology (n = 324) stands out with >90% of the trainees being female. Excluding gynecology, the female rate of surgeon trainees drops to 53.5% (524 of 980). Even though breast-endocrine and plastic surgery have a high female rate of trainees (>80% and >70%, respectively), they make up for a relatively small actual number of surgical trainees altogether (n = 23 and n = 40, respectively). For 2024, the total number of certified surgeons (n = 3636), with 1409 (38.8%) being female, was lower than the national average for all specialties (48.9%). A considerable number of male surgeons (>30%) are approaching retirement age within the next decade.
Conclusion:
Female rate of admission to medical school has been >60% for two decades. Female rate of trainees and specialist surgeons remains lower than the reported national average while improving in general surgery, orthopedics, and gastrointestinal surgery in terms of numbers and rate of females. Research into recruitment, retention and retirement projections is needed.
Keywords
Introduction
Attracting medical students to the surgical profession is of great importance. Inviting the novice student into the closed environment of the operating theater is a unique opportunity to present the attractiveness and value of a surgeon’s way of providing patient treatment.1–3 Unfortunately, issues related to barriers against gender balance are described globally and presented as still unresolved challenges in medicine.4–7
Becoming a medical doctor was historically a male profession across all specialties. Over the past several decades, there has been a steady increase in the number of women admitted to medical schools in Norway. A study from Norway covering the time periods from the 1950s up to the 1990s found that women would tend to choose medical specialties with lesser prestige; women would represent a relative minority among the academic elite; and there would be few women in leading positions in medicine. 8 Women who entered medicine during the latter half of the 20th century were a minority overall, with very few entering surgical disciplines as specialization. Indeed, a gender balance of 50:50 men and women in medical schools was only achieved at the turn of the millennium in Norway. 9 Since then, a majority of admittees to medical school has been women, as also reported in other Nordic countries.10,11 However, despite a female surplus in medical schools, the recruitment of women has been slow in several specialist disciplines, and particularly in some of the surgical disciplines. Around the year 2000, only about 5% of general surgeons were women in Norway. While some studies into medical students’ preferences were done around the millennium, these trends may not be relevant to modern-day students. 12 In 2010, the rate of women in general surgery in Norway was still <10%. 13 The slow admission rate and lack of gender balance led to discussions in major medical journals regarding the benefit of the high admission rate of women to medical school.14,15 In Norway, the restructuring of the training in surgery together with the lack of women’s recruitment to surgery has been discussed as a concern, 16 along with the change in surgical specialty training and restrictions in working hours. 17
Further investigations into the preferences and career choices of Norwegian medical students were done for certain student cohorts,18,19 but without the ability to clearly define why and what would influence medical students career choice. The most apparent findings may have been that preferences and balance between ambitions and prestige, together with views of lifestyle and family do change from the first year to the last year of medical school, with greater emphasis on opportunities for life–work balance toward the latter years. 19 These appear to be universal issues that are impacting on choice of medical careers globally. 4
Over the past decade, no studies and little focus have been put on the recruitment rate or the lag of female recruitment to surgical specialties. In this study, we aimed to investigate the gender rate of women in medical school and compare the corresponding gender balance across surgical specialties and some competing non-medical specialties for comparisons. The hypothesis is that surgical specialties have a lower rate of females compared to the long-standing high female admission rate to medical school.
Methods
Study ethics
No formal ethical approval was needed, as the data are anonymized and based on public repositories and statistics curated under the auspices of the Norwegian Medical Association (NMA).
Study setting
In Norway, admission to medical schools is based on grades or points from high school, with the grade requirements being among the highest averages for any type of study. Most of the admitted students also obtain their medical degree, and hence, the drop-out rate from medical school is low. After completing medical school (duration of 6 years), there is a mandatory 18 months of general clinical training to obtain a full medical license to practice medicine and start specialization. These 18 months include 1 year at a hospital (usually rotating through two or three specialties, including surgery and internal medicine) and a subsequent 6 months in general practice. After this mandatory period of clinical practice as a junior doctor, the candidate can apply for available positions for specialty training, including surgical training to become a specialist. Specialist training is set at 5 years but usually takes longer due to rotations, maternity/paternity leave periods, and bottlenecks in mandatory courses or required procedures needed to become a specialist.
No formal centralized program for specialty training exists, and the specialty training is employment-based and per application for positions. The mandatory and voluntary courses are based on a central core curriculum with some regional variations in delivery and rotations between surgical services. Hospitals are qualified for specialty training as either group 1 or group 2 training sites, with a formal period required at a group 1 training site (usually at university hospitals) to acquire experience with some more complex types of procedures or more centralized care of patients. The employer grants permissions for the period of training, while no guarantee exists for consultant positions after specialty training. An urban–rural gap in available specialists exists, also for filling training positions.
Study design
The study design includes an observational national cross-sectional cohort of registered medical students, candidates currently undergoing surgical training in one of the surgical specialties, and a number of assumed working-active consultants for the surgical specialties. The data are derived from statistics available through the Norwegian Medical Association (NMA) and Norway Statistics for working professions and students, with some restrictions implied. For all Norwegian doctors, the membership rate in the NMA is about 94% (and as high as 97% for those in medical training in Norway, as liability and indemnity insurance as a practicing doctor is part of the membership. Most non-members are staff in purely administrative or non-clinical positions), and hence, data were assumed to be valid and representative for the rates provided. The study aims to present national data on gender rates among medical students in Norway, as well as gender rates among surgical trainees and gender and age rates for surgical specialist across surgical disciplines.
Data accrual for each category
The number of medical students and the female rate of medical students are presented as determined by statistics provided by the NMA and its subsection Norwegian Medical Students’ Association (Norsk medisinerstudent forening, NMF), for the years 2010–2024, with the last statistics updated as per 6 February 2025. 20 The membership for medical students in the NMA is about 80% in Norway and about 45% for medical students abroad (based on numbers for 2024). However, the statistics from the NMA on the number of medical students are based on the registry for higher education (for Norwegian students), which gives the exact number of medical students per university and for the students enrolled at foreign medical schools from the number of medical students receiving grants to medical school from the Norwegian State Educational Loan Fund (Statens Lånekasse), which is the primary source for funding of higher education in Norway.
The number of surgeons in training and the female rate of surgeons in training are presented for the index year 2024, as available per 11 November 2024. To assess the point prevalence of surgeons in training, this was culled from the number of members in a specialist association at the time of data collection. Of note, for all members of the NMA, a registration to a specialist association is mandatory; hence, this serves as a good proxy for the numbers in training in that specialty at any given time point. Hence, a trainee registered as a member of the Norwegian Association for Gastrointestinal Surgery or Norwegian Association for Orthopedic Surgery, will be registered as such (either as “under training” if not specialist certified, or as “certified specialist,” if formally approved as specialist). For the two previous main specialties, General Internal Medicine and General Surgery, a voluntary opportunity to “double register” for both membership in “general surgery” (under the Norwegian Surgical Association) and also the subsequent subspecialty training of, for example, “gastrointestinal surgery” or “vascular surgery,” is possible. However, after 2019, general surgery is no longer required as a completed full training before subspecialty training, and all (surgical) specialties are now counted as a main specialty. This poses a risk for “double counting” of trainees in the past, who were members of both general surgery (Norwegian Surgical Association; NKF) and gastrointestinal surgery (NFGK) or other specialty surgery associations, but as all specialties have become main specialties since 2019, the risk of double counting should be limited. Considering a potential bias, it is toward a slight inflation of the number of members/trainees in general surgery. Per February 2025, the NMA had 36,060 memberships registered across 46 specialty associations, for a total of 32,750 unique members, suggesting 3310 with more than one registration, for a maximal rate of 10% of double registration in specialty associations (some may hold true double registration from training in two different specialties, if shifting from one specialty to another). Both general surgery and general internal medicine have been the main speciality bearing associations in the past, with subspecialty training (and membership registration) incorporated with its associated double registration, of which internal medicine is more than twice as large as general surgery (per February 2025, Norwegian Internal Medicine Association had 3426 members recorded, and Norwegian Surgical Association had 1465 members; not counting other memberships in any other surgical specialty associations for either of these). Hence, double registration will likely inflate general surgery to a smaller extent but be a valid approximation for the actual number of surgical specialty registrations across most surgical specialties.
The number of active consultant surgeons assumed to be in clinical practice was culled from data of all certified specialists registered at <70 years of age, as available per 11 November 2024. The point estimate of physicians in age assumed to be working-active will allow to give an assumed estimated number of surgeons in current clinical practice. Furthermore, a comprehensive view of actively working surgeons per gender and age groups (in 5-year increments) was culled and presented to give a point-prevalence estimate of the surgeon workforce, as of February 2025.
Surgical specialists, definition, and time periods
As there is no formal person registry available for each time period and for each speciality, there are some assumptions to take into consideration for the data set. For a time period, a specialist is registered when he or she has applied for board certification, and this application has been approved (central process held by the NMA; later by the Directory of Health). It does not imply that the same person works in that speciality, and further certified specialties may be applied for based on the given accreditation process at any given time period. Also, to be registered as a certified specialist implies that the person resides in Norway; hence, board-approved specialists in Norway working or living abroad are not counted. Finally, to account for the actual working-age population (and not include a disproportionate number of retired specialists), a cutoff for specialist was set at <70 years of age at any given time point for the current study.
Statistics and data interpretation
For the current study, the descriptive data have been provided in numbers and rates without a formal attempt at statistical analyses. We believe that p-values will not add to the quantitative information provided by graphs and tables and hence have avoided formal statistical analyses on top of the presentation of the current situation of medical students, persons registered in training, certified surgical specialists, and the female rates across these categories in Norway.
Results
The number of medical students with female rates is presented in Fig. 1A. After a decade of steady increase (2010–2020) in female rates, the number of women has stabilized at 70% over the past years. Among the total number of almost 5000 medical students, the number of medical students who are enrolled in medical schools abroad has been steady at about one-third, with a slight decline noted over recent years (from about 35% in 2017 to 30% in 2024; Supplementary information). The number of students admitted to Norwegian institutions has increased over the past few years, which may explain the slight decline in student going abroad. Poland and Hungary are the primary countries admitting Norwegian students abroad (Supplementary info), with Denmark as the only other Nordic country ranked as the fourth most common country abroad for Norwegian medical students.
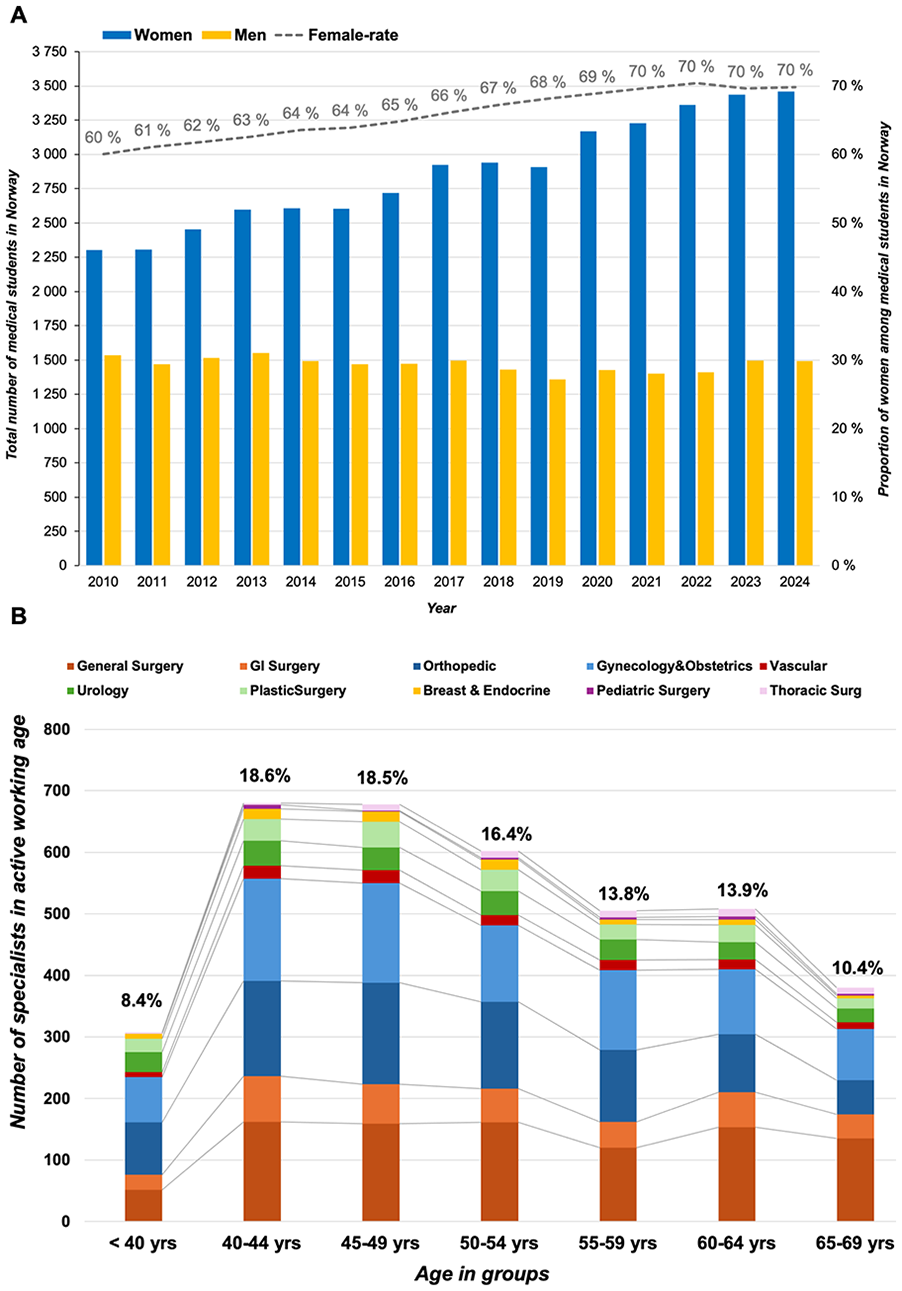
Medical students and the active surgical workforce. (A) The rate of females admitted to medical schools in Norway. (B) The number of active surgeons per discipline and per age groups in Norway.
For 10 surgical specialties, there were 3660 active surgeons (<70 years of age) as of February 2025. The number of active surgeons per specialty and age groups is given in Fig. 1B. As demonstrated, the number of active surgeons is declining for each 5-year incremental age group after 50 years of age. With a perceived age of retirement at 70 years (currently, the official retirement age is 67 years in Norway), over 10% of surgeons are expected to retire within the next 5 years and about 25% within the next 10 years, of which the vast majority will be male surgeons. For on-call covering specialties (i.e. general and gastrointestinal surgery), these numbers are even higher, at 12% in 5 years and 28% in the next decade, of which the majority are male surgeons.
As of November 2024, there were a total of 9601 doctors in training in Norway across all the 46 medical specialties, of which 6022 (62.7%) were women. Among all in training, there were 1304 (13.6%) who were registered in any of the 10 surgical specialties (Fig. 2A, B), and there were 817 women (62.7%) among these. Gynecology (n = 324) stands out with >90% of the trainees being female. Excluding gynecology, the female rate of surgeon trainees drops to 53.5% (524 of 980). Even though breast-endocrine and plastic surgery have a high female rate of trainees (>80% and >70%, respectively), they make up for a relatively small actual number of surgical trainees altogether (n = 23 and n = 40, respectively). For 2024, the total number of certified surgeons (n = 3636), with 1409 (38.8%) being female, was lower than the national average for all specialties (48.9%).
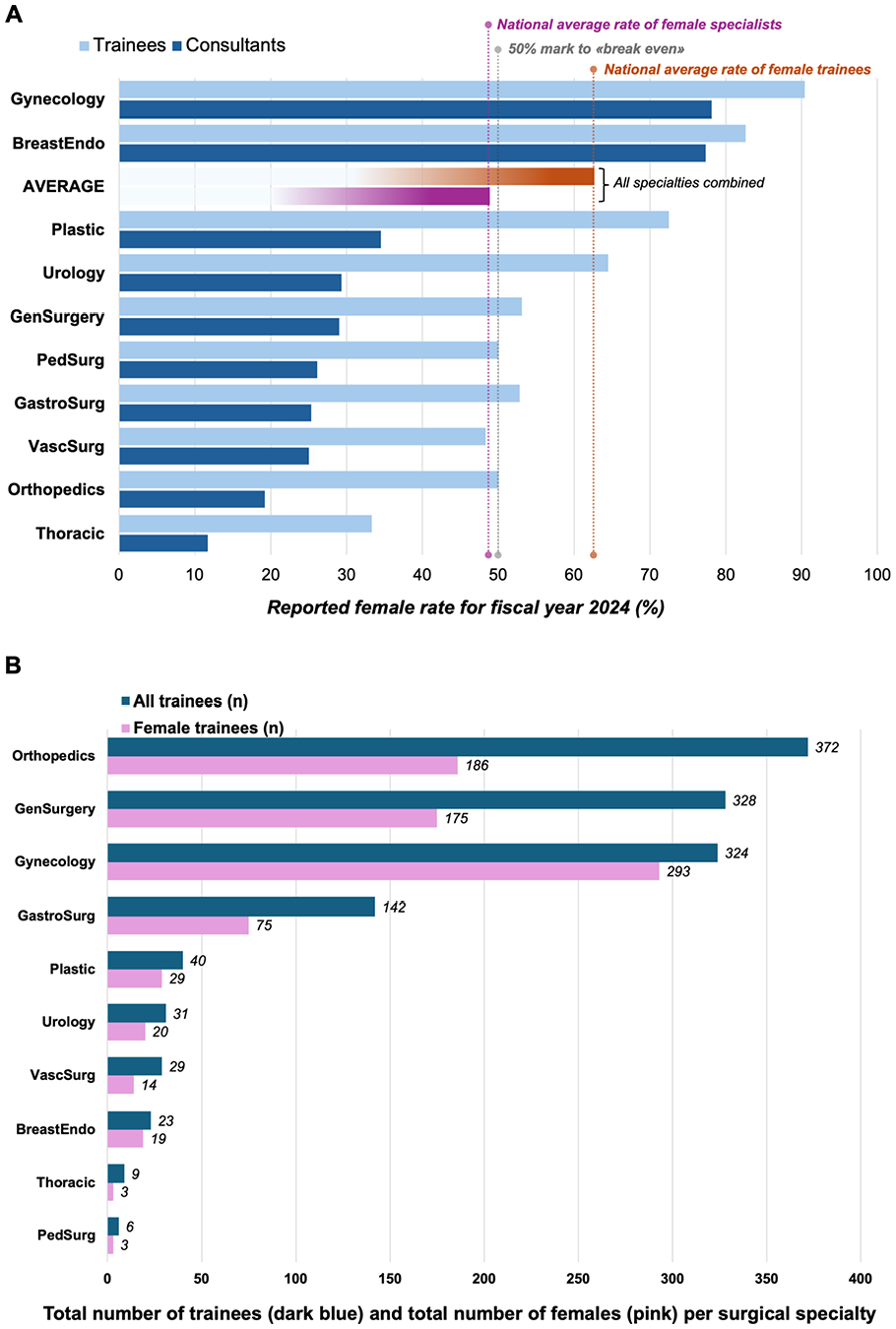
Rates of trainees and surgical specialists in Norway. (A) The rate of females in training and females as specialists across surgical specialties (index year 2024) and compared to the national average for all medical disciplines. (B) The absolute number of trainees in surgical specialties ranked according to numbers and number of females in training for each specialty (index year 2024).
The female rate at two-thirds of all in surgical training matches the average female rate across all other specialties. However, this rate only applies when including gynecology, as the rate otherwise is just more than half of all trainees. Also, there are numerical differences across each surgical specialty (Fig. 2B). In total numbers, orthopedics, general surgery, and gynecology together with gastrointestinal surgery make up the largest part of all female trainees in surgical training.
The corresponding total number of consultant surgeons for the surgical specialties was 3636 certified surgeons, with 1409 being female surgeon consultants (38.8%), which is lower than the national average for all medical specialties at 48.9%.
Considering the projection for retirement, which will influence the availability of surgeons in clinical practice and have an impact on the surgical workforce, there are considerable differences between male and female surgeon specialists (Fig. 3A, B), with a larger proportion of men approaching retirement age within the next 5 to 10 years. This difference becomes even more prominent when excluding gynecology and orthopedics and strictly focusing on the specialties dealing with what would be considered the on-call and general surgery coverage, mainly done by general and gastrointestinal surgeons (Fig. 4A, B).
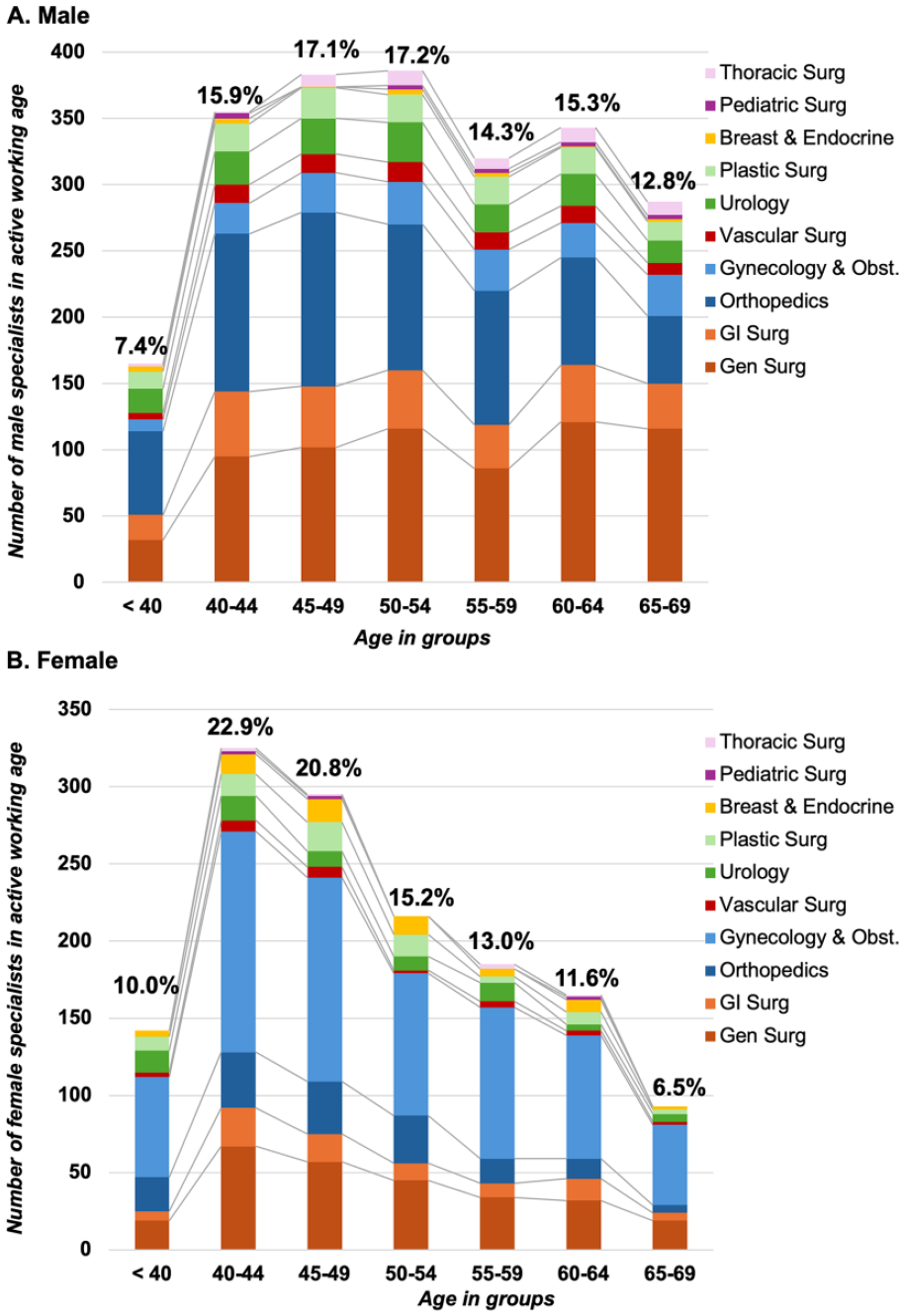
The number of active surgeons for 10 surgical disciplines and per age groups. (A) For males per surgical discipline and per age groups. (B) For females per surgical discipline and per age groups.
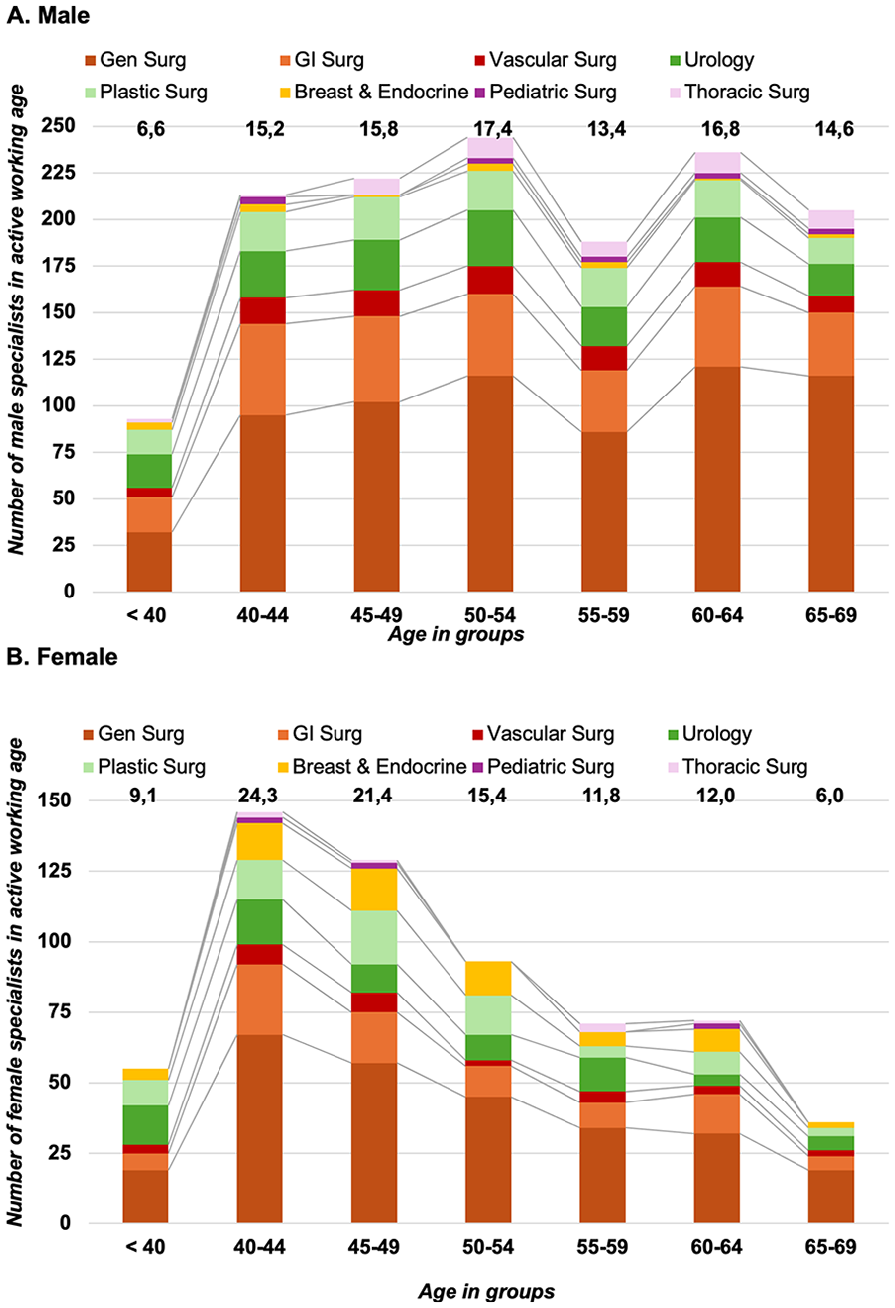
The number of active surgeons excluding gynecology and orthopedics. (A) For males per surgical discipline and per age groups. (B) For females per surgical discipline and per age groups.
Discussion
In this study, we found a steady female rate of 70% of all medical students in Norway (including those studying abroad). The female rate of trainees was 62.7% (all medical specialties included), and the trainee female rate was similar at 62.7% for all in surgery. However, the trainee rate in surgery is largely due to the very high rate of females in gynecology—without gynecology, the female rate of surgical trainees is 53.5%, which is lower than the national average of all medical specialties. The number of certified specialists in the surgical specialties investigated is lower than the national average as well (48.9%), with female certified surgeons at 38.8% in 2024. The numerical difference across surgical specialties is considerable, and hence, the time to “break even” for a gender balance and even to close the gender gap in some surgical disciplines may still take a considerable time—if not decades. Notably, a considerable proportion of male surgeons are approaching retirement age, which will influence the surgical workforce (Fig. 5).
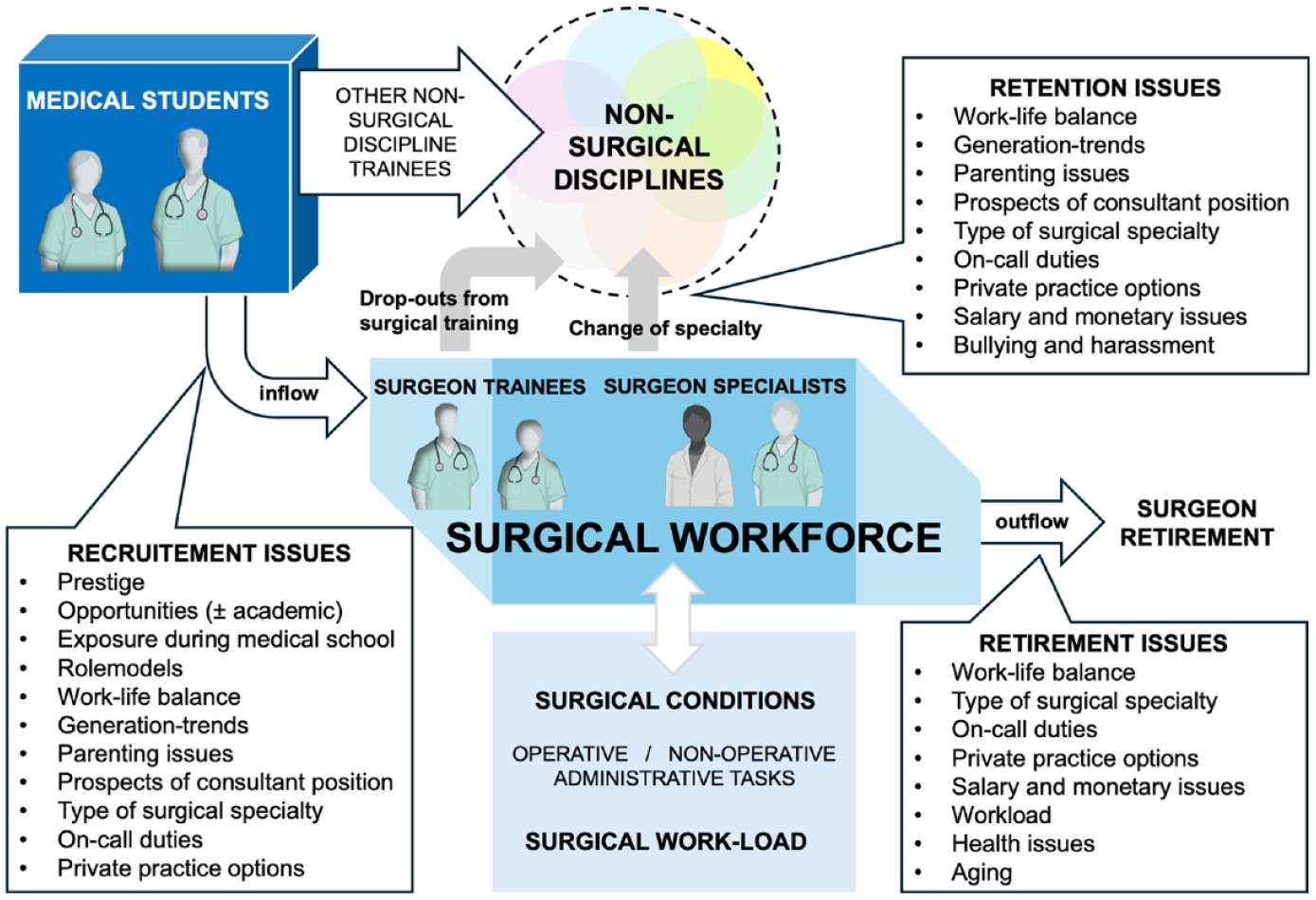
The inflow and outflow to the surgical workforce.
Achieving a “gender balance” in surgery may not be a goal in and of itself, as long as one can provide a sufficient number of surgeons to cover the public health care need for surgical conditions. We do not argue for a need for an absolute balance in genders per se, as it may well be that some specialties may thrive with a male or female predominance in a specialty. However, the need to achieve a balance is based on the share numbers: with a consistent rate of 60%–70% medical students being female for some two decades, the source to recruit new surgeons from is mainly female students (Fig. 5). Should female students choose not to (or, only to a minor degree) become surgeons, then there will be a deficiency of candidates entering surgery in the future, as both the number of men will be lower (as few enter medical school) and also the number of women will be low (as the recruitment is slow into surgery) and the elderly pool of surgeons (those 60 years and over) will eventually retire within the next decade (Fig. 5). The breaking point will be decided by the number of surgeons required to deliver safe and sustainable surgical care across hospitals, that is, the prevalence of surgical conditions in the population. Currently, no numbers currently exist nor have been proposed to project the need for future health care related to surgical disciplines. Surgical workload is hard to predict from the past, as it consists of surgical procedures but also a change in indications and disease spectrum. In addition, an increasing number of non-operative tasks fall on the surgeons to deliver. Also, an increase in administrative responsibilities and an increased workload to document and report are changing the working domains of surgeons.
It is unclear why there is a slow recruitment rate to surgery in general, even in the Nordic countries where the working conditions in general have been described as favorable,13,17,21 with social and welfare systems in place and an inclusive working regulation for parental leaves and social security in addition to less excessive working hours. This may not apply universally to all occupational areas, and the medical profession and particular surgery may come with certain strains on what is otherwise usually perceived as a good balance between work and life outside work. Similar observations have been made in Switzerland regarding surgery training, 22 and parental issues during training remain a global challenge. 23 Despite the observations of apparent slow recruitment to surgery among females, previous studies have shown that female students are not negative toward surgery as such, but various other factors may have an influence on choice of specialty career after medical school.18,19 A similar observation has been reported from the United States, showing a decline in the rate of female students going into surgical specialties. 24 Several studies have pointed to the positive role of exposure to surgery during medical school, that is, through surgical clerkships, as this may help break down barriers and perceptions of surgeons and surgical work and increase recruitment to surgical disciplines.1,25,26
There may be a general change in the perception of surgery as a career choice that may reflect to some degree the generation shifts, from the Baby Boomers to Millennials to the upcoming Generation Z.27,28 We would be careful with making swift and broad characterizations of medical students by generation characteristics, yet it is clear that the influence of upbringing, societal impacts, and access to learning technology (iPhones, tablets, electronic sources of information, social media) brings new opportunities and novel challenges in education and training. Also, different expectations, perspectives, and requirements may come with each generation and must be met by adaption and innovation where this is of benefit and serves progress for training and patient care (Fig. 5). New curricula and training platforms are being shaped, 29 including mentorship programs that have become very popular by demand.30,31 More broadly, a change in training from merely procedure counting to competency-based training is a further mind shift in surgical education. 32
There are ample data to suggest an existing implicit bias in the selection of candidates for positions and for career paths in medicine in which, among other factors, women are disfavored in several aspects.6,33–36 In a study from Sweden among medical student teachers, surgeons seemed to score lower on gender awareness than their non-surgical colleagues. 37 How women are met by their medical teachers may influence how they perceive the specialty or may consider it as their future workplace. The lack of gender role models and the impression of a harsh environment in surgery may represent factors that are deterring female away from surgery. 38 Further in-depth analysis is warranted in this field to investigate mechanisms and understand how to act to positively influence the medical students of today who will become the surgeons of tomorrow. Also, exposure to the surgery during medical school seems crucial to attract interest, as tried and reported in some surgical disciplines.39,40
Also, the skewed gender balance in gynecology (in favor of female trainee and specialists) is also of concern, as with the current rate, there will barely be any males left in this specialty in the near future. A sound gender balance may be warranted in both gender directions and across specialties. In a survey conducted by the Norwegian Gynecology Association, the responders mentioned that the reason for choosing gynecology and obstetrics was the variation, the practical and surgical inclination to treatment, and the importance of women’s health. While the latter may explain a female preponderance to selecting the specialty, the survey also disclosed that only 66% would have chosen the same specialty again, and more than one-third stated they had considered to quit or change specialty because of work-related strains. 41 Hence, not only recruitment to training but also retaining trained specialists will be crucial across surgical specialties going forward.
How to best identify and attract the next generation of students into surgical training has been much debated. To identify traits that fit with a “surgical personality,” a Dutch study investigated, proposed, and described traits related to surgery interest.42,43 This study found that surgeon-interested subjects scored higher on conscientiousness, open mindedness, and extraversion, and lower on neuroticism compared to non-surgically interested contemporaries. 43 A study from the United States even proposed screening high-school students for similar traits to identify surgeons for the future. 44 However, a more recent study from Sweden found that there are differences between male and female surgeons, 45 suggesting that one personality type (“the surgery personality”) is unlikely to be fit for specialty selection as such, and rather that difference and variation in personality traits may be complementary for the profession.46,47
In 2018, the NMA voted for a sex quota for admissions to medical schools in Norway, to ensure an admission rate of 40% of either gender to ensure a gender balance in admissions. 48 Gender-specific quotas have been practiced in the past also to increase female admissions to typical male-dominated areas such as data, programming, or electronic sciences, while male quotas have been practiced in psychology and veterinary sciences, as typical female-dominated sciences. A sex-based quotation system has yet to be practiced in the admission to medical school and remains under debate and for political evaluation. Importantly, diversifying the surgical workforce is essential, to maintain equal opportunities and access to training independent of background and beyond the gender balance.49,50
In summary, despite a high female rate of admissions to medical schools over the last two decades, the recruitment to training and to completed specialty training in surgery seems to lag. Gynecology is the outlier in volume and rate of females across all surgical disciplines, and some of the larger surgical specialties including general surgery, orthopedic surgery, and gastrointestinal surgery are approaching a gender balance.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969251355053 – Supplemental material for The gender gap between female medical students and recruitment to surgical training in Norway: A cross-sectional, nationwide cohort study of medical students, surgical trainees, and specialists
Supplemental material, sj-docx-1-sjs-10.1177_14574969251355053 for The gender gap between female medical students and recruitment to surgical training in Norway: A cross-sectional, nationwide cohort study of medical students, surgical trainees, and specialists by Kjetil Søreide, Torhild Veen, Elen M. Hauge, Martine Aarsland and Cecilie F. Torkildsen in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank senior statistician Anders Taraldset for providing updated data on surgical specialist from the NMA statistics.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.F.T. reports having received personal fees from AstraZeneca, Pfizer, and GlaxoSmithKline, but none with relevance to the current work. None of the other authors declare any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.