
Abstract
Study Design:
Retrospective cohort study.
Objective:
In orthopedic surgery, the use of antibiotic-impregnated spacers is a well-established method for treating periprosthetic joint infections with excellent outcomes. However, their application in head and neck surgery remains poorly documented, despite the high susceptibility of these patients to persistent infections. The objective of this study was to evaluate the 10-year outcomes of antibiotic spacers in the treatment of persistent mandibular infections unresponsive to conventional methods, prior to definitive reconstruction.
Methods:
We retrospectively reviewed patients with persistent mandibular infections treated with antibiotic-impregnated spacers between 2014 and 2023. Patient characteristics, surgical details, infection type, and clinical outcomes were assessed. The two-stage surgical protocol was described.
Results:
Seven patients (mean age 49 years, range 20–77) were included. Six had undergone complex mandibular reconstructions for malignant tumors (n = 3), benign tumors (n = 1), or congenital anomalies (n = 2). One patient had osteomyelitis of the jaw with extensive necrosis. Following spacer placement, complete resolution of infection occurred in 3/7 patients, a transition to non-suppurative infection in 3/7, and suppurative infection in 1/7. On average, infections recurred 5 months postoperatively. All infections resolved by the time of spacer removal, allowing definitive reconstruction.
Conclusion:
Antibiotic-impregnated spacers appear to be a promising adjunct in managing persistent mandibular infections, facilitating successful permanent reconstruction in complex head and neck cases.
Keywords
Introduction
Periprosthetic joint infection (PJI) is a serious complication in orthopedic surgery, affecting 0.7%–2% of total knee arthroplasty patients. Despite advances in treatment, PJIs continue to pose significant clinical challenges.1,2 A standard two-stage surgical approach is frequently employed, which involves temporary placement of antibiotic-loaded polymethylmethacrylate (PMMA) spacers. 3 These spacers deliver local antibiotics and promote a favorable tissue environment for subsequent permanent prosthetic reconstruction described by Masquelet and Begue. 4 The success rate of this technique is high, ranging from 75% to 100%.3,5 –7
In head and neck surgery, postoperative infections remain a significant cause of morbidity. 8 Extensive resections, reconstructions with vascularized flaps, exposure to contaminated anatomical sites, and patient groups with complex medical and surgical background contribute to a high risk of infection, reported in up to 43% of cases.9,10 These infections are particularly challenging when reconstruction involves hardware such as plates, TMJ prostheses, or custom implants, which support biofilm formation, and necessitate hardware removal for infection control. 11
Despite the success of antibiotic spacers in orthopedics, their use in head and neck surgery is rare. This study explores their application in persistent mandibular infections following major ablative and reconstructive procedures, reporting a 10-year single-center experience.
Methods
Study design and patient selection
We conducted a retrospective review of patients treated at the Department of Oral and Maxillofacial Diseases, Helsinki University Hospital, between 2014 and 2023. Inclusion criteria were: persistent mandibular infection resistant to conventional treatment, and treatment with a custom-made antibiotic-impregnated spacer.
Data collection
Patient data were extracted from electronic medical records, including demographics, comorbidities, prior surgeries, indication for spacer use, infection type (suppurative vs non-suppurative), timing of infection recurrence, complications, follow-up duration, and postoperative outcomes.
Suppurative infections were defined as those with purulence and/or fistula formation. 8 Non-suppurative infections included cellulitis, chronically open wounds, or dry fistulas. All infections were chronic infections, defined as persistent symptoms for over 4 weeks. 12
Spacer design and surgical technique
Spacers were manufactured intraoperatively using sterile technique as shown in Fig. 1. Preoperatively milled patient-specific titanium plates were embedded in gentamycin-loaded PMMA cement (Refobacin® Bone Cement R, Zimmer Biomet) within custom three-dimensional (3D)-printed molds. The cement was allowed to cure before the spacer was fixed with titanium screws.
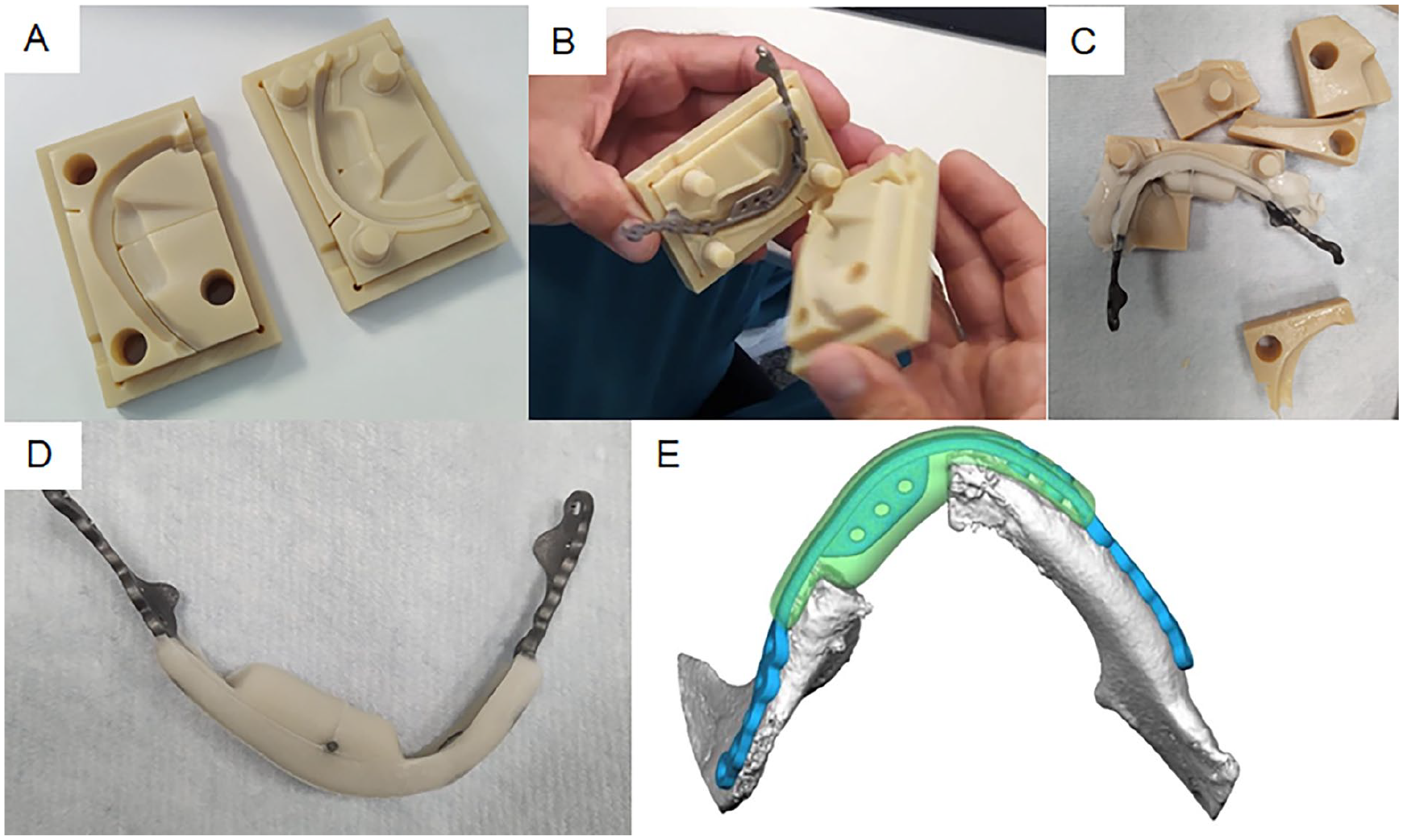
Preparation and 3D planning of the antibiotic-impregnated spacer for patient 7. A 76-year-old female with squamous cell carcinoma of the right floor of the mouth underwent extensive tumor resection, segmental mandibulectomy, and reconstruction using an osteocutaneous microvascular free flap with dental implants. Due to postoperative infection, a custom-made antibiotic spacer with a titanium plate core was designed and fabricated: (A) Two-part mold used for spacer fabrication, (B) Titanium plate positioned inside the mold; visualization of how the two halves of the mold are assembled after pouring bone cement over the plate, (C) The finalized spacer after cement has hardened and the mold has been removed, (D) Spacer in its final form prior to surgical placement and (E) Virtual 3D planning image showing the spacer aligned over the mandibular contour.
Virtual planning and manufacturing
High-resolution computed tomography (CT) scans were used to design the titanium plates and molds. Planning was performed collaboratively by an experienced maxillofacial surgeon and biomedical engineer. Computer numerical control (CNC)-milled titanium implants (grade 2, 0.3–0.4 mm thick) were combined with molds made from biocompatible resin (BioMed Clear®). Overflow canals and positioning pins were incorporated for precision molding (Figs 2 and 3). All components were heat-sterilized preoperatively.
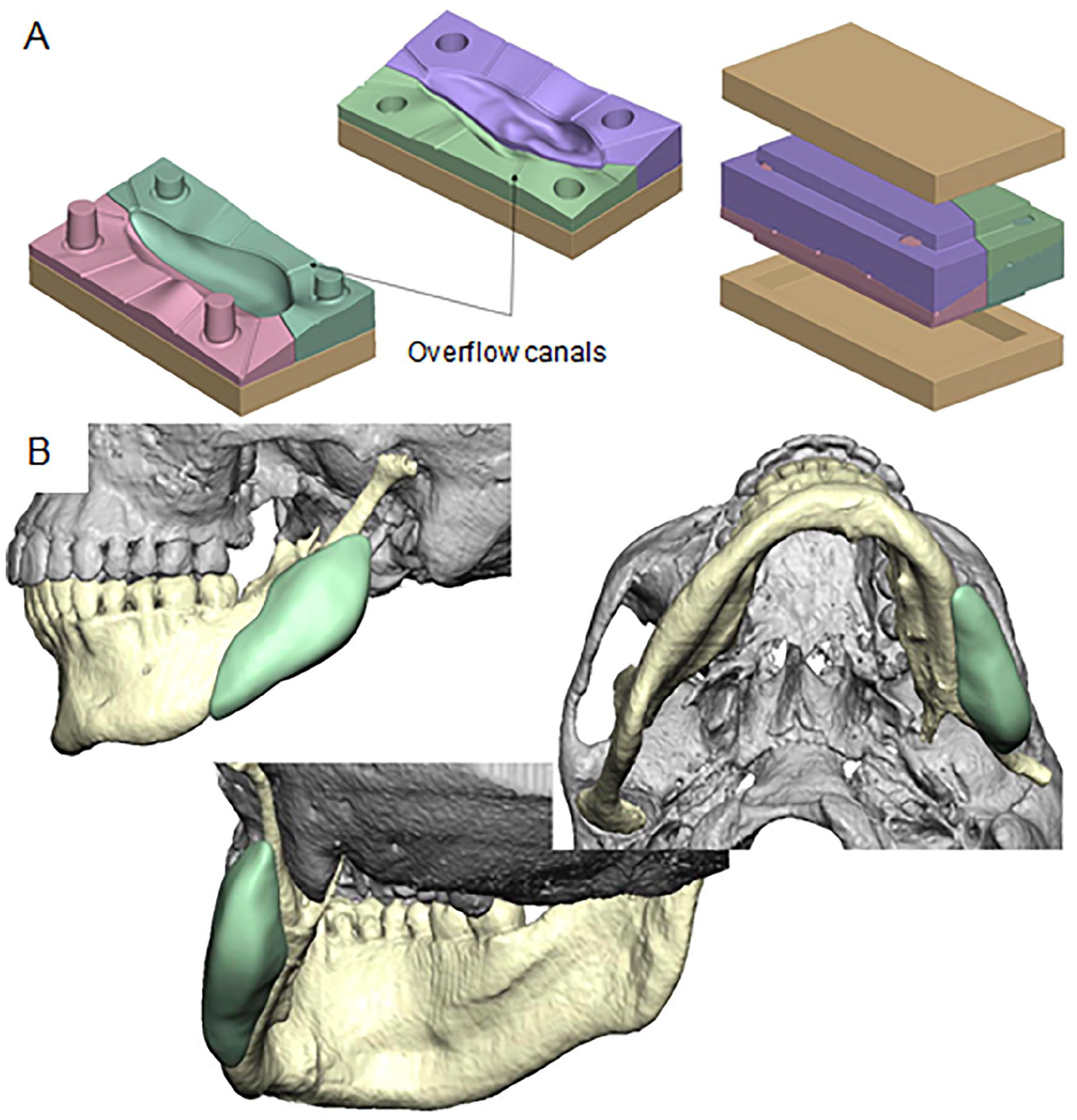
Three-dimensional planning of the spacer mold for patient 4, also illustrating the design of overflow canals. The mold was designed with overflow canals to allow excess cement to escape during pressing: (A) The mold consists of six parts: four forming the actual mold and two outer frame components. Arrows indicate the location of overflow canals. (B) Final positioning of the mold for the left mandibular angle region.
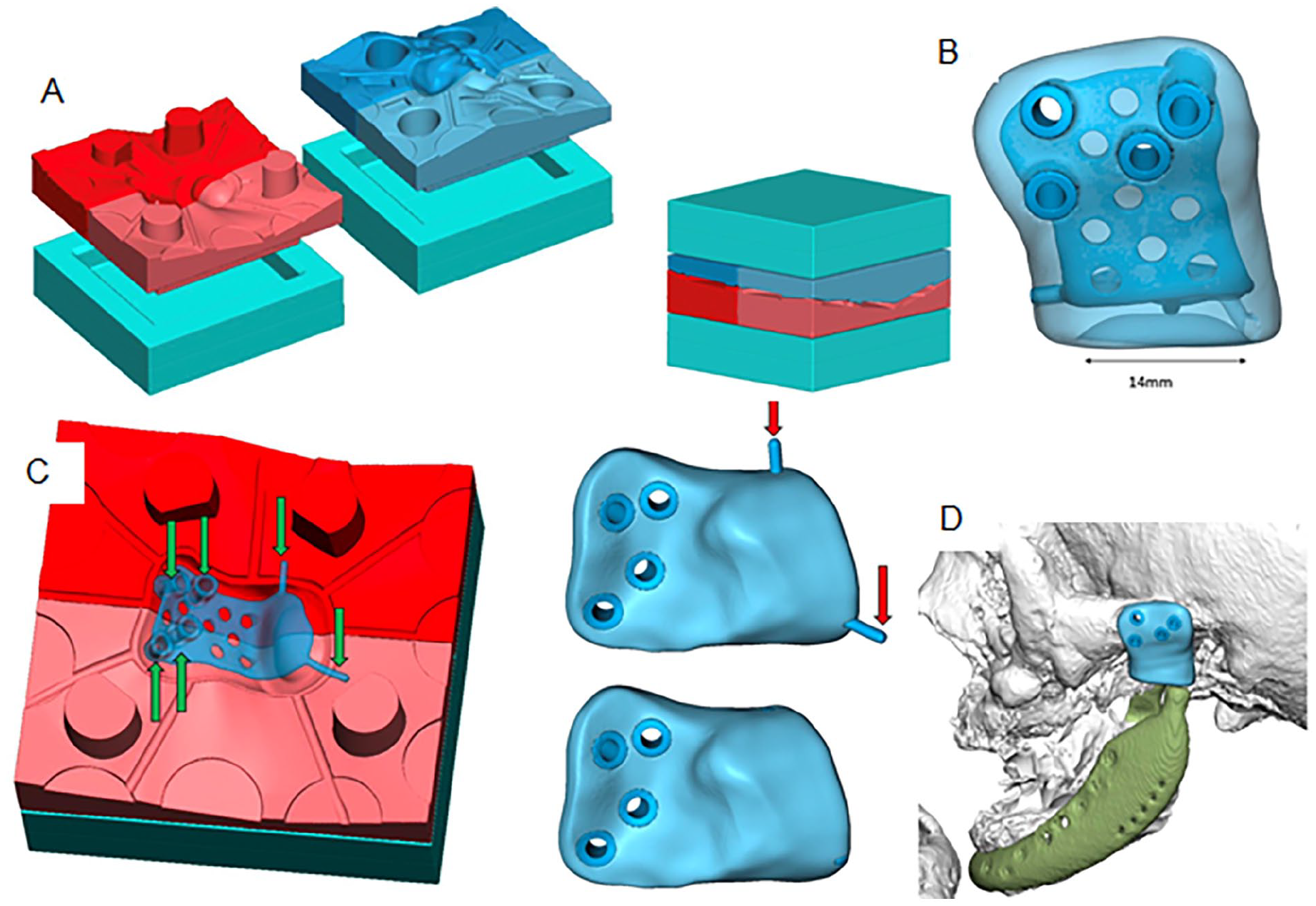
Three-dimensional design of the mold and antibiotic spacer for patient 2. A 33-year-old female with desmoplastic fibroma of the mandible underwent multiple surgeries including microvascular reconstruction and TMJ prosthesis placement, complicated by persistent postoperative infection. An antibiotic spacer replicating the TMJ prosthesis was planned: (A) Four-part mold system including mold components and frames, (B) Fossa component of the spacer, showing the titanium core embedded in cement, (C) Titanium plate secured in the mold with pins before cement application and (D) Final fit of the spacer replacing the TMJ fossa area.
Statistical analysis
Descriptive statistics were performed using IBM SPSS Statistics for Mac (version 24). Results are reported as means (range) and frequencies (%).
Results
Patient characteristics
Seven patients (6 females, 1 male) with a mean age of 49 years (range 20–77) were included (Table 1). Six had prior complex mandibular reconstructions: three for malignant tumors (parotid gland and floor of mouth), one for a benign tumor (desmoplastic fibroma), and two for congenital anomalies (Goldenhar syndrome and hemifacial microsomia). One patient had severe osteomyelitis and necrosis without prior oncologic surgery.
Patient demographics, details of the antibiotic spacer design, and infection status pre- and postoperatively.
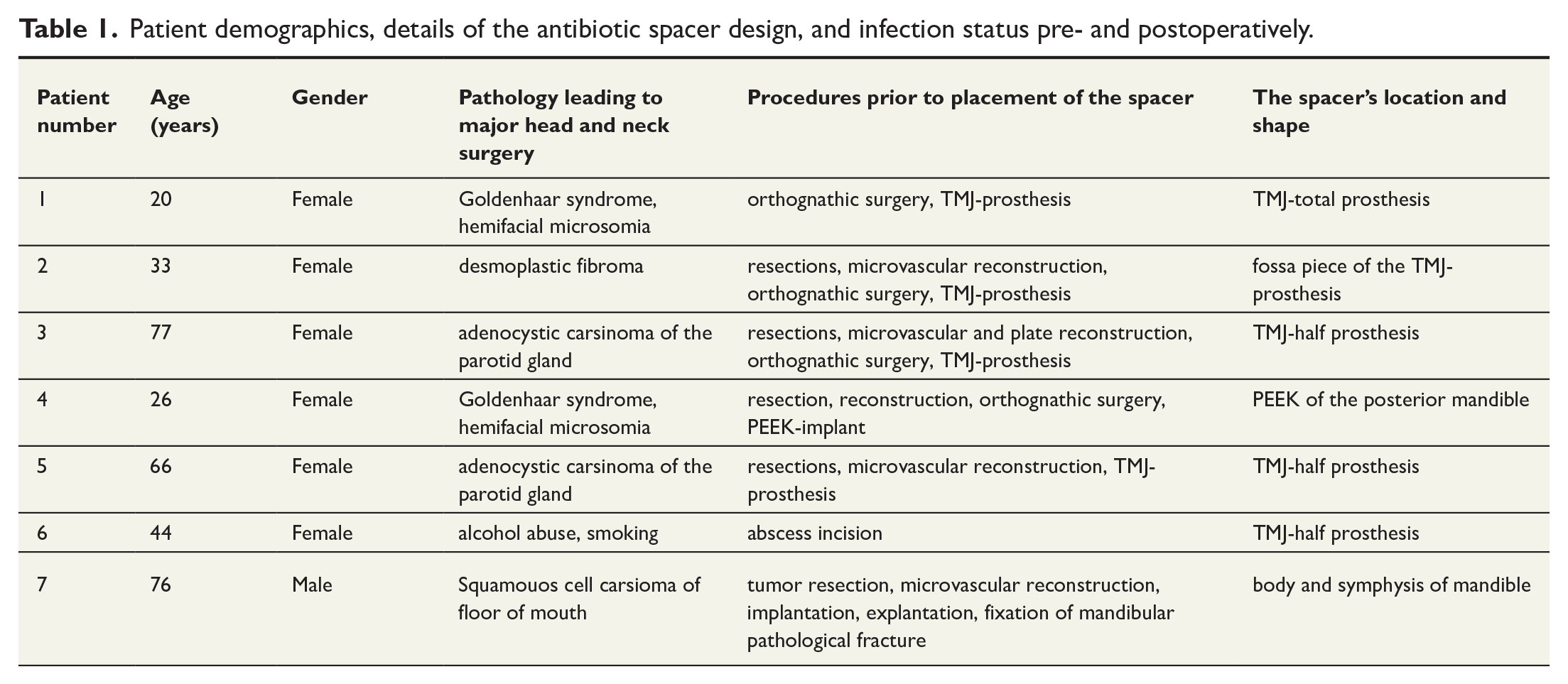
All patients had undergone multiple surgeries. Reconst-ruction materials included TMJ prostheses (n = 4), microvascular flaps (n = 6), and PEEK implants (n = 1). Two patients had received postoperative radiotherapy.
Spacer placement and outcomes
Indications for spacer placement included infected reconstruction plates (n = 5), extensive osteomyelitis with necrosis (n = 1), and post-implantation infection of a previously reconstructed neomandible with pathological fracture (n = 1). Preoperatively, infections were suppurative in four patients and non-suppurative in three.
Spacer designs included TMJ components (n = 4), fossa piece (n = 1), PEEK-replacing spacer (n = 1), and mandibular symphysis/body (n = 1) (Figs 2–7). Postoperatively, complete infection resolution occurred in three patients, conversion to non-suppurative infection in three, and persistent suppuration in one (Table 2).
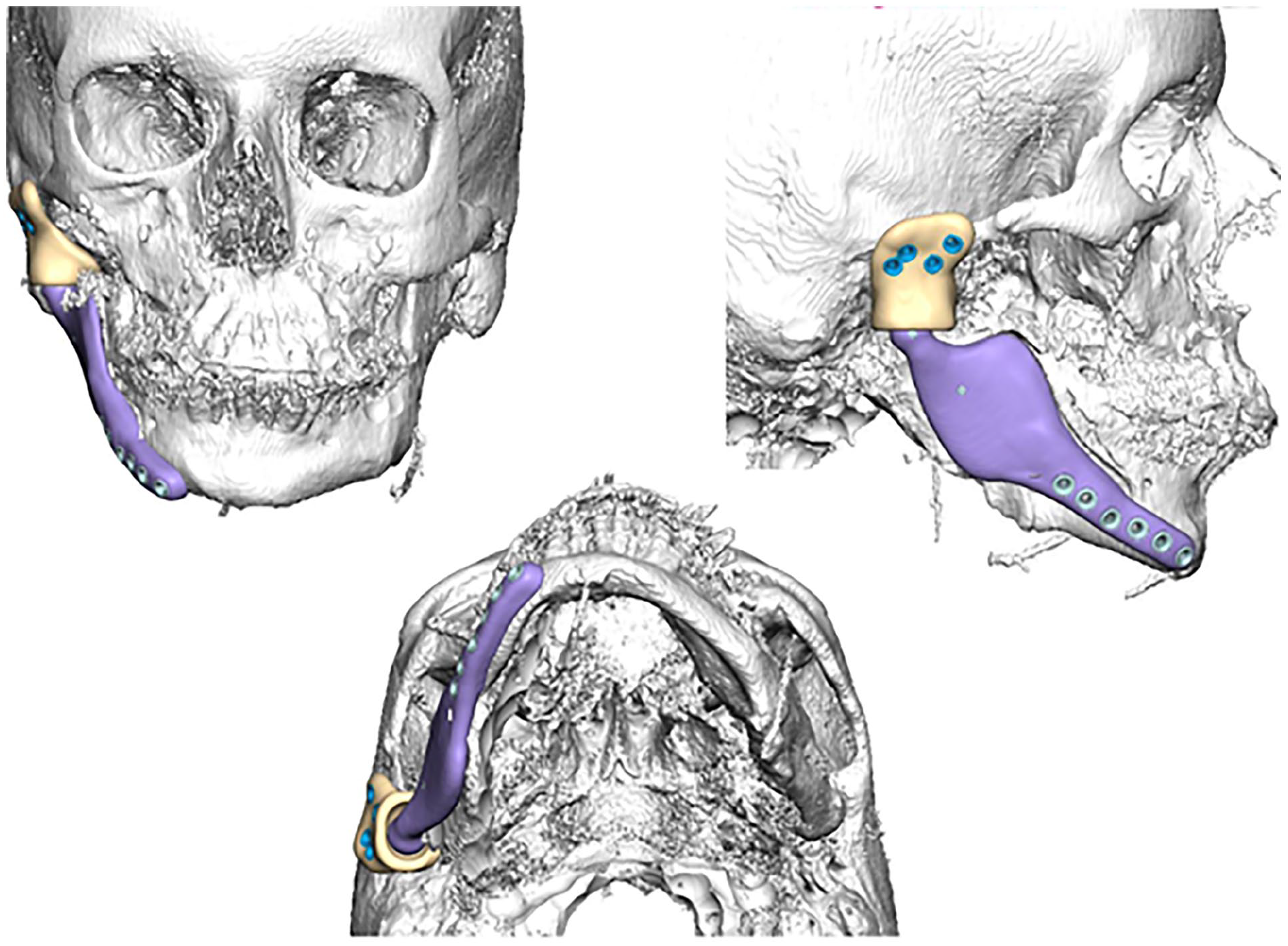
Three-dimensional design of the antibiotic spacer for patient 1. A 20-year-old female with Goldenhar syndrome and hemifacial microsomia had previously undergone orthognathic surgery including TMJ prosthesis placement, which became infected. A TMJ-shaped antibiotic spacer was designed to preserve the surgical site for future reconstruction.
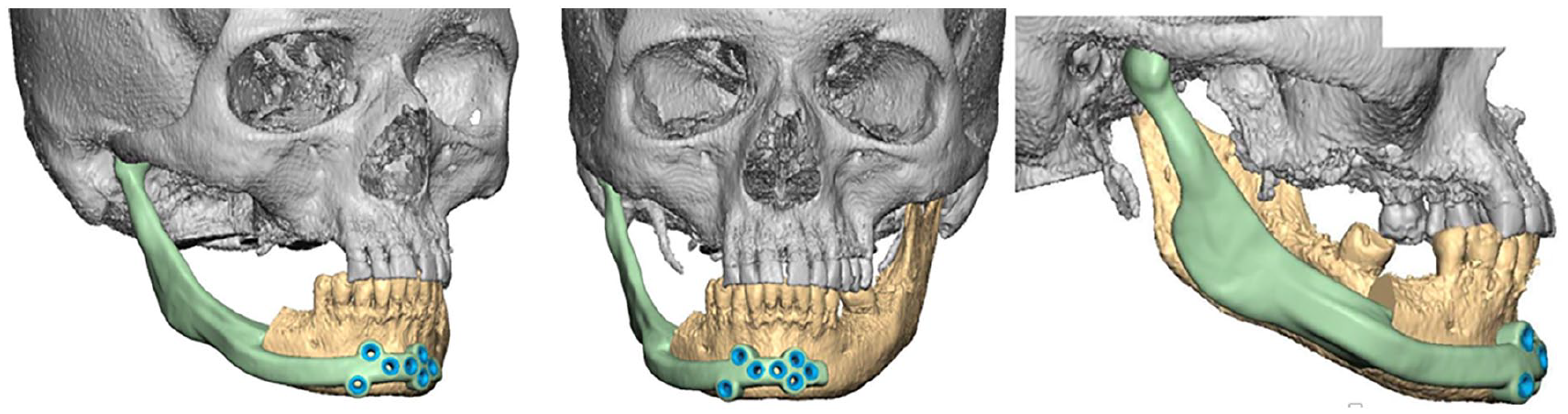
Three-dimensional design of the antibiotic spacer for patient 5. A 55-year-old female with advanced adenoid cystic carcinoma of the right parotid gland underwent tumor resection and reconstruction with a TMJ prosthesis. Following a persistent postoperative infection, a hemimandibular spacer with condylar extension was fabricated.
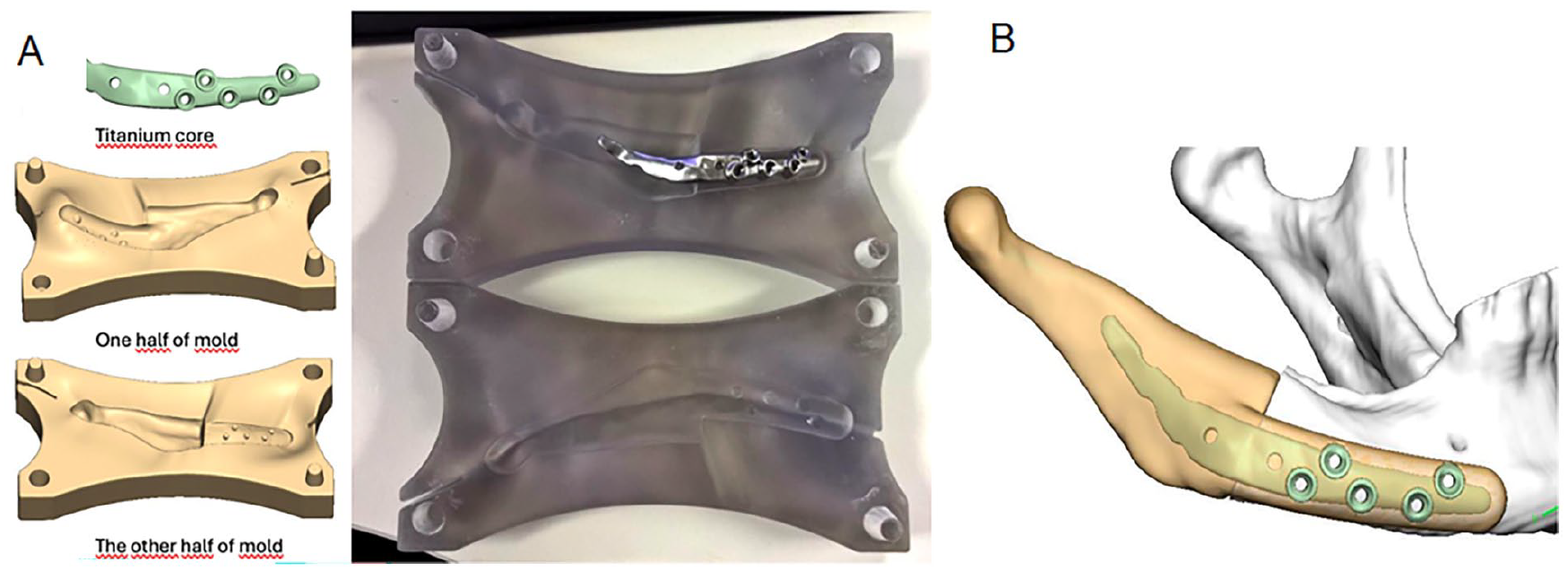
Three-dimensional planning of the mold and antibiotic spacer for patient 6. A 44-year-old female with chronic osteomyelitis and osteonecrosis of the right posterior mandible received a TMJ-half-shaped spacer extending anteriorly toward the symphysis: (A) Virtually planned mold and titanium plate shown both digitally and physically. (B) Final planned configuration of the antibiotic spacer.
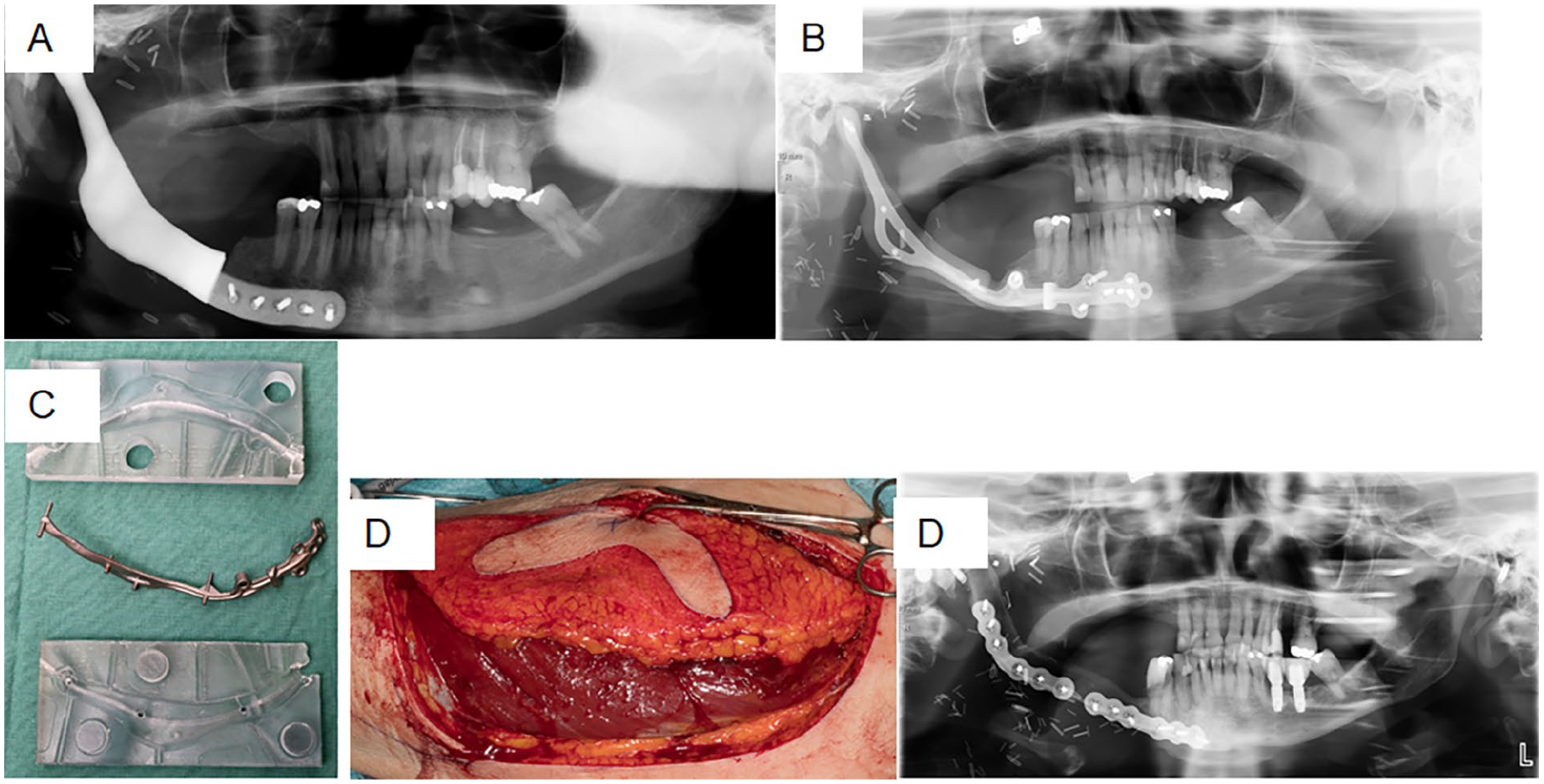
Pre- and postoperative OPGs of Patient nro 5: (A) Reconstruction of right segmental mandibulectomy that was performed with rest of extensive tumor resection without microvascular tissue transfer due to malignant tumor of parotid gland in another hospital. Onset of persistent infection, influenced by significant dead space in the resection bed, started after postoperative radiotherapy. Preoperative OPG prior to placement of the spacer, (B) Patient-specific implant replaced with a antibiotic-impregnated spacer (C) with an anterolateral thigh flap (D) and (D) After infection settled, spacer was replaced with a fibular free flap reconstruction. Postoperative OPG.
Clinical progression before and after spacer placement, including timing of spacer replacement and/or definitive reconstruction.
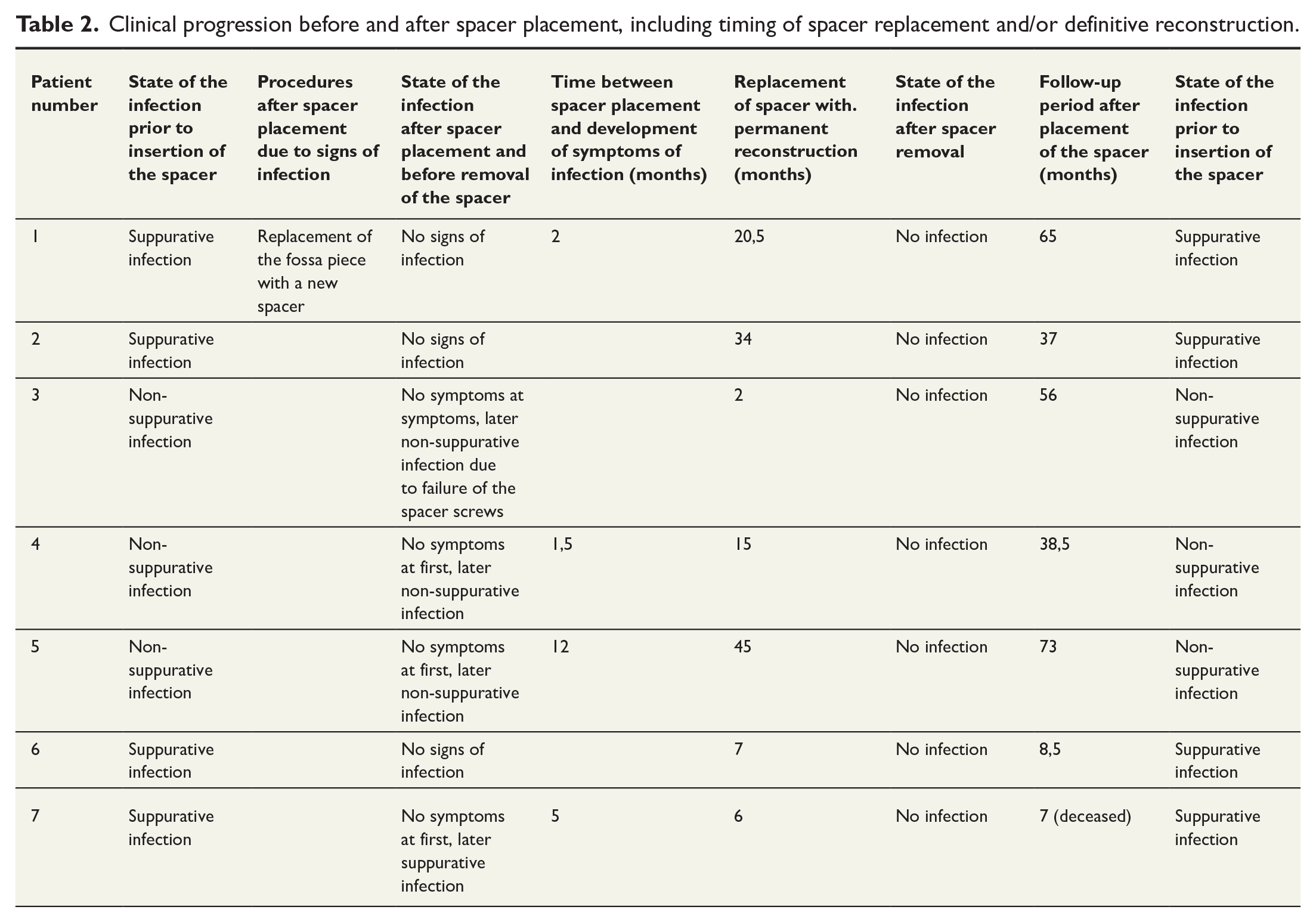
Infection recurrence occurred in four patients at an average of 5 months postoperatively (range 1.5–12 months). The average duration between spacer placement and permanent reconstruction was 19 months (range 2–45). Follow-up averaged 46 months (range 8.5–73).
In all cases, infection resolved by spacer removal, and definitive reconstruction was successfully performed (TMJ prosthesis n = 2, fibula flap n = 1, rib graft n = 1). One patient was lost to follow-up, and one died of unrelated causes postoperatively.
Discussion
This study presents the largest series to date of antibiotic-impregnated spacers used to treat persistent mandibular infections in patients with complex head and neck surgical histories. Our results demonstrate that antibiotic spacers effectively reduced infection severity and allowed for successful permanent reconstruction in all evaluable cases.
Persistent infections after mandibular reconstruction are notoriously difficult to treat, particularly in the presence of biofilm-coated hardware. Local delivery of high-concentration antibiotics via PMMA spacers provides a therapeutic advantage, especially when combined with surgical debridement and hardware removal. In addition to infection control, spacers maintain the original soft tissue envelope needed to accommodate the definitive implant or graft, facilitate safe extraoral access via preservation of anatomic location of nerves and vessels, and retain facial esthetics and contour. 13
The approach mirrors the principles of the Masquelet or Membrane Directed Bone Formation technique, wherein PMMA spacers not only provide antibiotic delivery but also induce a vascularized membrane conducive to bone regeneration.4,14,15 This membrane’s osteoinductive potential is highest within the first 2 months, supporting the rationale for early second-stage reconstruction. 15 Moreover, PMMA cement is an inert, well-tolerated, moldable, and easily trimmable material providing functional stability causing only minimal soft tissue contraction. 16 Gentamycin was selected for its broad-spectrum activity, thermostability, and established clinical use.14,17,18 The PMMA matrix ensures structural stability while supporting antibiotic elution. 18
Previous literature on spacer use in head and neck surgery is limited. Most reports focus on TMJ prosthesis infections,11,19 which is an incomparable clinical setting to the one presented in this article. However, their results with spacers replaced at 8–12 weeks with permanent prosthetic material were very promising.11,16,20 To our knowledge, only one prior study (Green et al. 21 ) has described similar applications in head and neck oncologic patients. The study included one patient with severe osteomyelitis and one with infected reconstructive material of the mandible, who received a tobramycin-impregnated spacer for a 3-month period with excellent results in terms of suppression of infection. These results are highlighting the novelty and importance of our findings.
Our results were encouraging in terms of suppression of the infections. However, the symptoms tended to recur at 6 months or later after placement of spacers. This suggests that an earlier replacement of the spacers might prevent infection from recurring, as also supported by the literature regarding osteoinductive properties of the Masqualet technique.4,14,15 This should be highlighted when planning future procedures and studies.
Our study is limited by small sample size, retrospective design, and patient heterogeneity. Nevertheless, it provides compelling evidence that antibiotic spacers may be a valuable adjunct in managing refractory infections in head and neck reconstruction.
Conclusion
Antibiotic-impregnated spacers are a promising tool for managing persistent mandibular infections following complex head and neck surgeries. In this series, all infections resolved with spacer use, allowing definitive reconstruction. These spacers offer the dual benefits of high local antibiotic delivery and preservation of surgical anatomy. Further prospective, multicenter studies are warranted to confirm these findings and establish standardized protocols.
Footnotes
Authors contributions
Malla Salli: Collected data, data analysis and interpretation, drafted the article
Emilia Marttila: Data interpretation, article revision, approval of the version of the article to be published
Karri Mesimäki: Design of the work, data interpretation, article revision, approval of the version of the article to be published
Tommy Wilkman: Design of the work, data interpretation, article revision, approval of the version of the article to be published
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.